

Abstract
Background
The purpose of this study was to investigate the primary factors associated with inappropriate out‐of‐hours emergency department (ED) use by patients with nonurgent conditions.
Methods
We compared patients with nonurgent conditions who made inappropriate, out‐of‐hours ED visits to patients who visited an acute care hospital during daytime consultation hours between May 30 and October 16, 2014, in terms of patient characteristics and reasons for consultation. Our goal was to identify factors associated with inappropriate ED use, defined as an out‐of‐hours, nonurgent, and unnecessary visits.
Results
We analyzed data from 84 patients who made inappropriate use of out‐of‐hours emergency care and 147 patients who sought care during regular consultation hours. In the inappropriate use group, “desire to be cured quickly” was the most common reason. Acute upper respiratory infection, acute gastroenteritis, and primary headache comprised 51.1% of diagnoses in the inappropriate use group. One factor associated with inappropriate use was two or more previous out‐of‐hours ED visits (odds ratio (OR) 3.19; 95% confidence interval (CI) 1.22‐8.31) (reference: 0 visits).
Conclusions
Patients with two or more previous out‐of‐hours ED visits were more than three times as likely to inappropriately use the ED compared to patients who had not visited the ED at all in the past 3 years.
Keywords: emergency medicine, inappropriate use, out‐of‐hours medical care
1. INTRODUCTION
Inappropriate out‐of‐hours use of the emergency department (ED) by patients with nonurgent conditions has become a problem in terms of increased medical expenses, crowding of emergency facilities,1 and burden placed on medical service providers.2 To properly address the problem of inappropriate ED use, associated factors and context require investigation.
Previous studies3, 4 showed that young age, lack of access to a primary care provider, dissatisfaction with the regular source of care, and anxiety and/or depression were factors contributing to nonurgent use of emergency medical care. However, the results of these studies were inconsistent.
To identify inappropriate use of EDs, previous studies defined medical urgency using criteria such as triage performed by nurses prior to physician consultation,5, 6 patient self‐reports of severity and necessity,7, 8 and whether or not hospitalization was necessary.9, 10 However, it is possible that patients who do not meet these criteria also require appropriate ED use.
Despite the fact that the above criteria are inadequate for identifying inappropriate use, a systematic review identified no studies that examined the judgment of the physicians in charge of patient consultations.3 The purpose of our study was to identify factors related to inappropriate ED use by comparing patients who sought medical care during regular consultation hours with those who visited EDs for out‐of‐hours care.
1.1. Study design and setting
This observational study was performed at Tsukuba Medical Center Hospital between May 30 and October 16, 2014. Tsukuba Medical Center Hospital is an acute care hospital located in a city in Ibaraki Prefecture. It has 453 beds and an emergency and critical care center. Since February 2006, all ambulatory emergency patients have been triaged by trained nurses to determine which patients are prioritized for physician consultation.11 Out‐of‐hours, all ambulatory patients are triaged and then the emergency physician on duty consults with patients. In contrast, during regular consultation hours on weekdays, general physicians consult with ambulatory patients in the general medicine department. This study was approved by the Tsukuba Medical Center Hospital Ethics Committee on June 18, 2013.
1.2. Study subjects
Subjects consisted of adult ambulatory patients who visited the ED between 17:30 and 22:00 on weekday evenings and patients who had an initial consultation with the department of general medicine during regular consultation hours on a weekday. Regular consultation hours at this hospital end at 17:30, while most regional out‐of‐hours clinics are open until 22:00.
The inclusion criteria consisted of the following: ≤3 days since symptom onset, The Japan Triage and Acuity Scale (JTAS)12 Level 4 or 5, chief complaint not related to traumatic injury, ambulatory status, and patient age ≥ 20 years.
The exclusion criteria consisted of the following: physician judgment of the inappropriateness of requesting study participation because of patient condition or other factors, dementia, difficulty understanding Japanese, withholding of consent, and hospitalization or referral to another medical facility.
JTAS is an ED urgency evaluation system based on the Canadian Triage and Acuity Scale (CTAS). JTAS is used prior to consultation as a support system to determine each patient's level of urgency and to determine the priority for consultation. Patients are placed into one of five levels: Level 1—resuscitation; Level 2—emergent; Level 3—urgent; Level 4—less urgent; and Level 5—nonurgent. Level 4 corresponds to conditions that would benefit from intervention or reassurance within 1‐2 hours because of factors such as patient age, distress, or potential for deterioration or complications. Level 5 corresponds to acute but nonurgent conditions as well as part of chronic problems. The expected hospitalization rate for CTAS Level 4 is between 3% and 10%, while that for Level 5 ranges from 1% to 4%.13 Since JTAS levels 1, 2, and 3 correspond to conditions in which emergency care is certainly appropriate, this study was limited to patients at JTAS levels 4 and 5.
1.3. Measurements
Self‐administered questionnaires were filled out by the patient and attending physician. The patient questionnaire collected data on patient characteristics (marital status, education level, number of cohabitants, and occupation), activities related to medical treatment (number of out‐of‐hours ED visits in the past 3 years, presence or absence of a primary care physician, regular clinic visits, and presence or absence of out‐of‐hours primary care clinics provided by municipal or local medical associations), the Hospital Anxiety and Depression Scale (HADS),14 and reasons for consultation. HADS was developed by Zigmond et al. as a self‐administered questionnaire to screen for anxiety and depression in patients with physical symptoms.14 It consists of anxiety and depression subscales, each with seven items. Each item is scored from 0 to 3; each subscale has a score interval between 0 and 21. A cut‐off score of 8 was used in this study to indicate anxiety and depression. A Japanese version of HADS was validated in a previous study.15
Regarding reasons for consultation, 12 choices, such as “desire to be cured quickly,” “wanted a prescription,” and “suggested by others,” were developed by the study authors based on prior research.16, 17 We included a 12th item, “inability to take time off from school or work during the day” to determine whether out‐of‐hours emergency care use was a matter of personal convenience. Only ED patients were asked about the 12th item. Answers for each choice were scored on a four‐point Likert scale of absolutely not, no, somewhat, or yes (Data S1 and S2).
The physician questionnaire collected data regarding patient gender and age, JTAS triage level, duration since symptom onset (few hours, half a day, 1 day, or 2‐3 days), and information from the medical consultation (chief complaint; diagnoses; whether treatment, laboratory testing, or imaging was performed; and whether a prescription was given). JTAS assessment was performed in accordance with guidelines by a triage nurse for out‐of‐hours emergency care and by the attending physician for initial visits at the department of general medicine during normal consultation hours. In order to identify inappropriate use, physicians made a determination after consultation regarding whether it was necessary to use out‐of‐hours emergency medical care only for patients who visited the ED (Data S3 and S4).
Patient questionnaires were distributed by an emergency visit assistant for out‐of‐hours visits and by the attending physician for visits during consultation hours. Physician questionnaires were distributed by an emergency visit assistant for out‐of‐hours visits and by an outpatient assistant for visits during consultation hours.
1.4. Statistical analysis
In order to compare inappropriate out‐of‐hours use of ED and regular consultation hour use, we defined the inappropriate use and consultation hour groups as follows: The inappropriate use group consisted of patients whose use of out‐of‐hours ED was determined by the attending physician to be unnecessary. The consultation hour group consisted of patients who initially visited the department of general medicine during weekday daytime consultation hours. The four‐point Likert scale for reasons for consultation was condensed to a two‐point scale by combining “absolutely not” and “no” responses as “no” and “somewhat” and “yes” responses as “yes.” The two groups were compared using Student's t test for continuous variables and the chi‐squared test for categorical variables. We used logistic regression to identify factors associated with inappropriate ED use. Independent variables consisted of demographic variables and variables that achieved P values of < 0.10 in the univariate analysis. The inclusion of independent variables in the multivariate analysis also took into consideration the number of patients in each group and the relationship between independent and dependent variables. Pearson's correlation analysis was performed between independent variables. Logistic regression results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). A P value < 0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS version 25 (IBM Corp, Armonk, NY, USA).
1.5. Sample size
This research sought to analyze the causes of inappropriate use with logistic regression. The model assumptions consisted of eight explanatory variables. Thus, a rough estimate of 80 (8 × 10) participants was determined to be the necessary sample size. Estimating a valid response rate of 80%, the necessary sample size was set at 100.18
2. RESULTS
A total of 413 patients met the inclusion criteria, which included 147 out‐of‐hours ED patients and 266 patients who initially visited the department of general medicine during regular consultation hours. There was no duplication of patients. Owing to staff workload, 35 and 100 patients in the two groups, respectively, were unable to complete the questionnaire. In addition, four and 19 patients, respectively, were excluded from the study because of withholding of consent, having a traumatic injury as the chief complaint, hospitalization, having dementia, or failure to answer the questionnaire. For out‐of‐hours emergency consultation, 24 patients whose use was determined to be appropriate by the attending physician were also excluded. Analysis was conducted on the remaining 84 patients in the inappropriate use group and 147 patients in the consultation hour group (Figure 1).
Figure 1.
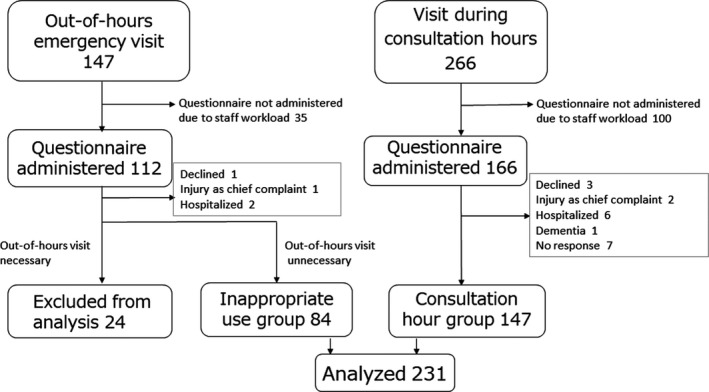
Study flowchart
2.1. Characteristics of study participants
The two groups had no significant differences in age, gender, having their own primary care physician, or awareness of out‐of‐hours primary care clinics provided by municipal or local medical associations. Anxiety and depression were identified in around 20% of patients in each group, with no significant difference between them. In the inappropriate use group, 98.8% of patients were classified at JTAS Level 4 (less urgent), which was a much higher proportion than the 57.1% in the consultation hour group (P < 0.0001). Regarding duration since symptom onset, 38.6% of the inappropriate use group had a duration of a few hours, 26.5% had half a day, 25.3% had 1 day, and 9.6% had 2‐3 days compared with 9.7%, 11.1%, 30.6%, and 48.6%, respectively, in the consultation hour group (P < 0.0001) (Table 1).
Table 1.
Patient characteristics (n = 231)
| Inappropriate use group (n = 84) | Consultation hour group (n = 147) | P value | |
|---|---|---|---|
| Male gender, n (%) | 51 (60.7) | 76 (51.7) | 0.19 |
| Age, mean ± SD | 43.5 ± 18.5 | 44.3 ± 17.6 | 0.75 |
| Triage level, n (%) | |||
| 4 (less urgent) | 83 (98.8) | 84 (57.1) | <0.0001 |
| 5 (nonurgent) | 1 (1.2) | 63 (42.9) | |
| Duration since symptom onset, n (%) | |||
| A few hours | 32 (38.6) | 14 (9.7) | <0.0001 |
| Half a day | 22 (26.5) | 16 (11.1) | |
| 1 d | 21 (25.3) | 44 (30.6) | |
| 2‐3 d | 8 (9.6) | 70 (48.6) | |
| Has a primary care physician, n (%) | 37 (54.4) | 65 (46.8) | 0.30 |
| Regular clinic visits, n (%) | 24 (34.8) | 51 (37.0) | 0.76 |
| Out‐of‐hours primary care clinic provided by a municipal or local medical association, n (%) | |||
| Presence | 35 (51.5) | 79 (56.4) | 0.79 |
| Absence | 17 (25.0) | 32 (22.9) | |
| Does not know | 16 (23.5) | 29 (20.7) | |
| Anxiety, n (%) | 17 (26.6) | 30 (22.1) | 0.48 |
| Depression, n (%) | 15 (23.1) | 30 (22.2) | 0.89 |
| Lives with others, n (%) | 57 (83.8) | 106 (77.4) | 0.28 |
| Diagnosis, n (%) | |||
| Acute upper respiratory infection | 18 (21.4) | 21 (14.3) | 0.44 |
| Acute gastroenteritis | 16 (19.0) | 30 (20.4) | |
| Primary headaches | 9 (10.7) | 13 (8.8) | |
| Musculoskeletal disorders | 5 (6.0) | 14 (9.5) | |
| Unspecified abdominal pain | 5 (6.0) | 4 (2.7) | |
| Other | 31 (36.9) | 65 (44.2) | |
| Laboratory testing was performed, n (%) | 11 (13.3) | 46 (31.5) | 0.002 |
| Imaging was performed, n (%) | 15 (18.1) | 34 (23.3) | 0.36 |
| Received prescriptions, n (%) | 58 (69.9) | 102 (69.4) | 0.94 |
The chi‐squared test was used for categorical variables, and Student's t test was used for continuous variables.
Abbreviation: SD, standard deviation.
2.2. Diagnoses and procedures
The five most prevalent diagnoses were the same in both groups: acute upper respiratory infection, acute gastroenteritis, primary headache, musculoskeletal disorder, and unspecified abdominal pain (Table 1).
In the inappropriate use group, 69.9% of patients received prescriptions and 18.1% underwent imaging studies, compared with 69.4% and 23.3% in the consultation hour group, respectively, indicating no significant difference. Laboratory testing was performed in 13.3% of patients in the inappropriate use group, a significantly lower rate than the 31.5% in the consultation hour group (P = 0.002) (Table 1).
2.3. Reasons for consultation
The reasons for consultation in both groups were, in order of prevalence, “desire to be cured quickly,” “wanted a doctor's opinion,” and “wanted to know whether the condition was serious.” The first two reasons were endorsed by more than 90% of patients in both groups. There was no significant difference between the two groups. Importantly, 38.7% of patients in the inappropriate use group indicated “inability to take time off from school or work during the day” as a reason (Table 2).
Table 2.
Reasons for consultation (n = 231)
| Inappropriate use group (n = 84) | Consultation hour group (n = 147) | P value | |
|---|---|---|---|
| Desire to be cured quickly, n (%) | 62 (92.5) | 134 (96.4) | 0.23 |
| Wanted a doctor's opinion, n (%) | 58 (90.6) | 135 (96.4) | 0.09 |
| Wanted to know whether the condition was serious, n (%) | 52 (83.9) | 109 (82.0) | 0.74 |
| Condition was not improving, n (%) | 50 (80.6) | 96 (72.2) | 0.20 |
| Wanted a prescription, n (%) | 46 (76.7) | 97 (73.5) | 0.64 |
| Wanted laboratory tests done, n (%) | 41 (65.1) | 98 (74.2) | 0.19 |
| Desire for treatment by a specialist, n (%) | 35 (59.3) | 94 (71.8) | 0.09 |
| Recommended by others, n (%) | 27 (45.8) | 56 (44.4) | 0.87 |
| Over‐the‐counter medicine was not working, n (%) | 21 (35.6) | 37 (29.6) | 0.41 |
| Wanted to know if I could attend work, school, or events, n (%) | 14 (24.1) | 34 (27.0) | 0.68 |
| Wanted an intravenous drip, n (%) | 12 (20.7) | 15 (12.1) | 0.13 |
| Inability to take time off from school or work during the day, n (%)a | 24 (38.7) | ‐ |
The chi‐squared test was used for all comparisons.
This item was analyzed in the inappropriate use group only.
2.4. Previous experience with out‐of‐hours ED visits
In the inappropriate use group, 45.7% had no previous out‐of‐hours ED visits at any hospital in the preceding years, 21.4% had one previous visit, and 32.9% had 2 or more previous visits, compared with 58.0%, 28.0%, and 14.0% in the consultation hour group, respectively. The number of previous ED visits was significantly associated with being in the inappropriate use group (P = 0.006) (Figure 2).
Figure 2.
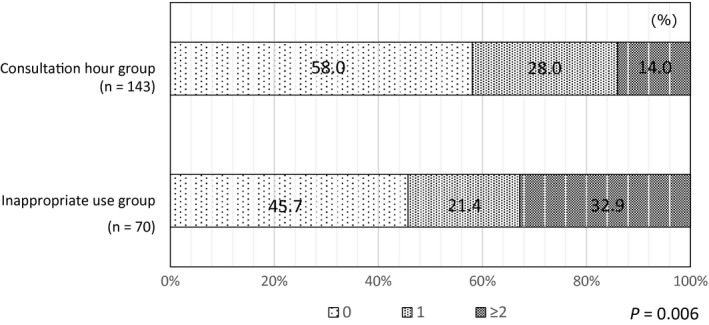
Number of out‐of‐hours emergency department visits in the past 3 y. The chi‐squared test was used to compare the three groups
2.5. Factors related to inappropriate use
We performed a multivariate analysis to identify factors related to inappropriate use. Logistic regression analysis was performed for inappropriate use, with independent variables of gender, age, presence of a primary care physician, duration since symptom onset (condensed to a two‐point scale, specifically “shorter than 1 day” and “1 day or more”), and reasons for consultation with P < 0.10 in the univariate analysis (“wanted a doctor's opinion,” “desire for treatment by a specialist”), and number of out‐of‐hours ED visits in the past 3 years. The JTAS triage level could not be adopted as an independent variable in multivariate analysis because there was only one JTAS triage Level 5 patient in the inappropriate use group. In the univariate analysis, there was a significant difference in the rate of laboratory testing between the two groups. However, the decision to perform laboratory testing was made by the same physicians who decided whether the visit was appropriate or not. Since both judgments were considered to be related, we did not adopt the presence or absence of laboratory testing as an independent variable in multivariate analysis. The correlation coefficient between variables was less than 0.4. Having two or more prior out‐of‐hours ED visits in the past 3 years was identified as a factor for inappropriate use (OR 3.19; 95% CI 1.22‐8.31) (reference: 0 visits). Duration since symptom onset of shorter than 1 day was correlated with inappropriate use (OR 5.35; 95% CI 2.58‐11.11) (reference: 1 day or more) (Table 3).
Table 3.
Factors associated with inappropriate use of the emergency department (n = 178)
| OR | 95% CI | P value | |
|---|---|---|---|
| Male gender | 1.32 | 0.63‐2.76 | 0.46 |
| Age (y) | 1.01 | 0.98‐1.03 | 0.71 |
| Has a primary care physician | 1.45 | 0.62‐3.41 | 0.39 |
| Duration since symptom onset | |||
| Shorter than 1 d | 5.35 | 2.58‐11.11 | <0.0001 |
| 1 d or more | Reference | ||
| Reason for consultation | |||
| Wanted a doctor's opinion | 0.23 | 0.05‐1.02 | 0.053 |
| Desire for treatment by a specialist | 0.52 | 0.24‐1.12 | 0.095 |
| Number of out‐of‐hours emergency department visits in the past 3 y | |||
| 0 | Reference | ||
| 1 | 0.96 | 0.39‐2.31 | 0.92 |
| ≥2 | 3.19 | 1.22‐8.31 | 0.018 |
The analysis was performed on a total of 178 subjects; 53 subjects were excluded due to insufficient data.
Abbreviations: CI, confidence interval; OR, odds ratio.
3. DISCUSSION
Our research identified characteristics and reasons associated with inappropriate out‐of‐hours use of EDs by patients with nonurgent conditions. Patients with two or more previous out‐of‐hours visits to the ED were more than three times as likely to inappropriately use out‐of‐hours emergency medical care. Research shows that many frequent users of emergency care are heavy users of primary care and other hospital services,19 which suggests the possibility that many cases of inappropriate use are by the same individuals. Instead of a broad, general effort to prevent inappropriate use, a campaign targeted at heavy users of medical services might be more effective.
Approximately 40% of patients in the inappropriate use group indicated “inability to take time off from school or work during the day” as a reason for their consultation, suggesting inappropriate ED use might be a matter of personal convenience. However, this was just a descriptive finding since the question was posed only to out‐of‐hours ED patients. In a study from Spain, “ease of emergency care use” was listed as a reason for consultation by 23.7% of patients,17 while a study from the United States reported that 31% of patients used emergency medical care because “appointments were not required.”20 In these countries, the rules and procedures for scheduling appointments during daytime hours might contribute to the use of emergency care as a matter of convenience. Owing to differences between systems and patient populations studied, a direct comparison is not possible. Although Japan has a healthcare system that emphasizes free access to daytime consultation, it is considered a serious problem that approximately 40% of patients who visited the ED outside of regular consultation hours did so for their personal convenience.
The most common reasons for ED consultation were “desire to be cured quickly,” “wanted a doctor's opinion,” “wanted to know whether the condition was serious,” and “condition was not improving.” In a previous study from Japan, “condition was not improving” was the most common reason for using emergency medical care.15 Furthermore, the three most common diagnoses for patients in the inappropriate use group, totaling 51.1%, were acute upper respiratory infection, acute gastroenteritis, and functional headaches. Even though such self‐limited conditions accounted for more than half of the patient visits in the inappropriate use group, 76.7% of patients indicated “wanted a prescription” as a reason for their consultation. Although the two groups did not differ in terms of diagnoses or reasons for consultation, duration since symptom onset of shorter than 1 day was correlated with inappropriate ED use. These results suggest that while some patients can wait until consultation hours to see doctors, others are unable to wait despite having only mild symptoms. This may be related to problems with the high frequency of inappropriate ED use in Japan. This is due not only to patient‐related factors but also to other issues as well. First, there is no restriction on hospital visits. Collecting additional copayment from patients without referrals is effective in suppressing consultations,21 but potential risks to patients must be considered. Next, physicians’ explanations about illnesses and preventive measures are insufficient, given that patients used the ED because they did not know the natural course of self‐limited conditions as described above. But it is a burden for physicians to provide complete information in the ED. It might be desirable for primary care physicians to regularly provide patients with explanations about the natural course of self‐limited conditions, self‐medication, and situations when a consultation is appropriate.
Our study results did not confirm a relationship between anxiety and/or depression and inappropriate out‐of‐hours ED use. The relationship between anxiety and depression and use of emergency medical care has been investigated in previous studies in other countries.4, 22 This may be due to factors such as the need for appointments and other limitations in those countries making it easier for patients with anxiety and/or depression to seek a quick consultation in the ED, whereas in Japan the system of free access allows patients to easily seek daytime consultations. The inappropriate use group may perceive differences between care during regular consultation hours and out‐of‐hours emergency care. Therefore, it might be important for the public to be informed of the differences between care during consultation hours and out‐of‐hours emergency medical care.
Regarding access to emergency and regional medical services, one study suggests that access to a primary care clinic helps prevent some inappropriate use of ambulance services.23 In our study, however, approximately 50% of patients in the inappropriate use group were aware of an out‐of‐hours primary care clinic provided by a municipal or local medical association. Our study also found that almost 70% of patients desire laboratory tests. When combined with the lack of such capabilities at many out‐of‐hours facilities, these patients might opt to visit an ED from the start.
Based on the judgment of physicians in charge of patient consultations, approximately 20% of study patients using out‐of‐hours EDs and who were triaged at levels 4 or 5 were in fact visiting appropriately. By removing them from the analysis, we believe we were able to more accurately evaluate the patients in the inappropriate use group.
Our study has several limitations. First, it involved a single facility, and the generalizability of results to other settings needs to be carefully considered. However, these results could apply to clinical settings responsible for regional emergency medical care. Next, this study was potentially underpowered to demonstrate differences in characteristics or reasons for consultation between the inappropriate use and consultation hour groups. Another limitation of this study was the large number of patients who were excluded due to staff workload. This raises the possibility that some characteristics of the inappropriate use group were not identified. Patients in the inappropriate use group had a shorter duration from symptom onset and higher urgency based on triage level than patients in the consultation hour group. Since a department of general medicine during consultation hours will generally differ from an out‐of‐hours ED in numerous ways, it is important to carefully interpret when results are applicable to each situation. We developed the questions on reasons for consultation based on prior studies and discussion among the authors, but there was insufficient validation. The number of each patient's previous visits was obtained from a self‐administered questionnaire, so recall bias may have been an issue. However, this information could not be obtained from their medical records at the hospital targeted for this survey since patients may have visited other hospitals as well.
Future studies with a larger sample size and greater variety of facilities, possibly with a designated researcher, are needed for a more detailed study.
4. CONCLUSION
Patients with two or more previous out‐of‐hours ED visits were more than three times as likely to use the ED compared to patients who had not visited the ED at all in the past 3 years.
CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Supporting information
ACKNOWLEDGEMENTS
This study was partially supported by grants from Tsukuba Medical Center Hospital.
Miyazawa A, Maeno T, Shaku F, et al. Inappropriate use of the emergency department for nonurgent conditions: Patient characteristics and associated factors at a Japanese hospital. J Gen Fam Med. 2019;20:146–153. 10.1002/jgf2.249
REFERENCES
- 1. Selby JV, Fireman BH, Swain BE. Effect of a copayment on use of the emergency department in a health maintenance organization. N Engl J Med. 1996;334(10):635–41. [DOI] [PubMed] [Google Scholar]
- 2. Lega F, Mengoni A. Why non‐urgent patients choose emergency over primary care services? Empirical evidence and managerial implications. Health Policy. 2008;88(2–3):326–38. [DOI] [PubMed] [Google Scholar]
- 3. Uscher‐Pines L, Pines J, Kellermann A, Gillen E, Mehrotra A. Deciding to Visit the Emergency Department for Non‐Urgent Conditions: a Systematic Review of the Literature. Am J Manag Care. 2013;19(1):47–59. [PMC free article] [PubMed] [Google Scholar]
- 4. Martin A, Martin C, Martin PB, Martin PA, Green G, Eldridge S. ‘Inappropriate’ attendance at an accident and emergency department by adults registered in local general practices: how is it related to their use of primary care? J Health Serv Res Policy. 2002;7(3):160–5. [DOI] [PubMed] [Google Scholar]
- 5. Northington WE, Brice JH, Zou B. Use of an emergency department by nonurgent patients. Am J Emerg Med. 2005;23(2):131–7. [DOI] [PubMed] [Google Scholar]
- 6. Afilalo J, Marinovich A, Afilalo M, Colacone A, Léger R, Unger B, et al. Nonurgent emergency department patient characteristics and barriers to primary care. Acad Emerg Med. 2004;11(12):1302–10. [DOI] [PubMed] [Google Scholar]
- 7. Gill JM, Riley AW. Nonurgent use of hospital emergency departments: urgency from the patient's perspective. J Fam Pract. 1996;42(5):491. [PubMed] [Google Scholar]
- 8. Doty MM, Holmgren AL. Health care disconnect: gaps in coverage and care for minority adults: findings from the commonwealth fund biennial health insurance survey (2005). Issue brief (Commonwealth Fund). 2006. [PubMed]
- 9. Campbell PAP. Emergency department use by family practice patients in an academic health center. Fam Med. 1998;30(4):272–75. [PubMed] [Google Scholar]
- 10. Han B, Wells BL. Inappropriate emergency department visits and use of the Health Care for the Homeless Program services by Homeless adults in the northeastern United States. J Public Health Manag Pract. 2003;9(6):530–7. [DOI] [PubMed] [Google Scholar]
- 11. Ueno Y, Kono M, Kizawa A, Kikuchi T, Sugegaya J, Atake S, Mashiko K. Evaluation of the quality of triage system by nurses at the emergency services. Nihon Kyukyu Igakukai Zasshi. 2009;20(3):116–25. (in Japanese) [Google Scholar]
- 12. Japanese Association for Acute Medicine, Japanese Association for Emergency Nursing, Japanese Society of Emergency Pediatrics, Japanese Society for Emergency Medicine . Japan Triage and Acuity Scale 2012 guidebook: Herusu Shuppan; 2012. (in Japanese)
- 13. Bullard MJ, Musgrave E, Warren D, Unger B, Skeldon T, Grierson R, et al. Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) Guidelines 2016. CJEM. 2017;19(S2):S18–S27. [DOI] [PubMed] [Google Scholar]
- 14. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–70. [DOI] [PubMed] [Google Scholar]
- 15. Kugaya A, Akechi T, Okuyama T, Okamura H, Uchitomi Y. Screening for Psychological Distress in Japanese Cancer Patients. Jpn J Clin Oncol. 1998;28(5):333–38. [DOI] [PubMed] [Google Scholar]
- 16. Sugai M, Tanaka Y, Mihara Y, Sasaki A, Meguro Y. Study about the reasonable visit of the secondary emergency room according to research on our visiting patients. Niigata‐ken Koseiren Med J. 2012;21(1):18–22. (in Japanese). [Google Scholar]
- 17. Sempere‐Selva T, Peiro S, Sendra‐Pina P, Martinez‐Espin C, Lopez‐Aguilera I. Inappropriate use of an accident and emergency department: magnitude, associated factors, and reasons–an approach with explicit criteria. Ann Emerg Med. 2001;37(6):568–79. [DOI] [PubMed] [Google Scholar]
- 18. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–9. [DOI] [PubMed] [Google Scholar]
- 19. Byrne M, Murphy AW, Plunkett PK, McGee HM, Murray A, Bury G. Frequent attenders to an emergency department: a study of primary health care use, medical profile, and psychosocial characteristics. Ann Emerg Med. 2003;41(3):309–18. [DOI] [PubMed] [Google Scholar]
- 20. Redstone PP. Nonurgent use of the emergency department. J Ambul Care Manag 2008;31(4):370–76. [DOI] [PubMed] [Google Scholar]
- 21. Inada H, Kobayashi Y, Tomida M, Ota N. Effect of Inceased Copayment on the Use of the Emergency Department at a Hospital. Iryo Keizai Kenkyu. 2012;23(2):95–106. [Google Scholar]
- 22. Backman AS, Blomqvist P, Svensson T, Adami J. Health care utilization following a non‐urgent visit in emergency department and primary care. Intern Emerg Med. 2010;5(6):539–46. [DOI] [PubMed] [Google Scholar]
- 23. Horibata K, Takemura Y. Inappropriate use of ambulance services by elderly patients with less urgent medical needs. Tohoku J Exp Med. 2015;235(2):89–95. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials