

Abstract
Objective
The purpose of this study was to investigate the effect of changes in overtime work hours on depressive symptoms among Japanese white‐collar workers.
Methods
Participant data were collected from a company's annual mental health survey in June 2013 and June 2014. The participants comprised 922 workers who responded to the survey in both the years and had records of monthly working hours in the past 2 years. We obtained information on monthly working hours from personnel records from June 2012 to May 2014. Depressive symptoms were measured by the Brief Job Stress Questionnaire. Changes in overtime work hours were measured by creating a five‐category variable for each monthly average of overtime work hours in the past year: (a) stable short, (b) decreased, (c) stable medium, (d) increased, and (e) stable long groups. Analysis of covariance was conducted to estimate the degree of depressive symptoms of each group for changes in overtime work hours.
Results
Significant differences among the groups were observed (F = 3.67, P = 0.006). In the Bonferroni multiple comparison test, significantly lower depressive symptoms were observed in the decreased group (point estimate = 9.56) compared to the stable short (10.76), stable medium (10.71), and increased groups (10.99). There was no significant difference between the decreased group and the stable long group (10.98).
Conclusions
A decrease in overtime work hours may prevent the deterioration of mental health. This knowledge could support the necessity of mental health measures through decreasing overtime work hours proposed by national policy in Japan.
Keywords: depressive symptoms, Japan, longitudinal studies, overtime work hours, work style reform
1. INTRODUCTION
The effect of overtime work hours on employees' physical and mental health has been a social problem in Japan for several decades, as evidenced by the words “Karoshi” (ie, death from overwork) and “Karojisatsu” (ie, suicide induced by overwork). Given these circumstances, the Japanese government is taking measures to reduce overtime work hours. For example, a law to promote measures to prevent death or suicide from overwork, “the Act to Accelerate Moves for the Prevention of Karoshi and Other Overwork‐Related Health Disorders” was legislated in 2014. In addition, the reduction of overtime work hours was included as an important item in “The Action Plan for the Realization of Work Style Reform” enacted by the Prime Minister of Japan, who is the chairman of the Council for the Realization of Work Style Reform, in 2017, and more recently, “The Act on the Arrangement of Related Acts to Promote Work Style Reform” was enacted in 2018.
Preceding studies have revealed the association of overtime work hours with physical health1 and the mechanisms underlying it.1 On the other hand, the association of overtime work hours with mental health has been inconsistent and inconclusive.2 Among seven longitudinal studies on the association of overtime work hours with doctor‐diagnosed depression which were systematically reviewed and meta‐analysed by Watanabe et al,2 only one study showed the significant association of overtime work hours with doctor‐diagnosed depression in women but not in men3; the other six studies failed to show the significant association4, 5, 6, 7, 8, 9 and the result of the meta‐analysis was not significant.2
This inconclusive evidence may be caused by an uncertain measurement of the working hours because of using self‐administered questionnaires or personal interviews in preceding studies.10 To date, only three cross‐sectional studies and one longitudinal study have investigated the association of objectively measured overtime work hours from personnel records with self‐reported psychological distress.6, 11, 12, 13 Furthermore, in the longitudinal studies meta‐analysed by Watanabe et al2 introduced above, overtime work hours were assessed only at a single point in time (ie, baseline), even though the working hours may change over time, which could also be considered as the cause of the uncertain results.
To address these limitations, the purpose of this study was to investigate the effect of changes in objectively measured overtime work hours obtained from personnel records on depressive symptoms among Japanese white‐collar workers through a 2‐year longitudinal study. We hypothesized that workers with decreased or stable short overtime work hours would experience lower levels of depressive symptoms than others (ie, increased, stable medium, or stable long overtime work hours).
2. METHODS
2.1. Participants
Data from the participants were collected from an annual mental health survey conducted among workers in a manufacturing company in Japan in June 2013 and June 2014. Responses to all questions were given on the participants' personal workplace computers, and unless all the responses to the questions were completed, they could not proceed to the next question.
At baseline (June 2013), 1321 workers were enrolled in the company, 1237 of whom responded to the survey (response rate = 93.6%). Of the 1237 workers at baseline, 1081 workers responded to the survey at follow‐up (June 2014) (follow‐up rate = 87.4%). Of these 1,081 workers, data obtained from the personnel records of 922 workers regarding their monthly working hours in the past 2 years from June 2014 were analyzed. The demographic and occupational characteristics of participants are shown in Table 1.
Table 1.
Demographic and occupational characteristics, job stressors and social supports, and depressive symptoms scores of participants
| Total (N = 922) | |||
|---|---|---|---|
| Mean (SD) | n (%) | Cronbach's α | |
| Baseline | |||
| Gender | |||
| Men | 820 (88.9) | ||
| Women | 102 (11.1) | ||
| Age | |||
| 20‐29 years old | 58 (6.3) | ||
| 30‐39 years old | 544 (59.0) | ||
| 40‐49 years old | 258 (28.0) | ||
| 50 years old or more | 62 (6.7) | ||
| Employment position | |||
| Manager | 88 (9.5) | ||
| Regular Employee | 834 (90.5) | ||
| Overtime work hours (monthly average) | 39.1 (22.4) | ||
| 44 h or less | 577 (62.6) | ||
| 45‐79 h | 305 (33.1) | ||
| 80 h or more | 40 (4.3) | ||
| Job stressors and social supports (BJSQ) | |||
| Job demands | 8.8 (2.0) | 0.82 | |
| Job control | 8.2 (1.7) | 0.69 | |
| Supervisor support | 7.5 (2.0) | 0.85 | |
| Coworker support | 7.7 (1.9) | 0.82 | |
| Depressive symptoms (BJSQ) | 10.8 (3.7) | 0.88 | |
| Follow‐up | |||
| Overtime work hours (monthly average) | 42.9 (24.6) | ||
| 44 h or less | 512 (55.5) | ||
| 45‐79 h | 333 (36.1) | ||
| 80 h or more | 77 (8.4) | ||
| Depressive symptoms (BJSQ) | 10.7 (3.6) | 0.88 | |
Abbreviation: BJSQ, brief job stress questionnaire.
The study's purpose and procedures were explained to the employees. Informed consent was not obtained for the secondary analysis of existing anonymous data. The Ethics Committee of Medical Research, University of Occupational and Environmental Health, Japan reviewed and approved the study procedures (No. H25‐163).
2.2. Measures
2.2.1. Changes in overtime work hours
As described above, we obtained the information on monthly working hours from the personnel records of the surveyed company from June 2012 to May 2014. Overtime work hours were defined as the total working hours over 160 hours during a month (ie, 40 hours per week × 4 weeks, which is the upper limit for working hours required by the Labor Standards Act in Japan). First, the monthly average of overtime work hours over the past year of each baseline and follow‐up survey was calculated (ie, the monthly average from June 2012 to May 2013 and from June 2013 to May 2014, respectively). Based on the monthly average of overtime work hours, the participants were classified into short (44 hours or less), medium (45‐79 hours), and long (80 hours or more) overtime groups at each time point of the survey, according to the law and the recommendation of the Ministry of Health, Labour and Welfare, Japan.14, 15
Changes in overtime work hours were measured by creating a five‐category variable for each monthly average of overtime work hours: (a) stable short group (short group at both baseline and follow‐up), (b) decreased group (medium or long group at baseline with short group at follow‐up or long group at baseline with medium group at follow‐up), (c) stable medium group (medium group at both baseline and follow‐up), (d) increased group (short group at baseline with medium or long group at follow‐up or medium group at baseline with long group at follow‐up), and (e) stable long group (long group at both baseline and follow‐up) (Figure 1).
Figure 1.
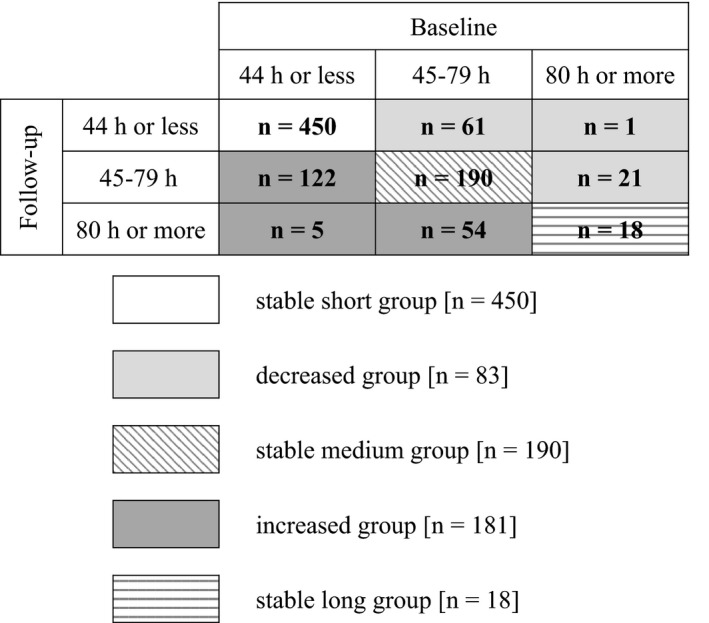
Classification of the changes in overtime work hours
2.2.2. Depressive symptoms
In this survey, depressive symptoms were measured by the Brief Job Stress Questionnaire (BJSQ),16 which is recommended for use in the Stress Check Program legislated in Japan in 2015 and is currently widely used in Japanese companies.17 The BJSQ is a 57‐item questionnaire developed based on the National Institute for Occupational Safety and Health (NIOSH) Model of Job Stress,18 and includes three aspects: job stressors, psychological and physical stress reactions, and buffering factors (ie, social supports). Depressive symptoms are one of the indices of psychological stress reactions. The BJSQ includes a six‐item scale measuring the extent of depressive symptoms during the past month with a four‐point response option from 1 = almost never to 4 = almost always (response range, 6‐24). In this sample, Cronbach's α coefficient was 0.88 at both baseline and follow‐up. Because there is no cutoff value of the scale score, it was used as a continuous variable: higher scores indicated higher levels of depressive symptoms.
2.2.3. Other covariates
Other covariates included demographic characteristics (ie, gender and age) and occupational characteristics (ie, employment position, job stressors, and social supports) at baseline.
Age was classified into four groups: 20‐29 years old, 30‐39 years old, 40‐49 years old, and 50 years old or older. Employment position was classified into two groups: manager and regular employee. Job stressors and social supports, such as scores of job demands, job control, supervisor support, and coworker support were assessed by the BJSQ introduced above. The BJSQ includes four three‐item scales: (a) the job demands scale (Cronbach's α coefficient was 0.82), (b) the job control scale (Cronbach's α coefficient was 0.69), (c) the supervisor support scale (Cronbach's α coefficient was 0.85), and (d) the coworker support scale (Cronbach's α coefficient was 0.82), each with a response range of 3‐12.
2.3. Statistical analysis
A series of analysis of covariance (ANCOVA) was conducted to estimate depressive symptoms and the standard error (SE) of changes in overtime work hours for each group. In the analyses, we first calculated the crude estimate (ie, without any adjustment) (Model 1). We then adjusted for demographic and occupational characteristics (ie, gender, age, and employment position) (Model 2); and subsequently for job control, supervisor support, and coworker support (Model 3); for job demands (Model 4); and finally for depressive symptoms at baseline (Model 5). If significant differences were observed with ANCOVA, the Bonferroni multiple comparison test was conducted. When we compared between the two groups with a Bonferroni multiple comparison test, the P values were multiplied by 10 (=5C2) because there were five independent groups. The level of significance was 0.05 (two‐tailed). Statistical analyses were performed using IBM SPSS Statistics version 22.
3. RESULTS
In the present sample, 820 men and 102 women were included. The average scores for depressive symptoms were 10.8 and 10.7 and the monthly average of overtime work hours in the past year were 39.1 hours and 42.9 hours at baseline and follow‐up, respectively (see Table 1). In the distribution of the participants’ changes in overtime work hours, 450 workers were in the stable short group, 83 in the decreased group, 190 in the stable medium group, 181 in the increased group, and 18 in the stable long group.
Table 2 shows the results of the estimated depressive symptoms scores by changes in overtime work hours. In the crude model, the estimated depressive symptoms scores of the stable short, decreased, stable medium, increased, and stable long groups were 10.59, 9.63, 10.95, 11.18, and 10.44, respectively, and significant differences among the groups were observed (Model 1). Significant differences among the groups were also observed after adjusting for demographic and occupational characteristics (Model 2), job stressors and social supports (Models 3 and 4), and depressive symptoms at baseline (Model 5) (F = 2.57‐3.67, P = 0.006‐0.037; Models 1‐5).
Table 2.
Depressive symptoms by changes in overtime work hours (Analysis of covariance (ANCOVA) was used to compare estimate scores)
| Changes in overtime work hours | n (%) | Mean (SD) | Model 1a | Model 2b |
|---|---|---|---|---|
| Estimate (SE) | Estimate (SE) | |||
| Stable short | 450 (48.8) | 10.59 (3.79) | 10.59 (0.17) | 10.64 (0.18) |
| Decreased | 83 (9.0) | 9.63 (2.79) | 9.63 (0.40)*, ** | 9.60 (0.40)*, ** |
| Stable medium | 190 (20.6) | 10.95 (3.57) | 10.95 (0.26)* | 10.90 (0.27)* |
| Increased | 181 (19.6) | 11.18 (3.52) | 11.18 (0.27)** | 11.12 (0.27)** |
| Stable long | 18 (2.0) | 10.44 (4.27) | 10.44 (0.85) | 10.32 (0.86) |
| P = 0.019 | P = 0.027 |
| Changes in overtime work hours | Model 3c | Model 4d | Model 5e |
|---|---|---|---|
| Estimate (SE) | Estimate (SE) | Estimate (SE) | |
| Stable short | 10.66 (0.17) | 10.79 (0.17)** | 10.76 (0.15)*** |
| Decreased | 9.65 (0.38)** | 9.56 (0.38)** | 9.56 (0.32)**, *** |
| Stable medium | 10.83 (0.26) | 10.68 (0.26) | 10.71 (0.22)** |
| Increased | 11.10 (0.26)** | 10.99 (0.26)** | 10.99 (0.22)*** |
| Stable long | 10.58 (0.82) | 10.31 (0.82) | 10.98 (0.70) |
| P = 0.037 | P = 0.030 | P = 0.006 |
Crude (ie, without any adjustment).
Adjusted for demographic and occupational characteristics (gender, age, and employment position).
Additionally adjusted for job control, supervisor support, and coworker support at baseline.
Additionally adjusted for job demands at baseline.
Additionally adjusted for depressive symptoms at baseline.
P < 0.10 (a marginally significant difference was observed between groups).
P < 0.05 (a significant difference was observed between groups).
P < 0.01 (a significant difference was observed between groups).
In the Bonferroni multiple comparison test, the decreased group had significantly lower depressive symptoms compared to the increased group (P = 0.012) and had marginally significant lower depressive symptoms compared to the stable medium group (P = 0.057) in the crude model (Model 1). After adjusting for demographic and occupational characteristics, job stressors and social supports, and depressive symptoms at baseline (Model 5), significantly lower depressive symptoms were observed in the decreased group compared to the stable short (P = 0.009), stable medium (P = 0.03), and increased groups (P = 0.002). There was no significant difference between the decreased group and the stable long group (P = 0.64).
4. DISCUSSION
This study demonstrated that workers with decreased overtime work hours experienced lower levels of depressive symptoms compared to the other overtime work hours groups. Compared to the stable short, stable medium, and increased overtime work hours groups, depressive symptoms were significantly lower in the decreased group. On the other hand, there were no significant differences among the other groups.
In this study, the workers with decreased overtime work hours had the lowest average depressive symptoms score (9.56) and statistically significant differences were observed compared to the stable medium and increased groups. Although not measuring changes in overtime work hours, preceding studies have reported that workers with short overtime work hours are less likely to experience psychological distress than those with long overtime work hours,11, 12 which partially supports our findings. As a reason for our findings and preceding ones, workers engaging in long working hours would experience poor quality and quantity of sleep, fatigue, and disruption of family and social activities,19 which are important determinants of mental health.20 In other words, workers with decreased overtime work hours may have increases in the time spent sleeping, recovery from fatigue, and family and social activities compared to stable medium or increased overtime work hours groups in this study, which may lead to lower levels of depressive symptoms among the decreased group. In the European Union (EU), at least an 11‐hour daily rest period (DRP: rest taken from daily work during a 24‐hour period, including sleep duration, leisure time, and commuting time) is stipulated in the EU's Working Time Directive.21 Because the DRP is necessary for a worker to recover from physical and mental exhaustion, decreasing overtime work hours may lead to securing a sufficient DRP and prevent adverse effects on mental health.
Contrary to our hypothesis, the stable short group had significantly higher depressive symptoms than the decreased group. There are two ways to interpret this result. First, the workers with decreased overtime work hours may have realized the favorable exposure change (ie, decreased overtime work hours), which influenced subjective depressive symptoms strongly. Second, we need to interpret this result carefully, because some participants who may have already suffered from mental health problems may be in the stable short group. Workers who have had mental health problems may be unable to work for a long time and/or received a workplace consideration (eg, prohibition of overtime work or transfer to a low workload position). If we had obtained information about the previous history of psychiatric disease or workplace considerations, we could have eliminated this influence.
There was no significant difference between the stable long group and other groups, including the decreased group, although the stable long group had a high depressive symptoms' score (10.98). Due to the small sample size (n = 18), a large variation in depressive symptoms scores in the stable long group occurred (SE = 0.70) and a statistically significant difference was not observed.
Our study has several strengths. Foremost, this is the first longitudinal study investigating the effect of changes in overtime work hours on depressive symptoms. Almost all the preceding studies on the association of overtime work hours with mental health measured the overtime work hours only once, such as baseline. Our longitudinal study considered exposure change over the years. Second, the response rate in this study was relatively high compared to other studies, which might diminish the effect of selection bias. Third, we obtained the information on monthly working hours from personnel records. As we mentioned earlier, most studies on the association of overtime work hours with mental health used self‐administered questionnaires or personal interviews.10 Although it is possible that the participants worked undeclared overtime (ie, took their work home or worked after clocking out), using personnel records is the most appropriate way to measure overtime work hours at present.10 We could investigate this association accurately using objectively measured working hours.
On the other hand, some possible limitations should be considered. First, all the participants in this study were white‐collar workers belonging to a single large company in Japan. They could obtain sufficient welfare benefits and were stably employed; therefore, generalizing the findings should be done with caution. Second, we surveyed only the participants who had been able to continue to work at the surveyed company over a 2‐year period. The workers with stable long or increased overtime work hours may have been more likely to take a leave of absence or leave the company due to physical or mental health problems during the surveyed period. There is a possibility that the effects were underestimated because of selection bias. Third, although we adjusted for gender as a covariate in the statistical model, our findings may not be applicable to women because almost all (88.9%) of the participants in this survey were men (see Table 1). Therefore, our findings should be replicated using a large sample of female employees in the future. Fourth, as described before, we could not obtain information about the previous history of psychiatric disease or workplace considerations. Considering this personal information would make the association clearer in the future. Fifth, we assessed depressive symptoms with the BJSQ, which is not specialized for evaluating depressive symptoms. Using validated questionnaires specialized for evaluating depressive symptoms, such as the Self‐Rating Depression Scale (SDS)22 or the Center for Epidemiologic Studies Depression (CES‐D)23 Scale, would have assessed the severity of depressive symptoms more precisely. In addition, the outcome of the present study is depressive symptoms, which are popular measures of mental health but not necessarily related to clinically significant mental health impairment. To provide more concrete evidence for the association of changes in overtime work hours with mental health among employees, research focusing on more severe mental health outcomes, such as major depressive disorders diagnosed by the International Statistical Classification of Diseases and Related Health Problems (ICD)24 or the Diagnostic and Statistical Manual of Mental Disorders (DSM),25 needs to be conducted. Sixth, although we discussed the differences in depressive symptoms among each group for changes in overtime work hours based on statistical significance, the differences were quite small. Therefore, we could not conclude that the differences in depressive symptoms observed in this study were practically significant. Seventh, although we assessed changes in overtime work hours using the monthly average of overtime work hours in the past year, we could not consider the detailed changes in monthly overtime work hours. For example, working short overtime work hours for longer periods (eg, 20 hours per month for 12 consecutive months) may have different effects on depressive symptoms compared to working long overtime work hours for shorter periods (eg, 80 hours per month for three consecutive months). Therefore, in future research, light should be shed on the detailed changes in monthly overtime work hours. Eighth, there were fewer participants who continued to work long overtime work hours (ie, stable long group) than the other overtime work hours groups. In the stable long group, the SE of the depressive symptoms score was large, which might have yielded a less accurate estimation of the depressive symptoms score. To increase the accuracy of estimation, we should invite a larger number of participants by asking multiple companies. Ninth, we could not get the reason for the changes in overtime work hours. There is a possibility that the reasons for the changes in overtime work hours were varied; for example, in the decreased group, a natural decline in workload, making efforts to reduce overtime, or being unable to work due to illness. In future, we should research the reasons for changes in overtime work hours. Tenth, since we could not consider the amount of changes in overtime work hours, it may occur as misclassification of overtime work hours categorization. Specifically, people in the boundary area (ie, around 44/45 hours or 79/80 hours) at baseline may change their overtime work hours categories by slightly changed at follow‐up. Finally, we could not assess some covariates. For example, residence, marital, and educational status may affect the association of overtime work hours with depressive symptoms. Future research should consider the effects of some covariation on the present findings.
To the best of our knowledge, this is the first study to investigate the effect of changes in overtime work hours on depressive symptoms through longitudinal design. In conclusion, a decrease in overtime work hours may prevent the deterioration of mental health. This knowledge could support the necessity of workplace mental health measures through decreasing overtime work hours proposed by a national policy in Japan.
DISCLOSURE
Approval of the research protocol: The Ethics Committee of Medical Research, University of Occupational and Environmental Health, Japan reviewed and approved the research procedures (No. H25‐163). Informed consent: Informed consent was not obtained for the secondary analysis of existing anonymous data. Registry and the registration no. of the study/Trial: N/A. Animal studies: N/A. Conflict of interest: Authors declare no Conflict of Interests for this article.
AUTHOR CONTRIBUTIONS
A.H. and A.I. conceptualized and designed the study; A.H. recruited participants and collected data; A.H., A.I., and K.M. analyzed and interpreted the data; A.H led the writing; A.I., K.M., and H.H. critically reviewed the manuscript; A.H., A.I., K.M., and H.H. approved the final version of the manuscript, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
ACKNOWLEDGMENT
This study was partially supported by UOEH Research Grant for Promotion of Occupational Health.
Hino A, Inoue A, Mafune K, Hiro H. The effect of changes in overtime work hours on depressive symptoms among Japanese white‐collar workers: A 2‐year follow‐up study. J Occup Health. 2019;61:320–327. 10.1002/1348-9585.12054
REFERENCES
- 1. Bannai A, Tamakoshi A. The association between long working hours and health: a systematic review of epidemiological evidence. Scand J Work Environ Health. 2014;40:5‐18. [DOI] [PubMed] [Google Scholar]
- 2. Watanabe K, Imamura K, Kawakami N. Working hours and the onset of depressive disorder: a systematic review and meta‐analysis. Occup Environ Med. 2016;73:877‐884. [DOI] [PubMed] [Google Scholar]
- 3. Shields M. Long working hours and health. Health Rep. 1999;11:33‐48. [PubMed] [Google Scholar]
- 4. Kawakami N, Araki S, Kawashima M. Effects of job stress on occurrence of major depression in Japanese industry: a case‐control study nested in a cohort study. J Occup Med. 1990;32:722‐725. [PubMed] [Google Scholar]
- 5. Kawakami N. Effects of overwork on sick leave due to mental disorders and the onset of ischemic heart disease and cerebrovascular disease: the JSTRESS Study In: Kawakami N, ed. Health and Labour Sciences Research Grants for Research on Occupational Safety and Health on Assessment of Stress Burden due to Overwork among Workers, FY 2009 report. Tokyo, Japan: Tokuyo University; 2010:10‐20. (in Japanese). [Google Scholar]
- 6. Ogasawara K, Nakamura Y, Aleksic B, et al. Depression associated with alcohol intake and younger age in Japanese office workers: a case‐control and a cohort study. J Affect Disord. 2011;128:33‐40. [DOI] [PubMed] [Google Scholar]
- 7. Virtanen M, Stansfeld SA, Fuhrer R, et al. Overtime work as a predictor of major depressive episode: a 5‐year follow‐up of the Whitehall II study. PLoS ONE. 2012;7:e30719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wang J, Patten SB, Currie S, Sareen J, Schmitz N. A population‐based longitudinal study on work environmental factors and the risk of major depressive disorder. Am J Epidemiol. 2012;176:52‐59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Niedhammer I, Malard L, Chastang JF. Occupational factors and subsequent major depressive and generalized anxiety disorders in the prospective French national SIP study. BMC Public Health. 2015;15:200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Fujino Y, Horie S, Hoshuyama T, et al. A systematic review of working hours and mental health burden. Sangyo Eiseigaku Zasshi. 2006;48:87‐97. [DOI] [PubMed] [Google Scholar]
- 11. Hino A, Inoue A, Kawakami N, et al. Buffering effects of job resources on the association of overtime work hours with psychological distress in Japanese white‐collar workers. Int Arch Occup Environ Health. 2015;88:631‐640. [DOI] [PubMed] [Google Scholar]
- 12. Nishikitani M, Nakao M, Karita K, Nomura K, Yano E. Influence of overtime work, sleep duration, and perceived job characteristics on the physical and mental status of software engineers. Ind Health. 2005;43:623‐629. [DOI] [PubMed] [Google Scholar]
- 13. Proctor SP, White RF, Robins TG, Echeverria D, Rocskay AZ. Effect of overtime work on cognitive function in automotive workers. Scand J Work Environ Health. 1996;22:124‐132. [DOI] [PubMed] [Google Scholar]
- 14. Expert M. Study Committee on Standard for Recognition of Brain and Heart Diseases: Report by the MHLW Expert Study Committee on Standard for Recognition of Brain and Heart Diseases. Tokyo, Japan: Occupational Disease Recognition Office of the MHLW Labour Standards Bureau; 2001:86‐111. (in Japanese). [Google Scholar]
- 15. Director‐General of the Ministry of Health, Welfare Labour Standards Bureau: Comprehensive Program for the Prevention of Health Impairment due to Overwork . Labour Standards Bureau Notification No.0212001, February 12, 2002. Tokyo, Japan: MHLW Labour Standards Bureau; 2002. [Google Scholar]
- 16. Shimomitsu T, Haratani T, Nakamura K, et al. Final development of Brief Job Stress Questionnaire mainly used for assessment of the individuals In: Kato M, ed. The Ministry of Labor sponsored grant for prevention of work‐related illness, FY1999 report. Tokyo, Japan: Tokyo Medical University; 2000:126‐164. [Google Scholar]
- 17. Kawakami N, Tsutsumi A. The Stress Check Program: a new national policy for monitoring and screening psychosocial stress in the workplace in Japan. J Occup Health. 2016;58:320‐6. [DOI] [PubMed] [Google Scholar]
- 18. Hurrell JJ Jr, McLaney MA. Exposure to job stress‐a new psychometric instrument. Scand J Work Environ Health. 1988;14(Suppl 1):27‐28. [PubMed] [Google Scholar]
- 19. Marchand A, Durand P, Haines V, Harvey S. The multilevel determinants of workers' mental health: results from the SALVEO study. Soc Psychiatry Psychiatr Epidemiol. 2015;50:445‐459. [DOI] [PubMed] [Google Scholar]
- 20. Harrington JM. Health effects of shift work and extended hours of work. Occup Environ Med. 2001;58:68‐72. [Google Scholar]
- 21. EUR‐Lex . Directive 2003/88/EC of the European parliament and of the council of concerning certain aspects of the organisation of working time. Off J Eur Union. 2003; L299:9‐19. [Google Scholar]
- 22. Zung WW. A self‐rating depression scale. Arch Gen Psychiatry. 1965;12:63‐70. [DOI] [PubMed] [Google Scholar]
- 23. Radloff LS. The CES‐D Scale: A self‐report depression. Scale for research in the general population. Appl Psychol Meas. 1977;1:385‐401. [Google Scholar]
- 24. World Health Organization . Classification of diseases (ICD). https://www.who.int/classifications/icd/en/. Accessed March 3, 2019.
- 25. American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM‐5. Washington D.C. 2013. [Google Scholar]