

Abstract
The aim of the current study was to develop a measurement approach to assess the learning opportunities provided by parents to their young children with autism spectrum disorder (ASD) during a free play task and to examine the relationship between learning opportunities and child performance on measures of cognition, ASD symptoms, and language. Participants were 91 children with ASD ages 12-24 months and their parents. Ordinary least squares regression was used. Results showed that children whose parents provided more learning opportunities had significantly higher cognitive scores and significantly higher vocabulary comprehension and production. The psychometric properties of the measurement approach were investigated and results indicated that it may be psychometrically sound.
Keywords: autism spectrum disorder, ASD, parent-child interaction, learning opportunities, measurement, video coding
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that affects approximately 1 in 59 children in the United States (Baio et al., 2018). Symptoms emerge early in childhood and although symptoms and severity vary widely from person to person, all individuals with ASD exhibit persistent impairments in reciprocal social communication and social interaction and restricted, repetitive patterns of behavior, interests, or activities (American Psychiatric Association [APA], 2013).
Outcomes of children with ASD vary greatly and are significantly affected by environmental experiences, as demonstrated in randomized controlled trials of intensive behavioral interventions (Dawson & Burner, 2013). Through a neurological lens, this makes a great deal of sense. According to Kandel (2006), experiences play a significant role in shaping the physical nature of the brain. While genetic and developmental processes specify connections among neurons, they do not specify the strength of those connections. Instead, it is experience that specifies strength, which is directly related to the long-term effectiveness of synaptic connections. Thus, while the potential for a child’s behaviors are built into the brain, it is that child’s experiences that alter the effectiveness of those built-in pathways.
Mundy and Neal (2001) proposed a transactional model to describe the nature of pathology in ASD. In this model, symptoms seen early in ASD are viewed both as effects of early pathological neurological processes, as well as agents of later pathological processes. More specifically, they proposed that an early deficit in social orienting and joint attention leads to lessened social information processing in infancy and early childhood. In turn, this impoverished social information input negatively feeds back on the development of the child, leading to insufficient input to promote typical neurological development. Over time, these processes continue to push the child farther and farther from typical development, both socially and neurologically. Similarly, Dawson and colleagues proposed a developmental model of risk, risk processes, symptom emergence, and adaptation in ASD, in which early genetic and environmental risk factors for ASD contribute to an atypical trajectory of brain and behavioral development, which result in altered patterns of interaction between the child and his environment, including altered interactions between the child and his parents. They referred to these altered interactions as risk processes, and argued that they work to prevent typical social and prelinguistic input, ultimately contributing to the full onset of ASD. Further, they stressed that parent-child interaction plays a key role in the development of the social brain, which has strong implications for the development of the child in a multitude of domains (Dawson, 2008; Dawson & Zanolli 2003). Supporting parent-child interaction through parent coaching is often the intervention of choice for young children from a variety of clinical populations, and this may be an effective strategy for increasing the social input necessary for optimal developmental growth in children with ASD.
There is some evidence that facilitating responsive parenting may improve outcomes of children with ASD (e.g., Aldred, Green, & Adams, 2004; Baker, Messinger, Lyons, & Grantz, 2010; Pickles et al., 2016). Siller and Sigman (2002; 2008) were among the first to conduct empirical research in this area. In a series of studies examining effects of parent-child interaction upon children with ASD, they found that higher levels of parental synchronization with children’s attention and activity during play was associated with increased child language and joint attention gains over time. Additional work has demonstrated the relationship between specific types of parent-child interactions and successful development of children with ASD within multiple domains, including play skills (Flippin & Watson, 2011) and vocabulary development (McDuffie & Yoder, 2010). However, there have been some parent-delivered intervention studies that have not shown positive effects on child outcome, or that have shown mixed effects (e.g., Carter et al., 2011). Other studies have found positive effects on child developmental gains; however, the level of gains was variable across children, correlated with number of hours of intervention, and did not differ from gains obtained from community interventions (Rogers et al., 2012).
Such mixed findings point to the importance of identifying the potent parental behaviors that are related to improved outcomes for children with ASD. The quantity of learning opportunities that parents provide, a concept previously studied within the field of education, is an important aspect of parent-child interaction that has not yet been studied in ASD. Previous research has demonstrated that when educators increase the quantity of learning opportunities provided to students (defined as behavioral sequences that include an antecedent, behavior, and consequence), the rate of learning for those students increases (Albers & Greer, 1991; Sutherland & Wehby, 2001). These learning opportunities are defined as behavioral sequences that include an antecedent, behavior, and consequence. The use of these sequences has been shown by scientists to increase learning in all individuals, including young children. According to basic principles within the science of learning, antecedent, behavior, and consequence are the three components that are critical to teach any person—including an infant or toddler with or at risk for ASD (Cooper et al., 2006; Lovaas, 2002).
Research on intellectual and developmental disabilities has described a similar idea with regard to treatment intensity. In fact, a grouping of early intervention approaches for children with ASD, referred to as naturalistic developmental behavioral interventions (Schreibman et al., 2015), relies heavily on natural contingencies and behavioral techniques, including provision of antecedents, behaviors, and consequences. While measures do exist that assess adult-child interaction on a more global scale (e.g., joint engagement coding [Adamson, Bakeman, Deckner, & Nelson, 2012] and the Brief Observation of Social Communication Change [BOSCC; Grzadzinski et al., 2016]), there is currently no thorough or systematic approach to quantifying provision of detailed behavioral contingencies—or learning opportunities—and investigating their specific effect on child learning. Warren, Fey, and Yoder (2007) noted that “virtually no systematic research has been conducted on the effects of different treatment intensities” but that this is a “variable that may be a key to optimizing intervention effects” (Warren et al., 2007, p. 70). These authors conceptualized treatment intensity as the frequency of teaching episodes present within an interaction, a concept that is closely related to the quantity of learning opportunities provided by teachers.
The current study aimed to define and measure the number of learning opportunities provided within parent-child interaction involving young children with ASD. Our aims were to:
-
(1)
develop a novel micro-analytic coding system to measure learning opportunities,
-
(2)
assess the psychometric qualities of the system, and
-
(3)
use the system to examine the relationship between the quantity of learning opportunities that parents provided during a free play task and child performance on standardized measures of cognition, ASD symptoms, and language.
We hypothesized that children of parents who provided a higher quantity of learning opportunities would demonstrate more advanced abilities than children of parents who provided a lower quantity of learning opportunities, after controlling for amount of early intervention received and child’s developmental quotient at entry to the study.
Methods
Participants
The sample included 91 children with ASD and their parents, who were participants in a larger study called the Parents and Toddlers Project (PTP), a multisite, randomized controlled trial investigating the efficacy of the Early Start Denver Model (ESDM; Dawson et al., 2010; Rogers & Dawson, 2010; Rogers et al., 2012). Table 1 presents demographic information on the 91 participants. Participants were recruited through the UC Davis MIND Institute, the University of Washington, and the University of Michigan. To be enrolled in the study, toddlers ages 12-24 months met the following criteria: (1) identified as high risk for ASD on two out of three screeners, consisting of the Early Screening of Autistic Traits Questionnaire (Swinkels et al., 2006), the Infant Toddler Checklist (Wetherby & Prizant, 2002), and the Modified Checklist for Autism in Toddlers (Robins, Fein, & Barton, 1999) (2) met criteria for ASD in a clinical assessment (defined by meeting the cutoff score on the Autism Diagnostic Observation Schedule [ADOS; Lord, Rutter, DiLavore, & Risi, 2003] as well as clinical judgement of ASD by two independent expert psychologists using DSM-IV criteria), (3) a developmental quotient of 35 or higher on the Mullen Scales of Early Learning (MSEL; Mullen, 1989; this was included as an inclusion criterion in order to assure that children were at a developmental level whereat the intervention would fit their developmental needs, in order to assure that children were not failing ADOS items due to general delays as opposed to having ASD, and to follow the procedures of Dawson et al. [2010]), and (4) English as one language spoken in the home. Exclusion criteria included parental self-reported significant mental illness or substance abuse, significant child medical conditions such as cerebral palsy, gestational age of less than 35 weeks, known identified genetic disorders related to developmental disabilities, and current or previous enrollment in intensive one-on-one ASD intervention of more than 10 hours per week (this was included as an exclusion criterion as researchers felt that it would have been difficult to attribute treatment response to the assigned group if children were also receiving many hours of one-on-one intervention weekly, which they defined as 10 or more). Participants in the PTP study were randomized into a treatment or comparison group. Those randomized to the treatment group received a 12-week intervention including weekly 1.5-hour sessions focused on teaching and coaching parents to deliver ESDM throughout natural daily caretaking routines and play periods with their child. Participants randomized to the comparison group received community services (treatment as usual).
Table 1.
Demographic Information on Study Sample
| Variable | Frequency | M | SD |
|---|---|---|---|
| Sex | |||
| Male | 71 | ||
| Female | 20 | ||
| Race | |||
| White | 71 | ||
| Black or African American | 4 | ||
| Asian | 3 | ||
| More than One Race | 13 | ||
| Family Income | |||
| Under $25,000 | 9 | ||
| $25,000-$49,999 | 14 | ||
| $50,000-$74,999 | 14 | ||
| $75,000-$99,999 | 24 | ||
| $100,000-$124,999 | 11 | ||
| $125,000+ | 11 | ||
| Not Provided | 8 | ||
| Maternal Education | |||
| Some High School | 3 | ||
| High School Diploma | 16 | ||
| Some College | 16 | ||
| College Degree | 35 | ||
| Some Graduate School | 1 | ||
| Graduate School Degree | 17 | ||
| Other | 2 | ||
| Not Provided | 1 | ||
| Age at Study Entry (Months) | 21.09 | 3.39 | |
| Mullen Developmental Quotient at Study Entry | 67.62 | 17.35 | |
| ADOS Total Score at Study Entry | 20.31 | 4.61 |
Procedures
The PTP study included an intake visit (evaluation 1), 12 weeks of weekly treatment (see Rogers et al. [2012] for a full description of the method), and a follow-up visit three months later (evaluation 2). Child measures, including the ADOS (Lord et al., 2003), MSEL (Mullen, 1989), and MacArthur-Bates Communicative Development Inventories: Words and Gestures (MCDI; Fenson et al., 2007), were administered at both of these visits. Children were assessed by examiners naïve to treatment status during visits to the research centers, and parents were present in the laboratory room with their children during administration of all measures. In addition, a parent-child free play task took place at both of these visits. For these, parents were presented with a standard set of toys and instructed to play as they normally would at home. The parent-child play, which lasted approximately 10 minutes, was recorded via two video cameras positioned in the laboratory room.
Development of Learning Opportunities Coding System
An aim of this study was to develop a valid description of learning opportunities that parents embed into play. The coding system focused on three occurrences: parental antecedent (A), child behavior (B), and parental consequence (C). The system was designed so that coders could reliably code all dimensions in a maximum of three passes through each video. Coders were permitted to watch the entire video three times through, or rewind and re-watch specific parent-child interactions up to three times each. A successful learning opportunity was defined as an interaction in which a child behavior resulted in a parental consequence that supported learning new skills or practicing existing skills in the domains of communication, social interaction, cognition, fine motor, functional or symbolic play, and expression of refusal or agreement. A learning opportunity could be instigated by the parent providing some type of antecedent that elicited a child behavior, or by the child behaving spontaneously. The possible patterns of learning opportunities are illustrated in Table 2. The examples provided within Table 2 represent the different structural possibilities of each interaction; additional details about each interaction were utilized in order to score an interaction as a successful learning opportunity or failed (see below).
Table 2.
Types and Examples of Learning Opportunities
| Shorthand | Description | Example |
|---|---|---|
| ABC | Parent provided antecedent, child engaged in related behavior, and parent provided consequence. | Parent: “Roll the ball!” Child: Rolled ball to parent. Parent: “Yeah! Nice job!” |
| A | Parent provided antecedent, child did not engage in related behavior, and parent did not provide consequence. | Parent: “Give me five!” |
| AB | Parent provided antecedent, child engaged in a related behavior, but parent did not provide consequence. | Parent: “Feed the bear.” Child: Put bottle to bear’s mouth. |
| BC | Child engaged in behavior without antecedent provided, and parent provided consequence. | Child: Counted “1, 2, 3, 4…” Parent: “5!” |
| B | Child engaged in behavior without antecedent provided, and parent provided no consequence. | Child: Pointed to shirt and labelled “Red!” |
| AC | Parent provided antecedent, child did not engage in related behavior, and parent provided a consequence. | Parent: “Want to sing a song?” Child: Ignored antecedent. Parent: “Old MacDonald Had a Farm…” |
Each child behavior was coded as either unwanted or appropriate. Unwanted behaviors included noncompliance, screaming, whining or crying without accompanying functional language, opening door of room to exit, running around room and/or from parent, throwing toys, displaying aggression toward parent, or engaging in obvious stereotypies or self-stimulatory behavior (e.g., flapping hands or hitting self), and were coded as such by reference to a detailed coding manual by individuals highly trained in working with young children with ASD. Children’s appropriate behaviors were organized into six categories: communication, social interaction, cognition, fine motor, functional and symbolic play, and expression of refusal or agreement. Definitions and examples of behaviors within each category are presented within Table 3. Certain, minimal child behaviors were not coded, including fiddling with a toy, picking up or putting down a toy, walking across the room, sitting down or standing up, and banging a wind-up toy on a table.
Table 3.
Definitions and Examples of Coded Child Behavior
| Category | Definition | Examples |
|---|---|---|
| Communication | Communicative act, with or without a social component | -Vocalizations (including approximations) -Reaching hand out to request |
| Social Interaction | Intentional interactive act directed toward parent | -Making direct eye contact -Waving hello to parent |
| Cognition | Attempt or demonstration of a cognitive skill | -Putting shape in shape sorter -Counting objects -Identifying colors, letters, shapes, numbers |
| Fine Motor | Attempt or demonstration of a fine motor skill | -Winding up toy -Coloring with crayon or marker -Stacking blocks |
| Functional and Symbolic Play Skills | Attempt or demonstration of functional or symbolic play skill | -Putting phone to ear -Feeding figurine or doll -Putting spoon, fork, or cup to mouth |
| Expression of Refusal or Agreement | Attempt or demonstration of appropriate refusal or agreement behavior | -Pushing aside toy (refusal) -Shaking head (refusal) -Saying “yes” (agreement) |
Each learning opportunity was categorized as successful or failed depending on whether a parent provided a consequence in response to the child’s behavior that supported learning. Parental consequence was coded as either positive (e.g., praise or continuation of play), a correction (e.g., punishment or negative consequence such as “No!”), or a prompt (e.g., physical assistance to wind up a toy). A successful learning opportunity was defined as one in which the parent provided a consequence that supported learning, including positively reinforcing an appropriate behavior or prompting a behavior that the child was unable to independently complete. A failed learning opportunity was defined as one in which the parent provided a consequence that did not support the child’s learning, including positively reinforcing an unwanted behavior, failing to provide a positive consequence in response to an appropriate behavior, or negatively responding to an appropriate behavior.
Three one-minute segments of each parent-child interaction video were coded. The coded minutes were derived from the beginning (minute 3; 3:00-3:59), middle (minute 5; 5:00-5:59), and end (minute 7; 7:00-7:59) of the interaction sequence to assess a wide range of play activities. Videos were coded by one of three individuals: the principal investigator, a post-doctoral fellow, or a Bachelor’s-level research assistant. Coders were trained on the coding system using parent-child interaction videos involving children not in the present sample, and training continued until raters reached adequate inter-rater reliability, represented by an intraclass correlation coefficient (ICC) of .70 or above with the first author for 10 consecutive tapes (Lohaus et al., 2004; Yoder & Warren, 2002). In order to assess rater drift, every fifth video was double-coded by the first author and each coder. Single-measure absolute-agreement inter-rater reliability was excellent on all examined codes (ICC for first rater = 0.97; ICC for second rater = 0.87).
Measures
Learning opportunities.
The quantity of successful learning opportunities was represented by a frequency count of successful learning opportunities. This variable was used as the independent variable within the primary analyses for this study.
Parental fidelity.
The ESDM teaching fidelity rating system is a 13-item measure of treatment fidelity developed and used by researchers who worked within the larger PTP study. This measure uses a 5-point Likert scale to examine each parent-child activity and indicates the degree to which parents adhere to ESDM treatment principles, including use of positive affect, managing child attention, managing unwanted behaviors, and engaging in dyadic exchanges. Fidelity was reliably coded by members of the PTP study team outside of those who coded for the current study, using videos drawn from the larger study that were also coded for learning opportunities. This variable was used within tests of convergent/concurrent validity.
Cognition.
The MSEL (Mullen, 1989) is a standardized developmental test for use with children aged 3-60 months. It uses colorful manipulatives and evaluates children on five subscales: gross motor, fine motor, visual reception, receptive language, and expressive language. For each subscale, a t-score, percentile, and age equivalent score is generated. The MSEL has adequate reliability and validity (Oosterling et al., 2010), including construct and divergent validity when used with children with ASD (Swineford, Guthrie, & Thurm, 2015). In order to maximize variability in scores, raw scores on the MSEL served as dependent variables in the current study. Following Rogers et al. (2012), subscales reflected three distinct developmental outcomes: (1) a verbal subscale (reflecting the expressive and receptive language domains), (2) a nonverbal subscale (reflecting the visual reception and fine motor domains), and (3) an overall average score (reflecting all four of these domains).
In addition to being used to create dependent variables, the MSEL was used as a covariate, as appropriate. Developmental quotient was calculated by utilizing the MSEL scores collected at entry to the study. It was created by dividing each child’s developmental age by his or her chronological age, and multiplying by 100.
ASD symptoms.
The ADOS (Lord et al., 2003) is a semi-structured, standardized observational assessment administered directly to children in order to assess symptoms of ASD. Standardized toys and activities are used to present opportunities for social and communicative interaction with the administrator. During these activities, the presence or absence of the child’s behavior of interest is recorded. Higher scores on the ADOS are indicative of greater abnormality. The reliability and validity of the measure are well-established (Lord et al., 2000). This measure was used according to procedures published by Gotham, Risi, Pickles, and Lord (2007). The appropriate module of the standardized ADOS based on each child’s language was administered and severity scores were generated to place data from different modules on the same metric. Assessors naive to assignment were trained to 85% reliability on the full range of scores and met research criteria. Inter-observer reliability at individual sites was assessed on at least 15% of interviews, and any deviation from standards led to retraining. The full range of scores was used, including 3s, in order to maximize the range of each item. This was done with agreement from Dr. Lord, and inter-rater reliability using 3s as scores was utilized in order to test the reliability of the approach. Three subscales were computed: (1) social affect, (2) restricted, repetitive behaviors, and (3) total, which was created by combining the prior two subscales.
Language.
The MCDI: Words and Gestures (Fenson et al., 2007) is a parent report questionnaire that evaluates the words and gestures that children use and understand in natural settings. This form is designed for children aged 8-18 months, and consists of 396 vocabulary words for parents to indicate whether their children produce and/or understand. In addition, parents record any gestures that their children use for communication. The MCDI has strong psychometric properties and is widely used to assess both typically-developing children and those with developmental delays, including ASD (Charman, Drew, Baird, & Baird, 2003; Luyster, Kadlec, Carter, & Tager-Flusberg, 2008). In order to maximize variability in scores, raw scores on the MCDI served as dependent variables in the current study. Four subscales were utilized: (1) phrases understood, representing how many phrases children seemed to understand (2) vocabulary comprehension, representing how many words children seemed to understand (3) vocabulary production, representing how many words children said, and (4) total gestures, indicating how many gestures children exhibited.
Intervention history.
Parent report of interventions that children received from birth until evaluation 2 was collected via telephone interview at the second evaluation, utilizing the CPEA Intervention History Interview (unpublished). Parents were asked for every type of intervention the child had received (e.g., one-on-one home-based treatment, speech therapy, occupational therapy, and parenting seminars), the date the intervention began and ended, the number of hours of each intervention per week, and the ratio of adults to children present during each intervention. The number of hours of each intervention was adjusted for ratio of adults to children, and all intervention hours were summed to create a covariate representing the total number of intervention hours that children received from birth to evaluation 2.
Data Analysis
Assessment of psychometric qualities.
One aim of the current study was to assess the psychometric qualities of the measurement approach through systematic study of reliability and validity. To assess the stability of learning opportunity provision across time, split-half reliability was examined. In order to do this, a subsample of study videos (n = 37) was coded for an additional 3 minutes. Scores from the originally-coded 3 minutes of interaction were compared to those from the second set of 3 minutes, using Spearman-Brown split-half coefficients. Convergent/concurrent validity was assessed by evaluating whether quantity of learning opportunities that parents provided correlated with the previously-validated, theoretically-related ESDM teaching fidelity rating system. Using Pearson product-moment correlation coefficients, convergent/concurrent validity was assessed for all videos, drawn from two time points of the larger PTP study, for which fidelity data was available (n = 158).
Relationship between quantity of learning opportunities and child performance.
The scores from standardized testing conducted at evaluation 2 were used as primary dependent variables. The primary independent variable (i.e., parental provision of learning opportunities) was derived from videos recorded at evaluation 1.
We hypothesized that the quantity of successful learning opportunities that parents provided to their young children with ASD would be positively related to child cognition, ASD symptoms, and language. Covariates for the analyses included children’s developmental quotient as measured at evaluation 1, as appropriate, and a summary score representing the total number of intervention hours that children received from birth to evaluation 2.
Ordinary least squares (OLS) regression was used to test the relationship between parental provision of learning opportunities and child outcomes, with the quantity of successful learning opportunities at evaluation 1 serving as the independent variable and children’s MSEL, MCDI, and ADOS scores from evaluation 2 serving as dependent variables. The p-value for all tests was set at alpha = 0.05, two-tailed.
Results
Assessment of Psychometric Qualities
Split-half reliability was moderate (r = 0.521, n = 37, p < .01), with the quantity of learning opportunities significantly positively correlated across the two coded portions of the video. Convergent/concurrent validity was also adequate (r = 0.420, n = 158, p < .001), with the quantity of learning opportunities significantly positively correlated with ESDM fidelity scores.
Relationship between Quantity of Learning Opportunities and Child Performance
Across the three minutes of coded video, the mean number of successful learning opportunities provided by parents at evaluation 1 (the primary independent variable) was 13.5, with a standard deviation of 6.5. As shown in Table 4, quantity of learning opportunities was significantly moderately related to average MSEL, nonverbal MSEL, verbal MSEL, MCDI vocabulary comprehension, and MCDI vocabulary production. These statistically significant relationships persisted even upon the addition of covariates (i.e., early intervention and initial developmental quotient, as appropriate) into the model.
Table 4.
Taxonomy of Multiple Regression Models Assessing Relationship between Quantity of Learning Opportunities and Child Performance
| Dependent Variable | n | est (se) | R2 | F(dF) | p of F |
|---|---|---|---|---|---|
| Average MSEL | 91 | 0.249*** (0.054) | 0.205 | 11.38 (2, 88) | <.0001 |
| Nonverbal MSEL | 91 | 0.146** (0.049) | 0.105 | 5.17 (2, 88) | <.01 |
| Verbal MSEL | 91 | 0.351*** (0.074) | 0.214 | 11.99 (2, 88) | <.0001 |
| MCDI Phrases Understood | 79 | 0.282 (0.152) | 0.206 | 6.47 (3, 75) | <.001 |
| MCDI Vocabulary Comprehension | 79 | 4.157* (1.679) | 0.302 | 10.82 (3, 75) | <.0001 |
| MCDI Vocabulary Production | 79 | 3.264** (1.065) | 0.454 | 20.82 (3, 75) | <.0001 |
| MCDI Total Gestures | 79 | 0.327 (0.210) | 0.307 | 11.06 (3, 75) | <.0001 |
| ADOS Social Affect | 91 | −0.152 (0.156) | 0.353 | 15.79 (3, 87) | <.0001 |
| ADOS Restricted, Repetitive Behaviors | 91 | 0.067 (0.040) | 0.131 | 4.36 (3, 87) | <.01 |
| Total ADOS | 91 | −0.085 (0.171) | 0.358 | 16.18 (3, 87) | <.0001 |
Notes. Covariates included developmental quotient (excluding models with MSEL as dependent variable) and hours of early intervention; correction for multiple testing was not calculated; differences in n across measures due to the fact that the MCDI relied on parent completion and return, and not all parents completed and returned the measure.
p < .05,
p < .01,
p < .0001
Average MSEL.
Quantity of learning opportunities was significantly associated with average MSEL scores (β = 0.249, t = 4.57, p < .0001). Quantity of learning opportunities and the covariate together accounted for 20.5% of the variance in scores (R2 = 0.205, F(2,88) = 11.38, p < .0001). Please refer to Figure 1 for a graphical representation of the final fitted model.
Figure 1.
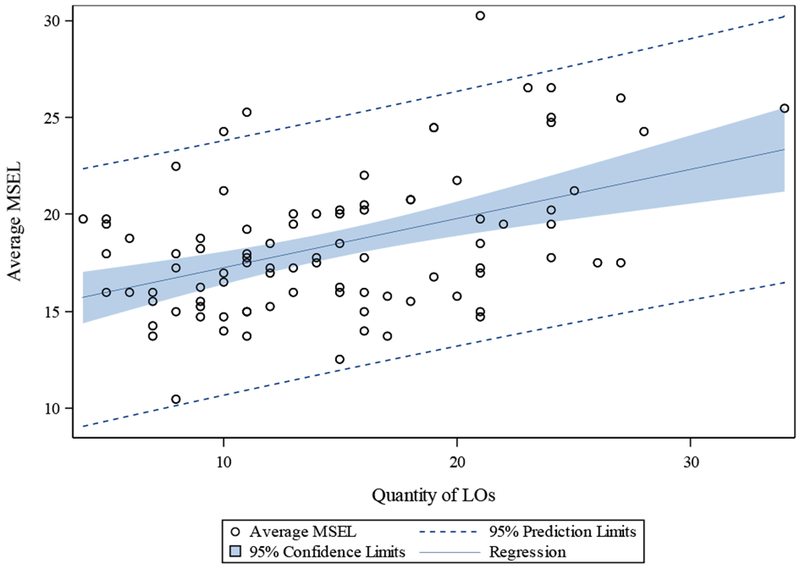
Relationship between quantity of learning opportunities and average MSEL
Nonverbal MSEL.
Quantity of learning opportunities was significantly associated with nonverbal MSEL scores (β = 0.146, t = 3.02, p < .01). Quantity of learning opportunities and the covariate together accounted for 10.5% of the variance in scores (R2 = 0.105, F(2,88) = 5.17, p < .01). Please refer to Figure 2 for a graphical representation of the final fitted model.
Figure 2.
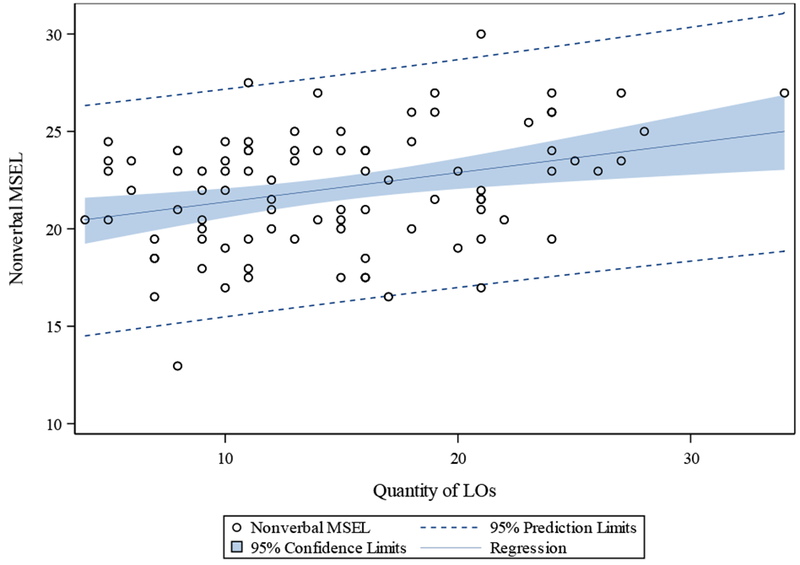
Relationship between quantity of learning opportunities and nonverbal MSEL
Verbal MSEL.
Quantity of learning opportunities was significantly associated with verbal MSEL scores (β = 0.351, t = 4.73, p < .0001). Quantity of learning opportunities and the covariate together accounted for 21.4% of the variance in scores (R2 = 0.214, F(2,88) = 11.99, p < .0001). Please refer to Figure 3 for a graphical representation of the final fitted model.
Figure 3.
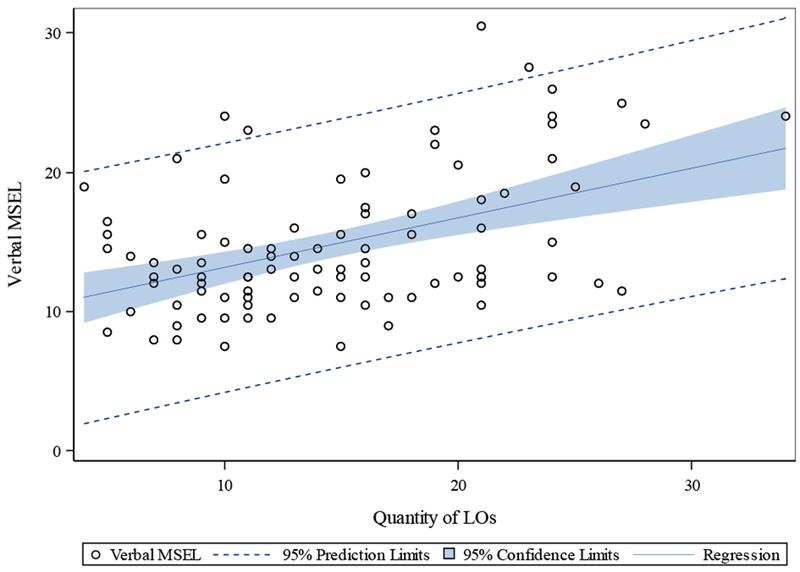
Relationship between quantity of learning opportunities and verbal MSEL
MCDI vocabulary comprehension.
Quantity of learning opportunities was significantly associated with MCDI vocabulary comprehension scores (β = 4.157, t = 2.48, p < .05). Quantity of learning opportunities and the covariates together accounted for 30.2% of the variance in scores (R2 = 0.302, F(3,75) = 10.82, p < .0001). Please refer to Figure 4 for a graphical representation of the final fitted model.
Figure 4.
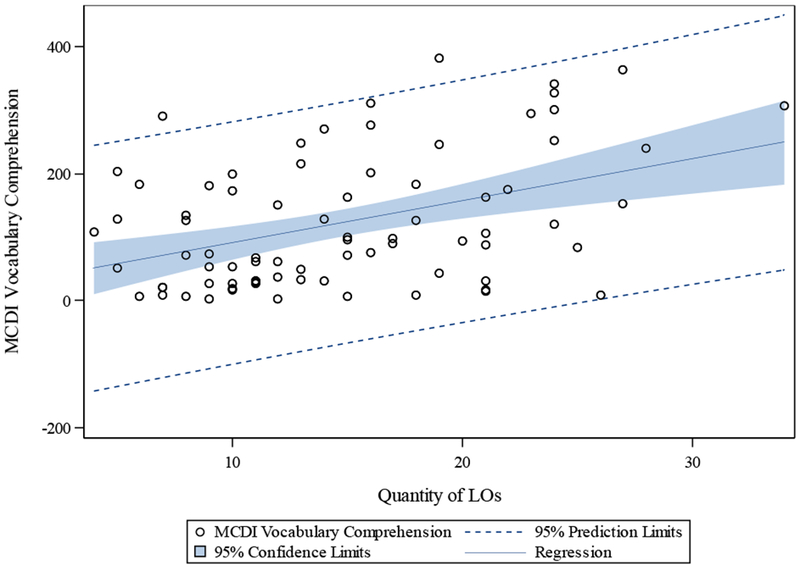
Relationship between quantity of learning opportunities and MCDI vocabulary comprehension
MCDI vocabulary production.
Quantity of learning opportunities was significantly associated with MCDI vocabulary production scores (β = 3.264, t = 3.06, p < .01). Quantity of learning opportunities and the covariates together accounted for 45.4% of the variance in scores (R2 = 0.454, F(3,75) = 20.82, p < .0001). Please refer to Figure 5 for a graphical representation of the final fitted model.
Figure 5.
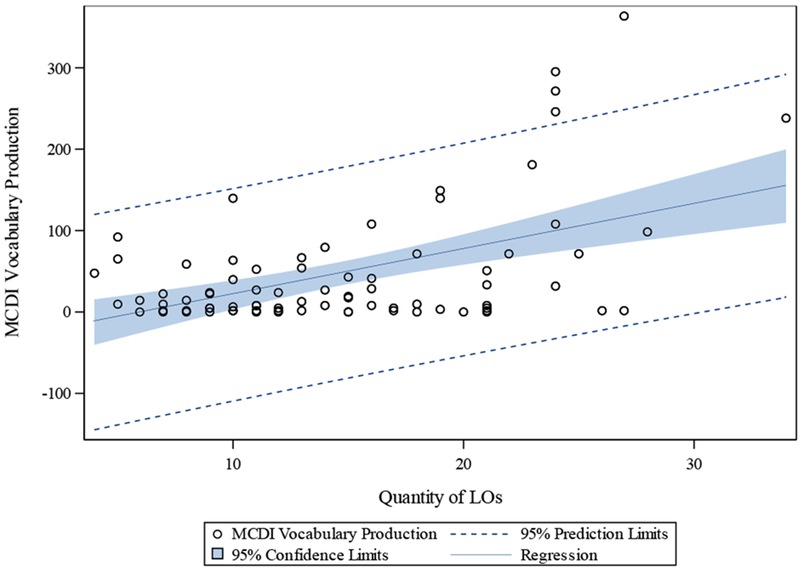
Relationship between quantity of learning opportunities and MCDI vocabulary production
Discussion
The primary aims of this study were to develop a micro-analytic coding system to identify learning opportunities provided by parents during play with their children, assess the psychometric properties of the coding system, and use it to examine the relationship between variation in the quantity of learning opportunities that parents provided to their young children with ASD and the performance of those children on tests of cognition, ASD symptoms, and language. The coding system was applied to videotaped interactions of parents interacting with their young children with ASD to quantify parent-provided learning opportunities. Results indicated that the coding system may be psychometrically sound, as it demonstrated moderate (r = 0.521, n = 37, p < .01) split-half reliability and adequate (r = 0.420, n = 158, p < .001) convergent/concurrent validity. Furthermore, the quantity of learning opportunities that parents provided during play was found to be moderately and significantly associated with the cognitive and language performance of children with ASD 12 weeks later.
Examination of split-half reliability indicated that quantity of learning opportunities provided is likely a relatively stable aspect of a parent’s interaction style, at least in the short-term and in a specific context, and that the 3 minute sample utilized for current study was an appropriate and meaningful amount of observational time. It should be noted that for the current study, interactions were coded solely based on time, and moments of downtime (e.g., transitions between interactive activities, child fussing, breaks for snacks) frequently occurred in coded minutes. Although the learning opportunity coding system was designed to capture teaching moments within all of these moments, it is likely that active, engaged, highly interactive play activities are more likely to be rich with learning opportunities. Coding solely by time and including these moments of downtime, thus, serves as a rigorous test of stability.
Learning opportunities scores correlated moderately (Cicchetti, 1994) with scores on the ESDM Teaching Fidelity Rating System, suggesting that the two coding systems, both designed to code parent behavior during interactions with children, are assessing a similar construct. Although the two coding systems are related, they differ in several important dimensions and capture different aspects of parent-child interaction. Fidelity scores examine interaction on a broader scale and contain both items theoretically included within learning opportunities (e.g., quality of behavioral teaching techniques) and those not specifically included within learning opportunities (e.g., adult language). In contrast, the learning opportunities coding system captures facets of parent-child interaction that are not reflected within fidelity coding, including examinations of interaction during “downtime” between active engagement in activities, specific frequencies of teaching episodes, and detailed information regarding parent delivery of learning opportunities and parent response to each spontaneous behavior of the child. Thus, both measures may be useful to include in future studies.
Results showed that the quantity of learning opportunities was moderately and significantly (Cicchetti, 1994) associated with children’s scores across 12 weeks on 5 of the 10 variables examined, even after controlling for early intervention and children’s initial developmental quotient, as appropriate. Quantity of learning opportunities was significantly related to child cognition (average, nonverbal, and verbal) and language (vocabulary comprehension and production). Quantity of learning opportunities was not significantly associated with ASD symptoms as measured by the ADOS. This is not surprising, given that this measure is qualitatively different from the others examined, as it is not designed to capture change, especially subtle change in child skills or symptoms, over time (Grzadzinski et al., 2016).
One interesting outcome of this portion of the analysis involves the lack of significance of the early intervention covariate with quantity of learning opportunities as the primary independent variable in the models. Although only a few studies have supported the effect of a specific number of hours on outcomes, the extant literature extensively supports the importance of early intervention in optimizing the development of young children with ASD. In fact, a study examining the same sample used for this study (Rogers et al., 2012) found that number of hours of early intervention was associated with greater child progress. The fact that, in these analyses, early intervention hours did not explain a significant amount of variance when quantity of learning opportunities was the primary independent variable indicates that in addition to the effects of early intervention, quantity of parent-provided learning opportunities is an important contributor to child performance, especially at very young ages. It is also important to note that the impact of parent-delivered learning opportunities in this study is in a context of very few hours per week of intervention being provided at study entry. Parents are extensively involved in toddler care and spend many hours with their children as compared to community interventionists. In addition, the quality of all intervention services being received was unknown, possibly impacting the result seen. Regardless, this data suggests the importance of parent-delivered learning opportunities and parent involvement in early intervention services. Both high-quality early intervention and high-quality parent-child interaction are likely to be important contributors to child outcomes.
Limitations of this research include the fact that it utilized a new measurement approach that will require further use and replication to assess its utility and reliability. In addition, the sample size was limited by the larger study, and future research would likely benefit from larger samples. There is a need to assess the ecological validity of this measurement approach by examining whether the parent-child interaction as observed in the laboratory was representative of that which occurred on a more regular basis at home.
Future research using the coding system developed for this study may help to address some of these limitations as well as yield needed information. A next logical step in this line of research may be to evaluate the change in provision of learning opportunities over time, especially in the context of parent coaching which is designed to alter these interactions. Another area of examination involves separating out child- versus parent-initiated learning opportunities, and assessing whether they contribute differentially to child performance. In addition, an examination of the effects of parental characteristics (e.g., education level, learning style, number of children, parental mental health, stress, and resources) on provision of learning opportunities will be helpful for understanding variables affecting this dimension of parenting behavior. Furthermore, although other types of parenting variables (e.g., parental sensitivity) were considered throughout the development of the coding system, it will be helpful for future studies to tease apart the effects of various aspects of parent behavior on child learning rates in order for parent-implemented interventions to identify the most powerful behaviors that parents have for helping their children progress. Similarly, an examination of the similarities and differences between learning opportunity provision and results of other, more commonly-used measures within ASD research (e.g., joint engagement coding [Adamson et al., 2012] and the Brief Observation of Social Communication Change [BOSCC; Grzadzinski et al., 2016]), could be enlightening in terms of understanding the most ideal approach to assessing parent-child and assessor-child interaction and their effects on child learning and development. Finally, the direction of the association found in this study cannot be determined. It is possible that children with higher scores on the outcome measures may be easier to interact with, making it easier for parents to provide learning opportunities to them. Future research, then, examining learning opportunity provision and child progress across time may help to clarify the nature and direction of this association. Regardless of the direction of the association, the finding of an association between the learning opportunities that parents provide during naturalistic interactions with their children and the children’s levels of cognitive and language ability 12 weeks later calls for more research to explore the implications of these findings for optimizing children’s developmental outcomes.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
This research was funded by Autism Speaks grants (A.E., S.R.) and by the National Institute of Mental Health (NIMH)/the National Institute of Child Health and Human Development (NICHD) grant MH R01 081757 (S.R.). The authors acknowledge the time and effort of the families involved in this study, Megan Manternach and Dr. Maria Fusaro for their help with video coding, Dr. Catherine Lord for her helpful comments on the research, and Dr. Scott Compton for his helpful comments regarding statistics.
This manuscript is based on the doctoral dissertation of Katherine S. Davlantis.
Contributor Information
Katherine S. Davlantis, Medical Investigation of Neurodevelopmental Disorders (MIND) Institute, Department of Psychiatry and Behavioral Sciences, University of California, Davis Medical Center; now at Woodbridge Autism Center, PLLC
Annette Estes, Department of Speech and Hearing Sciences, University of Washington.
Geraldine Dawson, Duke Center for Autism and Brain Development, Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine.
Sally J. Rogers, Medical Investigation of Neurodevelopmental Disorders (MIND) Institute, Department of Psychiatry and Behavioral Sciences, University of California, Davis Medical Center
References
- Adamson LB, Bakeman R, Deckner DF, & Nelson PB (2012). Rating parent-child interactions: Joint engagement, communication dynamics, and shared topics in autism, Down syndrome, and typical development. Journal of Autism and Developmental Disorders, 42(12), 2622–2635. doi: 10.1007/s10803-012-1520-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Albers AE, & Greer RD (1991). Is the three-term contingency trial a predictor of effective communication? Journal of Behavioral Education, 1(3), 337–354. doi: 10.1007/BF00947188 [DOI] [Google Scholar]
- Aldred C, Green J, & Adams C (2004). A new social communication intervention for children with autism: pilot randomised controlled treatment study suggesting effectiveness. Journal of Child Psychology and Psychiatry, 45(8), 1420–1430. doi: 10.1111/j.1469-7610.2004.00338.x [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders(5th ed.). Arlington, VA: Author. [Google Scholar]
- Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z, Dowling NF (2018). Prevalence of autism spectrum disorder among children aged 8 years - autism and developmental disabilities monitoring network, 11 sites, United States, 2014. Morbidity and Mortality Weekly Report Surveillance Summaries, 67(6), 1–23. doi: 10.15585/mmwr.ss6706a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baker JK, Messinger DS, Lyons KK, & Grantz CJ (2010). A pilot study of maternal sensitivity in the context of emergent autism. Journal of Autism and Developmental Disorders, 40, 988–999. doi: 10.1007/s10803-010-0948-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carter AS, Messinger DS, Stone WL, Celimli S, Nahmias AS, & Yoder P (2011). A randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. Journal of Child Psychology and Psychiatry, 52(7), 741–752. doi: 10.1111/j.1469-7610.2011.02395.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charman T, Drew A, Baird C, & Baird G (2003). Measuring early language development in preschool children with autism spectrum disorder using the MacArthur Communicative Development Inventory (Infant Form). Journal of Child Language, 30, 213–236. doi: 10.1017/S0305000902005482 [DOI] [PubMed] [Google Scholar]
- Cicchetti DV (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6(4), 284–290. doi: 10.1037/1040-3590.6.4.284 [DOI] [Google Scholar]
- Cooper JO, Heron TE, & Heward WL (2006). Applied behavior analysis (2nd ed.). Upper Saddle River, NJ: Prentice-Hall. [Google Scholar]
- Dawson G (2008). Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorders. Development and Psychopathology, 20, 775–803. doi: 10.1017/S0954579408000370 [DOI] [PubMed] [Google Scholar]
- Dawson G, & Bernier R (2013). A quarter century of progress on the early detection and reatment of autism spectrum disorder. Developmental Psychopathology, 25(4), 1455–1472. doi: 10.1017/S0954579413000710 [DOI] [PubMed] [Google Scholar]
- Dawson G, Rogers SJ, Munson J, Smith M, Winter J, Greenson J, …Varley J (2010).Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics, 125, e17–e23. doi: 10.1542/peds.2009-0958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawson G, & Zanolli K (2003). Early intervention and brain plasticity in autism In Rutter M (Ed.), Autism: Neural bases and treatment possibilities (pp. 266–274). London: Novartis. [PubMed] [Google Scholar]
- Fenson L, Marchman VA, Thal DJ, Dale PS, Rezick JS, & Bates E (2007). MacArthur-Bates Communicative Development Inventories. Baltimore, MD: Paul H. Brookes Publishing Co. [Google Scholar]
- Flippin M, & Watson LR (2011). Relationships between the responsiveness of fathers and mothers and the object play skills of children with autism spectrum disorders. Journal of Early Intervention, 33(3), 220–234. doi: 10.1177/1053815111427445 [DOI] [Google Scholar]
- Gotham K, Risi S, Pickles A, & Lord C (2007). The Autism Diagnostic Observation Schedule: Revised algorithms for improved diagnostic validity. Journal of Autism and Developmental Disorders, 37(4), 613–627. doi: 10.1007/s10803-006-0280-1 [DOI] [PubMed] [Google Scholar]
- Grzadzinski R, Carr T, Colombi C, McGuire K, Dufek S, Pickles A, & Lord C (2016). Measuring changes in social communication behaviors: Preliminary development of the Brief Observation of Social Communication Change (BOSCC). Journal of Autism and Developmental Disorders, 46(7), 2464–2479. doi: 10.1007/s10803-016-2782-9 [DOI] [PubMed] [Google Scholar]
- Kandel ER (2006). In Search of Memory: The Emergence of a New Science of Mind. New York, NY: W. W. Norton & Company, Inc. [Google Scholar]
- Lohaus A, Keller H, Ball J, Voelker S, & Elben C (2004). Maternal sensitivity in interactions with three- and 12-month-old infants: Stability, structural composition, and developmental consequences. Infant and Child Development, 13, 235–252. doi: 10.1002/icd.351 [DOI] [Google Scholar]
- Lord C, Risi S, Lambrecht L, Cook EH, Leventhal BL, DiLavore PC, …Rutter M (2000). The Autism Diagnostic Observation Schedule—Generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223. doi: 10.1023/A:1005592401947 [DOI] [PubMed] [Google Scholar]
- Lord C, Rutter M, DiLavore PC, & Risi S (2003). Autism Diagnostic Observation Schedule. Torrance, CA: Western Psychological Services. [Google Scholar]
- Lovaas OI (2002). Teaching individuals with developmental delays: Basic intervention techniques. Austin, TX: PRO-ED. [Google Scholar]
- Luyster RJ, Kadlec MB, Carter A, & Tager-Flusberg H (2008). Language assessment and development in toddlers with autism spectrum disorders. Journal of Autism and Developmental Disorders, 38, 1426–1438. doi: 10.1007/s10803-007-0510-1 [DOI] [PubMed] [Google Scholar]
- McDuffie A, & Yoder P (2010). Types of parent verbal responsiveness that predict language in young children with autism spectrum disorder. Journal of Speech, Language, and Hearing Research, 53, 1026–1039. doi: 10.1044/1092-4388(2009/09-0023) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mullen E (1989). Mullen scales of early learning. Cranston, RI: T.O.T.A.L. Child, Inc. [Google Scholar]
- Mundy P, & Neal AR (2001). Neural plasticity, joint attention, and a transactional social-orienting model of autism. International Review of Research in Mental Retardation, 23, 139–168. [Google Scholar]
- Oosterling I, Visser J, Swinkels S, Rommelse N, Donders R, Woudenberg T, Buitelaar J (2010). Randomized controlled trial of the Focus Parent Training for toddlers with autism: 1-year outcome. Journal of Autism and Developmental Disorders, 40, 1447–1458. doi: 10.1007/s10803-010-1004-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pickles A, Le Couteur A, Leadbitter K, Salomone E, Cole-Fletcher R, Tobin H, Green J (2016). Parent-mediated social communication therapy for young children with autism (PACT): long-term follow-up of a randomised controlled trial. Lancet, 388, 2501–2509. doi: 10.1016/S0140-6736(16)31229-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins DL, Fein D, & Barton ML (1999). Modified Checklist for Autism in Toddlers: self-published.
- Rogers SJ, & Dawson G (2010). Early Start Denver Model for young children with autism: promoting language, learning, and engagement. New York: The Guilford Press. [Google Scholar]
- Rogers SJ, Estes A, Lord C, Vismara L, Winter J, Fitzpatrick A, …Dawson G (2012). Effects of a brief Early Start Denver Model (ESDM)-based parent intervention on toddlers at risk for autism spectrum disorders: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1052–1065. doi: https://vpn.lib.ucdavis.edu/,DanaInfo=dx.doi.org+10.1016/j.jaac.2012.08.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schreibman L, Dawson G, Stahmer AC, Landa R, Rogers SJ, McGee GG, Halladay A (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45, 2411–2428. doi: 10.1007/s10803-015-2407-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siller M, & Sigman M (2002). The behaviors of parents of children with autism predict the subsequent development of their children’s communication. Journal of Autism and Developmental Disorders, 32(2), 77–89. doi: 10.1023/A:1014884404276 [DOI] [PubMed] [Google Scholar]
- Siller M, & Sigman M (2008). Modeling longitudinal change in the language abilities of children with autism: Parent behaviors and child characteristics as predictors of change. Developmental Psychology, 44(6), 1691–1704. doi: 10.1037/a0013771 [DOI] [PubMed] [Google Scholar]
- Sutherland KS, & Wehby JH (2001). Exploring the relationship between increased opportunities to respond to academic requests and the academic and behavioral outcomes of students with EBD: A review. Remedial and Special Education, 22, 113–121. doi: 10.1177/074193250102200205 [DOI] [Google Scholar]
- Swineford LB, Guthrie W, & Thurm A (2015). Convergent and divergent validity of the Mullen Scales of Early Learning in young children with and without autism spectrumdisorder. Psychological Assessment, 27(4), 1364–1378. doi: 10.1037/pas0000116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swinkels SHN, Dietz C, van Daalen E, Kerkhof IHGM, van Engeland H, & Buitelaar JK (2006). Screening for autistic spectrum in children aged 14 to15 months. I: The development of the Early Screening of Autistic Traits Questionnaire (ESAT). Journal of Autism and Developmental Disorders, 36(6), 723–732. doi: 10.1007/s10803-006-0115-0 [DOI] [PubMed] [Google Scholar]
- Warren SF, Fey ME, & Yoder PJ (2007). Differential treatment intensity research: Amissing link to creating optimally effective communication interventions. MentalRetardation and Developmental Disabilities, 13, 70–77. doi: 10.1002/mrdd [DOI] [PubMed] [Google Scholar]
- Wetherby A, & Prizant B (2002). Communication and Symbolic Behavior Scales Developmental Profile, First Normed Edition. Baltimore, MD: Paul H. Brookes. [Google Scholar]
- Yoder PJ, & Warren SF (2002). Effects of prelinguistic milieu teaching and parent responsivity education on dyads involving children with intellectual disabilities. Journal of Speech, Language, and Hearing Research, 45, 1158–1174. doi: 10.1044/1092-4388(2002/094) [DOI] [PubMed] [Google Scholar]