

Abstract
Introduction
Anterior cruciate ligament reconstruction (ACLR) is associated with poor return to sport and high graft re-rupture rates. This study explored the use of a wearable inertial sensor (ViMove) that incorporates an accelerometer and gyroscope, and MatScan pressure sensing mat (TekScan, South Boston, Massachusetts, USA) to provide objective return-to-sport measures.
Methods
Three cohorts’ ACLR patients, non-athletic controls and elite athletes (Australian seven’s rugby Olympic Gold medallist). Patients performed biometric and functional tests (thigh circumference and triple hop) and the ViMove knee module (consisting of single and double leg squats, hops and box drops) for lower limb alignment assessment, concurrently with force plate.
Results
Elite athletes had less varus/valgus (VV) movement during ViMove exercises compared with the ACLR cohort, who in turn had less VV malalignment than controls. When analysing side-to-side differences, single leg squats and box drop were asymmetrical in the ACL group, with greater malalignment in the reconstructed leg (p<0.05). Subgroup analysis failed to differentiate who passed or failed current return to sport assessment. TekScan pressure plate detected differences in double leg landing and flight time while hopping not detected with ViMove, suggesting ACL patients compensate by offloading the reconstructed leg to improve coronal alignment during double leg activity.
Conclusion
The inertial sensor detected differences in motion for patients following ACLR, which are known to be associated with graft rupture and were not detected with functional return to sport testing. Coupling the device with data from a pressure plate provides a powerful assessment tool detecting alignment differences known to be associate with graft failure only previously detected in formal gait analysis.
Keywords: ACL, accelerometer, knee acl, orthopaedics, sports
What are the new findings.
Wearable inertial sensors detect differences in coronal alignment during single leg functional activities in the assessment of return to sport for anterior cruciate ligament (ACL) reconstruction patients not accounted for by current functional return to sport tests. These coronal alignment abnormalities have been associated with a higher risk of graft rupture in ACL reconstruction patients.
How might it impact on clinical practice in the near future.
Wearable inertial sensors provide clinicians with a way of assessing coronal alignment in office which may improve graft survival or improve return to sport rates in ACL reconstruction patients.
Introduction
With an increasing worldwide incidence,1 2 anterior cruciate ligament (ACL) injuries are devastating to the athlete. The current gold standard of treatment for the pivoting athlete is reconstruction of the ACL using autograft or allograft ligament or tendon.3 Pooled return to sport rates are reported as 63% for preinjury level and 82% for recreational level sport following reconstruction,4 and as low as 46% has been reported for return to sport following revision ACL reconstruction.5
There are non-surgical and surgical factors associated with return to sport. Personality, gender, age, maximum activity score, fear of reinjury and priorities are non-surgical factors shown to be associated with return to sport rates.6–8 Surgical factors shown to be associated with a decrease return to sport include large articular lesions, while the literature on graft choice is less clear regarding allograft and autograft as well as hamstring versus bone patellar tendon bone grafts.6–8 It is essential to protect the graft from re-rupture as revision surgery is associated with poorer outcomes including lower patient reported outcome scores, higher rates of meniscal and chondral pathology and subsequent lower rates of return to sport.9 There are biological and functional considerations when returning to sport as explored in greater depth by Nagelli and Hewett.10 Biological considerations are dependent on graft type, patient and injury factors which affect the time to ligamentisation. However, the time since surgery and graft maturity does not correlate with functional outcomes.11 12
The importance of functional considerations in the return to sport is well supported. In 2014 Barber-Westin performed a systematic review which found only 4% of studies included used a hop test and 9% used muscle strength and 32% only relied on time.13 There has since been a vast expansion of literature, with Davies et al14 reporting a 56% increase in total literature regarding return to sport in ACL patients between 2014 and 2017. Formal motion analyses have identified differences including decreased knee flexion and power absorption during the load phase of gait and running that result in increased valgus moments on the knee and have been shown to increase the subsequent re-rupture rate.15 16 However, full gait analysis generally requires laboratory testing with digital motion capturing systems, considerable setup and training, and multiple markers, usually greater than 10, which often precludes its use from most healthcare workers.
Smart technology has the potential to change the way the clinician interacts with the patient through wearable inertial sensor technologies and influence postoperative recovery.17 It has recently been shown to be beneficial as part of a rehab assessment for ACL patients.18 19 ViMove (DorsaVi, East Melbourne, Australia) is one such device which incorporates the coordinates from an accelerometer and gyroscope into a user-friendly interface displaying lower limb alignment during functional activities. We hypothesised that there are differences in limb kinetics during functional activity that are not detected by current return to sport measures. The aim of the current study was to explore the utility of this accelerometer and gyroscope system as well as a pressure sensing mat (MatScan, TekScan, South Boston, Massachusetts, USA) in detecting kinetic differences in patients prior to return to sport following ACL reconstruction.
Methods
We performed a prospective case control study. Following institutional ethics approval, we recruited patients into three cohorts; ACL reconstructed patients, normal controls and elite athlete controls. ACL reconstructed patients were 8–15 months postsurgery returning to see the surgeon for a clearance to return to sport. The patients were recruited post this visit if they had a normal clinical examination, including absence of swelling, full range of motion negative Lachman’s, anterior draw and pivot shift tests and were returning to a pivoting (level 1) or lateral movement (level 2) as defined by Daniel et al.20
Normal patients were recruited from volunteers at UNSW Sydney and Prince of Wales Hospital. Patients were excluded if they participated in high level sport, gave a history of significant lower limb requiring surgery or causing ongoing disability, or achieved a Lysholm score of less than 100. Elite athletes consisted of Australian sevens rugby players who won the Olympic gold medal in 2016. Players were excluded if they had a current injury, history of knee surgery or Lysholm score of less than 100.
We used the standard ViMove settings for the knee module which involved five repeated measures for each functional test. Functional tests included the double leg squat, single leg squat, single leg hop, 50 cm box drops with single leg landing and double leg landing. The tibia accelerometer used a low-power 3D accelerometer (ST Microelectronics LSM303DLHC). Sampling rates were at 100, 20 and 20 Hz on the x-axis, y-axis and z-axis. These planes correlate with movements in vertical, anterior–posterior and mediolateral directions, respectively. Recordings were transmitted via ‘nRF24 AP2 Nordic Semiconductor ANT’ wireless chip to the computer with the installed manufacturer’s software (V.201.0.3491.8). The device was paired with software using manufacturer’s guidelines for a ‘Monitoring Session’ within the software. Once paired, the accelerometers were placed in the disposable adhesive application pads on the athlete’s tibia. These were placed according to the recommended anatomical locations as per manufacturer instructions21 a manual calibration step is not required.
We performed this concurrently with a MatScan pressure sensing mat (TekScan, South Boston, Massachusetts, USA) which provided a dynamic two-dimensional assessment of pressure to allow secondary analysis of asymmetry. The MatScan system was calibrated using a servohydraulic testing frame (MTS Systems, Eden Prairie, Minnesota, USA), independently calibrated by a third party. The test frame was used to apply loads of 500N, 2500N, 5000N and 7500N. The resulting calibration curve allowed compensation for non-linearity. Peak loads (N) and time of flight were determined from each function and each foot using the TekScan software. See figure 1 for set up.
Figure 1.

TekScan set up. Post-anterior cruciate ligament reconstructed athlete performing hop test, landing. Figure shows ViMove sensor placement along pretibial border and TekScan pressure plate.
As a reflection of current return to sport criteria assessing muscle volume, strength and power we also measured thigh circumference and the triple hop. Thigh circumference was measured a standardised distance of 5 cm from the top of the patella with the knee extended and the leg in a relaxed state with tape measure. The triple hop was performed with the contralateral leg first and the ACL leg second. The total distance for three continuous single hops was measured. The test was repeated if the patient was unable to achieve a stable final landing. A failure was deemed to be <90% of the contralateral side.13
While minimal, we dealt with missing variables through an expectation maximisation (EM) algorithm. For outliers these important results were included but changed to maximum physiological value deemed from other patients to reflect deviation from normal. Significant outliers were attributable to loss of balance or a fall when performing the activity.
Varus and valgus alignment were the key variable of interest. ViMove data reports valgus as a negative value, neutral as zero and varus deviation as a positive value, with the angle reflected in the numerical value (see figure 2). We transformed these values to their absolute values to reflect deviation from 0 (neutral alignment). A log transformation was performed to account for skewed data.
Figure 2.
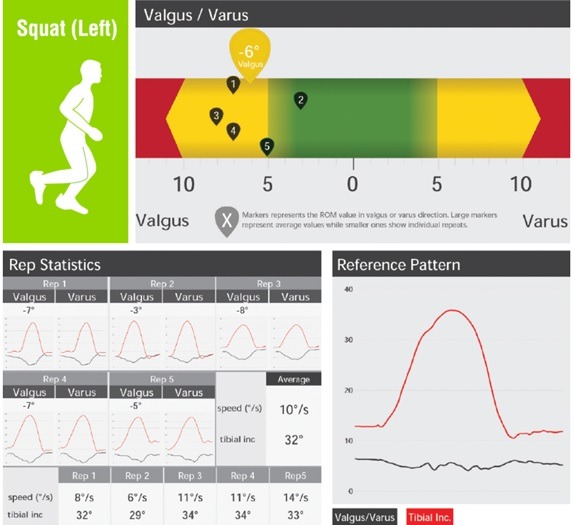
Standard ViMove data report. Typical ViMove data output. Demonstrates output for each of the five repetitions for the functional test—in this case a single leg squat. Figure shows the maximal varus/valgus displacement, along with tibial inclination range and speed of movement with each repetition.
For each functional test, we computed relative importance scores (RIS), denoting the proportional odds of a higher or lower outcome score for a specified level of a predictor variable, compared with reference group. A generalised estimating equations model was used to assess differences in central tendency between the left and right side for normal and elite athlete controls. For the ACL patients we compared reconstructed and contralateral leg of individuals with stratification and subgroup analysis. Variances for all models were estimated accounting for the complex (correlated) structure of the data. Model adequacy was examined using the Jacobian leverage method. Analyses were not adjusted for multiple comparisons given the exploratory nature of the study.
Statistical analysis was performed using Statistical Analysis Software (SAS) V.9.4.
Patient and public involvement
Patients were first involved at the recruitment phase of the research. Patients and the public were not involved in the study design. Patients were recruited passively at routine clinical follow-up, and the burden of participation was explained as part of the consent process. Patient satisfaction was not quantified objectively, although anecdotally the patients often wanted to refer friends and family members not eligible to participate in the study for testing. Patients were provided with direct feedback of their performance immediately post functional testing and they provided email address and will receive notification and a link to the publication once accepted.
Results
There was a total of 65 ACL patients, 27 normal patients and 10 elite athlete controls. The ACL cohort had 72% males versus 28% females with a mean age of 33.84 (SD 10.05) and a body mass index (BMI) of 25.96 (SD 4.27). The normal cohort had 63% males versus 37% females with a mean age of 25.93 (SD 9.71) and a BMI of 23.82 (SD 2.67). In the elite athlete cohort, 100% were females with a mean age of 22.80 (SD 3.64) and a BMI of 24.41 (SD 1.95).
When comparing groups to the ACL group as a baseline, the RIS was less than one for the elite athletes for the majority of the ViMove measures, meaning they were less likely to present a deviation from neutral alignment when performing these activities, and to a lesser degree of varus or valgus alignment when they did. This was statistically significant for double leg and single squat (p<0.01). The RIS for the normal cohort was greater than one, this means their alignment differed from neutral alignment more often and to a greater magnitude than the ACL cohort. This was statistically significant for double leg and single leg squat, box drop single and double leg (p<0.01). Single leg hop had the opposite effect with a RIS of 0.59. Increased age was associated with a RIS of greater than one for double and single leg box drop, and double leg squat (p<0.01). Female sex had a RIS of greater than one compared with males for double and single leg box drop (p=0.03 and p<0.01, respectively). An increased BMI was associated with RIS of less than one for double and single leg box drops and single leg squats (p<0.01 and p<0.03, respectively). No excessive Jacobian leverage values were detected, suggesting goodness-of-fit of the statistical models. See table 1 for further detail.
Table 1.
Proportional odds model—differences between groups
| Cohort | Compared with ACL leg | Compared with contralateral leg | ||||||||||||||
| Normal controls | Elite athletes | Normal controls | Elite athletes | |||||||||||||
| Test | RIS | LL | UL | P value | RIS | LL | UL | P value | RIS | LL | UL | P value | RIS | LL | UL | P value |
| Double leg squat | 1.73 | 1.16 | 2.57 | <0.01 | 0.44 | 0.25 | 0.77 | <0.01 | 1.12 | 0.74 | 1.68 | 0.60 | 0.38 | 0.21 | 0.67 | <0.01 |
| Single leg squat | 1.13 | 0.75 | 1.69 | 0.57 | 0.47 | 0.26 | 0.85 | 0.01 | 1.66 | 1.10 | 2.51 | 0.02 | 0.70 | 0.40 | 1.24 | 0.23 |
| Single leg hop | 1.04 | 0.66 | 1.63 | 0.86 | 1.57 | 0.89 | 2.77 | 0.12 | 0.59 | 0.38 | 0.92 | 0.02 | 0.65 | 0.37 | 1.16 | 0.15 |
| Box drop double leg land, left leg lead | 1.33 | 0.85 | 2.08 | 0.21 | 0.66 | 0.36 | 1.20 | 0.17 | 1.17 | 0.76 | 1.80 | 0.47 | 1.54 | 0.86 | 2.73 | 0.14 |
| Box drop double leg land, right leg lead | 1.85 | 1.18 | 2.91 | <0.01 | 0.97 | 0.54 | 1.74 | 0.91 | 2.12 | 1.36 | 3.31 | <0.01 | 1.20 | 0.67 | 2.16 | 0.55 |
| Box drop single leg land | 1.64 | 1.05 | 2.57 | 0.03 | 0.88 | 0.49 | 1.56 | 0.66 | 1.12 | 0.72 | 1.74 | 0.61 | 0.76 | 0.42 | 1.35 | 0.35 |
As a general rule, the ACL cohort performed better than the normal controls (RIS >1) but the elite athletes performed better than the ACL cohort (RIS <1). RIS >1 means more likely have deviation from neutral alignment, where as a RIS <1 means less likely to have deviation from neutral alignment. The greater the RIS value, the greater amount of varus or valgus compared with the ACL cohort. Results to two decimal places.
ACL, anterior cruciate ligament; LL, lower limit for RIS; RIS, relative importance score; UL, upper limit for RIS.
There were no side to side differences detected based on ViMove data in the normal patients. A difference was however detected in force distribution in landing pressures between sides, the opposite leg from the leading leg assumes more weight in the double leg land but otherwise the left side experienced a greater load (p<0.05) using the TekScan system. Asymmetry was noted in one of the double leg lands in the elite athlete cohort (table 2).
Table 2.
Contralateral limb differences
| Cohort | Normal controls | Elite athlete controls | ACL patients | ||||||
| Test | Left mean/median (SD/IQR) | Right mean/median (SD/IQR) | P value | Left mean/median (SD/IQR) | Right mean/median (SD/IQR) | P value | Contralateral mean/median (SD/IQR) | ACL mean/median (SD/IQR) | P value |
| Hop (s) | 0.235 (0.066) | 0.236 (0.064) | 0.85 | 0.321 (0.054) | 0.312 (0.050) | 0.35 | 0.235 (0.058) | 0.217 (0.054) | <0.001 |
| Hop P(N) | 1306.46 (368.82) | 1244.18 (365.75) | 0.03 | 1008.62 (200.18) | 998.11 (285.84) | 0.86 | 1369.57 (642.86) | 1368.36 (675.34) | 0.95 |
| Single leg land box drop P (N) | 1484.90 (477.64) | 1355.99 (414.28) | 0.01 | 1157.64 (278.68) | 1117.36 (336.34) | 0.61 | 1549.46 (770.01) | 1514.45 (723.58) | 0.21 |
| ACL leg lead box drop double leg land P (N) | 798.61 (286.52) | 699.87 (286.31) | 0.03 | 566.43 (189.48) | 429.27 (162.69) | 0.12 | 845.06 (464.47) | 720.72 (417.65) | 0.004 |
| Contralateral leg lead box drop double leg land P (N) | 710.27 (317.14) | 814.17 (383.90) | 0.05 | 435.60 (144.51) | 487.73 (192.19) | 0.46 | 950.23 (496.10) | 816.70 (410.79) | <0.001 |
| Double leg squat VV | 7 (11) | 8 (11) | 0.91 | 4.5 (7) | 4 (7) | 0.57 | 7 (7) | 6 (6) | 0.97 |
| Single leg squat VV | 9 (10.97) | 9 (8) | 0.73 | 5 (6) | 5 (8) | 0.74 | 7 (6) | 9 (7) | 0.02 |
| Hop VV | 0 (8.9) | 4 (8) | 0.73 | 5 (10) | 5 (8) | 0.87 | 5 (9) | 5 (9.94) | 0.91 |
| Single leg box drop VV | 8 (15) | 8 (12) | 0.46 | 4.5 (7) | 4 (7) | 0.29 | 7 (13) | 8.82 (14) | 0.04 |
| ACL leg lead box drop double leg land VV | 7 (15) | 5 (13) | 0.19 | 0 (9) | 0 (8) | 0.81 | 6 (13) | 5 (11) | 0.55 |
| Contralateral leg lead box drop double leg land VV | 6 (16) | 8 (18) | 0.21 | 4 (9) | 5.50 (14) | 0.04 | 4.20 (12) | 6 (15) | 0.10 |
TekScan data are reported as mean and SD as normally distributed data. Varus/valgus measures are reported as median and IQR due to skewed data. Hop time and p values reported to three decimal places otherwise two.
ACL, anterior cruciate ligament; P, pressure measured in Newtons (N); VV, varus/valgus deviation from neutral reported in degrees.
ACL patients presented greater deviation in the reconstructed leg when performing single leg activities—single leg box drop (p=0.04) and single leg squat (p=0.02). There were no differences detected in alignment in the double leg activities but the force plate showed that the reconstructed leg takes less force than the contralateral (p<0.01). The force plate also revealed a shorter flight time in the single leg hop in the reconstructed leg (p<0.001) (see table 2).
Subgroup analysis was performed based on whether the patient passed or failed the triple hop and quadriceps circumference (see table 3). This failed to account for the differences seen in the alignment or weight distribution differences. When comparing the Dorsavi data for those who passed the triple hop and thigh circumference test with those that did not, those that did not pass the triple hop and thigh circumference had a larger amount of coronal malalignment when performing a single leg hop (p=0.02) compared with those that did pass it.
Table 3.
Contralateral limb differences—ACL passed versus failed return to sport
| Test | Failed return to sport criteria (19) | Passed return to sport criteria (46) | ||||
| Contralateral mean/median (SD/IQR) | ACL mean/median (SD/IQR) | P value | Contralateral mean/median (SD/IQR) | ACL mean/median (SD/IQR) | P value | |
| Hop (s) | 0.220 (0.057) | 0.198 (0.053) | 0.01 | 0.242 (0.057) | 0.224 (0.052) | <0.001 |
| Hop P (N) | 1347.15 (596.08) | 1368.65 (637.23) | 0.56 | 1379.12 (675.15) | 1353.90 (707.30) | 0.25 |
| Single leg land box drop P (N) | 1492.20 (676.00) | 1509.83 (596.20) | 0.68 | 1572.78 (827.40) | 1508.60 (784.04) | 0.06 |
| ACL leg lead box drop double leg land P (N) | 1129.55 (616.50) | 622.55 (289.62) | 0.08 | 885.65 (431.41) | 831.49 (458.98) | 0.22 |
| Contralateral leg lead box drop double leg land P (N) | 789.03 (406.40) | 782.53 (293.03) | 0.01 | 864.64 (496.71) | 760.42 (462.85) | 0.002 |
| Double leg squat VV | 7 (6) | 7 (7) | 0.89 | 6 (5) | 6.96 (6) | 0.92 |
| Single leg squat VV | 8 (8) | 7 (6) | 0.14 | 9 (6) | 7 (6) | 0.16 |
| Hop VV | 3 (8) | 6 (11) | 0.02 | 5 (10) | 5 (9) | 0.42 |
| Single leg box drop VV | 12.87 (11.80) | 11.25 (11.84) | 0.99 | 7.42(13) | 6 (11) | 0.08 |
| ACL leg lead box drop double leg land VV | 6.33 (10.98) | 6.68 (15) | 0.27 | 3.5 (11) | 4.5 (11.02) | 0.91 |
| Contralateral leg lead box drop double leg land VV | 10.90 (17) | 9.63 (16) | 0.33 | 4.5 (13.5) | 4 (12) | 0.22 |
TekScan data are reported as mean and SD as normally distributed data. Varus/valgus measures are reported as median and IQR owing to skewed data. Hop time and p values reported to three decimal places otherwise.
ACL, anterior cruciate ligament; P, pressure measured in Newtons (N); VV, varus/valgus deviation from neutral reported in degrees.
Discussion
The present study explored the utility of smart technology (ViMove) and MatScan pressure sensing mat in assessing coronal plane alignment differences in the assessment of ACL reconstruction patients for return to sport assessment. Accelerometers have been utilised in assessment for return to sport post ACL reconstruction as demonstrated by Gokeler et al, where accelerometers were used to assess jump height and power output asymmetries with hop tests.18 19 We found differences in performance between groups and individuals. Our results suggest lower limb coronal control is associated with athletic ability, and younger age. This limits the ability to compare individuals with standardised values as reported by Herbst et al.22 This is evident in differences in based on sporting level, age, gender and BMI. This is in agreement with Webster et al who have previously demonstrated females are exposed to greater knee abduction moments than males.23 They found surgical factors do not predispose to knee adduction moment differences. The senior author performed the majority of reconstructions using hamstring and bone patella bone autografts in the present study. We did not perform stratification or subanalysis based on surgical factors on the premise that this has been previously investigated.
There is utility for current return to sport measures. Grindem et al24 demonstrated limb asymmetry for <90% strength and hop distance compared with the contralateral leg was associated with a greater incidence of graft rupture; 38.2%, versus those who had >90%; 5.6% incidence of re-rupture. This is not the first study to illustrate the ceiling effect of current return to sport criteria. While we only used quadriceps width and triple hop as a surrogate of return to sport testing, and did not include other measures of strength. Papalia et al25 reported no differences between return to sport rates of ACL patients who underwent rehabilitation with a proprioception based programme versus a traditional strength based programme and no differences between the cohorts in single hop, timed hop and crossover hop tests. However, in those who underwent proprioception based training showed less knee abduction moment compared with the patients in the traditional rehabilitation group. The triple, timed and crossover hops have been found to be of similar efficacy26 and we were not able to differentiate detected differences between those who failed and passed on subgroup analysis.
A limitation of the study is we did not perform our own independent validation of the software compared with sensor movement analysis, however, we relied on other data showing the software utilised in ViMove had repeatable and comparable measurements to optical sensors in functional assessment of the lower limb.12 23 The ViMove system has received Food and Drug Administration clearance for use to measure sagittal and coronal plane range of motion for low back and lumbar spine.
Another limitation of our study is that we have not shown the differences detected to be associated with risk of graft failure. However, this was beyond the scope of the current study. Our study aimed to explore the utility of new smart technologies in detecting differences in kinetics not detected through current return to sport measures which may place an athlete at increased risk of graft re-rupture. With ViMove as our measure, we were able to detect differences in lower limb control using tibial valgus as a surrogate measure for knee abduction. Differences in symmetry in knee abduction moments have been shown to be associated with an increased relative risk for graft re-rupture.15 23 27 We also detected differences between coronal alignment knee in single leg landing from vertical height box drops and single leg squats. Our study has shown utility of such smart technology devices which are more readily available and less time consuming to healthcare professionals and patients than formal gait analysis laboratory.
ViMove did not detect asymmetrical differences in coronal alignment in double leg activity. This may be accounted for by the patient compensating to take less of the force through the reconstructed leg. This is explained by the force plate detecting less force through the reconstructed leg in double leg landing. The symmetrical differences in the flight time for hopping detected by the TekScan force plate are supported by previous research.28 Accelerometers have the ability to predict ground reaction force, and ViMove does so in other ‘modules’ such as the running module. The application of this measurement for these activities would improve ViMove’s utility at screening for asymmetrical differences between individuals. Another limitation is we were not able to assess the sagittal plane for kinetic differences within or between subjects.
Conclusion
Smart technology utilising wearable inertial sensors allows for lower limb alignment assessment outside formal laboratory gait. This wearable sensor shows utility in assessment of ACL reconstructed patients returning to sport by detecting limb alignment differences which in other studies have been shown to be associated with graft re-rupture. ViMove specifically is able to detect differences between the reconstructed leg and contralateral side in single leg squats and single leg vertical height box drops. ViMove’s utility is improved by coupling with a force plate to detect force distribution differences between the limbs when performing double leg activities, as differences in pressure were detected between limbs with the MatScan pressure sensing mat.
Acknowledgments
We would like to thank the Australian women’s sevens rugby union side for the time donated to be tested and serve as a unique comparator for our study.
Footnotes
Contributors: All authors listed have substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data. Drafting the work or revising it critically for important intellectual content. Final approval of the version published. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding: This study was internally funded by the Surgical and Orthopaedic Research Laboratory at the University of NSW. No additional funding was received from this study.
Competing interests: None declared.
Patient consent for publication: Obtained.
Ethics approval: Human ethics research committee at Prince of Wales hospital- reference number HREC ref no: 18/020 (LNR/18/POWH/50).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request.
References
- 1.Moses B, Orchard J, Orchard J. Systematic review: annual incidence of ACL injury and surgery in various populations. Res Sports Med 2012;20:157–79. 10.1080/15438627.2012.680633 [DOI] [PubMed] [Google Scholar]
- 2.Zbrojkiewicz D, Vertullo C, Grayson JE. Increasing rates of anterior cruciate ligament reconstruction in young Australians:2000–15. [DOI] [PubMed]
- 3.Mohtadi NG, Chan DS, Dainty KN, et al. . Patellar tendon versus hamstring tendon autograft for anterior cruciate ligament rupture in adults. Cochrane Database Syst Rev 2011;(9). 10.1002/14651858.CD005960.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ardern CL, Webster KE, Taylor NF, et al. . Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med 2011;45:596–606. 10.1136/bjsm.2010.076364 [DOI] [PubMed] [Google Scholar]
- 5.Anand BS, Feller JA, Richmond AK, et al. . Return-to-Sport outcomes after revision anterior cruciate ligament reconstruction surgery. Am J Sports Med 2016;44:580–4. 10.1177/0363546515618381 [DOI] [PubMed] [Google Scholar]
- 6.Ardern CL, Taylor NF, Feller JA, et al. . Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med 2014;48:1543–52. 10.1136/bjsports-2013-093398 [DOI] [PubMed] [Google Scholar]
- 7.Wright RW, Magnussen RA, Dunn WR, et al. . Ipsilateral graft and contralateral ACL rupture at five years or more following ACL reconstruction: a systematic review. J Bone Joint Surg Am 2011;93:1159–65. 10.2106/JBJS.J.00898 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Krych AJ, Jackson JD, Hoskin TL, et al. . A meta-analysis of Patellar tendon autograft versus Patellar tendon allograft in anterior cruciate ligament reconstruction. Arthroscopy 2008;24:292–8. 10.1016/j.arthro.2007.08.029 [DOI] [PubMed] [Google Scholar]
- 9.Wright R, Spindler K, Huston L, et al. . Revision ACL reconstruction outcomes: moon cohort. J Knee Surg 2011;24:289–94. 10.1055/s-0031-1292650 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nagelli CV, Hewett TE. Should Return to Sport be Delayed Until 2 Years After Anterior Cruciate Ligament Reconstruction? Biological and Functional Considerations. Sports Med 2017;47:221–32. 10.1007/s40279-016-0584-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Claes S, Verdonk P, Forsyth R, et al. . The "ligamentization" process in anterior cruciate ligament reconstruction: what happens to the human graft? A systematic review of the literature. Am J Sports Med 2011;39:2476–83. 10.1177/0363546511402662 [DOI] [PubMed] [Google Scholar]
- 12.Myer GD, Martin L, Ford KR, et al. . No association of time from surgery with functional deficits in athletes after anterior cruciate ligament reconstruction: evidence for objective return-to-sport criteria. Am J Sports Med 2012;40:2256–63. 10.1177/0363546512454656 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Barber-Westin SD, Noyes FR. Objective criteria for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: a systematic review. Phys Sportsmed 2011;39:100–10. 10.3810/psm.2011.09.1926 [DOI] [PubMed] [Google Scholar]
- 14.Davies GJ, McCarty E, Provencher M, et al. . ACL return to sport guidelines and criteria. Curr Rev Musculoskelet Med 2017;10:307–14. 10.1007/s12178-017-9420-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Paterno MV, Schmitt LC, Ford KR, et al. . Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med 2010;38:1968–78. 10.1177/0363546510376053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sigward SM, Lin P, Pratt K. Knee loading asymmetries during gait and running in Early rehabilitation following anterior cruciate ligament reconstruction: a longitudinal study. Clin Biomech 2016;32:249–54. 10.1016/j.clinbiomech.2015.11.003 [DOI] [PubMed] [Google Scholar]
- 17.Iqbal MH, Aydin A, Brunckhorst O, et al. . A review of wearable technology in medicine. J R Soc Med 2016;109:372–80. 10.1177/0141076816663560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ebert JR, Edwards P, Currie J, et al. . COMPARISON OF THE 'BACK IN ACTION' TEST BATTERY TO STANDARD HOP TESTS AND ISOKINETIC KNEE DYNAMOMETRY IN PATIENTS FOLLOWING ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION. Int J Sports Phys Ther 2018;13:389–400. 10.26603/ijspt20180389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gokeler A, Welling W, Zaffagnini S, et al. . Development of a test battery to enhance safe return to sports after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2017;25:192–9. 10.1007/s00167-016-4246-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Daniel DM, Stone ML, Dobson BE, et al. . Fate of the ACL-injured patient. A prospective outcome study. Am J Sports Med 1994;22:632–44. 10.1177/036354659402200511 [DOI] [PubMed] [Google Scholar]
- 21.Raper DP, Witchalls J, Philips EJ, et al. . Use of a tibial accelerometer to measure ground reaction force in running: a reliability and validity comparison with force plates. J Sci Med Sport 2018;21:84–8. 10.1016/j.jsams.2017.06.010 [DOI] [PubMed] [Google Scholar]
- 22.Herbst E, Hoser C, Hildebrandt C, et al. . Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part II: clinical application of a new test battery. Knee Surg Sports Traumatol Arthrosc 2015;23:1283–91. 10.1007/s00167-015-3546-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Webster KE, Feller JA. The knee adduction moment in hamstring and Patellar tendon anterior cruciate ligament reconstructed knees. Knee Surg Sports Traumatol Arthrosc 2012;20:2214–9. 10.1007/s00167-011-1835-z [DOI] [PubMed] [Google Scholar]
- 24.Grindem H, Snyder-Mackler L, Moksnes H, et al. . Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med 2016;50:804–8. 10.1136/bjsports-2016-096031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Papalia R, Franceschi F, Tecame A, et al. . Anterior cruciate ligament reconstruction and return to sport activity: postural control as the key to success. Int Orthop 2015;39:527–34. 10.1007/s00264-014-2513-9 [DOI] [PubMed] [Google Scholar]
- 26.Reid A, Birmingham TB, Stratford PW, et al. . Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Phys Ther 2007;87:337–49. 10.2522/ptj.20060143 [DOI] [PubMed] [Google Scholar]
- 27.Myer GD, Ford KR, Khoury J, et al. . Three-dimensional motion analysis validation of a clinic-based nomogram designed to identify high ACL injury risk in female athletes. Phys Sportsmed 2011;39:19–28. 10.3810/psm.2011.02.1858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Moya-Angeler J, Vaquero J, Forriol F. Evaluation of lower limb kinetics during gait, sprint and hop tests before and after anterior cruciate ligament reconstruction. J Orthop Traumatol 2017;18:177–84. 10.1007/s10195-017-0456-9 [DOI] [PMC free article] [PubMed] [Google Scholar]