

Abstract
Background:
Migraine is a common cause of primary headache, with women being affected thrice as common as men. Very few studies are available on sexual dysfunction in female migraineurs. There are no published studies done on the same in India till now. This study was done to look for the prevalence and predictors of sexual dysfunction disorder in females suffering from migraine.
Materials and Methods:
This is a cross-sectional study done to look for the prevalence and predictors of female sexual dysfunction in migraine. Sixty female patients with migraine were studied. The International Headache Society's International Classification of Headache Disorders, 3rd Edition, was followed to diagnose migraine with or without aura. Migraine disability assessment scale was used to assess migraine-related disability, and Female Sexual Function Index (FSFI) score was used to assess female sexual function.
Results:
Sexual dysfunction was found in 78.3% migraineurs. The mean FSFI score was 23.1 ± 4.76. The FSFI scores in all the domains were lower in the individuals studied. Acute headaches resulted in loss of sexual desire among all the migraineurs.
Conclusion:
Sexual dysfunction is common in migraine with all domains of sexual function being affected. There is a significant negative correlation of sexual function with duration of acute episodes of headache and increasing frequency of migraine attacks per month.
Keywords: Female sexual dysfunction, headache, migraine, migraine disability
INTRODUCTION
Headache is a common complaint for which individuals seek medical help. Migraine is a common cause of primary headache and is more prevalent in females. The global burden of disease 2000[1] estimated global all-age prevalence of migraine at 14.7%. The average duration of migraine was lower in developed countries where effective treatment was available to a proportion of sufferers. The percent of time symptomatic of migraine ranged from 2.3% in developed countries to 9.2% in low-income countries. Worldwide, migraine is the 9th most common cause of years lost due to disability.[1]
Migraine in females gives rise to various psychosocial issues including sexual dysfunction. The etiopathogenesis of this is still debatable. There are very few studies which have looked for the presence and causes of sexual dysfunction in women with migraine. Sexual dysfunction is characterized by disturbance in various domains of sexual function as illustrated in Female Sexual Function Index (FSFI).[2] This study was undertaken to look for the prevalence and predictors of female sexual dysfunction in migraine.
MATERIALS AND METHODS
This cross-sectional study was carried out in the Department of Neurology, JSS hospital, which is a tertiary care hospital situated in Mysore, a city in the southern part of India. Sixty female patients with migraine were studied. The International Headache Society's International Classification of Headache Disorders, 3rd Edition, was followed to diagnose migraine with or without aura.[3]
Females of age 18–40 years with migraine and in active sexual relationship were included. Females with diabetes, hypertension or any other medical condition or taking drugs that would result in sexual dysfunction were excluded. Written informed consent was obtained from the study participants.
A structured questionnaire was used to collect the data regarding sociodemographic characteristics such as patient's age, educational status, occupation, and marital status. Headache characteristics including duration of migraine, duration of acute attacks of headache, frequency, and severity were assessed. Migraine disability assessment scale (MIDAS) was used to assess migraine-related disability.[4] The MIDAS is a brief, self-administered questionnaire designed to quantify migraine-related disability over a 3-month period. The FSFI[2] is a multidimensional self-report instrument used to assess the various dimensions of sexual function in women during the past 4 weeks. The FSFI is a 19-item questionnaire in which each item is scored on a scale of 0 (or 1) to 5. Higher scores indicate better sexual function. The cutoff values for various domains to say as dysfunction are desire <4.28, arousal <5.08, lubrication <5.45, orgasm <5.05, satisfaction <5.04, pain <5.51, and total score ≤26.55. Statistical analysis was performed using the IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp. Descriptive statistics were used to summarize all measurements. For two group comparisons, ANOVA and unpaired t-test were used. Spearman correlation test was used for correlation analysis. The level of statistical significance was set as P < 0.05.
RESULTS
All the study participants were married. The mean age of the participants was 33.53 ± 6.08 years. About 90% of the individuals had migraine without aura. The mean migraine duration was 3.89 ± 3.78 years [Table 1]. The mean duration of each headache episode was 22.6 ± 20.56 h, with frequency of 6.18 ± 3.65 per month. In a month, they had headache for 7.58 ± 3.65 days. The mean MIDAS was 7.58 ± 10.94, and 90% had moderate to severe disability. The mean FSFI scores were 23.1 ± 4.76 [Table 2], with lower scores seen in all domains of sexual function [Figure 1]. All the participants reported avoiding sex during acute episodes of headache. Migraineurs with higher frequency of headaches and higher migraine days per month had more sexual dysfunction [Table 3]. Although FSFI score was least in those with severe disability/Grade IV MIDAS score [Table 4], there was no statistically significant difference of FSFI score among different grades of MIDAS severity. There was a statistically significant negative correlation between duration of acute episode of headache and sexual desire [Table 5].
Table 1.
Characteristics of the study participants
| Mean±SD | |
|---|---|
| Age (years) | 33.53±6.08 |
| Migraine duration (years) | 3.89±3.78 |
| Duration of acute episode of headache (h) | 22.6±20.56 |
| Frequency/month | 6.18±3.65 |
| Migraine days | 7.58±3.65 |
| MIDAS | 23.8±10.94 |
| MIDAS: Grade I (n=2) | 4±1.41 |
| MIDAS: Grade II (n=4) | 9.5±1 |
| MIDAS: Grade III (n=20) | 15.05±2.37 |
| MIDAS: Grade IV (n=34) | 31.64±7.55 |
SD=Standard deviation, MIDAS=Migraine disability assessment scale
Table 2.
Female Sexual Function Index scores of the study participants
| FSFI | Participants (n=60), mean±SD |
|---|---|
| Desire | 3.25±1.05 |
| Arousal | 3.55±1.21 |
| Lubrication | 4.34±1.05 |
| Orgasm | 4.06±1.14 |
| Satisfaction | 3.74±1.34 |
| Pain | 4.14±1.27 |
| Total | 23.1±4.76 |
FSFI=Female Sexual Function Index, SD=Standard deviation
Figure 1.
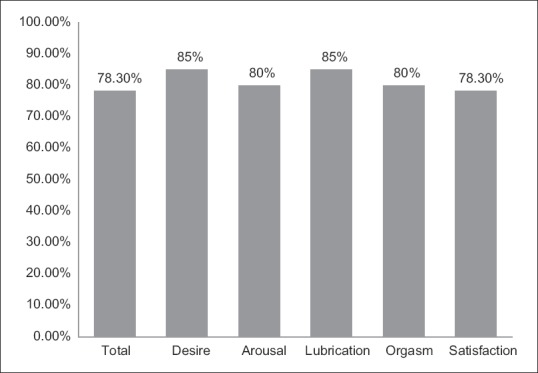
Prevalence of female sexual dysfunction and subscales of sexual dysfunction
Table 3.
Comparison of characteristics between two subgroups of migraine patients with or without female sexual dysfunction
| Sexual dysfunction | Mean±SD | P | |
|---|---|---|---|
| Present (78.33%) | Absent (21.67%) | ||
| Headache duration (years) | 4.07±8.87 | 2.75±3.92 | 0.345 |
| Duration of each migraine headache (h) | 24.19±21.97 | 16.85±13.52 | 0.249 |
| Frequency/month | 6.62±3.83 | 4.62±2.43 | 0.033 |
| Migraine days/month | 8.36±5.93 | 4.77±2.31 | 0.008* |
| MIDAS | 24.34±11.42 | 21.46±9.72 | 0.272 |
*Statistically significant P value. SD=Standard deviation, MIDAS=Migraine disability assessment scale
Table 4.
Comparison of Female Sexual Function Index domains with severity of migraine disability assessment scale grade
| FSFI | Mean±SD | P | |||
|---|---|---|---|---|---|
| Grade I (n=2) | Grade II (n=4) | Grade III (n=20) | Grade IV (n=34) | ||
| Desire | 4.5±1.27 | 3.15±0.75 | 3.42±1.01 | 3.08±1.08 | 0.25 |
| Arousal | 4.50±1.69 | 3.6±0.005 | 3.72±1.39 | 3.39±1.17 | 0.55 |
| Lubrication | 4.95±1.06 | 4.65±0.93 | 4.54±0.91 | 4.15±1.07 | 0.39 |
| Orgasm | 5.2±1.13 | 3.6±1.17 | 4.34±1.25 | 3.89±1.06 | 0.21 |
| Satisfaction | 5.4±0.84 | 3.9±1.14 | 4.08±1.41 | 3.43±1.29 | 0.1 |
| Pain | 4.00±1.13 | 4.6±1.64 | 4.02±1.48 | 4.16±1.15 | 0.87 |
| Total | 28.55±7.14 | 23.50±1.89 | 24.12±4.69 | 22.13±4.82 | 0.18 |
SD=Standard deviation, FSFI=Female Sexual Function Index
Table 5.
Correlation of various Female Sexual Function Index domains with migraine duration, duration of acute episode of headache, migraine frequency, and migraine disability assessment scale score
| Total | Desire | Arousal | Lubrication | Orgasm | Satisfaction | Pain | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r | P | r | P | r | P | r | P | r | P | r | P | r | P | |
| Migraine duration (years) | −0.13 | 0.32 | −0.11 | 0.43 | −0.20 | 0.11 | −0.08 | 0.53 | −0.06 | 0.63 | −0.13 | 0.30 | 0.056 | 0.66 |
| Duration of acute episode of headache (h) | −0.24 | 0.06 | −0.27 | 0.034* | −0.22 | 0.07 | −0.18 | 0.15 | −0.23 | 0.07 | −0.18 | 0.15 | 0.10 | 0.43 |
| Migraine frequency per month | −0.18 | 0.17 | −0.16 | 0.22 | −0.16 | 0.20 | −0.08 | 0.52 | −0.09 | 0.49 | −0.17 | 0.18 | −0.046 | 0.72 |
| MIDAS score | −0.22 | 0.09 | −0.16 | 0.20 | −0.14 | 0.28 | −0.18 | 0.15 | −0.15 | 0.22 | −0.30 | 0.01* | 0.06 | 0.61 |
*Statistically significant P value. MIDAS=Migraine disability assessment scale
DISCUSSION
Sexual health is a state of physical, emotional, mental, and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction, or infirmity.[5] Female sexual dysfunction is a multicausal and multidimensional problem. Female sexual dysfunction includes disorders of sexual desire, arousal, orgasmic, and sex pain.[6] In our study, 78.3% of the participants with migraine had sexual dysfunction. This is similar to many other studies done worldwide where the prevalence of female sexual dysfunction varied from 68%–90%.[7,8,9,10] We found in our study that all aspects of sexual health including desire, arousal, lubrication, orgasm, and satisfaction were affected in female migraineurs, which was similar to many other previous studies.[7,8,9,10] Houle et al.[11] did not find any correlation of headache intensity and average duration with sexual desire. In contrast, in our study, the duration of each episode had an effect on sexual functioning. Eraslan et al.[9] found no correlation of sexual dysfunction with MIDAS score or frequency of attacks whereas in our study, frequency of headache did affect sexual function. Sexual response is a complex process which involves hormonal, social, psychological, and neurovascular processes.[12,13,14] During acute migraine headache, there is hypersensitivity to various environmental stimuli. Negative experiences either emotional or physical lead to decreased sexual desire and inability to be sexually responsive.[15] Some studies have reported decreased sexual desire and arousal with chronic headache and migraine medication.[16,17,18,19,20,21] Alteration of sexual desire, arousal, and orgasm along with changes in pain threshold are some of the postulated causes of sexual dysfunction in migraineurs.[22,23,24] Many of the migraine prophylactic drugs including antiepileptic agents, betablockers, and analgesics can alter the balance of neurotransmitters and neuromodulators which play a role in central and peripheral sexual responses.[25] In our study, pain and hypersensitivity were the main factors responsible for female sexual dysfunction.
CONCLUSION
Sexual dysfunction is more common in migraine. All domains of sexual function are affected. There is a significant negative correlation of sexual function with duration of acute episodes of headache and increasing frequency of migraine attacks per month. Sexual dysfunction was not related to the severity of MIDAS score. Since migraine and sexual dysfunction affect the relationship of the migraineurs and their partners, care should be taken to identify and address this issue.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organisation methods and data sources for global burden of disease estimates 2000-2011. [Last accessed on 2019 Jan 11]. Available from: https://www.who.int/healthinfo/statistics/GlobalDALYmethods_2000_2011.pdf .
- 2.Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, et al. The female sexual function index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26:191–208. doi: 10.1080/009262300278597. [DOI] [PubMed] [Google Scholar]
- 3.Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition (beta version) Cephalalgia. 2013;33:629–808. doi: 10.1177/0333102413485658. [DOI] [PubMed] [Google Scholar]
- 4.Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the migraine disability assessment (MIDAS) questionnaire to assess headache-related disability. Neurology. 2001;56:S20–8. doi: 10.1212/wnl.56.suppl_1.s20. [DOI] [PubMed] [Google Scholar]
- 5.World Health Organization. Defining Sexual Health. Report of a Technical Consultation on Sexual Health. Geneva: World Health Organization; 2002. [Last accessed on 2019 Jan 11]. Available from: http://www.who.int/reproductivehealth/topics/gender_rights/defining_sexual_health.pdf . [Google Scholar]
- 6.Basson R, Berman J, Burnett A, Derogatis L, Ferguson D, Fourcroy J, et al. Report of the international consensus development conference on female sexual dysfunction: Definitions and classifications. J Urol. 2000;163:888–93. [PubMed] [Google Scholar]
- 7.Bestepe E, Cabalar M, Kucukgoncu S, Calıkusu C, Ornek F, Yayla V, et al. Sexual dysfunction in women with migraine versus tension-type headaches: A comparative study. Int J Impot Res. 2011;23:122–7. doi: 10.1038/ijir.2011.16. [DOI] [PubMed] [Google Scholar]
- 8.Ghajarzadeh M, Jalilian R, Togha M, Azimi A, Hosseini P, Babaei N, et al. Depression, poor sleep, and sexual dysfunction in migraineurs women. Int J Prev Med. 2014;5:1113–8. [PMC free article] [PubMed] [Google Scholar]
- 9.Eraslan D, Yalınay Dikmen P, Ilgaz Aydınlar E, Incesu C. The relation of sexual function to migraine-related disability, depression and anxiety in patients with migraine. J Headache Pain. 2014;15:32. doi: 10.1186/1129-2377-15-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Abdollahi M, Toghae M, Raisi F, Saffari E. The prevalence of female sexual dysfunction among migraine patients. Iran J Neurol. 2015;14:8–11. [PMC free article] [PubMed] [Google Scholar]
- 11.Houle TT, Dhingra LK, Remble TA, Rokicki LA, Penzien DB. Not tonight, I have a headache? Headache. 2006;46:983–90. doi: 10.1111/j.1526-4610.2006.00470.x. [DOI] [PubMed] [Google Scholar]
- 12.Salonia A, Munarriz RM, Naspro R, Nappi RE, Briganti A, Chionna R, et al. Women's sexual dysfunction: A pathophysiological review. BJU Int. 2004;93:1156–64. doi: 10.1111/j.1464-410X.2004.04796.x. [DOI] [PubMed] [Google Scholar]
- 13.Davis SR, Guay AT, Shifren JL, Mazer NA. Endocrine aspects of female sexual dysfunction. J Sex Med. 2004;1:82–6. doi: 10.1111/j.1743-6109.2004.10112.x. [DOI] [PubMed] [Google Scholar]
- 14.Berman JR, Bassuk J. Physiology and pathophysiology of female sexual function and dysfunction. World J Urol. 2002;20:111–8. doi: 10.1007/s00345-002-0281-4. [DOI] [PubMed] [Google Scholar]
- 15.Basson R. Female sexual response: The role of drugs in the management of sexual dysfunction. Obstet Gynecol. 2001;98:350–3. doi: 10.1016/s0029-7844(01)01452-1. [DOI] [PubMed] [Google Scholar]
- 16.Kwan KS, Roberts LJ, Swalm DM. Sexual dysfunction and chronic pain: The role of psychological variables and impact on quality of life. Eur J Pain. 2005;9:43–52. doi: 10.1016/j.ejpain.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 17.Orentreich N, Brind JL, Rizer RL, Vogelman JH. Age changes and sex differences in serum dehydroepiandrosterone sulfate concentrations throughout adulthood. J Clin Endocrinol Metab. 1984;59:551–5. doi: 10.1210/jcem-59-3-551. [DOI] [PubMed] [Google Scholar]
- 18.Rotter JI, Wong FL, Lifrak ET, Parker LN. A genetic component to the variation of dehydroepiandrosterone sulfate. Metabolism. 1985;34:731–6. doi: 10.1016/0026-0495(85)90023-x. [DOI] [PubMed] [Google Scholar]
- 19.Davis AR, Castaño PM. Oral contraceptives and libido in women. Annu Rev Sex Res. 2004;15:297–320. [PubMed] [Google Scholar]
- 20.Stimmel GL, Gutierrez MA. Sexual dysfunction and psychotropic medications. CNS Spectr. 2006;11:24–30. doi: 10.1017/s1092852900026730. [DOI] [PubMed] [Google Scholar]
- 21.Montejo-González AL, Llorca G, Izquierdo JA, Ledesma A, Bousoño M, Calcedo A, et al. SSRI-induced sexual dysfunction: Fluoxetine, paroxetine, sertraline, and fluvoxamine in a prospective, multicenter, and descriptive clinical study of 344 patients. J Sex Marital Ther. 1997;23:176–94. doi: 10.1080/00926239708403923. [DOI] [PubMed] [Google Scholar]
- 22.Gori S, Morelli N, Maestri M, Fabbrini M, Bonanni E, Murri L, et al. Sleep quality, chronotypes and preferential timing of attacks in migraine without aura. J Headache Pain. 2005;6:258–60. doi: 10.1007/s10194-005-0201-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Peres MF, Zukerman E, Young WB, Silberstein SD. Fatigue in chronic migraine patients. Cephalalgia. 2002;22:720–4. doi: 10.1046/j.1468-2982.2002.00426.x. [DOI] [PubMed] [Google Scholar]
- 24.Ambler N, Williams AC, Hill P, Gunary R, Cratchley G. Sexual difficulties of chronic pain patients. Clin J Pain. 2001;17:138–45. doi: 10.1097/00002508-200106000-00006. [DOI] [PubMed] [Google Scholar]
- 25.Basson R, Schultz WW. Sexual sequelae of general medical disorders. Lancet. 2007;369:409–24. doi: 10.1016/S0140-6736(07)60197-4. [DOI] [PubMed] [Google Scholar]