

The NIH is the federal steward of biomedical research in the United States. Taxpayers fund the NIH; the NIH supports research into the underlying biology, etiology, and treatment of diseases; and benefits of that research are returned to taxpayers. This is a large and complex enterprise, but at its core are two fundamental principles. The NIH is obligated to distribute its research grants and grant dollars in a fair and impartial manner among qualified investigators nationwide and to maximize the return on taxpayers’ investments.

The NIH should rethink how it doles out funding. Studies indicate that research output does not grow linearly with the amount of research project grant support—and that the greatest rates of return are achieved with intermediate levels of funding. Image credit: Dave Cutler (artist).
But to meet these obligations, the NIH must establish a better-balanced distribution of funding among institutions. Here, I describe why such changes are needed and propose a specific mechanism for how they could be implemented.
Diversity Matters
The director of the NIH, Francis Collins, has recognized that “the US biomedical research workforce does not currently mirror the nation’s population demographically” and that “recruiting and retaining a diverse set of minds and approaches is vital to harnessing the complete intellectual capital of the nation” (1). These systemic problems stem, in part, from unequal access to NIH grant support among investigators grouped by race (2), gender (3), age (4), institution (5), and state (6).
The differences in grant application success rates and award sizes among investigators grouped in various ways affect where the grant dollars go, leading to heavily skewed distributions of funding. For example, less than one in three applicants get any of their NIH research project grant applications funded over a five-year period (7), and among successful applicants, a small minority are strongly favored. Just 1% of awardees get about 11% of all grant dollars, and 10% of awardees get about 40% of the dollars (8). Large differences in success rates and award sizes between states, whose impacts on amounts of funding are multiplicative, contribute to a greater than 100-fold range in their research project grant funding per capita (6). The 10 top-funded states receive, on average, about 19 times more funding per capita than the bottom 10. Taxpayers in three quartiles of states are subsidizing research in one quartile of states. The amount of this subsidy (i.e., diverted funds that could otherwise be invested productively in their states of origin) is about $4 billion per year (6). Such disparities have persisted for decades despite congressionally supported NIH programs intended to promote the ability of investigators and institutions across the country to compete on equal footing for grant funding, as measured by parameters such as grant application success rates and aggregate funding (9).
An underappreciated consequence of chronic, state-level differences in the access to NIH research project grant funding is that they affect local research infrastructure (e.g., bricks and mortar, administrative support, core facilities, constellation of funded investigators, training programs) that is required for researchers to do their jobs efficiently. Therein lies a vicious cycle: Researchers in disadvantaged states have a lower likelihood of getting funded. And when they do secure funding, they get less money per award, which adversely affects local infrastructure (relative to that of well-funded states). And this, in turn, makes it even harder for them to compete successfully for funding. Moreover, the interstate disparities in NIH funding to investigators (and associated differences in infrastructure) contribute to the geographical disenfranchisement of students and trainees. When we consider how to address current inequities in funding, we must also consider ways to address the legacy of unbalanced allocations made in the past.
The Elephant in the Room
The NIH’s deputy director for extramural research, Michael Lauer, recently emphasized that the “NIH makes awards to institutions, not people” (10). This has to do with rules for all federal awards and the designation of an institution or organization as the responsible recipient. For NIH funding, such requirements “are intended to ensure fairness, equity, fiscal stewardship, and other protections in activities that receive NIH support” (10). Be that as it may, the fact that awards are made to institutions (not people or states) forces us to consider institutions as the fundamental units among which NIH funding is allocated. Inspection of data in the NIH RePORTER database, which is available to the public, reveals that the allocations of funding are profoundly skewed, favoring a tiny minority of institutions and disfavoring the vast majority. For example, just 2% of NIH-supported institutions get about 53% of all research project grant dollars, and the 10 top-funded institutions each get more dollars than do each of 35 to 40 entire states.
The implications are striking. Heavily skewed allocations of funding among institutions are an underlying cause of, and an impediment to rectifying, inequities in funding among states. This helps to explain why long-standing, congressionally supported NIH programs intended to improve access to funding among states (i.e., nationwide) have been ineffective (9). If the NIH is truly interested in “harnessing the complete intellectual capital of the nation” (1), it would have to reduce the vast disparities in funding to institutions. Factors such as scientific output per dollar of NIH grant funding, described below, support this assessment.
The Matthew Effect
There are clear reasons for the heavily skewed allocations of research dollars among institutions. Proximate causes include large differences in grant application success rates, funding rates (the percentage of applicants who get funded in a given fiscal year), and mean award sizes (5). In each case, these differences favor prestigious institutions over lower-profile institutions. Interestingly, top-ranked, favored institutions provide a lower return on taxpayers’ investments, as measured by the number of scientific publications and their aggregate relative citation ratios per dollar of research project grant funding (i.e., scientific productivity) (5).
In other words, the impacts of annual differences in the likelihood of securing funding and of award sizes between institutions compound over time, which reinforces the monopolization of resources by favored institutions.
The differences in success rates, funding rates, and award sizes among institutions are discordant with their productivity-based value to the national research enterprise, raising questions about impartiality of the funding process.
Favored institutions get more dollars per principal investigator (i.e., laboratory head), which supports larger laboratories. This has surprising impacts on the amount and nature of scientific output. First, although output increases with increasing lab size, it does not scale proportionately (11–13). Second, articles from smaller labs tend to be more innovative and succeed in terms of influence further into the future than those of larger labs, which tend to develop existing ideas (14). There is high value for research conducted by smaller laboratories and less-well-funded institutions, challenging the notion that bigger is better. Each type of research is arguably important, but one type is winning out at the expense of the other.
The practice of favoring already well-funded institutions with higher grant application success rates and larger award sizes, despite their lower productivity (Fig. 1), is a clear example of the Matthew effect in action (“the rich get richer”) (15, 16). As one might expect under the Matthew effect, this funding inequality has been growing for at least three decades with a small segment of institutions getting an increasing proportion of funds (17). In other words, the impacts of annual differences in the likelihood of securing funding and of award sizes between institutions compound over time, which reinforces the monopolization of resources by favored institutions. The same amplification process has been documented for unbalanced allocations of funding to institutions by Canada’s Natural Sciences and Engineering Research Council, along with projections that such imbalances, left unchecked, will decimate funding to the disfavored institutions (18).
Fig. 1.
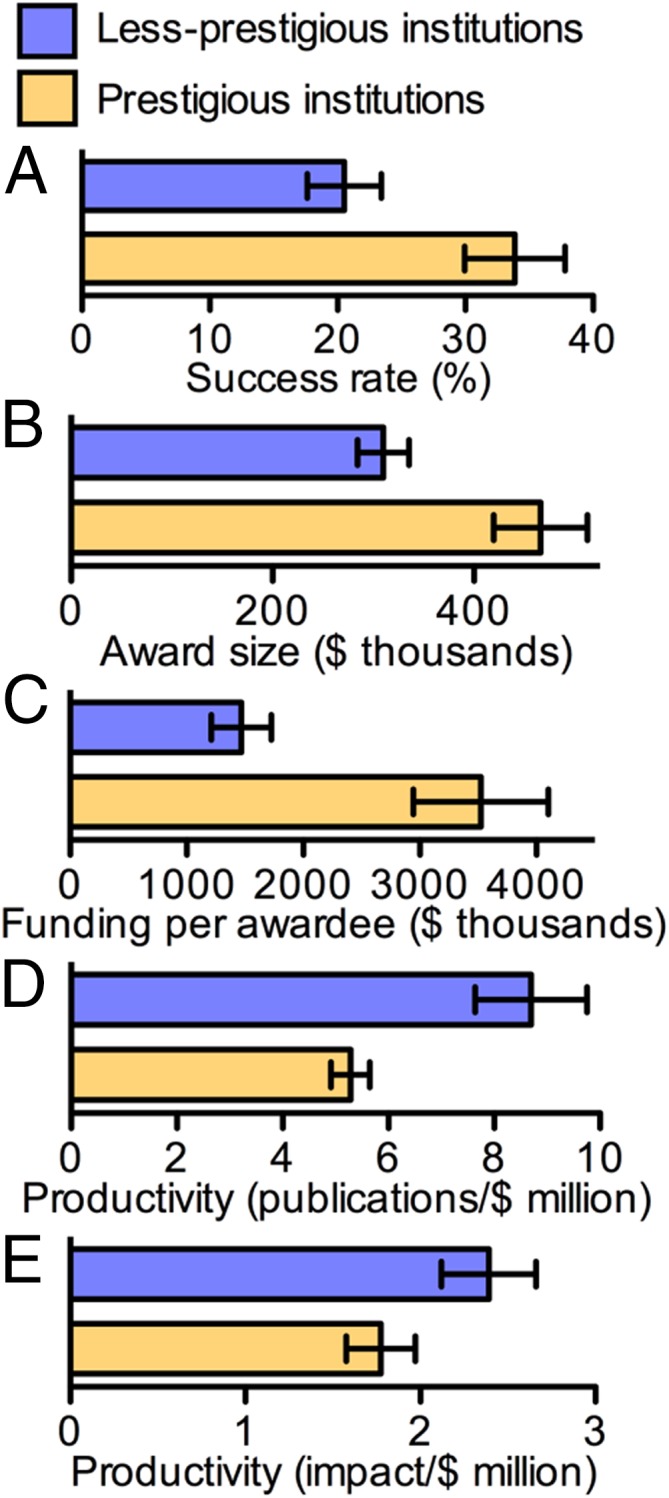
Nature of the problem. The NIH favors some institutions with higher grant application success rates (A), larger award sizes (B), and more dollars per awardee (C). This occurs even though disfavored institutions provide greater returns on taxpayers’ investments (D and E). Data are for NIH research project grants 2006–2015 (mean with 95% confidence interval); returns are the total number of grant-supported publications (D) and log-transformed Relative Citation Ratios (impact) of research publications (E), each normalized to total funding. Prestigious institutions: Harvard Medical School; Stanford University; Johns Hopkins University; University of California, San Francisco; University of Pennsylvania. Less-prestigious institutions: Indiana University-Purdue University at Indianapolis, University of Nebraska Medical Center, University of Oklahoma Health Sciences Center, West Virginia University, University of South Dakota, Eastern Virginia Medical School, State University of New York at Buffalo, University of Mississippi Medical Center, University of North Dakota, Louisiana State University Health Sciences Center Shreveport. See ref. 5 for additional information on how institutions were selected, the experimental approach, and primary data.
Diminishing Marginal Returns
When a principal investigator’s grant funding amount exceeds his or her capacity to carry out grant-related duties, such as the day-to-day management of laboratory personnel, productivity falls (19, 20). Such diminishing marginal returns apply at the population scale for dollars per award and dollars per investigator (21–24). They apply when award data are parsed by NIH institute, for “elite” investigators, and by human versus nonhuman model systems (12, 24, 25). They apply for unbalanced allocations of NIH funding to investigators grouped by institution and by state (5, 6). They also apply globally for research support from other funding agencies and in different nations (11, 13, 26, 27).
The costs of such diminishing marginal returns are arguably greatest where disparities in funding are greatest—which for NIH grant dollars occurs at the level of institutions. Because the NIH gives about 53% of all research project grant dollars to just 2% of supported institutions (the very well-funded ones) and very well-funded institutions tend to be considerably less productive than more modestly funded institutions (Fig. 1) (5), the heavily skewed allocations of funding to institutions have substantive implications for the efficiency with which precious, taxpayer-derived research dollars are being expended.
The NIH has a fiduciary obligation to maximize the return on taxpayers’ investments and, for reasons described above, this responsibility is tied intimately and mechanistically to another fiduciary obligation, which is to provide qualified investigators throughout the nation equal access to grants and grant dollars. Shortfalls in meeting these two obligations can thus be addressed simultaneously.
Indirect approaches to reduce disparities in allocations of funding are demonstrably ineffective (6, 9). More direct approaches, such as capping the number of research dollars that each investigator can receive, would increase substantially the diversity and productivity of the research enterprise and—in the opinion of thousands of concerned individuals—should be implemented (19, 20). However, such caps would, by definition, be applied only to investigators at the top end of the funding distribution, without any direct intervention for disparities in allocations of funding below the cap—or among entities such as institutions.
To most effectively reduce disparities among institutions and to do so in a systematic way, the NIH would have to address their underlying causes, which are wide gaps in grant application success rates and award sizes. In addition to reducing disparity, this approach would address correspondingly the impacts of diminishing marginal returns on net productivity of the research enterprise.
A Mechanism for Remediation
Because disparities in funding and diminishing marginal returns are coupled mechanistically, one can approach the problem from a different angle. I, therefore, propose a novel, straightforward, impartial mechanism to address the diminishing marginal returns caused by unbalanced allocations of funding.
The SR/P value, which is success rate divided by productivity, is a population-level metric that can be applied for investigators grouped in any way desired, such as by race, gender, age, institution, or state. It can be calculated by using any measure of productivity desired, such as the number of publications or net citation impact per dollar of funding. Differences in SR/P values provide an aggregate measure for the success rate–normalized, funding amount–normalized, scientific output–normalized magnitude of disparity.
For example, there is about a 2.4-fold difference in SR/P values between the groups of institutions shown in Fig. 1. Importantly, such differences encompass the impacts of diminishing marginal returns on scientific output (productivity) as well as controllable factors (differences in success rates and award sizes) that contribute to the diminishing marginal returns. Therefore, SR/P values provide a way to address, in proportion to their magnitude, the diminishing marginal returns.
To do so, the NIH would adjust success rates and award sizes of institutions to the extent necessary to achieve parity or near parity of their SR/P values. Success rates and award sizes could still vary among institutions, according to their productivity-based merit, up to but not exceeding the point at which their SR/P values depart from the target range. This mechanism would allow institutions at-large to compete on a more equal footing for grant support, would accommodate (and reward) the possibility that some institutions are of greater value to the research enterprise than others, and would maximize the return on taxpayers’ investments. The approach is of broad utility for investigators grouped in other ways, such as by state.
Under this proposed mechanism, there would be no changes in the peer review process, and grant applications still would be evaluated on the basis of their scientific merit. Paylines would be adjusted (wide gaps in success rates closed) for investigators stratified by institution, which the NIH is already doing for investigators stratified by age. The main difference is that the proposed mechanism (or variants thereof) would treat underlying causes of diminishing marginal returns in proportion to the magnitude of such marginal returns, thereby addressing systematically the inefficiencies caused by heavily skewed allocations of funding. Two senior NIH officials expressed interest in the utility of this mechanism, descriptions of which were forwarded to NIH data analysists for further evaluation. It seems reasonable to expect that the NIH will, in due course, make their findings available to the public.
Additional benefits of a better-balanced distribution of funding among institutions are like those described previously, including by senior NIH officials, for allocations of funding among investigators at-large (13, 19, 20, 24). Dollars that are currently being used inefficiently at the top of the funding distribution would be freed up for allocation elsewhere. The NIH would be able to support a greater number of investigators, would maximize the diversity of perspectives and tools that are harnessed, and would increase the likelihood of scientific breakthroughs. There would be less geographical disenfranchisement of students and trainees, improving the ability of the NIH to foster, support, and ultimately harness the talents of next-generation researchers.
In summary, a more egalitarian distribution of NIH grants and grant dollars among institutions would yield greater collective gains for the research enterprise and the taxpayers who support it. It is also a necessary step toward the NIH’s long-standing, congressionally supported, yet, thus far, lackluster commitment to reduce the vast disparities in funding to states. Because diminishing marginal returns on research funding apply globally, the problems and solutions defined here are likely germane to research grant support from other funding agencies worldwide.
Footnotes
The authors declare no conflict of interest.
Any opinions, findings, conclusions, or recommendations expressed in this work are those of the authors and have not been endorsed by the National Academy of Sciences.
References
- 1.Valantine H. A., Collins F. S., National Institutes of Health addresses the science of diversity. Proc. Natl. Acad. Sci. U.S.A. 112, 12240–12242 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ginther D. K., et al. , Race, ethnicity, and NIH research awards. Science 333, 1015–1019 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pohlhaus J. R., Jiang H., Wagner R. M., Schaffer W. T., Pinn V. W., Sex differences in application, success, and funding rates for NIH extramural programs. Acad. Med. 86, 759–767 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Levitt M., Levitt J. M., Future of fundamental discovery in US biomedical research. Proc. Natl. Acad. Sci. U.S.A. 114, 6498–6503 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wahls W. P., High cost of bias: Diminishing marginal returns on NIH grant funding to institutions. bioRxiv:10.1101/367847 (1 January 2018).
- 6.Wahls W. P., Biases in grant proposal success rates, funding rates and award sizes affect the geographical distribution of funding for biomedical research. PeerJ 4, e1917 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lauer M., How many researchers? Open Mike, NIH Extramural Nexus, 31 May 2016. https://nexus.od.nih.gov/all/2016/05/31/how-many-researchers/. Accessed 29 May 2019.
- 8.Collins F. S., New NIH approach to grant funding aimed at optimizing stewardship of taxpayer dollars. The NIH Director, 2 May 2017. https://www.nih.gov/about-nih/who-we-are/nih-director/statements/new-nih-approach-grant-funding-aimed-optimizing-stewardship-taxpayer-dollars. Accessed 29 May 2019.
- 9.National Academies of Science, Engineering, and Medicine , The Experimental Program to Stimulate Competitive Research (National Academies Press, Washington, DC, 2013). [PubMed]
- 10.Lauer M., Wait...it's not MY grant? Open Mike, NIH Extramural Nexus, 29 May 2018. https://nexus.od.nih.gov/all/2018/05/29/waitits-not-my-grant/. Accessed 29 May 2019.
- 11.Cook I., Grange S., Eyre-Walker A., Research groups: How big should they be? PeerJ 3, e989 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lauer M., Roychowdhury D., Patel K. C., Walsh R., Pearson K., Marginal returns and levels of research grant suport among scientists supported by the National Institutes of Health. bioRxiv:10.1101/142554 (1 January 2017).
- 13.Mongeon P., Brodeur C., Beaudry C., Lariviere V., Concentration of research funding leads to decreasing marginal returns. Res. Eval. 25, 396–404 (2016). [Google Scholar]
- 14.Wu L., Wang D., Evans J. A., Large teams develop and small teams disrupt science and technology. Nature 566, 378–382 (2019). [DOI] [PubMed] [Google Scholar]
- 15.Merton R. K., The Matthew Effect in science: The reward and communication systems of science are considered. Science 159, 56–63 (1968). [PubMed] [Google Scholar]
- 16.Perc M., The Matthew effect in empirical data. J. R. Soc. Interface 11, 20140378 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Katz Y., Matter U. B., On the biomedical elite: Inequality and stasis in scientific knowledge production. DASH, 11 July 2017. https://cyber.harvard.edu/publications/2017/07/biomedicalelite. Accessed 29 May 2019.
- 18.Murray D. L., et al. , Bias in research grant evaluation has dire consequences for small universities. PLoS One 11, e0155876 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Peifer M., The argument for diversifying the NIH grant portfolio. Mol. Biol. Cell 28, 2935–2940 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wahls W. P., The NIH must reduce disparities in funding to maximize its return on investments from taxpayers. eLife 7, e34965 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Basson J., Lorsch J., Dorsey T., Revisiting the dependence of scientific productivity and impact on funding level. NIGMS Feedback Loop Blog, 8 July 2016. https://loop.nigms.nih.gov/2016/07/revisiting-the-dependence-of-scientific-productivity-and-impact-on-funding-level/. Accessed 29 May 2019.
- 22.Lauer M., Applying the relative citation ratio as a measure of grant productivity. Open Mike, NIH Extramural Nexus, 21 October 2016. https://nexus.od.nih.gov/all/2016/10/21/applying-the-relative-citation-ratio-as-a-measure-of-grant-productivity/. Accessed 29 May 2019.
- 23.Lauer M., Citations per dollar as a measure of productivity. Open Mike, NIH Extramural Nexus, 28 April 2016. https://nexus.od.nih.gov/all/2016/04/28/citations-per-dollar/. Accessed 29 May 2019.
- 24.Lorsch J. R., Maximizing the return on taxpayers’ investments in fundamental biomedical research. Mol. Biol. Cell 26, 1578–1582 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Doyle J. M., et al. , Association of percentile ranking with citation impact and productivity in a large cohort of de novo NIMH-funded R01 grants. Mol. Psychiatry 20, 1030–1036 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schmoch U., Schubert T., Sustainability of incentives for excellent research—The German case. Scientometrics 81, 195–218 (2009). [Google Scholar]
- 27.Fortin J. M., Currie D. J., Big science vs. little science: How scientific impact scales with funding. PLoS One 8, e65263 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]