

Abstract
BACKGROUND:
Intrusion of maxillary incisors is the treatment of choice to correct deep bite problem in gummy smile patients.
AIM:
The objective of this study was to compare the effectiveness and efficiency of miniscrew-supported intrusion versus intrusion arch for treatment of deep bite.
METHODS:
The study sample consisted of 30 post pubertal patients (21 females and 9 males) with an age range from 17 to 29. They were divided into 2 groups (15 subjects in each group). Group 1 underwent maxillary incisor intrusion using miniscrews, and in group 2 intrusive arch was used. Pre and post-treatment lateral cephalometric x-rays and study models were made to evaluate the demo-skeletal effects. During the study period, no other intervention was attempted. Paired t-test was used to study the changes after treatment.
RESULTS:
The mean amount of overbite correction was 2.6 ± 0.8 (0.49 mm per month) in the miniscrew-supported intrusion group and 2.9 ± 0.8 (0.60 mm per month) in the intrusive arch group. No statistically significant difference was found in the extent of maxillary incisor intrusion between the two systems. The two intrusion systems were statistically different in the extent of incisor proclination, as an intrusive arch group tended to proline upper incisors more than miniscrews-supported intrusion group.
CONCLUSION:
Both systems successfully intruded the 4 maxillary incisors almost with no loss to the sagittal and vertical anchorage, although intrusive arch tended to proline upper incisors significantly.
Keywords: incisors intrusion, deep bite treatment, intrusive arch
Introduction
Deep overbite has been considered as one of the most common malocclusion problems that are difficult to be treated and retained. Correction of the deep bite is often a main objective of the orthodontic treatment because of its potentially detrimental effects on periodontal health, temporomandibular joint function, as well as esthetics. Prevalence of deep overbite was found to be 21% to 26% in the normal population, and about 75% in orthodontic patients [1], [2].
Extrusion of posterior teeth is one of the most common methods to correct deep bite in growing patients [3]. The intrusion of upper and/or lower incisors is a desirable method to correct deep bite in many adolescents and adult patients [4]. Flaring of incisors may be effective for the correction of mild to moderate deep bite. Relative intrusion is the treatment of choice for adolescents [5].
Maxillary incisor intrusion is the treatment of choice in non-growing patients to correct deep bite and gummy smile caused by super-eruption of maxillary incisors [6], [7]. Three treatment modalities were proved to effectively decrease deep overbite by intruding upper incisors: J-hooks headgear, intrusion arches and miniscrew system. However, the intrusion effect of J-hooks headgear may vary since it depends upon patient cooperation [8]. Although, intrusive arches are an alternative in wide spread use; undesirable side effects such as extrusion of posterior teeth and flaring of anterior teeth may compromise their efficiency [9].
The intrusive arch fabricated with TMA wire was found to exert the lowest force compared to utility arches of St.St. and Eligiloy [10], [11]. Recently, miniscrews were used to provide anchorage for intruding maxillary incisors by application of force close to the centre of resistance with no counteractive movement in molars. However, extra cost, patient tolerance and looseness of the screw during treatment may compromise their use [12], [13].
Since the comparative clinical performance of the intrusive arch and miniscrew-supported intrusion has not previously been reported, the objective of this study was to compare the effectiveness and efficiency of these two treatment modalities for maxillary incisor intrusion.
Material and Methods
The sample was selected from the population who sought orthodontic treatment at the outpatient clinic, Department of Orthodontics, Faculty of Oral and Dental Medicine, Beni-Suef University. Thirty post pubertal patients (21 females and 9 males) with deep bite and age range from 17 to 29 years participated in this study. The inclusion criteria for selection of both treatment groups were the following: post pubertal patients (as verified from their CVM [14]) with age more than 17 years, Class I or Class II malocclusion, excessive gingival display on smiling, 4 mm overbite or greater and super-eruption of maxillary incisors. While the exclusion criteria were: having missing teeth on the anterior maxillary area, any history of trauma or root canal treatment, previous orthodontic treatment, and having any hormonal disorder or syndromes. The detailed case history was taken for each patient. Clinical examination and an individualised diagnostic chart were made. The study was approved and supported by the medical, scientific ethics committee of Cairo University. A consent form was obtained from all the patients and/or parents after an explanation of the purpose of the study.
Table 1.
Demographic data
| Parameters | Miniscrew (n=15) | Intrusive arch (n=15) | P-value |
|---|---|---|---|
| Age (Years) | |||
| Mean ± SD | 19.5 ± 2.5 | 22.6 ± 5.3 | 0.057 |
| Gender n (%) | |||
| Male | 3 (20) | 6 (40) | 0.232 |
| Female | 12 (80) | 9 (60) | |
| Treatment duration (Months) | |||
| Mean ± SD | 5.3 ± 1 | 4.8 ± 1 | 0.152 |
*: Significant at P ≤ 0.05
This prospective clinical trial compared two non-compliance, segmented mechanics for treatment of deep overbite; Miniscrews-supported intrusion and intrusive arch. According to the treatment modality used, the participants were randomly allocated to the two groups. Group 1: maxillary incisor intrusion using miniscrews and group 2: maxillary incisor intrusion using intrusive arches.
The appliance used was a pre-adjusted edgewise Brackets (0.022” x 0.028”) slot size and Roth prescription (series2000; Ormco, Glendora, Calif). The posterior anchor unit was supported by a transpalatal arch with wire diameter (0.04”) and cemented to the first maxillary molar. The alignment was carried out in the upper arch using 0.016” and then (0.016” x 0.022”) nickel-titanium wires and followed by (0.016” x 0.022”) St.St. I was stabilizing arch wire (Ormco). After alignment, the brackets of the 4 maxillary incisors were laced by ligature wire, and the stainless-steel wire was cut into two buccal segments and a maxillary anterior segment.
In group1 intrusion of maxillary incisors was done using two miniscrews (Jeil medical Co., Seoul, Korea), 1.4 mm in diameter and 6 mm in length. The miniscrews were placed at the mucogingival junction distal to the maxillary lateral incisors. The miniscrews were loaded 2 weeks later with medium super-elastic nickel-titanium closed-coil springs (3M UnitekTM TAD constant force coil spring 3 mm medium force). A force of 100g was measured using a calibrated Dontrix gauge (Correx; Ortho Care, Saltaire, United Kingdom).
Figure 1.

Maxillary incisors intrusion using mini-screws (start of treatment)
In group 2 intrusion of upper incisors was done using an intrusive arch that was fabricated using 0.017” x 0.025” TMA (Ormco) wire and placed in the auxiliary slot of the maxillary bands. It was activated with a Tweed loop plier (Pin Tech Instruments, Sialkot, Pakistan) to produce an intrusive force of 100 g as applied and measured using the same force gauge.
Figure 2.

Maxillary incisor intrusion using the intrusive arch (start of treatment)
Control appointments were scheduled every 4 weeks, and the force level was checked at every appointment and adjusted whenever needed. No other treatment was performed until suitable overbite was achieved. Termination of the intervention was done after 6 months of treatment or if one of the following was observed 1) Reaching adequate overbite 2) Sever inflammation or miniscrews failure.
The outcome measures that were evaluated were; the rate of intrusion, skeletal, dental and soft tissue effects. Also, patient tolerance and pain experience were evaluated using a questionnaire with pain assessed as mild, moderate or severe. Evaluation of the skeleton-dental changes was carried out using lateral cephalometric radiographs and study models.
Figure 3.
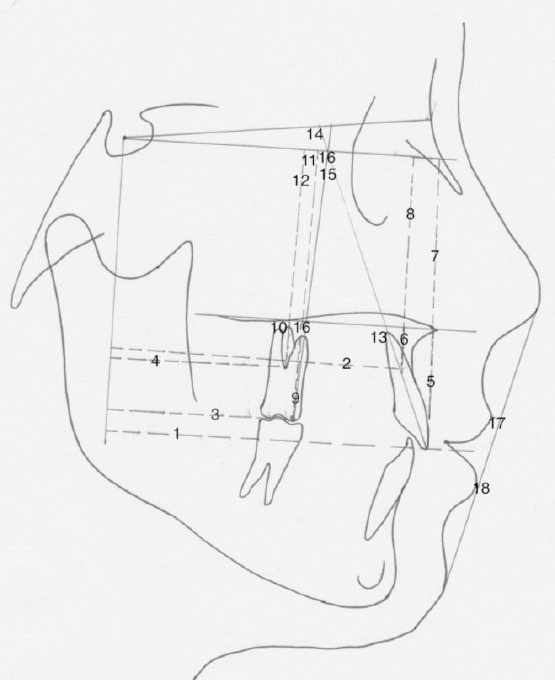
Dental and soft tissue measurements
1. U1-VCP, 2. CR-VCP, 3. U6-VCP, 4. CR-VCP, 5. U1PP, 6. CR-PP, 7. U1-HCP, 8. CR-HCP, 9. U6-PP, 10. CR-PP, 11. U6-HCP, 12. CR-HCP, 13. U1-PP0, 14. U1-SN0, 15. U1-HCP0, 16. U6PP0, 17. LS-Eplane, 18. LI-Eplane.
Statistical Analysis
A power analysis was designed to have adequate power to apply a 2-sided statistical test of the research hypothesis (Null hypothesis) that there was no difference between the two groups. Using alpha (α) level of 0.05 (5%) and Beta (β) level of 0.10 (10%), i.e. power= 90%; the predicted minimum sample size (n) was 11 cases in each group. Over-sampling was done to compensate for dropouts or any failures. After a 2-week interval, 15 study models and 15 cephalograms were randomly selected and re-measured by the same investigator for reproducibility of the measurements. Measurement error was assessed using Dahlberg’s formula: Measurement error=  ; Where (d) is the difference between the measurements and (n) is the number of duplicates. The errors were 0.28 mm for linear measurements and 0.5° for angular measurements in the lateral cephalometric radiographs. Also, it was 0.12 mm for the cast measurements. Numerical data were explored for normality using Kolmogorov-Smirnov and Shapiro-Wilk tests. Numerical data were presented as mean and standard deviation (SD) values. For parametric data; Student’s t-test was used to compare between the two groups. Paired t-test was used to study the changes after treatment in each group. For non-parametric data; Mann-Whitney U test was used to compare between the two groups. Wilcoxon signed-rank test was used to study the changes after treatment in each group. Qualitative data were presented as frequencies and percentages. The significance level was set at P≤0.05. Statistical analysis was performed with IBM® SPSS® Statistics Version 20 for Windows.
; Where (d) is the difference between the measurements and (n) is the number of duplicates. The errors were 0.28 mm for linear measurements and 0.5° for angular measurements in the lateral cephalometric radiographs. Also, it was 0.12 mm for the cast measurements. Numerical data were explored for normality using Kolmogorov-Smirnov and Shapiro-Wilk tests. Numerical data were presented as mean and standard deviation (SD) values. For parametric data; Student’s t-test was used to compare between the two groups. Paired t-test was used to study the changes after treatment in each group. For non-parametric data; Mann-Whitney U test was used to compare between the two groups. Wilcoxon signed-rank test was used to study the changes after treatment in each group. Qualitative data were presented as frequencies and percentages. The significance level was set at P≤0.05. Statistical analysis was performed with IBM® SPSS® Statistics Version 20 for Windows.
Results
The total rate of intrusion was 2.6 ± 0.8 for miniscrews-supported intrusion group and 2.9 ± 0.8 for the intrusive arch group. The monthly rate of intrusion was 0.49 mm/month for miniscrews-supported intrusion group and 0.60 mm/month for Intrusive arch group.
Table 2.
Comparison between rates of intrusion in the two groups
| Parameters | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| Treatment duration (months) | 5.3 ± 1 | 4.8 ± 1 | 0.152 |
| Total rate of intrusion (mm) | 2.6 ± 0.8 | 2.9 ±0.8 | 0.461 |
| Monthly rate of intrusion (mm) | 0.49 | 0.60 |
There was no statistically significant difference between mean changes in skeletal measurements of the two groups.
The intrusive arch group showed statistically significantly higher mean an increase in U1-VCPmm, U1-PP°, U1-SN° and U1-HCP° than Miniscrew group. Miniscrew group showed a statistically significantly higher decrease in CR-PPmm than the intrusive arch group.
Table 3.
Comparisons between amounts of change in skeletal measurements in the two groups
| Skeletal measurements | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| Anteroposterior SNA (°) | 1 ± 4.7 | -0.1 ± 0.4 | 0.967 |
| SNB (°) | 0 ± 0 | -0.1 ± 0.3 | 0.775 |
| ANB (°) | -0.2 ± 0.4 | -0.1 ± 0.3 | 0.539 |
| A-VCP (mm) | -0.3 ± 0.4 | -0.1 ± 0.4 | 0.567 |
| B-VCP (mm) | 0 ± 0 | -0.2 ± 0.5 | 0.775 |
| AB perpendicular to HCP Vertical | -0.3 ± 0.6 | -0.03 ± 0.1 | 0.512 |
| GoMe.SN (°) | 0 ± 0 | 0.3 ± 0.6 | 0.367 |
| N-ANS (mm) | -0.2 ± 0.5 | 0 ± 0 | 0.539 |
| ANS-ME (mm) | 0.1 ± 0.3 | 0.3 ± 0.6 | 0.539 |
| ANS-HCP (mm) | 0.1 ± 0.3 | 0 ± 0 | 0.539 |
| PNS-HCP (mm) Rotation | 0.1 ± 0.5 | 0 ± 0 | 0.775 |
| SN.PP (°) | 0.1 ± 0.3 | 0 ± 0 | 0.539 |
| GoMe.PP (°) | 0.1 ± 0.4 | 0.4 ± 1 | 0.148 |
*: Significant at P ≤ 0.05.
There was no statistically significant difference between mean changes of other dental and soft tissue measurements in the two groups
Table 4.
Comparisons between changes in dental measurements in the two groups
| Dental Measurements | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| Anteroposterior U1-VCP (mm) | -1 ± 1.7 | 1.8 ± 2.6 | 0.002* |
| CR-VCP (mm) | -1.5 ± 0.9 | -0.7 ± 1.4 | 0.174 |
| U6-VCP (mm) | 0 ± 0 | -0.3 ± 0.6 | 0.217 |
| Molar CR-VCP (mm) Vertical | 0 ± 0 | 0 ± 0 | 1.000 |
| UI-PP (mm) | -2.9 ± 1.1 | -2.4 ± 0.9 | 0.233 |
| CR-PP (mm) | -2.3 ± 0.8 | -1.6 ± 0.8 | 0.026* |
| U1-HCP (mm) | -2.9 ± 2 | -2.8 ± 1.1 | 0.775 |
| CR-HCP (mm) | -2.6 ± 1.9 | -2.3 ± 1.8 | 0.187 |
| U6-PP (mm) | 0 ± 0 | -0.1 ± 0.3 | 0.775 |
| Molar CR-PP (mm) | 0 ± 0 | -0.03 ± 0.1 | 0.775 |
| U6-HCP (mm) | 0 ± 0 | -0.1 ± 0.4 | 0.775 |
| Molar CR-HCP (mm) Rotation | 0 ± 0 | -0.3 ± 1.3 | 0.775 |
| U1-PP (°) | 2.3 ± 5.7 | 7.9 ± 4.7 | 0.010* |
| U1-SN (°) | 2 ± 5.5 | 7.7 ± 4.7 | 0.006* |
| U1-HCP (°) | 2.2 ± 5.9 | 7.7 ± 4.2 | 0.013* |
| U6-PP (°) | 0.03 ± 0.1 | -1 ± 1.5 | 0.098 |
| U6-SN (°) | -0.1 ± 0.3 | -0.8 ± 1.3 | 0.116 |
| U6-HCP (°) | -0.1 ± 0.3 | -0.7 ± 1.2 | 0.116 |
Significant at P ≤ 0.05.
The intrusive arch group showed statistically significantly higher mean an increase in overjet than Miniscrew group. There was no statistically significant difference between mean changes of other cast measurements in the two groups.
Figure 4.

Maxillary incisors intrusion using (left) miniscrews and (right) intrusive arch
Similarly, there was no statistically significant difference regarding patients’ tolerance to treatment between the two groups after treatment.
Table 5.
Comparisons between changes in soft tissue measurements in the two groups
| Soft tissue Measurements | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| LS-E plane (mm) | -0.3 ± 0.6 | -0.06 ± 0.7 | 0.345 |
| LI-E plane (mm) | -0.1 ± 0.3 | -0.2 ± 0.6 | 0.539 |
*: Significant at P ≤ 0.05.
Discussion
Deep bite is a complex orthodontic problem that needs to be corrected. Maxillary incisor intrusion is recommended in non-growing patients with deep overbites, especially in those with a gummy smile [15]. The position of maxillary incisors, especially about the upper lip is a key factor in determining the type of treatment since overbite correction with maxillary incisor intrusion in patients with insufficient incisor display leads to flattening of the smile arc and reduces smile attractiveness [16], [17].
Table 6.
Comparisons between changes in cast measurements of the two groups
| Cast Measurements | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| Over bite (mm) | -2.6 ± 0.8 | -2.9 ± 0.8 | 0.461 |
| Over jet (mm) | -0.4 ± 1.2 | 1.4 ± 1.1 | <0.001* |
| Inter-canine width (mm) | -0.6 ± 0.5 | -0.4 ± 0.7 | 0.653 |
| Inter-molar width (mm) | 0 ± 0 | 0 ± 0 | 1.000 |
Significant at P ≤ 0.05.
The only applied force was the maxillary incisor intrusion force to evaluate the genuine treatment efficiency of the two intrusion systems. It is suggested that an intrusive force should be constant, and low load-deflection mechanisms should be used during incisor intrusion [6].
Table 7.
Comparisons between patients’ tolerance of treatment in the two groups
| Tolerance | Miniscrew | Intrusive arch | P-value |
|---|---|---|---|
| n, (%) Tolerance |
10 (66.7) | 6 (40) | 0.143 |
| Pain, discomfort or inflammation | 5 (33.3) | 9 (60) |
*: Significant at P ≤ 0.05.
Different force ranges from 40 to 100 g have been used in recent literature. Steenbergen compared the effect of 40 g and 80 g [18]. Polat used 80 g [13], and Senisik used a range from 90 to 100g [19] while Deguchi et al. used 80-120 g [8].
Conventional intrusion-arch mechanics frequently cause labial tipping of the incisors, which does not always give favourable treatment outcomes [4], [9]. To minimise this effect, the forces were applied through the centre of resistance (CR) to intrude the teeth without producing any labial or lingual rotation. The centre of resistance can be estimated to be located near the geometric centre of their root. In-vitro studies with different methods such as the laser reflection technique, holographic interferometry, photo-elastic stress analysis the finite element method [20] and in-vivo studies were performed to determine the CR of the incisors. All showed that the CRs of the 4 incisors lie 8 to 10 mm apically and 5 to 7 mm distally to the lateral incisors. By placing the screws laterally to the maxillary lateral incisors, the intrusive force could be applied close to the CR of the 4 incisors [21].
Segmented mechanics have been used in this trial as it was claimed to avoid any anterior torque. A system of this type is described as being statically determinate.
Most of the previous studies used either the incisor crown tip or the apex for the evaluation of the amount of intrusion. If the attainment of true intrusion is the purpose of treatment, its evaluation should be made using the centre of resistance of the incisor. Only a few studies have incorporated the CR for the measurement of the amount of intrusion [13], [22], [23]. Therefore the CR of the maxillary central incisor was determined for each patient rather than for the anterior segment because of its ease of location and high reproducibility [13], [18]. It was taken as the point located at one-third of the distance of the root length apical to the alveolar crest.
Two reference planes were constructed for measurement confirmation of dental movements. The first reference plane was the constructed horizontal plane (drawn 7o to the SN plane) and the second was constructed vertical at the Sella point as the palatal plane could not be reliable due to its position near to the area of intrusion. Polat-ozsoy found that the palatal plane moved after intrusion [13].
Overbite correction was faster in the intrusive arch group since overbite reduction was obtained by both maxillary incisor intrusion and protrusion.
Repeated measures showed no statistically significant intergroup difference in the value of maxillary incisor true intrusion. Mean amount of true intrusion in the group (1) was 2.6 ± 1.9 and in the group (2) 2.3 ± 1.8. These results are almost similar to Senisik in comparing miniscrews and Connecticut intrusive arch [10].
After intrusion, in the miniscrew group, there was a statistically significant decrease in mean U1-VCPmm, CR-VCPmm, U1-PPmm, CR-PPmm, U1-HCPmm, and CR-HCPmm that show that the maxillary incisors moved upward and backwards. The possible reason for the maxillary incisor retraction could be the direction of the intrusion force, which may be applied distal to the CR of the four incisors, these results agree with those of recent studies [8], [23]. Further, a comparison of this study with previous reports of incisor intrusion with miniscrews cannot be made because of the differences in the direction of force application and measurements. In this study miniscrews placed between laterals and canines resulting in over bite correction by 2.6 ± 0.8 mm while using a mini implant placed between the maxillary central incisors by Ohnishi et al. in obtained 3.5 mm of incisor intrusion relative to the maxillary incisor tip [12]. Kim et al. applied a segmental intrusion force between the maxillary central incisors [24].
In the intrusive arch group, there was a statistically significant increase in mean U1-VCP mm, U1-PP0, U1-SN0, and U1-HCP0 measurements after treatment, showing incisors proclamation of 7.70 with this intrusion mechanics. Kinzel et al found similar amounts of proclination during incisor intrusion with conventional mechanics [23]. The minimum amount of proclination shown in literature was by Weiland et al, using intrusion base arches [25]. However, Vansteenbergen et al found about 80 of incisor proclination using the same arch [18].
In contrast, Deguchi et al. achieved retrusion of maxillary incisors during maxillary incisor intrusion, which was at variance with the present study [8]. In their study, an additional force in the posterior direction was applied with the intrusive force; thus, during the intrusion, retrusion of maxillary incisors was obtained. According to the results of this study, maxillary incisor intrusion with miniscrews was effective in reducing the amount of protrusion.
The overbite was significantly reduced with intrusive arch by 2.9 ± 0.8 mm and miniscrew treatment by 2.6 ± 0.8 mm. Over bite reduction in the intrusive arch was obtained by both maxillary incisor intrusion and protrusion. However, there was no statistically significant difference between the two groups in over bite reduction. There was a statistically significant difference in over jet between the two groups after treatment. The intrusive arch group showed a significant increase in overjet while decreased in miniscrews group.
First maxillary molars showed no significant changes in both groups. In miniscrew–supported intrusion there was no strain on the posterior segment while in intrusive arch group anchorage reinforcement was done due to the risk of distal molar tipping as recommended in intrusion mechanics. DeVincenzo and Winn used a Nance appliance with intrusion arches and minimised the amount of molar movement [26]. In the present study, the posterior anchorage unit was stabilised using dual mechanics; a heavy stainless steel arch wires and TPA to counteract the moments produced during incisor intrusion [27].
Inter canine width significantly decreased in both groups, and that was one of the side effects of intrusion mechanics as mentioned by Burstone. Inter molar width was preserved in the present study using a passive transpalatal arch.
The side effects in this study were minimal; two miniscrews were loosened in the first month of orthodontic force loading. These were replaced immediately, although, there was no statistically significant difference concerning patient’s tolerance between the two groups. Clinically patients in the intrusive arch group reported more discomfort than miniscrews group.
The selection of either miniscrew-supported intrusion or intrusive arch must depend on the diagnosis, treatment objectives and substantiated with evidence. According to the result of this study, maxillary incisor intrusion with miniscrews was effective in reducing the amount of protrusion. Hence advocated in patients with deep bite and proclaimed incisors while intrusive arch may be recommended in patients with excessive over the bite and retruded incisors.
In conclusion, Both intrusion arches and miniscrews’ supported intrusion were effective in reducing deep overbite with a total amount of upper incisors’ intrusion of (2.6 ± 0.8 mm) and (2.9 ± 0.8 mm) respectively. Selection between the two techniques should be based on the pretreatment maxillary incisors’ position as intrusion arches may result in a further increase in incisors’ inclination contrary to miniscrews’ supported intrusion.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Bergersen E. A longitudinal study of anterior vertical overbite from eight to twenty years of age. Angle Orthod. 1988;58(3):237–256. doi: 10.1043/0003-3219(1988)058<0237:ALSOAV>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Proffit W, FIelds HJ, Moray LJ. Prevalence of malocclusion and orthodontic treatment need in the US. Int J Adult Orthodon Orthognath Surg. 1998;13:97–106. [PubMed] [Google Scholar]
- 3.Hellsing E, Hellsing G, Eliasson S. Effects of fixed anterior biteplane therapy: a radiographic study. Am J Orthod Dentofacial Orthop. 1996;110:61–68. doi: 10.1016/s0889-5406(96)70088-4. https://doi.org/10.1016/S0889-5406(96)70088-4. [DOI] [PubMed] [Google Scholar]
- 4.Otto RL, Anholm JM, Engel G a. A comparative analysis of intrusion of incisor teeth achieved in adults and children according to facial type. Am J Orthod. 1980;77:437–446. doi: 10.1016/0002-9416(80)90108-6. https://doi.org/10.1016/0002-9416(80)90108-6. [DOI] [PubMed] [Google Scholar]
- 5.Hellsing E. Increased overbite and craniomandibular disorders.a clinical approach. Am J Orthod Dentofac Orthop. 1990;98:516–522. doi: 10.1016/0889-5406(90)70018-8. https://doi.org/10.1016/0889-5406(90)70018-8. [DOI] [PubMed] [Google Scholar]
- 6.Burstone CR. Deep overbite correction by intrusion. Am J Orthod. 1977;72(1):1–22. doi: 10.1016/0002-9416(77)90121-x. https://doi.org/10.1016/0002-9416(77)90121-X. [DOI] [PubMed] [Google Scholar]
- 7.Ng J, Major PW, Heo G, Flores-Mir C. True incisor intrusion attained during orthodontic treatment: A systematic review and meta-analysis. Am J Orthod Dentofac Orthop. 2005;128:212–219. doi: 10.1016/j.ajodo.2004.04.025. https://doi.org/10.1016/j.ajodo.2004.04.025 PMid: 16102407. [DOI] [PubMed] [Google Scholar]
- 8.Deguchi T, Murakami T, Kuroda S, Yabuuchi T, Kamioka H, Takano-Yamamoto T. Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofac Orthop. 2008;133:654–660. doi: 10.1016/j.ajodo.2006.04.047. https://doi.org/10.1016/j.ajodo.2006.04.047 PMid: 18456138. [DOI] [PubMed] [Google Scholar]
- 9.Davidovitch M, Rebellato J. Two-couple orthodontic appliance systems utility arches: a two-couple intrusion arch. Semin Orthod. 1995;1:25–30. doi: 10.1016/s1073-8746(95)80085-9. https://doi.org/10.1016/S1073-8746(95)80085-9. [DOI] [PubMed] [Google Scholar]
- 10.Sifakakis I, Pandis N, Makou M, Eliades T, Christoph B. Forces and moments generated with various incisor intrusion systems on maxillary and mandibular anterior teeth. Angle Orthod. 2009;79:928–933. doi: 10.2319/120908-622.1. https://doi.org/10.2319/120908-622.1 PMid: 19705954. [DOI] [PubMed] [Google Scholar]
- 11.Lewis P. Correction of deep overbite: a report of three cases. Am J Orthod Dentofac Orthop. 1987;91:342–345. doi: 10.1016/0889-5406(87)90177-6. https://doi.org/10.1016/0889-5406(87)90177-6. [DOI] [PubMed] [Google Scholar]
- 12.Ohnishi H, Yagi T, Yasuda Y, Takada K. A mini-implant for orthodontic anchorage in a deep overbite case. Angle Orthod. 2005;75:444–452. doi: 10.1043/0003-3219(2005)75[444:AMFOAI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Polat-Ozsoy O, Arman-Ozcirpici A, Veziroglu F. Miniscrews for upper incisor intrusion. Eur J Orthod. 2009;31:412–416. doi: 10.1093/ejo/cjn122. https://doi.org/10.1093/ejo/cjn122 PMid: 19289539. [DOI] [PubMed] [Google Scholar]
- 14.Wong RWK, Alkhal H a, Rabie a BM. Use of cervical vertebral maturation to determine skeletal age. Am J Orthod Dentofac Orthop. 2009;136(4):484.e6. doi: 10.1016/j.ajodo.2007.08.033. https://doi.org/10.1016/j.ajodo.2007.08.033 PMid: 19815140. [DOI] [PubMed] [Google Scholar]
- 15.Janzen E. A balanced smile is a most important treatment objective. Am J Orthod. 1977;72:359–372. doi: 10.1016/0002-9416(77)90349-9. https://doi.org/10.1016/0002-9416(77)90349-9. [DOI] [PubMed] [Google Scholar]
- 16.Lindauer SJ, Lewis SM, Shroff B. Overbite correction and smile Aesthetics. Semin Orthod. 2005;11:62–66. https://doi.org/10.1053/j.sodo.2005.02.003. [Google Scholar]
- 17.Sarver D, Ackerman M. Dynamic smile visualization and quantification: Part I. Evolution of the concept and dynamic records for smile capture. Am J Orthod Dentofac Orthop. 2003;124(1):4–12. doi: 10.1016/s0889-5406(03)00306-8. https://doi.org/10.1016/S0889-5406(03)00306-8. [DOI] [PubMed] [Google Scholar]
- 18.Van Steenbergen E, Burstone CJ, Prahl-Andersen B, Aartman IH a. The influence of force magnitude on intrusion of the maxillary segment. Angle Orthod. 2005;75(5):723–729. doi: 10.1043/0003-3219(2005)75[723:TIOFMO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 19.Senisik NE, Turkkahraman H. Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofac Orthop. 2012;141:723–733. doi: 10.1016/j.ajodo.2011.12.024. https://doi.org/10.1016/j.ajodo.2011.12.024 PMid: 22640674. [DOI] [PubMed] [Google Scholar]
- 20.Turk T, Elekdag-Turk Dincer M. Clinical evaluation of the centre of resistance of the upper incisors during retraction. Eur J Orthod. 2005;27:196–201. doi: 10.1093/ejo/cjh096. https://doi.org/10.1093/ejo/cjh096 PMid: 15817629. [DOI] [PubMed] [Google Scholar]
- 21.Burstone CJ. Biomechanics of deep overbite correction. Semin Orthod. 2001;7:26–33. https://doi.org/10.1053/sodo.2001.21059. [Google Scholar]
- 22.Hong RK, Hong HP, Koh HS. Effect of Reverse Curve Mushroom Archwire on Lower Incisors in Adult Patients: A Prospective Study. Angle Orthod. 2001;71(6):425–432. doi: 10.1043/0003-3219(2001)071<0425:EORCMA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Kinzel J, Aberschek P, Mischak I, Droschl H. Study of the extent of torque, protrusion and intrusion of the incisors in the context of Class II, division 2 treatment in adults. J Orofac Orthop. 2002;63(4):283–299. doi: 10.1007/s00056-002-0109-2. https://doi.org/10.1007/s00056-002-0109-2 PMid: 12198744. [DOI] [PubMed] [Google Scholar]
- 24.Kim TW, Kim H, Lee SJ. Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient. Am J Orthod Dentofac Orthop. 2006;130:676–685. doi: 10.1016/j.ajodo.2005.07.013. https://doi.org/10.1016/j.ajodo.2005.07.013 PMid: 17110268. [DOI] [PubMed] [Google Scholar]
- 25.Weiland F, Bantleon H, Droschl H. Evaluation of continuous arch and segmented arch leveling techniques in adult patients--a clinical study. Am J Orthod Dentofac Orthop. 1996;110(6):647–652. doi: 10.1016/s0889-5406(96)80042-4. https://doi.org/10.1016/S0889-5406(96)80042-4. [DOI] [PubMed] [Google Scholar]
- 26.DeVincenzo JP, Winn MW. Maxillary incisor intrusion and facial growth. Angle Orthod. 1987;57:279–289. doi: 10.1043/0003-3219(1987)057<0279:MIIAFG>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Matsui S, Caputo a a, Chaconas SJ, Kiyomura H. Center of resistance of anterior arch segment. Am J Orthod Dentofac Orthop. 2000;118:171–178. doi: 10.1067/mod.2000.103774. https://doi.org/10.1067/mod.2000.103774 PMid: 10935957. [DOI] [PubMed] [Google Scholar]