

Abstract
Background. Effective treatment methods are needed for moderate/severely impairment chronic stroke. Objective. The questions were the following: (1) Is there need for long-dose therapy or is there a mid-treatment plateau? (2) Are the observed gains from the prior-studied protocol retained after treatment? Methods. Single-blind, stratified/randomized design, with 3 applied technology treatment groups, combined with motor learning, for long-duration treatment (300 hours of treatment). Measures were Arm Motor Ability Test time and coordination-function (AMAT-T, AMAT-F, respectively), acquired pre-/posttreatment and 3-month follow-up (3moF/U); Fugl-Meyer (FM), acquired similarly with addition of mid-treatment. Findings. There was no group difference in treatment response (P ≥ .16), therefore data were combined for remaining analyses (n = 31; except for FM pre/mid/post, n = 36). Pre-to-Mid-treatment and Mid-to-Posttreatment gains of FM were statistically and clinically significant (P < .0001; 4.7 points and P < .001; 5.1 points, respectively), indicating no plateau at 150 hours and benefit of second half of treatment. From baseline to 3moF/U: (1) FM gains were twice the clinically significant benchmark, (2) AMAT-F gains were greater than clinically significant benchmark, and (3) there was statistically significant improvement in FM (P < .0001); AMAT-F (P < .0001); AMAT-T (P < .0001). These gains indicate retained clinically and statistically significant gains at 3moFU. From posttreatment to 3moF/U, gains on FM were maintained. There were statistically significant gains in AMAT-F (P = .0379) and AMAT-T P = .003.
Keywords: stroke, coordination, rehabilitation, upper limb, function
Introduction
Many stroke survivors do not fully recover upper limb function following stroke, leading to significant disability and diminished quality of life.1 Effective treatments are needed for chronic, severely impaired stroke survivors.2 Other studies showed improved upper limb motor function in chronic stroke for mild/moderately impaired,3-13 with traditional “constraint induced” treatment studies enrolling only those with preserved wrist and finger extension (acceptance rate, 10%).14 However, for those with moderate/severe impairment after stroke, improvement in function has been more difficult to realize. A recent study of constraint-induced movement therapy in more severe stroke reported no clinically significant change in upper limb Fugl-Meyer assessment scores.15 Others have also tested the application of technologies and devices, in moderately/severely impaired chronic stroke survivors, with the following: functional electrical stimulation (FES),16-18 sequenced bilateral and unilateral task orientated training,19 mirror therapy,20 progressive abduction loading therapy,21 contralaterally controlled FES,22 and robotics.23-27 Limitations included small sample size,16-18,22-23 lacking control group,16,23 lacking statistically significant gains on impairment or functional measures,23 lacking clinically significant change,20,21,23-25,27 lacking retention of clinically significant gains,16,19,25,26 or lacking study of retention.20,23 Furthermore, many studies do not include both a measure of impairment and an array of actual everyday functional tasks. Our work has focused on moderately/severely impaired chronic stroke survivors, and in prior work we developed and tested a protocol that combines technology applications and motor learning.28,29 We found clinically and statistically significant gains for those with moderate/severe stroke considerably beyond that reported by others (eg, gains in coordination, Fugl-Myer coordination scale [FM], and gains on the Arm Motor Ability Test [AMAT; 13 complex functional tasks]).
Others have cited this work stating that “a change in impairment of this magnitude was previously considered almost impossible in chronic stroke patients,”30 and that this is important first evidence for use of high dose neurorehabilitation.31 Therefore, we considered it important to replicate the administration of the upper limb motor learning protocol in a follow-on study and again quantify response. Another consideration was that we had not given technology a full chance in application to the “whole arm,” that is, both distal and proximal upper limb regions. Therefore, a first purpose was to replicate administration of the upper limb motor learning protocol and to include a treatment group that would receive technology applications to both distal and proximal limb regions. In addition, there were 2 important and unanswered questions regarding the dose and efficacy of this new treatment protocol.
The first question is whether a shorter treatment duration (ie, <300 hours) could produce the same degree of recovery, given that the existing protocol was tested in the paradigm of long-duration dose of 300 hours of therapy. Therefore, in the current work, we administered the same protocol as in prior work,28 and acquired mid-treatment (at 150 hours of treatment) data on the Fugl-Meyer impairment measure, which underlies complex functional task performance. We studied whether a mid-treatment plateau occurred or whether significant recovery occurred in response to the second half of treatment (mid-treatment to posttreatment).
The second question is whether the observed gains can be retained after cessation of treatment. Therefore, we studied retention of gains at 3 months after treatment ended.
Methods
Study Design
This was a singleblind, intervention study, stratified using standard methods, according to the following: (1) impairment level of the upper limb, in order to equalize impairment across groups and (2) relative impairment proximal/distal, so one with greater shoulder/elbow impairment would not be assigned to the group focused on distal treatment, for example. There were 3 groups, as follows: (1) distal-focused technology applications group for 30% of treatment time, (2) proximal-focused technology applications for 30% of treatment time, and (3) equal proximal and distal technology applications for 30% of time. The remaining 70% of therapy time within each of the 3 groups was spent performing functional task practice guided by motor learning principles. Functional and impairment measures were acquired by a blinded examiner at pre-, post-treatment and 3-month follow-up (3moF/U), and the FM impairment measure was acquired also at mid-treatment.
Subjects
Inclusion criteria included the following: >6 months post single unilateral stroke; ≥trace muscle contraction, of the affected wrist extensors; stable medically; no other prior neurological condition; and ability to follow 2-step commands. The institutional review board provided study oversight; subjects provided written informed consent.
Intervention
Therapy was implemented 5 hours per day (total), 5 days per week, for 12 weeks.28 Technology-assist coordination training was 1.5 hours per session, with content for each group as follows: Distal Group, FES for wrist/hand muscles (EMS + 2 [Staodyn, Inc, Longmont, CO]; Proximal Group, FES and robotics for shoulder/elbow muscles/movements (Vectra Pro (Chatanooga Group, Inc, Hixson, TN) and InMotion2 Shoulder-Elbow-Robot; InteractiveMotion Technologies, Inc, Cambridge, MA); and Whole Arm Group, equal proximal and distal applications of technology. The remainder of each session (3.5 hours/session) consisted of motor learning of coordinated movements, task component, and full task practice.28
Participants were encouraged to take short rest breaks when their motor performance degraded; therefore, rest breaks were individualized. Participants were highly motivated to work hard, but rest periods were important for productive practice to occur. Also, in the middle of the 5-hour session, we took a 1-hour lunch break, so the schedule was as follows: 2.5 hours treatment, 1-hour lunch break, and 2.5 hours of treatment. On average, participants rested about 15 minutes for every hour of participation.
From our prior work, we are aware that a 1:3 group therapy paradigm (therapist:patients) affords several advantages. First, it is less costly than the 1:1 paradigm, rendering the research more affordable. Second, participants enjoy the comradery and social aspects of the small group, and assist each other in numerous ways. Third, with 3 participants in a group, there are always 2 participants working independently (as set up by the therapist), which is preferable in terms of learning. The technologies were of some assistance, in that a participant could be set up with either FES or robotics as a practice-assist device, freeing up the therapist for that time to work more closely with another participant. The 1:3 paradigm does require that the therapist is able to hold in mind simultaneously, the detailed goals and ability levels of 3 participants and multitask throughout the entire session. Treatment planning is necessary outside of the patient treatment sessions. The successful treatment and progression are dependent on the following: accurate analysis32 of motor deficits33; insightful synthesis of multiple, broad, and related factors34 influencing motor dyscontrol35; and generalization from known experience and creativity34 in generating a customized approach to treatment planning and progression, accounting for unique arrays of symptomatology.35
Overall Principles of Treatment
The goal of training is recovery of the movement components composing functional tasks, as well as recovery of performance of the whole complex task. The motor learning protocol is based first on our clinical observations that those with moderate/severe impairment are not able to productively practice complex functional tasks at the beginning of treatment. Rather, it is important to first treat at the level of isolated joint movement coordination, if impairment is present at that level. Some31 have described this as treatment at the neurophysiological level, which was described early by Brunnstrom,36 Twitchell,37 and later by Crow and Harmeling-van der Wel.38 Krakauer and Carmichael31 recognize this accurately as different from repetition of task practice or even task component practice. We organized our treatment according to the hierarchy given in Table 1. The hierarchy begins with training isolated joint movement coordination of the scapula, shoulder, elbow, forearm, wrist, fingers, and thumb. As an individual mastered more coordinated motor control of single and/or multiple joints, we incorporated those movements into functional task components, and subsequently whole task practice. For each of these levels of training, we applied the following motor learning principles: movement practice as close to normal as possible,39,40 high number of repetitions,41-44 attention to the motor task,45 and training specificity.46 A few examples of practiced task components are reaching, grasp preparation, and grasp. In order to encourage participation, functional tasks that were meaningful to the subject were selected from an array of over 60 tasks (each of which could be divided into task components), and practiced with supplies and tools that were made readily available.
Table 1.
Upper Limb Training Protocol: Treatment Progression Hierarchy for Coordinated Movement Practice.a
| A. Muscle activation in synergy |
| B. Single joint movement in synergy |
| C. Single joint movement, out of synergy * Coordination training * Speed of movement training |
| D. Alternating joint movement (flexion and
extension) * Coordination training * Speed of movement training |
| E. Task component practice * Coordination training * Speed of movement training |
| F. Full functional task practice * Coordination training * Speed of movement training |
Table from Daly (2012) and McCabe (2015).
Accurate Selection of the Initial Task Difficulty Is Critical
Prior to assigning a motor task within the motor learning program of Table 1, performance of motor tasks was assessed for characteristics given in Table 2. The results of that assessment determined at which point in Table 1, the learner should begin for that day, for a given motor task. Progression of the motor learning program through the hierarchy of difficulty in Table 1 was dependent on iterative assessment each day and within each session, as is the case in clinical neurorehabilitation practice. We followed the maxim, “test-treat-test.”
Table 2.
Guidelines for Assigning Initial Training Level and Progression of Practice Task.
| Step | Guideline |
|---|---|
| 1 | 50% of normal range of movement is executed, volitionally, independently; or 50% of motor task is executed with support of verbal or tactile facilitation; or 50% of normal range of movement is executed, along with motor assist device. |
| 2 | Normal level of effort is expended during task (no holding breath or associative reactions in other limbs or trunk; relaxed uninvolved muscles). |
| 3 | If motor compensatory strategies are employed, at least half of motor task is performed without compensatory strategies |
| 4 | Five or more repetitions of motor task can be performed in a row with only a “beat” between before motor task deteriorates into uncoordinated or incorrect fashion. |
Example
The training provided for the task in Table 1 (point A) can serve as an example of the finely incrementalized approach used in this motor learning (ML) protocol 28. For inability to activate a given muscle in any body position, the first treatment goal is to facilitate and elicit volitional muscle activation on demand. In a severely paretic muscle, activation was first elicited within a synergistic mass pattern, because in our prior work, we found that this is the easiest condition under which to obtain volitional muscle activation. For example, we may begin with the subject in the side-lying position with the involved limb, uppermost, and supported on an exercise board in the horizontal plane. The limb can be positioned within a synergistic pattern for the “start” position. The clinician can provide minimal assistance, gradually withdrawing external manual or device assistance as soon as the individual begins to regain volitional control during practice. As the individual recovers the ability to control muscle activation in this most facilitated position, motor task practice can be progressed to more difficult body positions.
Treatment progression occurs in finely incrementalized steps. Some of the methods used to incrementally support improved performance are as follows: awareness training of normal and abnormal movements; body position to mitigate abnormal muscle tone; functional electrical stimulation to provide sensory feedback regarding muscle activation or to assist in practice of volitional movements; support of limb segments during movement practice (eg, either an overhead sling or a shoulder/elbow robot support of the upper limb); closed-chain motor practice (eg, weightbearing on palm or forearm) and open-chain motor practice; isometric, eccentric, and concentric muscle contraction practice; breakdown of meaningful tasks into separate movement components; practice of movement accuracy; speed practice; practice of variable movement directions and variable speed control; and empowerment of the individual to practice independently.47 For a number of subjects, there was abnormal soft tissue tightness, in which case tissue mobilization techniques were employed to stretch tissue to accommodate more normal active range of movement. For this, we iteratively stretched and strengthened in small increments in order to ensure maintenance of lengthened tissue. This type of treatment was routinely required for scapular/humeral tissue and recovery of more normal movement patterns. FES and robotics were used as support devices or movement-assist devices to support practice of more normal movement patterns.
Measures
We used the Fugl-Meyer Assessment (FM). A dictionary definition of coordination is as follows: “the ability to use different parts of the body together smoothly and efficiently.” This definition inherently contains a spatial and temporal component. That is, to work together, movement about joints must be occurring in a correct relative timeframe for the given movement(s). In the upper limb in some cases, this means that one joint must be stabilized and held motionless while another joint movement is executed for the given function. The FM contains items assessing coordination of upper limb movement of 4 categories as follows: (1) 15 items (46% of the score) assessing coordination of single joint movement without interference from other joint muscle activations, (2) 12 items of movement about more than one joint (36% of score), (3) trajectory movement execution (9% of the score), and (4) joint movement in response to a tap or blow (reflex response; 9% of the score).48 The FM is considered a hierarchical scale of motor coordination performance of single and multiple joints, and lays out the pattern of motor recovery set forth by Brunnstrom,36 Twitchell,37 and Crow and Harmeling-van der Wel.38 As such, the FM is the coordination impairment measure of choice for the motor learning protocol utilized here, which is based on the hierarchical progression given in Table 1. Internationally, the FM is the most widely used measure of coordination in stroke research.49 For ease of discussion, we will refer to the FM as a measure of coordination.
FM was obtained at Pre-, mid-, Post-treatment and at 3moF/U. For the most meaningful results, the FM should be used in conjunction with a measure of actual functional tasks,49 which was satisfied in the current study by AMAT, the timed domain (AMAT-T) and the “function” domain (AMAT-F). The AMAT is a reliable, valid, and homogeneous measure of 13 actual functional tasks. AMAT is a “unique standardized measure”, as a homogenous measure of complex functional tasks, indicating ADL (activities of daily living) limitation,50 compared to other measures of functional tasks that include impairment items (eg, Wolf Motor Function Test) or limit to a few movements rather than actual functional task performance (eg, Action Research Arm Test). AMAT is valid across a broad range of impairment levels50 and is strongly correlated with FM.51 AMAT time was the time to perform the tasks (AMAT-T; 13 tasks, timed/summed). The AMAT function domain (AMAT-F) is an ordinal observational coordination measure (averaged; known minimal clinically important difference for AMAT-F is 0.44 points52). Example tasks include ‘use a spoon to scoop up bean” and “unscrew jar lid”).
The Stroke Impact Scale (SIS)53 was used to assess self-report recovery in a standardized manner. We calculated the overall score and the domain scores of “Hand” and “Daily Living,” which were the most germane subscales in the current study.
We acquired qualitative therapist observational data and subject self-report data. Therapist observations of changes in impairment and functional task performance were recorded. Also, we queried the subjects during the course of their participation. We recorded answers to the question: Is there anything you can do this week that you were unable to do at the beginning of the study?
Statistical Analyses
In study measures, departures from normality were indicated by the QQ plot and Shapiro-Wilk test of normality, therefore nonparametric methods were used for analyses. To determine if differences occurred between groups, we used ordinal regression with group as the factor variable and the pre-treatment measure as a covariate. For the Fugl-Meyer coordination test, to determine whether time (baseline, mid-, posttreatment, and 3moF/U) was significant, we used the nonparametric Friedman test.54 Since time was significant, we then conducted further post hoc analysis to study change over time, using the nonparametric Wilcoxon signed rank test, and distribution free confidence intervals55 to determine statistical significance. The same procedure was employed to identify significant gain between time points in the AMAT-F, AMAT-T, and SIS measures. The Hochberg procedure was used to correct for multiple testing (only corrected P values reported).
Correlations were calculated using the Spearman method to explore the potential association between baseline impairment level (FM) and impairment improvement (FM), as well as between impairment gain (FM) and gain in functional task performance (AMAT-T and AMAT-F). We generated descriptive statistics to characterize the baseline, posttreatment, and gain scores separately for the hemorrhagic and ischemic subjects
Results
Baseline
Table 3 provides baseline subject characteristics. Group assignment was: Proximal Group (n = 10), Distal Group (n = 8), and Whole Arm Group (n = 18) (Figure 1, CONSORT study flow diagram).
Table 3.
Baseline Characteristics (n = 36).
| Group | Stroke Type | Years Poststroke | Age Range (Years) | Gender | |||||
|---|---|---|---|---|---|---|---|---|---|
| Ischemic | Hemorrhagic | 0.5-3 | >4 | 21-49 | 50-62 | ≥63 | Male | Female | |
| Proximal Group | 7 | 3 | 10 | 0 | 3 | 5 | 2 | 7 | 3 |
| Distal Group | 5 | 3 | 6 | 2 | 2 | 4 | 2 | 6 | 2 |
| Whole Arm Group | 14 | 4 | 18 | 0 | 2 | 11 | 5 | 15 | 3 |
Figure 1.

Patient flow CONSORT (Consolidated Standards of Reporting Trials) diagram.
No adverse events occurred as a result of participation in the study.
The unequal sample size across the three groups could have occurred for at least 2 reasons. First, we conducted a stratification procedure such that the Whole Group received enrollees from the whole pool of candidates, whereas each of the other 2 groups were blocked in terms of receiving subjects with the “wrong” location, respectively, of impairment in the limb. Second, after stratifying, we used a random procedure of assigning to the treatment groups. A random procedure does not always result in equal sample size.
Descriptive Statistics
The impairment severity distribution across the whole group treated (n = 36), based on initial FM score was as follows: mild, n = 2; moderate, n = 4; severe, n = 30 based on the following ranges: mild = 43-66; moderate = 29-42; severe = 0-28.56
There was an attrition rate of 17% from beginning of enrollment (n = 38) to follow-up (7/38), which was equally distributed across the 3 groups (3, 2, and 2, respectively). The most frequent reason for leaving the study at any time point was difficulty with transportation. For this 7-person subsample, FM change scores ranged from 6 to 18 points with a mean change of 11.2 points, both comparable to the whole cohort performance.
At baseline, for hemorrhagic stroke, FM mean was 23.1 (±7.4) and for ischemic stroke, FM was 22.8 (±10.4), a difference of 0.3 points. At posttreatment, for hemorrhagic stroke, FM was 33.6 (±10.1) and ischemic stroke was 32.3 (±12.7), a difference of 1.3 points. The FM mean gain score was 10.5 points for hemorrhagic stroke and 9.5 points for ischemic stroke; the difference in gain score was 1 point. These very close descriptive results indicate no difference in baseline or treatment response for ischemic versus hemorrhagic stroke.
Group Comparison of Treatment Response: Baseline to 3-Month Follow-up
Treatment Groups
At baseline, there was no difference among the 3 groups on any study measure (P ≥ .27), age (P = .85), or time since stroke (P = .39). There were a significantly greater number of males (n = 15) in the Whole Arm Group (P = .02). There was no difference across treatment groups in response to treatment according to the AMAT-T (P = .160), AMAT-F (P = .33), or FM (P = .97). Given that there was no significant difference across the 3 groups, we combined the 3 groups (Table 4) in the study of 2 questions: (1) Was >150 hours of therapy beneficial and (2) Were significant gains retained at follow-up?
Table 4.
FM, AMAT-T, and AMAT-F Organized by Time Point (n = 31).
| Measure | Pretreatment, Mean (SD) | Posttreatment, Mean (SD) | Follow-up, Mean (SD) |
|---|---|---|---|
| FM | 21.8 (8·2) | 31.5 (11·3) | 31.3 (11·9) |
| AMAT-T | 1722 (644) | 1353 (677) | 1244 (665) |
| AMAT-F | 2.03 (0.83) | 2.49 (0.94) | 2.61 (0.95) |
| a: FM for pre-, mid-, and posttreatment (n = 36) | |||
| Pretreatment, Mean (SD) | Mid-treatment, Mean (SD) | Posttreatment, Mean (SD) | |
| 22.9 (9.6) | 27.6 (10.8) | 32.7 (11.9) | |
| n = 36, group used for pre vs mid and mid vs post comparisons. | |||
Abbreviations: FM, Fugl-Meyer assessment; AMAT-T, Arm Motor Assessment Test (Time domain); AMAT-F, AMAT Function domain assessing coordination; SD, standard deviation.
Was >150 Hours of Therapy Beneficial? Change From Mid-Treatment (150 Hours of treatment) to Posttreatment (300 Hours of Treatment)
We found that there was a statistically and clinically significant improvement from mid- to posttreatment for the FM (Figure 2; Table 5a), indicating an additionally significant improvement (FM improvement = 5.1 points) during the second half of treatment, which extended from 150 to 300 hours of treatment. This “second half” improvement was greater than the FM improvement of 4.7 points that was observed during the first half of treatment (from 0 to 150 hours of treatment; Figure 2; Table 5a). The total FM improvement, then, from pre- to posttreatment was 9.8 points (Figure 2), which is double the minimum clinically important difference (MCID) for the FM.57
Figure 2a.
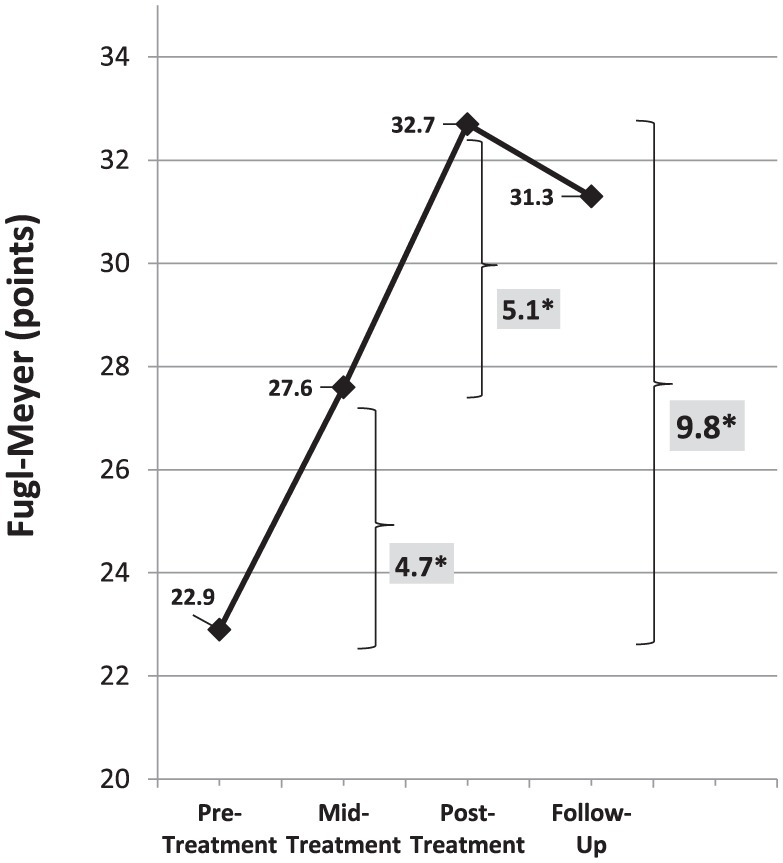
No plateau at mid-treatment indicated by clinically and statistically significant gain in coordination from mid- to posttreatment.
*Clinically and statistically significant improvements from pre- to mid- and from mid- to posttreatment, and overall from pre- to posttreatment. The minimum clinically important difference (MCID) for Fugl-Meyer is 4.25.
Table 5.
Results of Treatment Response.
| (a) FM | ||||
|---|---|---|---|---|
| Comparison | Mean Gain (SE) | P | 95% CI | Effect Size |
| pre/mida | 4.7 (0.60) | <.0001 | (4, 6) | 0.54 |
| mid/posta | 5.8 (0.68) | <.0001 | (3, 6) | 0.59 |
| pre/posta | 9.8 (0.97) | <.0001 | (7, 11) | 0.60 |
| post/follow-up | 2.0 (0.70) | .5315 | (−2, 1) | 0.08 |
| pre/follow-up | 9.4 (1.28) | <.0001 | (5, 13) | 0.61 |
| (b) AMAT-F | ||||
| Comparison | Mean (SE) | P | 95% CI | Effect Size |
| pre/post | 0.47 (0.07) | <.0001 | (0.23, 0.55) | 0.60 |
| post/follow-up | 0.11 (0.05) | .0379 | (0, 0.18) | 0.26 |
| pre/follow-up | 0.57 (0.07) | <.0001 | (0.34, 0.73) | 0.62 |
| (c) AMAT-T | ||||
| Comparison | Mean (SE) | P | 95% CI | Effect Size |
| pre/post | 370 (60.7) | <.0001 | (219, 392) | 0.60 |
| post/follow-up | 109 (28.0) | .0003 | (24, 182) | 0.43 |
| pre/follow-up | 478 (57.0) | <.0001 | (303, 553) | 0.62 |
Abbreviations: FM, Fugl-Meyer; AMAT-T, Arm Motor Ability Test (Time domain); AMAT-F, Arm Motor Ability Test (Function domain); CI, confidence interval; SE, standard error.
n = 36; all other comparisons, n = 31.
Figure 2b.
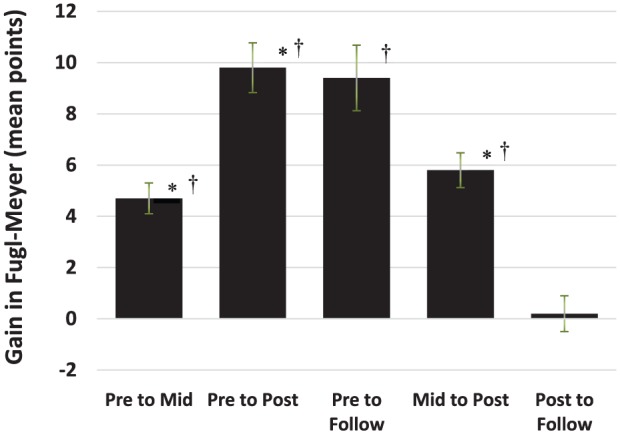
Gain in Fugl-Meyer.
*N = 36; other comparisons, N = 31.
†P < .0001.
І = standard error.
Were Posttreatment Gains Maintained at Follow-up After 3 Months of No Treatment? (Change From Posttreatment to 3moF/U)
For the FM coordination scale, we found that the significant gains achieved throughout treatment were maintained three months after cessation of treatment (Table 5a; ie, no change from posttreatment to 3moF/U).
For the AMAT-F, we found a clinically and statistically significant improvement in task performance from pre- to posttreatment (Table 5b). Subsequently, there was additional statistically significant improvement from posttreatment to 3MoFU (Table 5b; Figure 3).
Figure 3a.
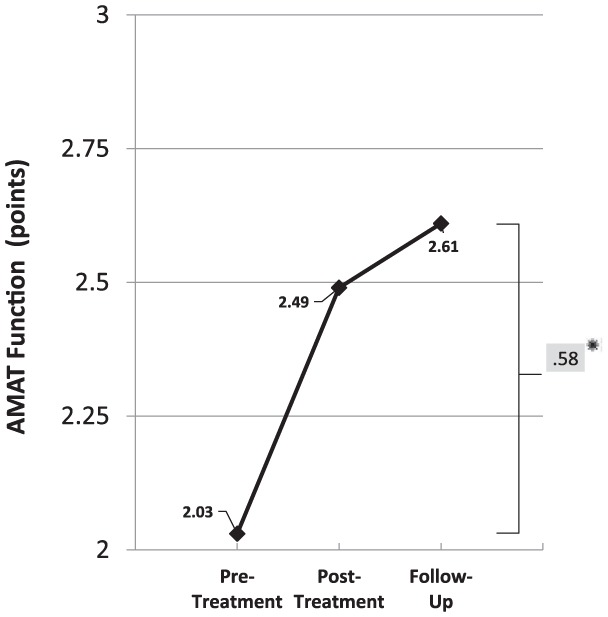
Arm Motor Ability Test Function (AMAT-F) clinically and statistically significant improvement from pre-treatment to follow-up.
*Clinically and statistically significant gain from pretreatment to follow-up.
Minimum clinically important change for AMAT-F is 0.44 points.
Statistically significant gain from posttreatment to follow-up.
Figure 3b.
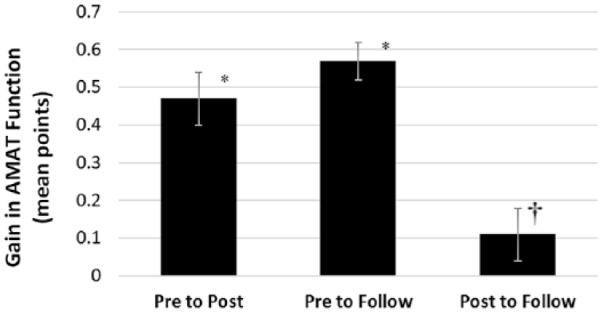
Gain in Arm Motor Ability Test Function (AMAT-F).
*P < .0001. †P = .0379. І, standard error.
For AMAT-T, we also found a statistically significant improvement in functional task performance from pretreatment to post-treatment (Table 5c; Figure 4). Subsequently, there was additional statistically significant improvement in AMAT-T from posttreatment to 3MoFU (Table 5c; Figure 4).
Figure 4a.

Arm Motor Ability Test Time (AMAT-T) statistically significant improvement from pre- to posttreatment and from posttreatment to follow-up.
*Statistically significant improvement (P < .05).
Figure 4b.

Gain in Arm Motor Ability Test Time (AMAT-T).
*P < .0001. †P = .0003. І, standard error.
Correlation Analysis
FM baseline was poorly correlated with FM at 3MoFU (r = 0.37; P = .04). FM improvement was correlated at the fair level58 with AMAT-T improvement (r = 0.50; P = .0041) and at the good level58 with AMAT-F improvement (r = 0.68; P < .0001).
Multidomain Self-Report Measure
The SIS self-report measure showed statistically significant improvement in both subscales of Daily Activities and Hand, as well as the overall SIS (P ≤ .016; Table 6).
Table 6.
Stroke Impact Scale (SIS).
| SIS_Domain | Pretreatment | Posttreatment | Difference | P |
|---|---|---|---|---|
| Daily activities, mean (SD) | 69.7 (16.2) | 74.9 (17.9) | 5.2 (13.6) | .016 |
| Hand, mean (SD) | 21.3 (25.6) | 41.3 (29.3) | 20 (24.7) | .00015 |
| Total SIS, mean (SD) | 515.1 (96) | 579.8 (107.6) | 64.7 (66.1) | 2.90E-05 |
Qualitative Data
Data on therapist observations showed that subjects made progress in impairment-level upper limb movements (Supplementary Table SIa). These were captured in the FM measure. Supplementary Table SIb contains examples of improved functional tasks and life role participation activities. These included such things as recovered self-care, independence in eating, home and community activities and return to work for 3 individuals
Discussion
First, this is a replication of results from a prior study,28 in which we obtained impairment and functional task improvement equal to or beyond clinically significant improvements. In the current study, our results again showed a magnitude of gains beyond what has been published, to date. To our knowledge, this study contributes a first-ever report of 2 important points. First, over 150 hours of therapy were necessary in this protocol in order to achieve statistically and clinically significant recovery according to the FM, at twice the MCID (Figure 2). Second, this recovery of coordination was maintained for three months after the end of therapy, and functional task performance continued to statistically improve from posttreatment to 3MoFU (Figures 3 and 4), suggesting further consolidation of the gains in upper limb coordination into improved functional task performance.
Impairment Gains From mid- to Posttreatment Support Benefit of Over 150 Hours of Treatment
The gain (FM) of 4.7 points from baseline to mid-treatment was clinically significant. At midpoint, there was no plateau. Rather, there was subsequent additive statistically and clinically significant improvement in coordination (FM) from mid- to posttreatment (5.1 points). This is evidence that as long as treatment was administered, impairment improved even during treatment throughout weeks 6 to 12. After treatment cessation, though impairment gains were maintained, the lack of further gain in impairment suggests that additional neurorehabilitation would be necessary if further gains in joint movement coordination were to be realized.
Significant Additional Gains Exhibited in Functional Task Performance for 3 Months After Treatment Cessation
During the treatment time (pre-/posttreatment), neurorehabilitation produced statistically (AMAT-T; AMAT-F) and clinically significant (AMAT-F) gains in functional task performance (Figures 3 and 4). This is reasonable, considering coordination is foundational for functional task performance and coordination also had improved. Notably, additional statistically significant gains were exhibited in both AMAT-T and AMAT-F from posttreatment to 3moF/U. That finding along with the improved coordination (Figure 2) continuing up to the posttreatment time point, suggests that the improvement in joint movement coordination up to that posttreatment time point may have somewhat preceded subsequent consolidation of coordination into improved functional task performance during the 3 months between end of treatment and follow-up testing.
Magnitude of Retained Gains From Pretreatment to 3moF/U: Comparison With Other Treatment Studies Reporting Retention Results at Follow-up
Chronic Moderate/Severe Impairment Results
In the current study, retained/improvement (from baseline to after 3 months of no treatment) in coordination was 9.5 points (pretreatment 21.8 points and 3/moFU, 31.3 points; Table 4, left panel, first row, n = 31)); this is approximately double the MCID of 4.25 points, the benchmark for FM clinical significance,57 and which is greater than that reported by others for patients with chronic moderate/severe impairment (eg, 3-5 points on the FM).59-61
Chronic Mild/Moderate Impairment Results
Additionally, we can compare our results to other studies of chronic stroke but for those with lesser and more workable mild/moderate impairment. For our more impaired cohort (severe/moderate), our results were equal to62 or better than for those with lesser impairment, according to retained improvement.5,17,63-65 We identified one study of lesser impaired subjects reporting a greater retained gain than our more severe subjects.66
Chronic Moderate/Severe Functional Task Performance Results
Additionally supporting high magnitude of retained gains in the current study, coordination improvement was sufficient to produce retained gains in functional task performance (AMAT-F; 0.50-point gain) which is greater than the benchmark for clinically important change (0.44 points),52 and to our knowledge, not yet reported at this magnitude by others for those with moderate to severe baseline impairment.
Magnitude of Pre-/Posttreatment Gain
Many studies do not present follow-up results. Therefore, here we include review of studies with only pre-/post-treatment data. In our cohort, we had the following severity levels at baseline: severe, n = 30; moderate, n = 4; and mild n = 2).56
Impairment
In the current work, the mean FM score at baseline was 22.88 ± 9.6, which is considered severe. The mean pre-/posttreatment gain in the current work was 9.8 (±5.8) points. Baseline impairment level at this severe level was comparable to our past work for which we used the same treatment protocol as in the current study; and the results of treatment are consistent with our prior study, as well.28,29 For this more severe level of impairment, our results in response to treatment are almost double that reported by others who studied similar impairment level (4.7-5.5 FM point gains, respectively).17,61 For studies of those with greater impairment level than ours, gains ranged from 1.2 to 4.01 FM points,15,22,24,67 and for studies of more mildly impaired subjects than ours, FM gains ranged from 2 to 14 points.3,4,6,11,21,27,63,66,68,69
Function
Additionally supporting high magnitude of pre- to posttreatment gains in the current work, coordination improvement was sufficient to produce functional task gains (AMAT-F; 0.46 points), which were equal to or greater than the benchmark for clinically important change (0.44 points).52 The qualitative results provide examples of the meaningful nature of these improvements in function and life role activities (Supplementary Table SIb). Three participants reported a return to employment; many noted greater independence in everyday function and return to satisfying leisure activities. Furthermore, the SIS results indicated significantly greater activities of daily living and hand function. Taken together, these results can provide a catalyst to drive change in the way we approach rehabilitation in the chronic phase of stroke.
This magnitude of improvement may have been achieved due to the finely incrementalized approach. For example, the treatment protocol targeted, in part, the coordination deficits that are assessed with the FM limb-movement items. Improved FM score indicated progression through the difficulty hierarchy38 shown in Table 1. Normally coordinated movements are required for normal performance of daily tasks. For example, simple reaching forward requires extension at the elbow and flexion at the shoulder, which is considered out of synergy because one joint is extending while the contiguous joint is flexing. As these more coordinated movements are achieved, then components of functional tasks can be performed.
Association of Baseline Impairment Severity to Both Impairment Recovery and Recovery of Functional Task Performance
Relationship of FM Baseline to FM at 3MoF/U
There was poor correlation (r = 0.37) between FM baseline and FM gain at 3moF/U. This suggests that severity of impairment at baseline (FM measure) is not necessarily linearly associated with ability to respond to treatment according to that impairment measure. This could have occurred due to either or both of the factors that may have been operative: weakness and dyscoordination. Recovery of muscle strength was occurring to some extent. In fact, others have studied the FM in the acute stage after stroke and concluded that its variability in assessing recovery may reflect changes in both strength and coordination.31 It is certainly a well-known fact that strength is a necessary requirement for coordinated joint movement. Though strength is necessary, it is not sufficient; that is, even in the presence of the required strength, coordination control is still necessary in order to execute coordinated upper limb movements.70 Some participants in the current study began with very little active joint movement, and it was obvious that some strength recovery was necessary in order to even begin to work on isolated coordination control. But it was our observation that strength improvement alone did not result in ability to perform the FM test items or functional movement components. This is a common clinical finding, as well; that is, chronic stroke survivors can exhibit the necessary muscle strength, but inability to perform the coordinated movement normally executed by that same muscle. As early as 1995, evidence was published quantifying the clinically known phenomenon of abnormal co-contraction of upper limb muscles preventing normal coordinated movement after stroke.71 In our study, we observed that even in the presence of sufficient muscle strength, further hours of motor practice were required in order to achieve isolated joint movement control (within and outside of synergy, without abnormal co-contractions). For that training, we applied the hierarchy in Table 1, and we observed incremental improvement that was much slower than would be expected if only strength recovery were operative.
Relationship between recovery of isolated joint movement coordination (FM gain) and recovery of functional task performance (AMAT). Improved isolated joint movement control (FM) was correlated at a “fair” level58 with AMAT-T gain (r = 0.50; P = .004) and more highly correlated with improved AMAT-F gain (r = 0.68; P < .0001). The AMAT-T is a measure of speed of task performance, which could potentially incorporate compensatory strategies; this possibility might have resulted in a lower correlation than might have occurred if all the improvement in AMAT-T occurred as a result of recovered coordination. In contrast, the AMAT-F is a measure of how close the task performance is to normal, coordinated movements. The correlation of r = 0.68 is a “good” level correlation and suggests that the improvement in AMAT-F task performance of more normally coordinated movement components is well-associated with the improvement in the FM impairment measures of isolated joint movement control. Taken together with our milestone results in Tables SIa and SIb, it is reasonable to consider that there is a relationship between the following factors: treatment targeted first to isolated joint movement control and then to task component and task practice; recovery of joint movement coordination during treatment; measurement of recovery of joint movement coordination (FM) and recovery of more coordinated functional task performance (AMAT-F).
Dose
According to mid- and posttreatment results, the long-dose, high-intensity treatment was required in order to produce double the clinically significant impairment gains achieved, which were sufficiently robust to produce clinically significant functional task performance gains, greater than previously reported for functional task practice (ie, on the AMAT). Our results provide evidence supporting benefit of longer duration, intensive intervention, for the most efficacious outcome.
In other published work, optimal dose for recovery of functional task performance has not been fully elucidated.14,32 A recent meta-analysis reported a very small dose-response relationship for those with persistent deficits after stroke, receiving either 57 hours versus 24 hours of intervention.72 In a recent study, within 32 hours treatment, total repetition numbers were varied across 4 groups (3200 repetitions, 6400, 9600, or individual maximum repetitions) for chronic stroke with mild to moderate upper limb impairment; the reported results stated small, and not clinically significant change on the primary “function” measure (Action Research Arm Test) for 2 of 4 groups, and number of repetitions did not affect change.73
That study has a detailed companion manual,74 which provided some means to compare it with the current protocol. There were a number of differences between that study73 and the current study. First, the dose in the study by Lang et al73 was much smaller than the current study (32 hours versus 300 hours in the current study). Second, the subjects in the study by Lang et al73 were less impaired, having been required to exhibit baseline ability to open the hand, grasp, and pick up several objects. Third, there was a statement of no significant change reported in the SIS, whereas in the current study, we showed a significant improvement in the SIS Hand and Daily Activities subscales. Fourth, the study by Lang et al73 described the exercises as follows: “repetitions were compound movements, including reaching, grasping, manipulating, and releasing.” In contrast, the current motor learning protocol employed training for single joint movements and 2-joint movements that were practiced in a manner to elicit practice as close to a normal movement as possible. Some level of mastery of these was required before practicing task components. Fifth, the progression of practice difficulty in the Lang et al study appears to have been based largely on the number of repetitions in a timed period and the subject’s perceived fatigue during performance.74 In contrast, the current protocol was based first on obtaining a practice movement that was as close to normal as possible, most often with some type of assistance in order to achieve practice of a more coordinated movement. Only with achievement of more coordinated movement was speed of movement then considered in the treatment. Sixth, there is a statement in the Lang manual74 about progression occurring at the point of 90% achievement at their ‘current’ level. In our protocol, we considered advancing to a next level of difficulty at about 50% of achievement (e.g., of range of motion, etc). At the initiation of each new motor task, it was generally not possible to practice a functional task movement that would have been productive in the sense of being as close to normal as possible. Thus, our current motor learning protocol may be composed of more finely incrementalized practice of movements and task components, rendering them more amenable to finely graded improvements that accumulated over time and translated to functional task performance improvement. This difference in practice paradigm could have resulted in the more dramatic gains in the current study, whereby we showed both clinically and statistically significant gains on the FM, first at the 150-hour dose, and then with continued and comparable additive clinically and statistically significant improvement from mid-treatment (after another 150 hours) to the end of treatment (300 hours dose).
Another study (constraint-induced movement therapy) reported a gain of 7.4 FM points in a mild, chronic cohort (n = 13), who received 265 hours of therapy (1:1 treatment plus constraint-worn hours).62 Taken together, that cohort study of mild participants plus the current work for moderate/severely impaired, the 265 to 300 hours of therapy, respectively, is quite promising. And, in the current work, the associated functional gains from baseline to 3-month follow-up (eg, AMAT-F) were 0.58 which is greater than the 0.44 benchmark52 for clinically significant improvement on the AMAT-F.
Cost/Benefit Considerations
Currently, the average annual cost of yearly rehabilitation for patient with chronic stroke is about $12 000.1 The question should be about how this money should be spent. Perhaps, it is not wise to provide low-dose therapies every year that cannot achieve important functional gains. We need more detailed studies of cost-efficiency of poststroke rehabilitation to be able to properly allocate limited resources. In the current study, benefits are first reflected in improvement of activities of daily living, captured by the AMAT-F and SIS subscale of Daily Activities. These gains result in less caregiver need, reducing cost of care. Second, benefits are reflected in the self-reported recovery of life role participation activities. These gains result in more family and community involvement, precluding the isolation that can cause depression and downward spiraling comorbidities. Third, and potentially most important, this study presents the discovery that such gains are actually possible in the chronic stage after stroke. The mechanisms underlying these changes are largely still unknown. Although in prior work, we found a relationship between AMAT gain score and changes in task-related brain activation, according to variables derived from functional magnetic resonance imaging signal.75 The current result justifies the additional work that is now needed to develop cost-efficient therapies. In the meantime, considering financial cost, we can note that therapy was provided at a 1:3 therapist to patient ratio. Therefore, the rough cost per patient for 300 hours of therapy would be $5,000 (based on the following: $50 per hour for 1 therapist or $15,000 per 300 hours of therapy, divided by 3 patients to 1 therapist = $5000 per patient for 300 hours of therapy (based on the average cost of occupational therapy; https://health.costhelper.com/occupational-therapy.html#extres2). Therefore, the cost of our intervention is somewhat less than other current regular healthcare expenditures. Further tipping the balance are such events as return to employment as we observed with 3 of our participants or reduced need of caregiver support with daily activities, which we observed in a number of participants.
Summary of Likely “Active Ingredients”
Distilling the evidence presented and discussion points, it is reasonable to consider that the following are the probable “active ingredients,” producing the results of the study:
Accurate initial training level.
Awareness training of normal and abnormal movement patterns, which empowers and motivates the patient to self-monitor and self-progress.
Training focused on recovery of the coordination of isolated joint movements and multiple joint movements, with multiple treatment strategies employed to support practice of movement as close to normal as possible.
Accurately titrated progression of treatment.
Very finely incrementalized progression of treatment, utilizing an array of methods to support motor practice as close to normal as possible, and attention (and celebration) to small goal achievement).
Clearly stated goals for each small incrementalized practice.
Incorporation of newly recovered joint movement coordination into task component practice.
Task and task component selection customized as much as possible to align with the interests and needs of each individual.
Engagement of as many strategies as necessary to obtain continued attention and high repetition practice of coordinated movements.
Observation and monitoring of inattention or fatigue, and with rest periods held in that case.
Weekly team meeting of clinical team in which obstacles to progression are described and problem solving is offered by team members.
Periodic team-treatment, whereby another therapist visits the treatment sessions and offers observations and suggestions.
Conclusions
Rather than plateauing at mid-treatment (150 hours of treatment), there was subsequently, additive statistically and clinically significant improvement in coordination (FM) from mid- to immediately posttreatment, indicating the benefit of >150 hours of therapy. And in contrast, during the follow-up time of no treatment, there was no further change in coordination, supplying evidence that as long as treatment was administered, impairment improved even from weeks 6 to 12, and when treatment ceased after 12 weeks, gains were maintained, but there was no longer any continuation of coordination improvement. Notably, clinically and statistically significant gains in functional task performance were realized during the intervention phase and continued to statistically improve throughout the 3-month follow up. Most important, participants reported everyday functional improvement that was meaningful to each of them in their individual lives.
Supplemental Material
Supplemental material, Supplementary_Tables for Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke by Janis J. Daly, Jessica P. McCabe, John Holcomb, Michelle Monkiewicz, Jennifer Gansen and Svetlana Pundik in Neurorehabilitation and Neural Repair
Acknowledgments
Thanks to Lynn Dirk, MAMC, who provided technical assistance in creating the graphs.
Footnotes
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website at along with the online version of the article.
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Department of Veterans Affairs grant # B3709 and Career Scientist Award B5080S.
ORCID iD: Michelle Monkiewicz  https://orcid.org/0000-0002-5294-0913
https://orcid.org/0000-0002-5294-0913
References
- 1. Winstein CJ, Stein J, Arena R, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47:e98-e169. [DOI] [PubMed] [Google Scholar]
- 2. Hayward K, Barker R, Brauer S. Interventions to promote upper limb recovery in stroke survivors with severe paresis: systematic review. Disabil Rehabil. 2010;32:1973-1986. [DOI] [PubMed] [Google Scholar]
- 3. Lin KC, Chen YA, Chen CL, Wu CY, Chang YF. Effects of bilateral arm training on motor control and functional performance in chronic stroke: randomized controlled study. Neurorehabil Neural Repair. 2010;24:42-51. [DOI] [PubMed] [Google Scholar]
- 4. Lin KC, Wu CY, Liu JS, Chen YT, Hsu CJ. Constraint-induced therapy versus dose-matched control intervention to improve motor ability, basic/extended daily functions, and quality of life in stroke. Neurorehabil Neural Repair. 2009;23:160-165. [DOI] [PubMed] [Google Scholar]
- 5. Wolf SL, Winstein CJ, Miller JP, et al. Retention of upper limb function in stroke survivors who have received constraint-induced movement therapy: EXCITE randomised trial. Lancet Neurol. 2008;7:33-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Linder SM, Rosenfeldt AB, Dey T, Alberts JL. Forced aerobic exercise preceding task practice improves motor recovery poststroke. Am J Occup Ther. 2017;7:7102290020p1-7102290020p9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Hara Y, Ogawa S, Tsujiuchi K, Muraoka Y. A home-based rehabilitation program for the hemiplegic upper extremity by power-assisted functional electrical stimulation. Disabil Rehabil. 2008;30:296-304. [DOI] [PubMed] [Google Scholar]
- 8. Gharib NM, Aboumousa AM, Elowishy AA, Rezk-Allah SS, Yousef FS. Efficacy of electrical stimulation as an adjunct to repetitive task practice therapy on skilled hand performance in stroke: randomized controlled trial. Clin Rehabil. 2015;29:355-364. [DOI] [PubMed] [Google Scholar]
- 9. Lee YY, Lin KC, Cheng HJ, Wu CY, Hsieh YW, Chen CK. Effects of combining robot-assisted therapy with neuromuscular electrical stimulation on motor impairment, motor and daily function, and quality of life in patients with chronic stroke: a double-blinded randomized controlled trial. J Neuroeng Rehabil. 2015;12:96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Colomer C, Llorens R, Noé E, Alcañiz M. Effect of a mixed reality-based intervention on arm, hand, and finger function on chronic stroke. J Neuroeng Rehabil. 2016;13:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Wu CY, Yang CL, Chuang LL, et al. Effect of therapist-based versus robot-assisted bilateral arm training on motor control, functional performance, and quality of life after chronic stroke: clinical trial. Phys Ther. 2012;92:1006-1016. [DOI] [PubMed] [Google Scholar]
- 12. Baldwin CR, Harry AJ, Power LJ, Pope KL, Harding KE. Modified constraint-induced movement therapy is a feasible and potentially useful addition to the community rehabilitation tool kit after stroke: a pilot randomised control trial. Aust Occup Ther J. 2018;65:503-511. [DOI] [PubMed] [Google Scholar]
- 13. Ju Y, Yoon IJ. The effects of modified constraint-induced movement therapy and mirror therapy on upper extremity function and its influence on activities of daily living. J Phys Ther Sci. 2018;30:77-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kwakkel G, Veerbeek JM, van Wegen EE, Wolf SL. Constraint-induced movement therapy after stroke. Lancet Neurol. 2015;14:224-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Uswatte G, Taub E, Bowman MH, et al. Rehabilitation of stroke patients with plegic hands: randomized controlled trial of expanded constraint-induced movement therapy. Restor Neurol Neurosci. 2018;36:225-244. [DOI] [PubMed] [Google Scholar]
- 16. Meadmore KL, Exell TA, Hallewell E, et al. The application of precisely controlled functional electrical stimulation to the shoulder, elbow and wrist for upper limb stroke rehabilitation: a feasibility study. J Neuroeng Rehabil. 2014;11:105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Page SJ, Levine PG, Basobas BA. “Reps” aren’t enough: augmenting functional electrical stimulation with behavioral supports significantly reduces impairment in moderately impaired stroke. Arch Phys Med Rehabil. 2016;97:747-752. [DOI] [PubMed] [Google Scholar]
- 18. Kraft GH, Fitts SS, Hammond MC. Techniques to improve function of the arm and hand in chronic hemiplegia. Arch Phys Med Rehabil. 1992;73:220-227. [PubMed] [Google Scholar]
- 19. McCombe Waller S, Whitall J, Jenkins T, et al. Sequencing bilateral and unilateral task-oriented training versus task oriented training alone to improve arm function in chronic stroke. BMC Neurol. 2014;14:236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Colomer C, Noé E, Llorens R. Mirror therapy in chronic stroke survivors with severely impaired upper limb function: a randomized controlled trial. Eur J Phys Rehabil Med. 2016;52:271-278. [PubMed] [Google Scholar]
- 21. Ellis MD, Carmona C, Drogos J, Dewald JPA. Progressive abduction loading therapy with horizontal-plane viscous resistance targeting weakness and flexion synergy to treat upper limb function in chronic hemiparetic stroke: a randomized clinical trial. Front Neurol. 2018;9:71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Carda S, Biasiucci A, Maesani A, et al. Electrically assisted movement therapy in chronic stroke patients with severe upper limb paresis: a pilot, single-blind, randomized crossover study. Arch Phys Med Rehabil. 2017;98:1628-1635.e2. [DOI] [PubMed] [Google Scholar]
- 23. Page SJ, Hill V, White S. Portable upper extremity robotics is as efficacious as upper extremity rehabilitative therapy: randomized controlled pilot trial. Clin Rehabil. 2013;27:494-503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Lo AC, Guarino PD, Richards LG, et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N Engl J Med. 2010;362:1772-1783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Klamroth-Marganska V, Blanco J, Campen K, et al. Three-dimensional, task-specific robot therapy of arm after stroke: multicentre, parallel-group randomised trial. Lancet Neurol. 2014;13:159-166. [DOI] [PubMed] [Google Scholar]
- 26. Wu X, Guarino P, Lo AC, Peduzzi P, Wininger M. Long-term effectiveness of intensive therapy in chronic stroke. Neurorehabil Neural Repair. 2016;30:583-590. [DOI] [PubMed] [Google Scholar]
- 27. Kim GW, Won YH, Seo JH, Ko MH. Effects of newly developed compact robot-aided upper extremity training system (Neuro-X®) in patients with stroke: a pilot study. J Rehabil Med. 2018;50:607-612. [DOI] [PubMed] [Google Scholar]
- 28. McCabe J, Monkiewicz M, Holcomb J, Pundik S, Daly JJ. Comparison of robotics, functional electrical stimulation, and motor learning methods for treatment of persistent upper extremity dysfunction after stroke: a randomized controlled trial. Arch Phys Med Rehabil 2015;96:981-990. [DOI] [PubMed] [Google Scholar]
- 29. Daly JJ, Hogan N, Perepezko EM, et al. Response to upper-limb robotics and functional neuromuscular stimulation following stroke. J Rehabil Res Dev 2005;42:723-736. [DOI] [PubMed] [Google Scholar]
- 30. Ward N. F1000Prime Recommendation of [McCabe J et al., Arch Phys Med Rehabil. 2015;96:981-90]. In F1000Prime, 22 Jan 2018. doi: 10.3410/f.725259675.793541781 [DOI] [Google Scholar]
- 31. Krakauer JW, Carmichael ST. Chronic hemiparesis: motor learning, compensation, and the challenge of reversing impairment in late stroke. In: Broken Movement: The Neurobiology of Motor Recovery After Stroke. Cambridge, MA: MIT Press; 2017:174-176. [Google Scholar]
- 32. Lang CE, Lohse KR, Birkenmeier RL. Dose and timing in neurorehabilitation: prescribing motor therapy after stroke. Curr Opin Neurol. 2015;28:549-555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. van der Lee JH, Snels IA, Beckerman H, Lankhorst GJ, Wagenaar RC, Bouter LM. Exercise therapy for arm function in stroke patients: systematic review of randomized controlled trials. Clin Rehabil. 2001;15:20-31. [DOI] [PubMed] [Google Scholar]
- 34. Bloom BS, Englehart MB, Furst EJ, Hill WH, Krathwohl DR. Taxonomy of Educational Objectives: The Classification of Educational Goals. Handbook 1: Cognitive Domain. New York, NY: Longman; 1956. [Google Scholar]
- 35. Riolo L. Skill differences in novice and expert clinicians in neurologic physical therapy. Neurology Report. 1996;20:60-64. [Google Scholar]
- 36. Brunnstrom S. Motor testing procedures in hemiplegia: based on sequential recovery stages. Phys Ther. 1966;46:357-375. [DOI] [PubMed] [Google Scholar]
- 37. Twitchell TE. The restoration of motor function following hemiplegia in man. Brain. 1951;74:443-480. [DOI] [PubMed] [Google Scholar]
- 38. Crow JL, Harmeling-van der Wel BC. Hierarchical properties of the motor function sections of the Fugl-Meyer assessment scale for people after stroke: a retrospective study. Phys Ther. 2008;88:1554-1567. [DOI] [PubMed] [Google Scholar]
- 39. Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science. 1996;272:1791-1794. [DOI] [PubMed] [Google Scholar]
- 40. Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-dependent alterations of movement representations in primary motor cortex of adult squirrel monkeys. J Neurosci. 1996;16:785-807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Pascual-Leone A, Torres F. Plasticity of the sensorimotor cortex representation of the reading finger in Braille readers. Brain. 1993;116(pt 1):39-52. [DOI] [PubMed] [Google Scholar]
- 42. Butefisch C, Hummelsheim H, Denzler P, Mauritz KH. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J Neurol Sci. 1995;130:59-68. [DOI] [PubMed] [Google Scholar]
- 43. Elbert T, Pantev C, Wienbruch C, Rockstroh B, Taub E. Increased cortical representation of the fingers of the left hand in string players. Science. 1995;270:305-307. [DOI] [PubMed] [Google Scholar]
- 44. Dean CM, Shepherd RB. Task-related training improves performance of seated reaching tasks after stroke. A randomized controlled trial. Stroke. 1997;28:722-728. [DOI] [PubMed] [Google Scholar]
- 45. Singer R, Lidor R, Cauraugh JH. To be aware or not aware? What to think about while learning and performing a motor skill. Sport Psychol. 1993;7:19-30. [Google Scholar]
- 46. Plautz EJ, Milliken GW, Nudo RJ. Effects of repetitive motor training on movement representations in adult squirrel monkeys: role of use versus learning. Neurobiol Learn Mem. 2000;74:27-55. [DOI] [PubMed] [Google Scholar]
- 47. Resnik L, Jensen GM. Using clinical outcomes to explore the theory of expert practice in physical therapy. Phys Ther. 2003;83:1090-1106. [PubMed] [Google Scholar]
- 48. Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. method for evaluation of physical performance. Scand J Rehabil Med. 1975;7:13-31. [PubMed] [Google Scholar]
- 49. Santisteban L, Térémetz M, Bleton JP, Baron JC, Maier MA, Lindberg PG. Upper limb outcome measures used in stroke rehabilitation studies: a systematic literature review. PLoS One. 2016;11:e0154792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. O’Dell MW, Kim G, Rivera L, et al. A psychometric evaluation of the Arm Motor Ability Test. J Rehabil Med. 2013;45:519-527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Chae J, Labatia I, Yang G. Upper limb motor function in hemiparesis: concurrent validity of the Arm Motor Ability test. Am J Phys Med Rehabil. 2003;82:1-8. [DOI] [PubMed] [Google Scholar]
- 52. Fulk G, Martin R, Page SJ. Clinically important difference of the Arm Motor Ability Test in stroke survivors. Neurorehabil Neural Repair. 2017;31:272-279. [DOI] [PubMed] [Google Scholar]
- 53. Richardson M, Campbell N, Allen L, Meyer M, Teasell R. The stroke impact scale: performance as a quality of life measure in a community-based stroke rehabilitation setting. Disabil Rehabil. 2016;38:1425-1430. [DOI] [PubMed] [Google Scholar]
- 54. Daniel WW. Applied Nonparametric Statistics. 2nd ed. Boston, MA: PWS-Kent; 1990. [Google Scholar]
- 55. Hahn GJ, Meeker WQ. Statistical Intervals: A Guide for Practitioners. New York, NY: John Wiley & Sons; 1991. [Google Scholar]
- 56. Woytowicz EJ, Rietschel JC, Goodman RN, et al. Determining levels of upper extremity movement impairment by applying a cluster analysis to the Fugl-Meyer Assessment of the upper extremity in chronic stroke. Arch Phys Med Rehabil. 2017;98:456-462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Page SJ, Fulk GD, Boyne P. Clinically importance differences for the upper-extremity Fugl-Meyer Scale in people with minimal to moderate impairment due to chronic stroke. Phys Ther. 2012;92:791-798. [DOI] [PubMed] [Google Scholar]
- 58. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 2nd ed. Upper Saddle River, NJ: Prentice Hall Health; 2000. [Google Scholar]
- 59. Fasoli SE, Krebs HI, Stein J, Frontera WR, Hughes R, Hogan N. Robotic therapy for chronic motor impairments after stroke: follow-up results. Arch Phys Med Rehabil. 2004;85:1106-1111. [DOI] [PubMed] [Google Scholar]
- 60. Chang JJ, Tung WL, Wu WL, Huang MH, Su FC. Effects of robot-aided bilateral force-induced isokinetic arm training combined with conventional rehabilitation on arm motor function in patients with chronic stroke. Arch Phys Med Rehabil. 2007;88:1332-1338. [DOI] [PubMed] [Google Scholar]
- 61. Lum PS, Burgar CG, Shor PC, Majmundar M, Van der Loos M. Robot-assisted movement training compared with conventional therapy techniques for rehabilitation of upper-limb motor function after stroke. Arch Phys Med Rehabil. 2002;83:952-959. [DOI] [PubMed] [Google Scholar]
- 62. Page SJ, Murray C, Hermann V. Affected upper-extremity movement ability is retained 3 months after modified constraint-induced therapy. Am J Occup Ther. 2011;65:589-593. [DOI] [PubMed] [Google Scholar]
- 63. Patten C, Condliffe EG, Dairaghi CA, Lum PS. Concurrent neuromechanical and functional gains following upper-extremity power training post-stroke. J Neuroeng Rehabil. 2013;10:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Persch AC, Page SJ, Murray C. Paretic upper extremity movement gains are retained 3 months after training with an electrical stimulation neuroprosthesis. Arch Phys Med Rehabil. 2012;93:2122-2125. [DOI] [PubMed] [Google Scholar]
- 65. Chuang LL, Chen YL, Chen CC, et al. Effect of EMG-triggered neuromuscular electrical stimulation with bilateral arm training on hemiplegic shoulder pain and arm function after stroke: a randomized controlled trial. J Neuroeng Rehabil. 2017;14:122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Nam C, Rong W, Li W, Xie Y, Hu X, Zheng Y. The effects of upper-limb training assisted with an electromyography-driven neuromuscular electrical stimulation robotic hand on chronic stroke. Front Neurol. 2017;8:679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Finley MA, Fasoli SE, Dipietro L, et al. Short-duration robotic therapy in stroke patients with severe upper-limb motor impairment. J Rehabil Res Dev. 2005;42:683-692. [DOI] [PubMed] [Google Scholar]
- 68. Takebayashi T, Takahashi K, Moriwaki M, Sakamoto T, Domen K. Improvement of upper extremity deficit after constraint-induced movement therapy combined with and without preconditioning stimulation using dual-hemisphere transcranial direct current stimulation and peripheral neuromuscular stimulation in chronic stroke patients: a pilot randomized controlled trial. Front Neurol. 2017;8:568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Jung K, Jung J, In T, Kim T, Cho HY. The influence of task-related training combined with transcutaneous electrical nerve stimulation on paretic upper limb muscle activation in patients with chronic stroke. NeuroRehabilitation. 2017;40:315-323. [DOI] [PubMed] [Google Scholar]
- 70. Daly JJ, Ruff RL. Construction of efficacious gait and upper limb functional interventions based on brain plasticity evidence and model-based measures for stroke patients. ScientificWorldJournal. 2007;7:2031-2045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Dewald JP, Pope PS, Given JD, Buchanan TS, Rymer WZ. Abnormal muscle coactivation patterns during isometric torque generation at the elbow and shoulder in hemiparetic subjects. Brain. 1995;118(pt 2):495-510. [DOI] [PubMed] [Google Scholar]
- 72. Lohse KR, Lang CE, Boyd LA. Is more better? Using metadata to explore dose-response relationships in stroke rehabilitation. Stroke. 2014;45:2053-2058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Lang CE, Strube MJ, Bland MD, et al. Dose response of task-specific upper limb training in people at least 6 months poststroke: a phase II, single-blind, randomized controlled trial. Ann Neurol. 2016;80:342-354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Lang CE, Birkenmeier RL. Upper-Extremity Task-Specific Training After Stroke or Disability. Bethesda, MD: American Occupational Therapy Association; 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Pundik S, McCabe JP, Hrovat K, et al. Recovery of post stroke proximal arm function, driven by complex neuroplastic bilateral brain activation patterns and predicted by baseline motor dysfunction severity. Front Hum Neurosci. 2015;9:394. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Supplementary_Tables for Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke by Janis J. Daly, Jessica P. McCabe, John Holcomb, Michelle Monkiewicz, Jennifer Gansen and Svetlana Pundik in Neurorehabilitation and Neural Repair