

Abstract
Background:
This study assessed the outcomes, at skeletal maturity, for 34 patients in whom congenital pseudarthrosis of the tibia (CPT) had been treated with intramedullary (IM) rod fixation.
Methods:
The results in skeletally mature patients in whom type-4 CPT had been treated with an IM rod at an average of 11.9 years earlier were reviewed. The rod procedures varied according to whether both the tibia and the fibula were resected and both bones (type A) or just the tibia (type B) were fixed with an IM rod or whether only the tibia was resected and the fibula received no surgery (type C). Outcome grading ranged from unequivocal union with brace-free function (grade 1) to a functional limb with residual angulation or cortical defects (grade 2) to a severely impaired extremity with insufficient union or refracture (grade 3).
Results:
Thirty-four patients were evaluated at a mean age of 16.9 years, a mean of 11.9 years after their initial surgical procedure. Seventeen patients had a grade-1 result; 11 patients, grade 2; and 6, grade 3. Thus, 82% (28) of the 34 patients had a functional extremity at maturity. All patients with a final grade-3 outcome eventually requested amputation. The final outcomes were not affected by the age at the initial fracture or surgery, the presence of neurofibromatosis-1, or cross-ankle fixation. A total of 58 IM rod procedures were performed in the 34 patients. Twenty-four (73%) of the 33 type-A procedures produced grade-1 or 2 outcomes, as did 14 (88%) of the 16 type-B procedures. Of the 9 type-C procedures, none produced a grade-1 result and 4 produced a grade-2 outcome. The results of types A and B combined were superior to those of type-C procedures (p = 0.03). Refracture occurred in 13 of 33 patients with initial stability/union after rod fixation, with 3 of those fractures remaining ununited at the latest follow-up. A dystrophic fibula had no effect on the eventual achievement of a grade-1 or 2 outcome.
Conclusions:
This review, in which all patients had reached skeletal maturity, documents functional (grade-1 or 2) outcomes in 82% of cases of IM rod fixation for CPT. This finding was almost identical to the result in our earlier report and confirms the long-term value of permanent IM rod fixation in maintaining union and function in patients with CPT. Procedures not addressing the fibula produced inferior results. Although 13 patients had a refracture following initial union, only 3 of these fractures failed to heal with additional treatment.
Level of Evidence:
Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
Treatment of congenital pseudarthrosis of the tibia (CPT) by intramedullary rod (IM) fixation was originally described by Charnley (1956)1, with a transankle fixation technique described later by Williams (1965)2. In a previous investigation (2002) at our institution assessing the clinical and radiographic outcomes of variations of this method, procedures that involved resection and grafting of the fibular pseudarthrosis or osteotomy of the intact fibula were more effective at achieving union and preserving alignment and function than those in which no fibular surgery was performed3. However, the long-term functional outcome of an extremity with CPT is notoriously uncertain, as the prevalence of refracture can exceed 50% and can occur years after initial union. In reviews specifically addressing this late outcome, Dobbs et al.4 reported that 12 of 18 patients eventually had a refracture at an average 9 years and Shah et al.5 found that 6 of 11 patients had a refracture at an average of 5.6 years. Studies of the results of the Ilizarov method for CPT have shown 33% to 42% refracture rates in patients followed to maturity6,7. As skeletal maturity is thought to impart a certain degree of protection of the tibia, final outcomes should be assessed after this milestone has been reached8,9.
In our original study of the results of IM fixation for CPT3, only two-thirds of the patients had reached skeletal maturity. With this in mind, we reevaluated the original cohort of 23 patients, and added 11 more patients, to determine the outcome at skeletal maturity. Our hypothesis was that union and function would be maintained by the long-term presence of IM fixation.
Materials and Methods
This retrospective review included 23 patients treated from 1978 to 19923 and an additional 11 patients treated since 1992 (Table I); all had unilateral CPT. Inclusion criteria included surgical treatment with IM rod(s)1,2 and autogenous bone-grafting with follow-up through skeletal maturity; all surgical interventions were performed at our institution. Nineteen of the 34 patients had neurofibromatosis type 1 (NF-1). The mean age was 3 years (range, newborn to 13 years) at the first fracture and 5 years (range, 0.8 to 13.4 years) at the first surgery.
TABLE I.
Patient and Surgical Procedure Data
| Patients (N = 34) | Surgical Procedures | |
| Age* (yr) | ||
| 1st op. | 5.0 (0.8-13.4) | — |
| Final follow-up | 16.9 (4.7-25) | — |
| Follow-up time* (yr) | 11.9 (1-19) | — |
| NF-1 | 19 | — |
| Fibular pseudarthrosis | 15 | — |
| Mean ops. per patient | 2.5 | — |
| Cross-ankle fixation | 18 | 24 |
| BMP-2 use | 12 | 15 |
| A procedure | — | 33 |
| B procedure | — | 16 |
| C procedure | — | 9 |
| Contralateral epiphysiodesis | 9 | 9 |
| Ipsilateral hemiepiphysiodesis | 10 | 10 |
The values are given as the mean with the range in parentheses.
Surgical procedures were characterized as described in 20023 (Figs. 1-A, 1-B, and 1-C; Table II). All patients had type-4 CPT10, and all procedures included resection of the tibial pseudarthrosis and surrounding hamartomatous tissue, placement of autogenous iliac crest bone graft, and internal fixation with an IM rod. A 2-piece Williams rod with a threaded male-female connection was inserted antegrade when transankle fixation was necessary, with the male component withdrawn from the heel once cross-ankle fixation was achieved (Fig. 1-C)2. If transankle fixation was unnecessary, due to the surgeon’s decision that satisfactory fixation in the distal tibial metaphysis was achievable, either a Williams rod or a flexible titanium or stainless-steel (Ender) rod was inserted, either antegrade from the proximal part of the tibia or retrograde from the medial malleolus. Type-A procedures included fibular pseudarthrosis resection or fibular shortening osteotomy stabilized by IM fixation, with a sufficient amount of the fibula resected to permit osseous contact at the tibial resection site, especially if the fibula was intact, which could then be compressed during weight-bearing (Fig. 1-A). Type-B procedures were identical to type A except fibular IM fixation was omitted, usually because of a diminutive fibular diaphysis (Fig. 1-B). Type-C procedures included rod fixation and grafting of the tibia but left the fibula untreated (Fig. 1-C). Bone morphogenetic protein-2 (BMP-2)11 was used to augment 15 operations in 12 patients, at the discretion of the surgeon. Ankle transfixation2 was required in 24 procedures (18 patients) to stabilize a short distal tibial segment. Repeat autogenous bone-grafting was performed 10 times during rod revision procedures and 3 times as a single separate procedure.
Figs. 1-A, 1-B, and 1-C Three variations of the Charnley-Williams technique.
Fig. 1-A.

In a type-A procedure, resection of the tibial pseudarthrosis and resection of the fibular pseudarthrosis or shortening of an intact fibula are carried out, after which bone bones are treated with an IM rod and bone graft.
Fig. 1-B.
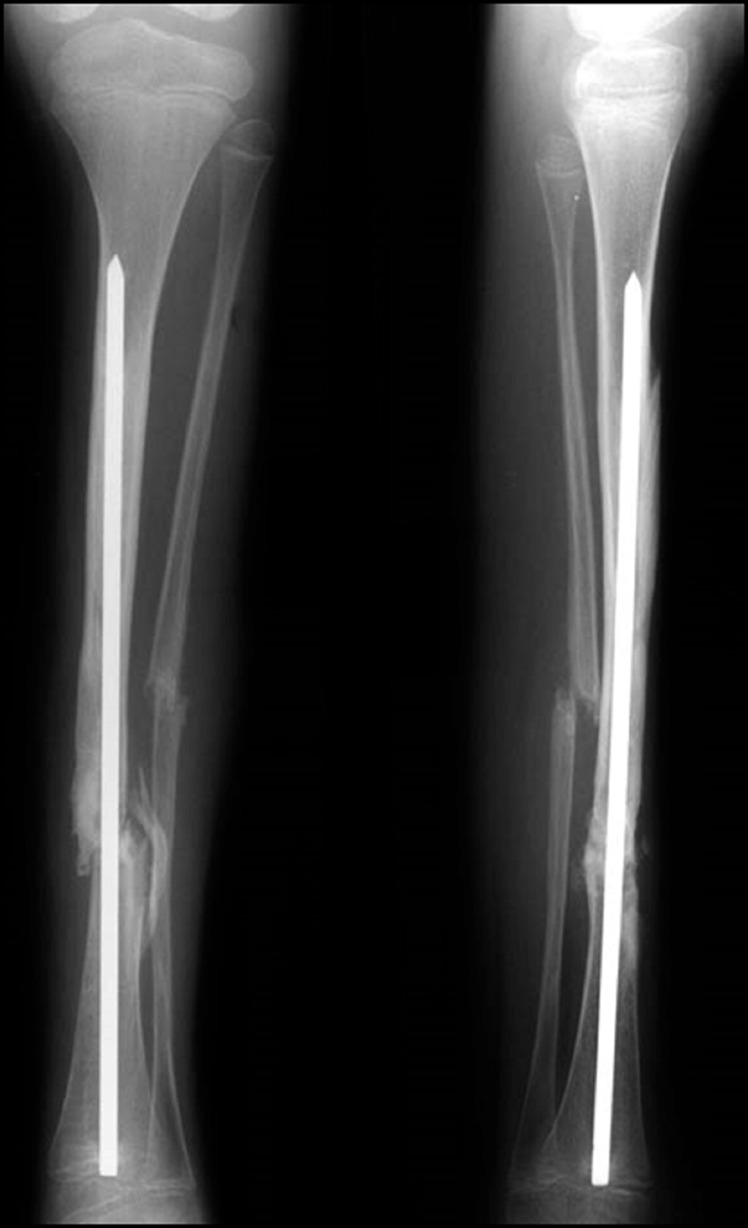
Type B is the same procedure as type A except that no fibular IM rod is placed.
Fig. 1-C.

In a type-C procedure, only the tibia is treated with pseudarthrosis resection, bone-grafting, and insertion of an IM rod. No fibular surgery is performed.
TABLE II.
Technique Variations of IM Rod Procedures
| Type of Procedure | |||
| Bone Status | A | B | C |
| Tibial pseudarthrosis | |||
| Resection | + | + | + |
| Shortening | + | + | − |
| Bone-grafting | + | + | + |
| IM rod | + | + | + |
| Fibular pseudarthrosis | No treatment | ||
| Resection | + | + | |
| Shortening | + | + | |
| Bone-grafting | + | + | |
| IM rod | + | − | |
| Fibula intact | No treatment | ||
| Osteotomy | + | + | |
| Shortening | + | + | |
| IM rod | + | − | |
Follow-up was calculated from the date of the initial surgery to the final clinical follow-up, or to the date of amputation for the patients requesting that procedure. The mean follow-up time was 11.9 years, ranging from 1 year (1 patient requested amputation only 1 year after the initial procedure) to 19 years. Four patients had an amputation prior to maturity.
Postoperatively, all patients were managed with a non-weight-bearing long leg or hip spica cast for 4 to 6 weeks followed by a weight-bearing cast, to encourage compression at the pseudarthrosis site. A protective orthosis was then used for a duration of 3 months to indefinitely, depending on the quality of union and patient comfort. Orthoses were discarded when grade-1 union was achieved or at the patient’s discretion.
Outcomes were graded as described in 20023. Grade-1 outcomes consisted of unequivocal union (4 cortices healed); full brace-free weight-bearing function; and satisfactory alignment, which could include ≤10° of coronal or sagittal malalignment or a limb-length discrepancy of ≤3 cm. An ipsilateral hemiepiphysiodesis or a contralateral epiphysiodesis to achieve these outcomes did not preclude a grade-1 outcome. Grade-2 outcomes described a functionally useful limb, with use of a brace if necessary for activity, and persisting valgus or sagittal bowing for which additional surgery had been considered but not performed because of a lack of refracture or symptoms or because the patient refused. Grade-2 outcomes included radiographic evidence of persisting cortical defects in the tibia. Grade-3 outcomes consisted of dystrophic tibial segments or nonunion resulting in a disabled extremity that required surgical treatment. When a patient had a refracture that subsequently healed after surgical or nonsurgical treatment, resulting in a functional limb, the outcome was graded according to the final alignment and function. Refractures that did not heal led to a grade of 3. For comparative clinical outcome assessment, we combined grade-1 and grade-2 results to accurately capture limbs that were functionally useful.
A Fisher exact test was used to compare the 3 grades of outcomes with the 3 types of procedures.
Results
Thirty-four patients with CPT were evaluated at a mean of 11.9 years (range, 1 to 19 years) after their initial surgical procedure, or to the date of a below-the-knee amputation. The age at the time of follow-up averaged 16.9 years (range, 4.7 to 25 years). With exclusion of the patients requesting amputation, the mean follow-up age was 18 years, which was a mean of 13 years following the initial surgery. All 28 patients with an intact extremity had reached skeletal maturity by the time of follow-up. Seventeen of the 34 patients had a grade-1 result; 11, grade 2; and 6, grade 3 (Table III), with all patients with grade 3 eventually requesting amputation. Thus, 28 (82%) of the 34 patients had a functional extremity (a grade-1 or 2 result) at skeletal maturity.
TABLE III.
Patient Outcomes
| Grade 1 (N = 17) | Grade 2 (N = 11) | Grade 3 (N = 6) | P Value | |
| No. of procedures | 0.26 | |||
| 1 | 6 | 5 | 3 | |
| 2 | 11 | 4 | 2 | |
| 3 | 0 | 2 | 1 | |
| NF-1 | >0.99 | |||
| No | 8 | 5 | 2 | |
| Yes | 9 | 6 | 4 | |
| Fibular dystrophy | 0.20 | |||
| No | 12 | 4 | 3 | |
| Yes | 5 | 7 | 3 | |
| Cross-ankle fixation | 0.66 | |||
| No | 10 | 3 | 3 | |
| Yes | 7 | 8 | 3 | |
| BMP-2 | 0.68 | |||
| No | 12 | 7 | 3 | |
| Yes | 5 | 4 | 3 |
As some patients required >1 operation, the outcomes of each of the 58 individual rod procedures were determined (Tables IV through VII). Grade-1 or 2 outcomes were produced by 24 (73%) of the 33 type-A and 14 of the 16 type-B procedures, whereas none of the 9 type-C procedures resulted in a grade-1 outcome and 4 resulted in grade 2. Outcomes varied according to the procedure type (p = 0.05), with type-C procedures producing inferior outcomes compared with types A and B combined (p = 0.03, Table VII).
TABLE IV.
Patients with Single IM Rod Procedure
| Case | Age at 1st Op. (yr + mo) | NF-1 | Procedure Type | Cross-Ankle Fixation | BMP-2 | Outcome Grade | Follow-up Time (yr) | Age at Final Follow-up (yr + mo) | Refracture | Other Procedures* |
| 1 | 5 + 8 | A | + | 1 | 13 | 18 + 7 | ||||
| 3 | 5 + 1 | B | 1 | 14.5 | 19 + 9 | |||||
| 4 | 2 + 1 | + | A | + | 2 | 17 | 19 + 0 | BG | ||
| 6 | 9 + 5 | + | A | 1 | 10 | 19 + 9 | ||||
| 13 | 1 + 9 | B | + | + | 2 | 19 | 20 + 6 | + | ||
| 18 | 1 + 1 | + | C | + | + | 3† | 10.5 | 11 + 6 | ||
| 20 | 1 + 11 | + | A | + | 1 | 16 | 17 + 10 | HE, BG | ||
| 23 | 0 + 11 | + | B | + | 2 | 17 | 17 + 11 | HE | ||
| 24 | 10 + 11 | B | 1 | 8.5 | 19 + 3 | |||||
| 25 | 4 + 5 | + | A | 1 | 13.5 | 18 + 3 | HE, BG | |||
| 26 | 8 + 10 | A | 3† | 1 | 10 + 0 | |||||
| 28 | 1 + 11 | + | A | + | + | 3† | 3 | 4 + 9 | ||
| 32 | 12 + 6 | A | + | 2 | 6 | 18 + 6 | + | |||
| 33 | 12 + 3 | + | A | + | + | 2 | 13 | 25 + 0 |
BG = bone graft and HE = hemiepiphysiodesis.
Below-the-knee amputation performed.
TABLE V.
Patients with 2 IM Rod Procedures*
| Case* | Age at 1st Op. (yr + mo) | NF-1 | Procedure Type | Cross-Ankle Fixation | BMP-2 | Outcome Grade | Follow-up Time (yr) | Total Follow-up Time (yr) | Age at Final Follow-up (yr + mo) | Refracture | Other Procedures† |
| 2a | 3 + 7 | C | 2 | 5 | 11 + 7 | ||||||
| 2b | 8 + 11 | B | 3‡ | 3 | 8 | + | BG | ||||
| 5a | 4 + 4 | + | C | 3 | 0.7 | 18 + 0 | |||||
| 5b | 5 + 0 | A | + | 1 | 13 | 13.7 | BG | ||||
| 7a | 6 + 11 | A | 2 | 7.5 | 19 + 3 | HE | |||||
| 7b | 14 + 4 | B | + | 1 | 5 | 12.5 | BG | ||||
| 8a | 1 + 8 | + | A | + | + | 2 | 10 | 18 + 3 | + | HE | |
| 8b | 11 + 10 | B | + | 1 | 6.5 | 16.5 | BG | ||||
| 9a | 5 + 1 | + | A | + | 3 | 1 | 17 + 2 | ||||
| 9b | 6 + 2 | B | + | 1 | 11 | 12 | |||||
| 11a | 2 + 6 | + | A | 2 | 2.5 | 18 + 0 | |||||
| 11b | 5 + 1 | A | 1 | 13 | 15.5 | ||||||
| 12a | 1 + 0 | C | + | 3 | 4 | 15 + 6 | |||||
| 12b | 5 + 3 | A | + | + | 1 | 10 | 14.5 | ||||
| 14a | 1 + 7 | B | 3 | 2 | 15 + 9 | ||||||
| 14b | 3 + 6 | A | + | 2 | 12 | 14 | |||||
| 15a | 5 + 6 | B | 2 | 9 | 18 + 1 | + | HE | ||||
| 15b | 15 + 0 | B | 1 | 3.5 | 12.5 | BG | |||||
| 17a | 7 + 4 | A | 3 | 0.4 | 16 + 7 | ||||||
| 17b | 7 + 8 | A | 1 | 9 | 9.4 | + | BG | ||||
| 19a | 2 + 1 | + | A | + | 2 | 6 | 18 + 4 | ||||
| 19b | 8 + 3 | C | 2 | 10 | 16 | BG | |||||
| 21a | 7 + 6 | B | 2 | 6 | 18 + 6 | + | |||||
| 21b | 13 + 5 | C | 2 | 5 | 11 | ||||||
| 22a | 1 + 10 | + | A | + | 2 | 3.5 | 18 + 7 | ||||
| 22b | 5 + 4 | C | + | 2 | 13 | 16.5 | BG | ||||
| 27a | 10 + 11 | + | A | 2 | 1.5 | 18 + 0 | + | HE | |||
| 27b | 12 + 6 | B | + | + | 1 | 5 | 6.5 | ||||
| 30a | 3 + 11 | A | + | 2 | 5 | 14 + 0 | + | ||||
| 30b | 9 + 1 | B | + | 1 | 5 | 10 | |||||
| 31a | 13 + 6 | + | A | + | 3 | 3 | 17 + 9 | + | |||
| 31b | 16 + 6 | A | + | 3‡ | 1 | 4 | |||||
| 34a | 5 + 4 | + | A | + | 2 | 0.5 | 12.9 | I&D | |||
| 34b | 5 + 9 | A | + | 1 | 6.5 | 7 | HE |
a = 1st operation and b = 2nd operation.
BG = bone graft, HE = hemiepiphysiodesis, and I&D = irrigation and debridement.
Below-the-knee amputation performed.
TABLE VI.
Patients with ≥3 IM Rod Procedures
| Case* | Age at 1st Op. (yr + mo) | NF-1 | Procedure Type | Cross-Ankle Fixation | BMP-2 | Outcome Grade | Follow-up Time (yr) | Total Follow-up Time (yr) | Age at Final Follow-up (yr + mo) | Refracture | Other Procedures† |
| 10a | 3 + 2 | + | A | + | 3 | 1 | |||||
| 10b | 4 + 1 | A | + | 2 | 12 | + | HE | ||||
| 10c | 15 + 10 | B | 2 | 2.5 | 15.5 | 18 | |||||
| 16a | 1 + 6 | + | A | + | 2 | 2 | |||||
| 16b | 3 + 4 | C | + | 3 | 7.5 | + | |||||
| 16c | 10 + 9 | C | 3 | 3 | + | BG | |||||
| 16d | 13 + 6 | A | 3‡ | 1.5 | 14 | 15 + 6 | |||||
| 29a | 3 + 5 | A | 3 | 1 | |||||||
| 29b | 4 + 6 | A | 2 | 4 | + | BG | |||||
| 29c | 8 + 4 | B | 2 | 8.5 | 13.5 | 16 + 8 | HE |
a = 1st operation, b = 2nd operation, c = 3rd operation, and d = 4th operation.
HE = hemiepiphysiodesis and BG = bone graft.
Below-the-knee amputation performed.
TABLE VII.
Outcomes by Type of IM Rod Procedure
| Procedure Outcomes (N = 58) (no.) | ||||
| Grade 1 | Grade 2 | Grade 3 | P Value | |
| Procedure type | 0.05 | |||
| A (n = 33) | 9 | 15 | 9 | |
| B (n = 16) | 8 | 6 | 2 | |
| C (n = 9) | 0 | 4 | 5 | |
| A + B vs. C | 0.03 | |||
| B vs. C | 0.012 | |||
| A vs. C | 0.12 | |||
| NF-1 | 0.85 | |||
| No | 8 | 11 | 6 | |
| Yes | 9 | 14 | 10 | |
| Fibular involvement | 0.23 | |||
| No | 12 | 12 | 7 | |
| Yes | 5 | 13 | 9 | |
| Cross-ankle fixation | 0.92 | |||
| No | 10 | 14 | 10 | |
| Yes | 7 | 11 | 6 | |
| BMP-2 | 0.92 | |||
| No | 12 | 19 | 12 | |
| Yes | 5 | 6 | 4 | |
Fourteen patients had only 1 IM rod procedure (Table IV), and 11 of the 14 had a grade-1 or 2 outcome. Seventeen patients underwent 2 IM rod procedures (Table V), and 15 of the 17 had a final grade-1 or 2 outcome. Only 3 patients underwent ≥3 procedures (Table VI). There was no difference in patient outcome on the basis of the number of rod procedures performed (Table III).
As previously reported3, the age at the initial fracture did not affect the patient outcome. The initial fracture occurred at a mean of 3.73 years of age in the patients with a grade-1 outcome, 2.25 years of age in those with grade 2, and 2.68 years of age in those with grade 3 (p = 0.36). The presence of NF-1, a dystrophic fibula (pseudarthrosis, bowing, or hypoplasia), or cross-ankle fixation also did not affect final patient or procedure outcomes (Tables III and VII). The 15 patients with fibular dystrophy did require hemiepiphysiodesis more frequently for valgus deformity (required in 7 patients) compared with the 19 patients with an intact fibula (required in 3 patients; p = 0.07).
When the procedures that addressed the fibula (types A and B) were combined into a single group, they were found to result in better outcomes (p = 0.03) than those that left the fibula untouched (type C) (Table VII). This was due to the efficacy of type-B procedures, the outcomes of which were found to be superior to those of type C when the 2 types of procedures were directly compared (p = 0.012). Somewhat unexpectedly, type-A procedures did not result in statistically better outcomes than type C (p = 0.12). Technically, type-A procedures are identical to type B except for the use of fibular IM fixation (Figs. 1-A and 1-B, Table II), presumably omitted from type-B procedures because of a diminutive fibular diaphysis, although this could not be confirmed by review of operative notes.
Thirteen of 33 patients who had obtained stability and union after the initial surgery had a refracture, with 3 of these refractures remaining ununited and the patient eventually undergoing amputation. Refractures occurred in the diaphysis where the rod was in situ or they occurred at the proximal or distal tip of the IM rod where the tibial epiphysis had grown off and was no longer “protected” by internal splinting. All but 3 refractures subsequently healed after either external immobilization or revision with a new IM rod.
Patients with a normal fibula were more likely to have a grade-1 outcome following surgery (12 of 31 procedures) than those in whom the fibula was dystrophic (5 of 27) (p = 0.09). However, a limb with a dystrophic fibula was no less likely to have a grade-1 or 2 outcome compared with one with an intact fibula (p = 0.23) (Table VII).
BMP-211,12 was utilized in 15 procedures for 12 patients, at the discretion of the operating surgeon. Of the 15 procedures in which BMP-2 was applied, 9 were initial operations and 6 were revisions; 14 were type-A or B procedures, 11 of which achieved a grade-1 or 2 outcome. However, 3 amputations were also performed following BMP-2 application, including in 1 patient who underwent 2 separate revisions with BMP-2 but did not have fracture-healing. The percentage of grade-1 or 2 outcomes (Table III) did not differ between those who received BMP-2 (9 of 12 patients) and those who did not (19 of 22) or between procedures with BMP-2 (11 of 15) and those without BMP-2 (31 of 43) (Table VII).
In addition to the 58 rod procedures, 10 ipsilateral hemiepiphysiodeses in 10 patients were performed to control valgus deformity. In 4 cases, the alignment improved, changing the outcome from grade 2 to grade 1; in 5, there was insufficient correction to affect the grade of the outcome. Limb-length discrepancy ranged from 0 to 7 cm in the 28 patients who retained the extremity, and measured <2.5 cm in 18. Nine contralateral epiphysiodeses were performed to treat the discrepancies. In total, 87 procedures—58 IM rod procedures, 10 ipsilateral hemiepiphysiodeses, 9 contralateral epiphysiodeses, 6 amputations, 3 separate autogenous bone-graft procedures, and 1 debridement for infection—were performed for the entire cohort of 34 patients (mean, 2.5 procedures per patient).
Discussion
CPT has a well-documented history of resistance to successful treatment. Initial union of the pseudarthrosis is considered necessary, but not necessarily sufficient, for satisfactory useful long-term function of the limb. IM fixation is intended not only to promote union but also to impart longer-term protection against refracture, since the percentage of initially consolidated tibiae that refracture, sometimes years later, can exceed 50% even with an IM rod in place4,5,13. Refracture threatening limb preservation has also been reported in >40% of cases that have undergone meticulous reconstruction with an augmented Ilizarov technique7. Refractures occurred in 13 patients in our series, often but not exclusively at the proximal or distal tip of the IM rod. Late residual deformities—ankle valgus, procurvatum, and limb-length discrepancy—are associated with an increased fracture risk and reduced utility of the limb3,8,14-16. Final evaluation of the results of a surgical technique or evaluation of prognostic factors should therefore be performed at skeletal maturity at a minimum. Consequently, we updated our analysis of the results of the Charnley-Williams procedure after all patients had achieved this milestone.
Controversy surrounds the treatment of this condition. In a multicenter study by the European Paediatric Orthopaedic Society, the success rate of IM rod procedures was reported to be <50%9,17, which was remarkably lower than the 87% rate of successful union and functional utility that we reported in 20023. The outcomes in the current expanded cohort of patients evaluated after reaching skeletal maturity confirm our earlier findings, emphasizing management of the fibula in particular. Other factors can certainly affect union and outcomes. At our institution, iliac crest bone graft is used exclusively when treating CPT, but other investigators have used fibular and tibial grafts successfully18. BMP-2 or 7 has been used to enhance healing11,12,19-22. Augmenting IM fixation with an external fixator can provide compression at the tibial pseudarthrosis site23-26. Recommendations for the appropriate number of attempts to achieve union have varied: Sofield27 recommended 2 or 3 attempts before considering amputation, whereas Lehman et al.28 suggested proceeding directly to amputation without any surgical reconstruction. A decision to amputate should rely on the high probability of poor long-term function when sufficient union was only transiently or was never actually achieved9. In our series, 6 patients with persistent disability due to insufficient union requested amputation, with 3 doing so after only 1 rod procedure. The other 11 patients who had only 1 procedure all had a grade-1 or 2 outcome. Ultimately there was no difference in the final patient outcome related to the number of attempts at IM rod fixation (Table III).
The association of CPT with NF-1 is well known. However, our results suggest that NF-1 does not affect the outcomes of IM rod procedures for CPT (Tables III and VII), and this is consistent with an earlier report29. We also did not find the age at the initial fracture to be prognostic. The patients with an intact fibula at presentation did not have better final outcomes than those with a dystrophic fibula (Table III), although hemiepiphysiodesis to treat valgus deformity was performed more often (in 7 of 15 patients) when the fibula was dystrophic than when it was intact (3 of 19 patients) (p = 0.07). Other investigators have also found that ankle valgus results from fibular pseudarthrosis, even after successful fibular union or synostosis4,9,17.
Management of an intact fibula when treating a tibial pseudarthrosis is controversial. Dobbs et al. found that refracture was more common when a fibular pseudarthrosis was not addressed compared with when it was resected4. End-to-end fibular osteosynthesis or creation of a tibia-fibula synostosis was considered a “key principle” by Seo et al., although 10 of 24 patients in their study had a refracture despite their emphasis on the fibula7. In other series, union was achieved without fibular osteotomy or resection6,30,31. We hypothesize that an intact fibula keeps the tibia distracted, and thus an osteotomy of an intact fibula permits compression at the tibial pseudarthrosis site. Our data confirm that fibular osteotomy or resection (a type-A or B procedure) produces better outcomes (p = 0.03) than procedures in which the fibula is not addressed (type C) (Table VII), which is consistent with other studies7.
Type-B procedures were significantly better at maintaining union and alignment than type-C procedures (p = 0.012), whereas type-A procedures, which differed from type B only by the addition of fibular fixation (Figs. 1-A and 1-B), did not improve outcomes (p = 0.12) compared with type C. Although operative notes rarely described a reason for omission of fibular IM fixation, radiographic review suggested that the fibula was too diminutive to permit rod insertion in many cases. The superiority of fibular fixation (type-A procedure) may not have been proved in our study because the small size of the comparison groups led to the study being underpowered, but we emphasize that treatment of the fibula by resection and grafting, with or without fixation, is critical to achieve union with the Charnley-Williams technique for the tibia.
The value of BMP-2 administration cannot be confirmed from these results (Tables III and VII). Due to the retrospective nature of the study and the uncontrolled, discretionary use of BMP-2, objective validation of each BMP-2 application was not attempted. Overall, this study is clearly limited by its retrospective nature and the heterogeneous degree of limb dystrophy. Multivariate statistical analysis did not identify any factor that affected the radiographic and functional outcomes, other than type-C procedures being less effective.
In spite of these limitations, this review of 34 patients with type-4 CPT treated with the Charnley-Williams technique showed that essentially the same percentage of patients—17 of 34 (50%)—had a grade-1 outcome at skeletal maturity (at a mean follow-up of 13 years [excluding those who underwent amputation]) as was reported in 20023. Similarly, the combined group of patients with type-A or B procedures (fibular surgery performed) had better outcomes than those with type-C procedures (no treatment of the fibula); 82% of the patients with a type-A or B procedure had a useful, functional limb (a grade-1 or 2 outcome) compared with 87% reported in 20023, confirming the long-term maintenance of successful union and a functional limb. No type-C procedure produced a grade-1 outcome, again confirming the 2002 result. Although we cannot explain why type-B procedures but not type A were more effective than type C, these findings at skeletal maturity confirm that permanent IM fixation results in a functional limb in >80% of patients and that one should always operate on the fibula.
Footnotes
Investigation performed at Texas Scottish Rite Hospital for Children, Dallas, Texas
Disclosure: The authors indicated that no external funding was received for any aspect of this work. On the Disclosure of Potential Conflicts of Interest forms, which are provided with the online version of the article, one or more of the authors checked “yes” to indicate that the author had a relevant financial relationship in the biomedical arena outside the submitted work (http://links.lww.com/JBJSOA/A103).
References
- 1.Charnley J. Congenital pseudarthrosis of the tibia treated by intramedullary nail. J Bone Joint Surg Am. 1956. April;38(2):283-90. [PubMed] [Google Scholar]
- 2.Williams PF. Fragmentation and rodding in osteogenesis imperfecta. J Bone Joint Surg Br. 1965. February;47:23-31. [PubMed] [Google Scholar]
- 3.Johnston CE., 2nd. Congenital pseudarthrosis of the tibia: results of technical variations in the Charnley-Williams procedure. J Bone Joint Surg Am. 2002. October;84(10):1799-810. [PubMed] [Google Scholar]
- 4.Dobbs MB, Rich MM, Gordon JE, Szymanski DA, Schoenecker PL. Use of an intramedullary rod for treatment of congenital pseudarthrosis of the tibia. A long-term follow-up study. J Bone Joint Surg Am. 2004. June;86(6):1186-97. [DOI] [PubMed] [Google Scholar]
- 5.Shah H, Doddabasappa SN, Joseph B. Congenital pseudarthrosis of the tibia treated with intramedullary rodding and cortical bone grafting: a follow-up study at skeletal maturity. J Pediatr Orthop. 2011. Jan-Feb;31(1):79-88. [DOI] [PubMed] [Google Scholar]
- 6.Vanderstappen J, Lammens J, Berger P, Laumen A. Ilizarov bone transport as a treatment of congenital pseudarthrosis of the tibia: a long-term follow-up study. J Child Orthop. 2015. August;9(4):319-24. Epub 2015 Aug 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Seo SG, Lee DY, Kim YS, Yoo WJ, Cho TJ, Choi IH. Foot and ankle function at maturity after Ilizarov treatment for atrophic-type congenital pseudarthrosis of the tibia: a comprehensive outcome comparison with normal controls. J Bone Joint Surg Am. 2016. March 16;98(6):490-8. [DOI] [PubMed] [Google Scholar]
- 8.Crossett LS, Beaty JH, Betz RR, Warner W, Clancy M, Steel HH. Congenital pseudarthrosis of the tibia. Long-term follow-up study. Clin Orthop Relat Res. 1989. August;245:16-8. [PubMed] [Google Scholar]
- 9.Tudisco C, Bollini G, Dungl P, Fixen J, Grill F, Hefti F, Romanus B, Wientroub S. Functional results at the end of skeletal growth in 30 patients affected by congenital pseudoarthrosis of the tibia. J Pediatr Orthop B. 2000. April;9(2):94-102. [DOI] [PubMed] [Google Scholar]
- 10.Crawford AH, Jr, Bagamery N. Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop. 1986. Jan-Feb;6(1):72-88. [DOI] [PubMed] [Google Scholar]
- 11.Richards BS, Oetgen ME, Johnston CE. The use of rhBMP-2 for the treatment of congenital pseudarthrosis of the tibia: a case series. J Bone Joint Surg Am. 2010. January;92(1):177-85. [DOI] [PubMed] [Google Scholar]
- 12.Richards BS, Anderson TD. rh-BMP-2 and intramedullary fixation in congenital pseudarthrosis of the tibia. J Pediatr Orthop. 2018. April;38(4):230-8. [DOI] [PubMed] [Google Scholar]
- 13.Joseph B, Somaraju VV, Shetty SK. Management of congenital pseudarthrosis of the tibia in children under 3 years of age: effect of early surgery on union of the pseudarthrosis and growth of the limb. J Pediatr Orthop. 2003. Nov-Dec;23(6):740-6. [DOI] [PubMed] [Google Scholar]
- 14.Inan M, El Rassi G, Riddle EC, Kumar SJ. Residual deformities following successful initial bone union in congenital pseudoarthrosis of the tibia. J Pediatr Orthop. 2006. May-Jun;26(3):393-9. [DOI] [PubMed] [Google Scholar]
- 15.Karol LA, Haideri NF, Halliday SE, Smitherman TB, Johnston CE., 2nd Gait analysis and muscle strength in children with congenital pseudarthrosis of the tibia: the effect of treatment. J Pediatr Orthop. 1998. May-Jun;18(3):381-6. [PubMed] [Google Scholar]
- 16.Kristiansen LP, Steen H, Terjesen T. Residual challenges after healing of congenital pseudarthrosis in the tibia. Clin Orthop Relat Res. 2003. September;414:228-37. [DOI] [PubMed] [Google Scholar]
- 17.Keret D, Bollini G, Dungl P, Fixsen J, Grill F, Hefti F, Ippolito E, Romanus B, Tudisco C, Wientroub S; European Paediatric Orthopaedic Society (EPOS). The fibula in congenital pseudoarthrosis of the tibia: the EPOS multicenter study. J Pediatr Orthop B. 2000. April;9(2):69-74. [DOI] [PubMed] [Google Scholar]
- 18.Khan T, Joseph B. Controversies in the management of congenital pseudarthrosis of the tibia and fibula. Bone Joint J. 2013. August;95-B(8):1027-34. [DOI] [PubMed] [Google Scholar]
- 19.Birke O, Schindeler A, Ramachandran M, Cowell CT, Munns CF, Bellemore M, Little DG. Preliminary experience with the combined use of recombinant bone morphogenetic protein and bisphosphonates in the treatment of congenital pseudarthrosis of the tibia. J Child Orthop. 2010. December;4(6):507-17. Epub 2010 Oct 21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fabeck L, Ghafil D, Gerroudj M, Baillon R, Delincé P. Bone morphogenetic protein 7 in the treatment of congenital pseudarthrosis of the tibia. J Bone Joint Surg Br. 2006. January;88(1):116-8. [DOI] [PubMed] [Google Scholar]
- 21.Lee FY, Sinicropi SM, Lee FS, Vitale MG, Roye DP, Jr, Choi IH. Treatment of congenital pseudarthrosis of the tibia with recombinant human bone morphogenetic protein-7 (rhBMP-7). A report of five cases. J Bone Joint Surg Am. 2006. March;88(3):627-33. [DOI] [PubMed] [Google Scholar]
- 22.Spiro AS, Babin K, Lipovac S, Stenger P, Mladenov K, Rupprecht M, Rueger JM, Stuecker R. Combined treatment of congenital pseudarthrosis of the tibia, including recombinant human bone morphogenetic protein-2: a case series. J Bone Joint Surg Br. 2011. May;93(5):695-9. [DOI] [PubMed] [Google Scholar]
- 23.Agashe MV, Song SH, Refai MA, Park KW, Song HR. Congenital pseudarthrosis of the tibia treated with a combination of Ilizarov’s technique and intramedullary rodding. Acta Orthop. 2012. October;83(5):515-22. Epub 2012 Oct 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mathieu L, Vialle R, Thevenin-Lemoine C, Mary P, Damsin JP. Association of Ilizarov’s technique and intramedullary rodding in the treatment of congenital pseudarthrosis of the tibia. J Child Orthop. 2008. December;2(6):449-55. Epub 2008 Oct 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nicolaou N, Ghassemi A, Hill RA. Congenital pseudarthrosis of the tibia: the results of an evolving protocol of management. J Child Orthop. 2013. October;7(4):269-76. Epub 2013 Jun 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shabtai L, Ezra E, Wientroub S, Segev E. Congenital tibial pseudarthrosis, changes in treatment protocol. J Pediatr Orthop B. 2015. September;24(5):444-9. [DOI] [PubMed] [Google Scholar]
- 27.Sofield HA. Congenital pseudarthrosis of the tibia. Clin Orthop Relat Res. 1971. May;76:33-42. [DOI] [PubMed] [Google Scholar]
- 28.Lehman WB, Atar D, Feldman DS, Gordon JC, Grant AD. Congenital pseudoarthrosis of the tibia. J Pediatr Orthop B. 2000. April;9(2):103-7. [DOI] [PubMed] [Google Scholar]
- 29.Masserman RL, Peterson HA, Bianco AJ., Jr Congenital pseudarthrosis of the tibia. A review of the literature and 52 cases from the Mayo Clinic. Clin Orthop Relat Res. 1974. Mar-Apr;99:140-5. [PubMed] [Google Scholar]
- 30.Fern ED, Stockley I, Bell MJ. Extending intramedullary rods in congenital pseudarthrosis of the tibia. J Bone Joint Surg Br. 1990. November;72(6):1073-5. [DOI] [PubMed] [Google Scholar]
- 31.Joseph B, Mathew G. Management of congenital pseudarthrosis of the tibia by excision of the pseudarthrosis, onlay grafting, and intramedullary nailing. J Pediatr Orthop B. 2000. January;9(1):16-23. [DOI] [PubMed] [Google Scholar]