

Abstract
Inflammatory phenomenon, including cell-free fetal DNA (cffDNA), is one of the various causes of preterm delivery. Always, there is a trend in the prediction and prevention of preterm labor. Herein, the aim of this study is to assess the value of cffDNA levels in serum of pregnant women for prediction of spontaneous preterm labor. A case–control study with nonrandomized convenience sampling was conducted. One hundred women qualifying for the study were enrolled. The participants were divided into two groups of healthy nulliparous pregnant women (n = 50) and nulliparous pregnant women experiencing preterm labor (n = 50). Then, venous blood was sampled from each participant and its plasma was separated and analyzed. The mean age of women in the experimental group was 22.90 years with the standard deviation of 4.04, while in the control group these two values were 23.78 and 4.37, respectively. In the experimental group, 29 patients (58%), and in the control group, 27 patients (54%) had cffDNA. The mean of the counted DNA in the experimental group was 2080/03 with the standard deviation of 909/792 while the same values for the control group were 1183/26 and 620/720, in the same order. The statistical analysis revealed that this difference was meaningful at P = 0.001. Furthermore, in the experimental group, cffDNA increased with increase in the age and the difference was meaningful. Finally, increasing pregnancy age in the experimental group led to an increase in the number of cffDNA (P = 0.001). The results of this study indicated that the cumulative frequency of preterm labor for women with positive cffDNA was significantly higher. High levels of cells' DNA in the serum of pregnant mothers increase the risk of spontaneous preterm labor. These observations may have implications for preterm labor.
Key words: Cell-free fetal DNA, dilatation and effacement, early preterm labor, late preterm labor, prematurity
INTRODUCTION
Despite considerable effort aimed at decreasing its incidence, preterm birth (PTB) remains the foremost cause of perinatal morbidity and mortality.[1] Annually, 15 million deliveries happen prematurely and approximately one million babies die due to complications of prematurity and screening strategies are imperfect.[2,3] Currently, multiple preventive modalities are used to prevent PTB including treatment of intrauterine infection, progesterone therapy, cerclage of the cervix, nutritional supplementations, and lifestyle modifications; however, the incidence of PTB remains high.[4]
It has been suggested that some circulating biomarkers may differ in pregnancies that experience spontaneous PTB from those delivering at term and that these differences may have predictive value.[1,5,6] In addition, it has been showed that labor is an inflammatory process, and elevated levels of inflammatory cells and pro-inflammatory agents have been found in maternal and fetal tissues during parturition. Hence, it is suggested that inflammation plays a crucial role in preterm and term labor.[7]
Cell-free fetal DNA (cffDNA) is fetal DNA which circulates freely in the maternal blood. The cffDNA is measurable in the maternal serum and increases with gestational age (GA) and its greater concentrations is found in association with some pregnancy complications.[2,8] In fact, cffDNA is a novel promising biomarker that has been used in numerous obstetrical researches, especially in prenatal diagnosis and complicated pregnancies. It is easily detectable by polymerase chain reaction tests.[9] The pro-inflammatory properties of cffDNA and its conceivable effects on pregnancy and labor are mysterious. Previous studies suggest an association between preterm labor and higher maternal serum levels of cffDNA in the second and third trimester and at onset of PTB. Along with the pro-inflammatory effects of cffDNA, its elevation with GA and during labor suggests a potential role in the pathogenesis of spontaneous PTB.[2]
Regarding the high importance of prediction and prevention of preterm labor, this study was conducted to assess the value of cffDNA levels in the serum of pregnant women for the prediction of spontaneous preterm labor.
MATERIALS AND METHODS
Study design
A case–control study with nonrandomized convenience sampling was conducted. One hundred women qualifying for the study were enrolled.
Study setting and population
The selected women were then briefed about the objectives of the study and consented to participant in the study.
The participants were divided into two groups of healthy nulliparous pregnant women and nulliparous pregnant women experiencing preterm labor. There were 50 participants in each group.
Inclusion criteria were nulliparous pregnant women with GA of <37 weeks and body mass index of between 20 and 29.9 kg/m2. Exclusion criteria were presence of any pathology in placenta including detachment, preeclampsia, or disease including diabetes mellitus, sexually transmitted diseases, or first-trimester vaginal hemorrhage (the placental health was defined according to the ultrasonography performed in the third trimester), receiving tocolytic therapy for preventing the delivery. Further, each woman in the control group who delivered before 37th week was excluded from the study.
The study was confirmed by local research committee. All participants signed the informed consent. The data were collected by bipartite questionnaire including comprehensive information about demography, interview, and complementary ultrasonography, findings of clinical examination, offspring gender, and maternal blood sample results. The venous blood (2.5 cc) was sampled from each participant and its plasma was separated. The separated and frozen plasma was then sent to the research center of Imam Khomeini Hospital for further investigation. DNA extraction was performed using Macherey-Nagel Company kit.
Data analysis
The data obtained from the used checklists along with data from the participants' blood samples were inputted into SPSS for Windows, Version16.0. SPSS inc., Chicago for statistical analysis and P < 0.05 was considered statistically significant. To analyze the data, descriptive statistical procedures including frequency counts and tables and inferential statistical techniques such as t-test and Chi-square were used.
RESULTS
The study conducted on 100 women (including 50 cases and 50 controls). The average GA was 23.84 ± 4.58 weeks in cases and 23.06 ± 4.04 weeks in controls (P = 0.369). Twenty women (40%) in cases and 19 women (38%) in controls had blood group and Rh of A+ (P < 0.05).
Twenty-nine women (58%) in cases and 27 women (54%) in controls had cffDNA (P < 0.518) [Table 1].
Table 1.
Presence or absence of cell-free fetal DNA
| Variable | Cases |
Controls |
Summation | ||
|---|---|---|---|---|---|
| 28-34 weeks | 35-37 weeks | 28-34 weeks | 35-37 weeks | ||
| Presence of DNA (%) | 14 (56) | 15 (60) | 16 (64) | 11 (44) | 56 |
| Absence of DNA (%) | 11 (44) | 10 (40) | 9 (36) | 14 (56) | 44 |
| Summation | 25 | 25 | 25 | 25 | 100 |
The average cffDNA in cases was 1570.64 ± 207.64 copy number in GA of 28–34 in comparison with 2555.47 ± 198.87 copy number in GA of 35–37 (P = 0.002). Furthermore, the average cffDNA in controls was 1109.50 ± 387.46 copy number in GA of 28–34 in comparison with 1467.36 ± 547.25 copy number in GA of 35–37 (P = 0.057). As confirmed by t-test, the GA was directly related with average serum cffDNA (P = 0.007) [Diagrams 1 and 2].
Diagram 1.
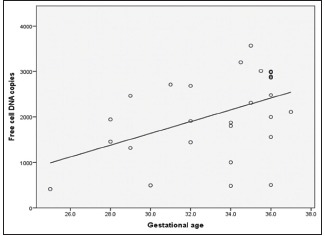
The relation with gestational age and serum cell-free fetal DNA in cases
Diagram 2.
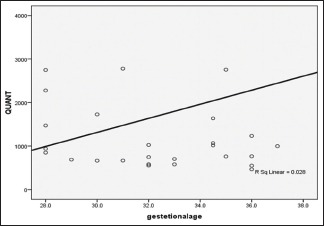
The relation with gestational age and serum cell-free fetal DNA in controls
The most specificity was in DNA level >3000 and the most sensitivity was in DNA level of 500. The comparison of specificity and sensitivity was performed to obtain a cffDNA level as an index for using in screening and diagnostic tests. The level of 1000 had acceptable specificity and sensitivity in this survey [Table 2].
Table 2.
Comparison of specificity and sensitivity according to the cell-free fetal DNA level
| DNA level | Cases |
Controls |
Sensitivity (%) | Specificity (%) | ||
|---|---|---|---|---|---|---|
| Positive | Negative | Positive | Negative | |||
| 500 | 26 | 24 | 26 | 24 | 52 | 48 |
| 1000 | 22 | 28 | 12 | 38 | 44 | 76 |
| 1500 | 18 | 32 | 8 | 42 | 36 | 84 |
| 2000 | 8 | 42 | 4 | 46 | 16 | 92 |
| 2500 | 8 | 42 | 3 | 47 | 16 | 94 |
| 3000 | 5 | 45 | 0 | 50 | 10 | 100 |
| 3500 | 3 | 47 | 0 | 50 | 6 | 100 |
DISCUSSION
We studied pregnant women to assess the value of cffDNA levels in serum of pregnant women for prediction of spontaneous preterm labor. Currently, reducing the incidence of spontaneous PTB is one of the challenges in obstetrics and gynecology wards.[4,10]
Despite the great researches and supreme efforts made for decreasing preterm labor, it remains as the leading cause of perinatal mortality and morbidity. We studied nulliparous pregnancies because women with previous prenatal loss are at higher risk of PTB.[11,12]
The difference between GA in cases and controls was not statistically significant. Further, according to the results of ANOVA test, the difference between Blood Group (BG) of Participants and Premature birth in cases and controls was not statistically significant. However, we could not find any published study comparing the BG in such patients.
Twenty-nine women (58%) in cases and 27 women (54%) in controls had cffDNA, and resemble to previous studies,[13] the difference was not significant. However, the average count of cffDNA was statistically significant between the studied groups (P = 0.001).
In a study by Leung et al., serum levels of cffDNA were significantly higher in cases than controls.[14] In addition, Farina et al. suggested that high maternal serum cffDNA is associated with an increased risk of spontaneous preterm delivery. This observation may have implications for the understanding of the mechanisms of disease that is associated with preterm labor.[15] These findings are compatible with our results.
However, Quezada et al. investigated the alteration of cffDNA in pregnant women and concluded that in the spontaneous preterm delivery groups (<34 weeks' gestation, 34–37 weeks, <37 weeks), compared to the term delivery group, there was no significant difference in cffDNA and its measurement is not predictive of spontaneous preterm delivery.[13]
We found statistically significant and direct correlation between GA and cffDNA, both in cases and controls. As gestation advances, serum cffDNA levels increase.[16] Leung et al.[14] and Dugoff et al.[17] suggested that serum levels of cffDNA were significantly higher in cases than controls and Goldfarb et al. concluded that elevated levels of cffDNA in maternal serum may initiate the labor.[18]
Women in labor have a greater serum cffDNA concentration.[16] Compatible with our findings, Farina et al. showed that the cumulative rate of early preterm delivery (GA <30 weeks) was significantly higher for women with cffDNA concentrations, and high levels of fetal cffDNA were associated with a high rate of preterm delivery.[15] Quezada et al.[13] and Illanes et al.[19] could not find any significant correlation between cffDNA and GA at delivery. They suggested that cffDNA does not reliable for the prediction of preterm labor.[13,19]
The diversity in the achieved results may be due to differences in GA or preterm labor. We assessed the correlation of maternal serum cffDNA and spontaneous preterm labor.
Limitations
This is a small study that includes only the results of one institution, and therefore, it is not necessarily representative of the nation as a whole.
CONCLUSIONS
As showed by our results, cffDNA biomarker can be used as a simple and noninvasive test for prediction of preterm labor with specificity of 46%, sensitivity of 58%, positive predictive value of 51%, and negative predictive value of 52%. However, the need for further research is highlighted.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Cantonwine DE, Zhang Z, Rosenblatt K, Goudy KS, Doss RC, Ezrin AM, et al. Evaluation of proteomic biomarkers associated with circulating microparticles as an effective means to stratify the risk of spontaneous preterm birth. Am J Obstet Gynecol. 2016;214:631.e1–11. doi: 10.1016/j.ajog.2016.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.van Boeckel SR, Davidson DJ, Norman JE, Stock SJ. Cell-free fetal DNA and spontaneous preterm birth. Reproduction. 2018;155:R137–45. doi: 10.1530/REP-17-0619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Glover AV, Manuck TA. Screening for spontaneous preterm birth and resultant therapies to reduce neonatal morbidity and mortality: A review. Semin Fetal Neonatal Med. 2018;23:126–32. doi: 10.1016/j.siny.2017.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Malouf R, Redshaw M. Specialist antenatal clinics for women at high risk of preterm birth: A systematic review of qualitative and quantitative research. BMC Pregnancy Childbirth. 2017;17:51. doi: 10.1186/s12884-017-1232-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tucker CM, Berrien K, Menard MK, Herring AH, Daniels J, Rowley DL, et al. Predicting preterm birth among women screened by north carolina's pregnancy medical home program. Matern Child Health J. 2015;19:2438–52. doi: 10.1007/s10995-015-1763-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sabour S. Prediction of spontaneous preterm delivery in women with threatened preterm labour: A prospective cohort study of multiple proteins in maternal serum. BJOG. 2012;119:1544. doi: 10.1111/j.1471-0528.2012.03487.x. [DOI] [PubMed] [Google Scholar]
- 7.Cappelletti M, Della Bella S, Ferrazzi E, Mavilio D, Divanovic S. Inflammation and preterm birth. J Leukoc Biol. 2016;99:67–78. doi: 10.1189/jlb.3MR0615-272RR. [DOI] [PubMed] [Google Scholar]
- 8.Thurik FF, Lamain-de Ruiter M, Javadi A, Kwee A, Woortmeijer H, Page-Christiaens GC, et al. Absolute first trimester cell-free DNA levels and their associations with adverse pregnancy outcomes. Prenat Diagn. 2016;36:1104–11. doi: 10.1002/pd.4940. [DOI] [PubMed] [Google Scholar]
- 9.Sifakis S, Koukou Z, Spandidos DA. Cell-free fetal DNA and pregnancy-related complications (review) Mol Med Rep. 2015;11:2367–72. doi: 10.3892/mmr.2014.3118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Stock SJ, Norman E. Management of a woman with a previous preterm birth. J Obstet Gynecol Reprod Med. 2013;20:190–5. [Google Scholar]
- 11.Cunningham F, Leveno K, Bloom S, Hauth J, Rouse D, Spong C. Williams Obstetrics. 23rd ed. USA: MacGraw-Hil; 2010. pp. 880–5. [Google Scholar]
- 12.Stock SJ, Ismail KM. Which intervention reduces the risk of preterm birth in women with risk factors? BMJ. 2016;355:i5206. doi: 10.1136/bmj.i5206. [DOI] [PubMed] [Google Scholar]
- 13.Quezada MS, Francisco C, Dumitrascu-Biris D, Nicolaides KH, Poon LC. Fetal fraction of cell-free DNA in maternal plasma in the prediction of spontaneous preterm delivery. Ultrasound Obstet Gynecol. 2015;45:101–5. doi: 10.1002/uog.14666. [DOI] [PubMed] [Google Scholar]
- 14.Leung TN, Zhang J, Lau TK, Hjelm NM, Lo YM. Maternal plasma fetal DNA as a marker for preterm labour. Lancet. 1998;352:1904–5. doi: 10.1016/S0140-6736(05)60395-9. [DOI] [PubMed] [Google Scholar]
- 15.Farina A, LeShane ES, Romero R, Gomez R, Chaiworapongsa T, Rizzo N, et al. High levels of fetal cell-free DNA in maternal serum: A risk factor for spontaneous preterm delivery. Am J Obstet Gynecol. 2005;193:421–5. doi: 10.1016/j.ajog.2004.12.023. [DOI] [PubMed] [Google Scholar]
- 16.Herrera CA, Stoerker J, Carlquist J, Stoddard GJ, Jackson M, Esplin S, et al. Cell-free DNA, inflammation, and the initiation of spontaneous term labor. Am J Obstet Gynecol. 2017;217:583.e1–8. doi: 10.1016/j.ajog.2017.05.027. [DOI] [PubMed] [Google Scholar]
- 17.Dugoff L, Barberio A, Whittaker PG, Schwartz N, Sehdev H, Bastek JA, et al. Cell-free DNA fetal fraction and preterm birth. Am J Obstet Gynecol. 2016;215:231.e1–7. doi: 10.1016/j.ajog.2016.02.009. [DOI] [PubMed] [Google Scholar]
- 18.Goldfarb I, Berk T, Phillippe M. 164: Cell-free fetal DNA like sequences stimulate innate immunity. Am J Obstet Gynecol. 2015;212:S97. [Google Scholar]
- 19.Illanes S, Gomez R, Fornes R, Figueroa-Diesel H, Schepeler M, Searovic P, et al. Free fetal DNA levels in patients at risk of preterm labour. Prenat Diagn. 2011;31:1082–5. doi: 10.1002/pd.2838. [DOI] [PubMed] [Google Scholar]