

Sir,
Cocaine remains among the most common cause of acute drug-related emergency department visits. Herein, we describe a case of “crack lung,” an acute pulmonary complication occurring after cocaine smoking.
Paramedics brought to the emergency department a 48-year-old male who was found unresponsive in a park. His wife reported that the patient had smoked cocaine a few hours before the presentation. On examination, Glasgow Coma Scale was 12 (E3V4M5), temperature 38°C, pulse 145 bpm, blood pressure 140/80 mmHg, and oxygen saturation 60% on room air. Arterial blood gases showed mixed respiratory and metabolic acidosis. Electrocardiogram showed sinus tachycardia. Oxygen, naloxone, glucose, and thiamine were administered. Mental status improved and oxygen saturation rose to 99%. A chest radiograph [Figure 1a] and thoracic computed tomography showed diffuse alveolar ground-glass infiltrates on both the lungs, without pleural effusions or cardiomegaly and without evidence of pulmonary embolism. The patient was admitted in our department and was treated with ampicillin-sulbactam. Fever and hypoxemia resolved within 24 h and the chest radiograph 48 h after admission [Figure 1b] was markedly improved. The patient was discharged home 5 days after admission.
Figure 1.
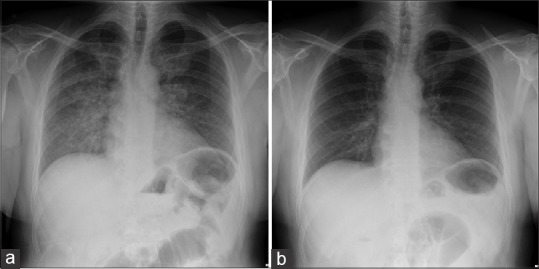
(a) Chest radiograph of the patient on admission showing diffuse alveolar infiltrates (b) follow-up chest radiograph 48 h after admission with marked radiologic improvement
Smoked cocaine (crack) induces a variety of acute and chronic pulmonary complications including pulmonary edema, alveolar hemorrhage, eosinophilic pneumonia, pneumothorax, and thromboembolic disease.[1] Mechanisms include thermal airway injury, direct cellular toxicity, provocation of inflammatory damage, barotrauma, and vasospasm leading to ischemia. “Crack lung” refers to an acute syndrome of diffuse alveolar damage and hemorrhagic alveolitis that occurs within 48 h of smoking crack. Patients present with dyspnea, fever, cough, or hemoptysis which may progress to respiratory failure. Radiographic findings are nonspecific and include diffuse alveolar infiltrates and ground-glass opacities. Bronchoalveolar lavage, if performed, helps excluding infection and diffuse alveolar hemorrhage and shows carbonaceous debris and hemosiderin-laden macrophages.[2] The presence of >25% eosinophils indicates acute eosinophilic pneumonia and administration of corticosteroids is warranted. Treatment of crack lung is supportive with oxygen supplementation and conservative fluid management. The temporal relationship between cocaine use, onset of hypoxemia, and chest radiography findings suggests the diagnosis. In the absence of complications, symptoms, and hypoxemia resolve spontaneously.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Restrepo CS, Carrillo JA, Martínez S, Ojeda P, Rivera AL, Hatta A, et al. Pulmonary complications from cocaine and cocaine-based substances: Imaging manifestations. Radiographics. 2007;27:941–56. doi: 10.1148/rg.274065144. [DOI] [PubMed] [Google Scholar]
- 2.Forrester JM, Steele AW, Waldron JA, Parsons PE. Crack lung: An acute pulmonary syndrome with a spectrum of clinical and histopathologic findings. Am Rev Respir Dis. 1990;142:462–7. doi: 10.1164/ajrccm/142.2.462. [DOI] [PubMed] [Google Scholar]