

Abstract
A 53-year-old man developed acute left leg pain and edema 2 weeks after lumbar interbody fusion. A computed tomography venogram demonstrated acute thrombosis extending from the deep veins of the calf all the way to and including the common iliac vein owing to external compression of common iliac vein secondary to extruded bone graft material. Endovascular intervention without the use of thrombolysis was performed using a novel percutaneous mechanical thrombectomy system (ClotTriever, Inari Medical, Irvine, Calif), allowing clot removal in single session. Clot removal and stenting were performed with resolution of symptoms and only mild swelling with prolonged standing at the 6-month follow-up.
Acute deep vein thrombosis (DVT) continues to be a major health issue in the United States, with approximately half a million new cases annually.1 Intervention is considered in patients with severely symptomatic proximal DVT, usually by using combined mechanical and pharmacologic methods to remove thrombus.2, 3 Recent bleeding events or high-risk surgery can be prohibitive to the use of thrombolytic agents. In these cases, mechanical thrombectomy alone may be considered. Most devices currently used for percutaneous venous mechanical thrombectomy were initially designed for use in the arterial system and subsequently used for venous thrombosis with or without modification. With the patient's consent, we describe the use of a novel percutaneous device (ClotTriever, Inari Medical, Irvine, Calif) designed specifically for the rapid removal of large venous clot burden in proximal DVT cases.
Case description
A 53-year-old man underwent an anterior lumbar interbody fusion for isthmic spondylolisthesis at L5-S1 that was complicated by right common iliac vein (CIV) bleeding requiring repair with several interrupted Prolene sutures. At his 2-week postoperative visit, he was found to have significant left leg swelling involving the entire leg and thigh. There was no swelling involving the right leg. Venous duplex demonstrated acute obstruction of the left common femoral vein (CFV), femoral vein (FV), popliteal vein, and posterior tibial vein. Computed tomography venogram confirmed acute obstruction of his left CIV through the CFV with no thrombus extending into the inferior vena cava (IVC). There was also evidence of bone matrix migration from the intervertebral space that had migrated adjacent to the CIV, causing severe vein compression (Fig 1).
Fig 1.
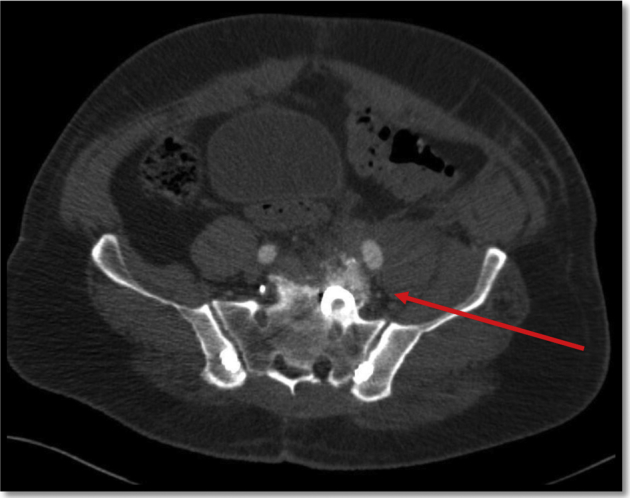
Computed tomography venogram with evidence of bone matrix causing compression of left common iliac vein (CIV).
Owing to the proximity of his complicated spine operation, the decision was made to proceed with mechanical thrombectomy without the use of tissue plasminogen activator. The ClotTriever System is a percutaneous device designed to facilitate the removal of significant amounts of thrombus from larger veins without the need for pharmacotherapy (Fig 2) within 6 weeks of an event. The device consists of two pieces; one is a 13F sheath equipped with a funnel at the proximal end and a large bore hemostatic valve, with attached large suction syringe, designed to facilitate clot removal in concert with the primary device, the ClotTriever catheter. The catheter incorporates a retractable coring element that, when deployed, is designed to capture thrombus from vessels up to 16 mm in diameter, which is then directed into a long collection bag that is then withdrawn through the sheath for retrieval.
Fig 2.

ClotTriever (Inari Medical). The current version of the device consists of a 13F sheath, retractable coring element catheter, and hemostatic valve attached to clot reservoir (Courtesy of Inari Medical, Irvine, Calif).
Initial venography was performed through an 8F sheath inserted in the popliteal vein and demonstrated minimal flow in the FV, CFV, and iliac veins with visualization of collaterals (Fig 3). Owing to the length of the ClotTriever device, an exchange length guidewire was inserted through the 8F sheath across the left iliac veins and IVC into the superior vena cava, with the distal aspect positioned in the right subclavian vein. The 8F sheath was exchanged for the 13F ClotTriever sheath. The ClotTriever catheter was inserted over the guidewire and positioned in the IVC. The coring element and braided nitinol collection bag were then deployed and the device was withdrawn through the left iliac and FVs, capturing the thrombus in the bag. The thrombus was extracted with removal of the device through the 13F sheath. A total of three devices were used. Repeat venography revealed in-line flow in the left iliac veins and IVC with a stenosis at the left CIV level that was confirmed by intravascular ultrasound examination and stented using an 18- × 90-mm WallStent. Poststenting examination revealed a robust in-line flow with minimal remaining thrombus and no collateral flow (Fig 4). The patient was discharged 1 day after intervention with anticoagulation therapy and compression stockings. At the 6-month follow-up from his procedure, he denied any significant leg pain and reported only mild swelling of his left leg with long periods of standing.
Fig 3.
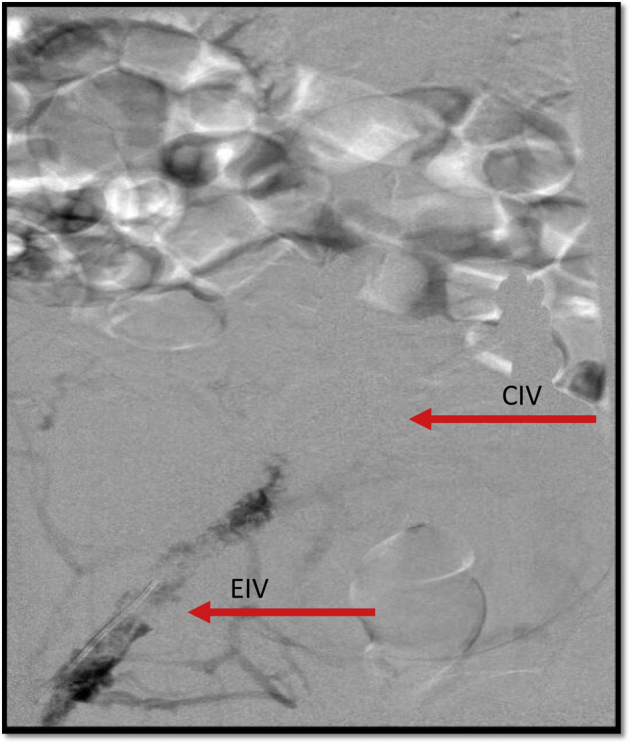
Venography of left lower extremity and pelvis in the prone position demonstrating obstruction of common iliac vein (CIV) with thrombus visualized in common femoral vein (CFV) and external iliac vein. The arrows demonstrated a partially occluded external iliac vein (EIV), a completely occluded CIV, and the CIV stent.
Fig 4.
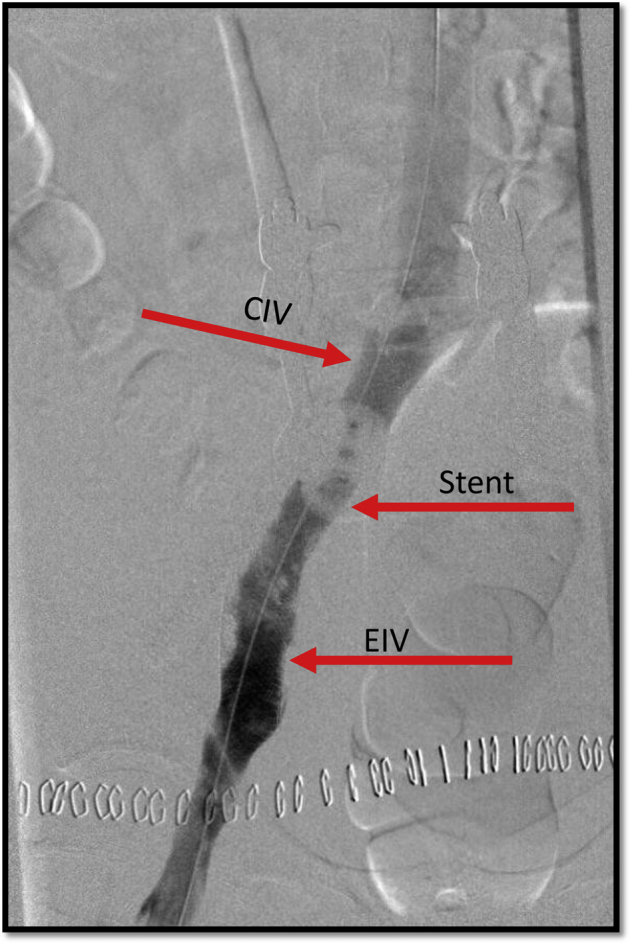
Completion venography demonstrating patent iliac vein stent. The arrows delineate the common iliac vein (CIV) and external iliac vein (EIV).
Discussion
The treatment for proximal DVT can range from sole medical management to use of adjunct endovascular therapies for clot debulking. The mainstay of endovascular therapies involving use of thrombolysis therapy for a period of up to 72 hours.4, 5, 6, 7, 8 The use of thrombolysis not only increases bleeding risks for the patient, but also requires the use of intensive care unit beds, a costly expense and scarce resource in many hospitals.9, 10
This case demonstrates the use of a novel device that allows minimally invasive clot extraction in patients with a relative or absolute contraindication to lytic therapy or those patients that would benefit from a single session treatment. The device facilitates single session treatment of acute to subacute iliofemoral and caval DVT without the need for intensive care or prolonged infusion times. Relative contraindications include the presence of an IVC filter, a venous stent, IVC clot burden, and small caliber vessels (<6 mm). Since this case was performed, improvements to the ClotTriever device have been made, allowing the reuse of devices for multiple passes through a thrombus in a case and shortening the length of the collection bag to eliminate the need to open the collection bag within the heart. Further experience will determine whether this device is cost effective in the care of patients with acute extensive DVT.
Conclusions
Symptomatic iliofemoral DVT in patients at increased risk for thrombolysis therapy can be treated quickly and efficiently using a novel percutaneous device designed specifically for single session treatment of large vein thrombosis. As this device continues to mature, further investigation will be needed to determine how it compares with other mechanical thrombectomy devices and in which patients with DVT it is most effective.
Footnotes
Author conflict of interest: none.
The editors and reviewers of this article have no relevant financial relationships to disclose per the Journal policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
References
- 1.Nutescu E.A., Crivera C., Schein J.R., Bookhart B.K. Incidence of hospital readmission in patients diagnosed with DVT and PE: clinical burden of recurrent events. Int J Clin Pract. 2015;69:321–327. doi: 10.1111/ijcp.12519. [DOI] [PubMed] [Google Scholar]
- 2.Wang C.N., Deng H.R. Percutaneous endovenous intervention plus anticoagulation versus anticoagulation alone for treating patients with proximal deep vein thrombosis: a meta-analysis and systematic review. Ann Vasc Surg. 2018;49:39–48. doi: 10.1016/j.avsg.2017.09.027. [DOI] [PubMed] [Google Scholar]
- 3.Khanna A.K., Singh S. Postthrombotic syndrome: surgical possibilities. Thrombosis. 2012;2012:520604. doi: 10.1155/2012/520604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Meissner H., Gloviczki P., Comerota A.J., Dalsing M.C., Eklof B.G., Gillespie D.L. Early thrombus removal strategies for acute deep venous thrombosis: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2012;55:1449–1462. doi: 10.1016/j.jvs.2011.12.081. [DOI] [PubMed] [Google Scholar]
- 5.Comerota A.J. Thrombolysis for deep venous thrombosis. J Vasc Surg. 2012;55:607–611. doi: 10.1016/j.jvs.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 6.Liu F., Lu P., Jin B. Catheter-directed thrombolysis for acute iliofemoral deep venous thrombosis. Ann Vasc Surg. 2011;25:707–715. doi: 10.1016/j.avsg.2010.12.002. [DOI] [PubMed] [Google Scholar]
- 7.Pianta M.J., Thomson K.R. Catheter-directed thrombolysis of lower limb thrombosis. Cardiovasc Intervent Radiol. 2011;34:25–36. doi: 10.1007/s00270-010-9877-z. [DOI] [PubMed] [Google Scholar]
- 8.Lin P.H., Ochoa L.N., Duffy P. Catheter-directed thrombectomy and thrombolysis for symptomatic lower-extremity deep vein thrombosis: review of current interventional treatment strategies. Perspect Vasc Surg Endovasc Ther. 2010;22:152–163. doi: 10.1177/1531003510378756. [DOI] [PubMed] [Google Scholar]
- 9.Watson L., Broderick C., Armon M.P. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev. 2014;23:CD002783. doi: 10.1002/14651858.CD002783.pub3. [DOI] [PubMed] [Google Scholar]
- 10.Ng T.T., Sigman M., Weaver F.A. Basic data related to thrombolytic therapy for acute venous thrombosis. Ann Vasc Surg. 2014;28:1039–1044. doi: 10.1016/j.avsg.2013.12.002. [DOI] [PubMed] [Google Scholar]