

Abstract
Purpose:
To compare the relationship between anti-tobacco industry attitudes and intention and attempts to quit smoking across 6 young adult peer crowds.
Design:
A cross-sectional bar survey in 2015.
Setting:
Seven US cities (Albuquerque, Los Angeles, Nashville, Oklahoma City, San Diego, San Francisco, and Tucson).
Participants:
Two thousand eight hundred seventeen young adult bar patrons who were currently smoking.
Measures:
Intention to quit in the next 6 months and having made a quit attempt in the last 12 months were binary outcomes. Anti-industry attitudes were measured by 3 items indicating support for action against the tobacco industry. Peer crowd affiliation was measured using the I-Base Survey.
Analysis:
Adjusted multivariable logistic regression models examined the association between anti-industry attitudes and the outcomes for the total sample and for each peer crowd.
Results:
Overall, anti-industry attitudes were positively associated with both intention to quit (odds ratio [OR] = 1.37, 95% confidence interval [CI] = 1.24–1.52) and attempt to quit (OR = 1.14, 95% CI = 1.03–1.27). Intriguingly, the relationship between anti-industry attitudes and intention to quit differed by peer crowd affiliation, with significant associations for Homebody, Partier, Hipster, and Hip Hop, but not for Young Professional and Country.
Conclusions:
Developing health communication messages that resonate with unique peer crowd values can enhance the relevance of public health campaigns. Tobacco control practitioners should tailor anti-industry messages to promote intention to quit smoking among the highest risk young adults.
Keywords: smoking cessation, anti-tobacco industry, peer crowd, young adults
Purpose
While smoking rates are declining, young adults continue to have a high tobacco use prevalence,1 and high rates of tobacco co-use with alcohol.2 Bars and nightclubs are an important context in which tobacco use occurs. Smoking prevalence among young adult bar patrons ranged from 35% to 47%, approximately 2- to 4-fold higher than young adults in general.3,4 This may be partly due to tobacco marketing campaigns targeting young adults in bars/nightclubs as bar patrons are considered to be key influencers.5,6 In addition, during young adulthood, many tobacco experimenters either become established smokers or quit.6 Therefore, young adult bar patrons should be a priority population for tobacco control.
Many communication strategies address smoking among young adults. For more than a decade, strong anti-industry messages have been shown to motivate adolescents and young adults to rebel against tobacco companies and reject tobacco products.7 Indeed, anti-tobacco attitudes are significantly associated with smoking behavior and intentions to quit among young adults worldwide.8–11 In the United States, the national “truth” campaign decreased smoking initiation among youth,12,13 with some effect on attitudes and intent to quit among young adults.14 This campaign has recently been expanded from only targeting adolescents to including young adults.15
Several theories (ie, social identity and social norms theories) and empirical studies have proposed “peer crowd affiliation” as a promising approach for health education campaigns among young adults.3,16,17 Peer crowd is defined as a macrolevel connection between individuals with similar interests, lifestyles, influencers, and habits.16 Research has delineated many different peer crowds among youth and young adults.17,18 However, common peer crowds found among US young adults are Young Professional, Homebody, Partier, Country, Hipster, and Hip Hop. These peer crowd labels reflect different sets of certain characteristics as described elsewhere.17 For example, Partier young adults prioritize going out to bars and nightclubs as part of their social identity, more than other young adults, with these social environments playing a more central role to their lifestyle, which led to the informal name “Partiers.” Social identity and social norms theories postulate that individuals who identify with a high-risk peer crowd are more likely to engage in risk behaviors. Consistent with these theories, empirical research has also demonstrated different smoking rates by peer crowd; finding, for example, high smoking rates among Hip Hop individuals and low smoking rates among Young Professionals.3,17 Tobacco companies have a long history of using young adult psychographic segmentation in marketing their products,19 including Hip Hop and Hipster cultures.5,20 This tailoring can be applied to anti-tobacco campaigns to prevent smoking and promote cessation.3,17 Indeed, the US Food and Drug Administration (FDA) Fresh Empire national campaign, launched in 2015, targeted the Hip Hop peer crowd to prevent and reduce tobacco use among at-risk multicultural youth.21 Likewise, bar interventions targeting Hipster22 and Partier young adults23,24 provided early evidence on the effectiveness of peer crowd-tailored approaches to decreasing young adult smoking.
Since each peer crowd shares a unique set of values and norms, their attitudes toward the tobacco industry may be different from each other. A previous study indicated that the “truth” campaign had differential effects on producing antismoking beliefs across adolescent peer crowds.25 In addition, based on the prism model of communication effects,26 in which an individual’s identity moderates the effect of media messages on behaviors, we expect that peer crowd affiliation will moderate the effect of anti-tobacco industry messages on intention to quit smoking. However, no previous research has examined whether the association between anti-tobacco industry attitudes on intention to quit smoking differs by peer crowd affiliation. To address this gap, using data from a bar survey in 7 cities, we aimed to (1) examine the relationships between anti-tobacco industry attitudes and smoking cessation predictors (ie, intention to quit, attempt to quit smoking cigarettes); and (2) examine the differences of these relationships across peer crowds. We hypothesized that (1) anti-tobacco industry attitudes are positively associated with smoking cessation predictors, and (2) these relationships differ by peer crowd affiliation.
Methods
Design
A cross-sectional survey was conducted among 7871 young adult bar and club goers in 2015, in 7 US cities (Albuquerque, Los Angeles, Nashville, Oklahoma City, San Diego, San Francisco, and Tucson). Data were collected as part of a larger study evaluating the effectiveness of bar and nightclub interventions to decrease young adult smoking. The city selection process was convenience sampling to leverage partnerships with some local health departments funding interventions (Oklahoma City, Albuquerque) and to take advantage of existing infrastructure for research in all 7 cities. Participants were recruited using time–location sampling based on venues, dates, and times, a strategy suitable for difficult-to-reach populations.27 The lists of popular bars for young adults as well as common dates and times during which young adults were most likely to attend those bars were obtained through key informant interviews. Then random venues, dates, and times were selected from the lists for survey administration. More information about the study design is provided elsewhere.28
Samples
Participants aged 18 to 26 years old and not visibly intoxicated were invited to fill out a paper survey. Participants provided informed consent and received a $5 incentive. Of 7871 total respondents, 2817 participants reporting smoking cigarettes one day or more during the last 30 days were included in this analysis. To decrease participant burden while maximizing number and variety of questions, the survey instruments were developed using the 3-form planned missing design.29 Each of 3 survey versions contained a core set of 32 items (ie, demographics and tobacco use), and 2 variant sets of 46 form-specific questions (eg, anti-tobacco industry attitudes). This design is particularly well suited to the situation of bar surveys, where respondents face many distractions, so time burden, data quality, and response rate are critical issues to take into account.
Our study was approved by the Committee on Human Research of University of California San Francisco, and its ethics approval number is 10–02964.
Measures
Outcome variables.
The primary outcome was intention to quit smoking cigarettes in the next 6 months. The outcome was dichotomized such that participants who chose “will quit in the next month or 6 months” or “currently trying to quit” were coded as having an intention to quit. In contrast, those who chose “no plan to quit,” “may quit in future but not in the next 6 months,” or “don’t need to quit” were coded as having no intention to quit. Current smoking participants with recanting responses (ie, “already quit smoking,” “not smoked in the past 12 months”) were coded as missing.
The secondary outcome was measured by the item “During the past 12 months, have you stopped smoking for 1 day or longer because you were trying to quit?”; also dichotomized for data analyses. Participants who reported “have tried to quit” were coded as having attempted to quit. Conversely, participants reporting “had not tried to quit” or “don’t smoke enough to have to quit” were coded as not having attempted to quit. Similar to the primary outcome, those with the recanting responses were coded as missing.
Independent variable.
Based on our previous studies,8,11 anti-tobacco industry attitudes were measured by 3 items, “I want to be involved with efforts to get rid of cigarette smoking,” “I would like to see the cigarette companies go out of business,” and “Taking a stand against smoking is important to me.” The response score for each item ranged from 1—”Not at all” to 5—”A great deal,” with higher scores indicating higher support for action against the tobacco industry. The mean score across the 3 items was treated as a continuous variable in our analyses for reasons described previously.8,11
Peer crowd measure.
Peer crowd identification was measured using a photo-based measurement tool, the “I-Base Survey,” created by Rescue Agency.17,21 It included a grid of images of young adults that has demonstrated effectiveness and consistency in identifying health risk behaviors among common peer crowds across numerous studies and settings.3,17,30 Respondents were instructed to choose 3 photos that “best fit into their group of friends,” and 3 photos that “least fit into their group of friends.” These choices were scored (ie, 3, 2, 1 for “the best fit”; and −3, −2, −1 for “the least fit” based on rank) to assign people to peer crowds. The total score for each peer crowd ranged from −12 to 12. A single categorical variable was created based on the peer crowd with the highest score. For example, if a person scored 8 points on Hipster picture selection and 4 points on Partier picture selection, they would be classified as Hipster.
Other covariates.
Participants reported smoking within 30 minutes of waking, number of smoking days during the last 30 days, and average number of cigarettes per smoking day. We created a smoking intensity variable (average number of cigarettes consumed per day) by multiplying the number of days participants smoked during the last 30 days by the number of cigarettes they usually smoked each day on their smoking days, and then dividing the product by 30.31
Demographic characteristics (ie, age, gender, race/ethnicity, educational attainment, location) were obtained. Age was calculated based on self-reported date of birth. Race/ethnicity was measured by combining race (White, Black, Asian, Hawaiian/Pacific Islander, American Indian/Alaskan Native, or more than one race) and ethnicity (Hispanic or not). This variable was recoded into 5 categories (ie, “Non-Hispanic White,” “Non-Hispanic Black,” “Non-Hispanic Alaska Native/Pacific Islander,” “Non-Hispanic other,” and “Hispanic”). Educational attainment was categorized as “No college,” “In college,” and “College graduate.” These variables were dichotomized later in logistic models (“Other” vs “Non-Hispanic White” for race/ethnicity; and “In/graduate from college” vs “No college” for educational attainment). For binge drinking, participants were asked if they drank at least 5 shots/drinks for men or 4 shots/drinks for women within a few hours on one day or more during the last 30 days.
Analysis
Missing data issues were addressed using multiple imputation. The anti-tobacco industry attitude variables (36.6% missing) can be assumed to be missing completely at random due to the planned missing values from the 3-form study design. Several other variables (ie, intention to quit, attempt to quit, smoking within 30 minutes of waking) were missing due to contradictory responses. For example, current smokers later reported “never smoked” in the question for smoking within 30 minutes of waking (30.1%), or “not smoked in the past 12 months/quit smoking completely” in the questions for intention to quit (13.9%), and attempt to quit (11.2%). To address this, we assumed that the later contradictory responses were missing at random conditional on prior observed responses, and then imputed them later. We followed the recommendations of Moons et al to use all observed data in the imputation process,32 and imputed all variables (ie, predictors, covariates, outcomes) in the analysis model and other auxiliary variables (eg, smoking status). We applied multiple imputation via chained equations to create 50 imputed data sets, analyzed them using the logistic regression models described below, and then combined the estimates from the 50 logistic regression analyses. As recommended by Stern et al,33 we also conducted a robustness check by repeating all analyses using only complete data (without imputation).
Descriptive statistics were computed from the complete data for the total sample and for each peer crowd. Logistic regression models on imputed data were used to examine the association between anti-tobacco industry attitudes and smoking cessation predictors (ie, intention to quit, attempt to quit), adjusting for demographic variables (ie, age, gender, race/ethnic, education), binge drinking, and other smoking-related variables (eg, smoking within 30 minutes of waking, smoking intensity). These covariates were selected based on previous studies.4,8,34 The interaction term between anti-tobacco industry attitudes and peer crowd group was tested for each outcome. Only the interaction term for the outcome intention to quit was significant (data not shown). To interpret this significant interaction, we then conducted 6 additional logistic regression models to examine different effects of anti-tobacco industry attitudes on intention to quit for 6 peer crowd groups. All tests of hypotheses were 2-tailed with a significance level of α less than .05. Data were analyzed using Stata version 15.
Results
Sample Description
A description of the total sample and of each peer crowd is presented in Table 1. Participants were on average 23.89 years old (standard deviation [SD] = 2.29). The sample was predominantly female (57.43%), and racially/ethnically diverse with 44% non-Hispanic white and 31% Hispanic. Participants had relatively high levels of education with 38% currently enrolled and 35% graduated from college. Approximately one-third of the sample had an intention to quit smoking cigarettes in the next 6 months (33.17%), and 40.48% reported making at least one quit attempt in the last 12 months. Among the 6 peer crowds, the Hipster group made up the largest proportion of the sample (33.01%). The mean score on the anti-tobacco industry attitudes scale was 2.30 (SD = 1.10), with the lowest among the Country group (M = 2.15, SD = 1.12) and the highest among the Young Professional group (M = 2.43, SD = 1.12).
Table 1:
Characteristics of the Bar Survey Participants.
| Characteristics, n (%) | Total | Young Professional |
Homebody | Country | Partier | Hipster | Hip Hop |
|---|---|---|---|---|---|---|---|
| 2817 (100.0) | 368 (13.06) | 244 (8.66) | 270 (9.58) | 514 (18.25) | 930 (33.01) | 491 (17.43) | |
| Anti-tobacco industry attitudes, mean (SD) | 2.30 (1.10) | 2.43 (1.12) | 2.39 (1.17) | 2.15 (1.12) | 2.27 (1.10) | 2.30 (1.09) | 2.29 (1.07) |
| Efforts to get rid of cigarette smoking | 2.22 (1.18) | 2.33 (1.20) | 2.34 (1.32) | 2.05 (1.21) | 2.21 (1.16) | 2.23 (1.17) | 2.18 (1.13) |
| See the cigarette companies go out of business | 2.44 (1.30) | 2.62 (1.30) | 2.57 (1.37) | 2.29 (1.31) | 2.35 (1.25) | 2.47 (1.29) | 2.35 (1.28) |
| Against smoking is important | 2.26 (1.23) | 2.36 (1.26) | 2.27 (1.31) | 2.08 (1.22) | 2.26 (1.22) | 2.22 (1.19) | 2.32 (1.25) |
| Smoking characteristics | |||||||
| Intention to quit smoking | 826 (33.17) | 95 (30.45) | 78 (36.45) | 77 (31.69) | 132 (28.76) | 282 (34.06) | 162 (37.33) |
| Attempt to quit in the last year | 1023 (40.48) | 126 (37.39) | 93 (43.66) | 90 (38.63) | 169 (37.39) | 362 (42.79) | 183 (41.03) |
| Smoking within 30 minutes of waking | 566 (28.67) | 55 (23.40) | 56 (33.14) | 70 (35.11) | 118 (32.96) | 157 (23.19) | 110 (32.45) |
| Average cigarettes smoked per day, mean (SD) | 3.77 (6.86) | 2.53 (4.84) | 5.13 (9.91) | 5.20 (7.88) | 4.01 (7.62) | 3.73 (6.31) | 3.03 (5.41) |
| Demographic characteristics | |||||||
| Age, mean (SD) | 23.89 (2.29) | 24.10 (2.07) | 23.99 (2.16) | 23.63 (2.44) | 23.61 (2.20) | 24.14 (2.41) | 23.64 (2.21) |
| Gender | |||||||
| Male | 1172 (42.57) | 162 (44.75) | 107 (44.77) | 113 (43.80) | 192 (38.17) | 392 (43.12) | 206 (42.74) |
| Female | 1581 (57.43) | 200 (55.25) | 132 (55.23) | 145 (56.20) | 311 (61.83) | 517 (56.88) | 276 (57.26) |
| Race | |||||||
| NH white | 1223 (44.06) | 168 (46.80) | 103 (42.56) | 104 (38.81) | 224 (44.27) | 442 (48.31) | 182 (37.45) |
| NH black | 175 (6.30) | 17 (4.74) | 17 (7.02) | 28 (10.45) | 39 (7.71) | 32 (3.50) | 42 (8.64) |
| NH Alaska Native/Pacific Islander | 232 (8.36) | 42 (11.70) | 28 (11.57) | 23 (8.58) | 48 (9.49) | 60 (6.56) | 31 (6.38) |
| NH other | 289 (10.41) | 26 (7.24) | 34 (14.05) | 31 (11.57) | 52 (10.28) | 86 (9.40) | 60 (12.35) |
| Hispanic | 857 (30.87) | 106 (29.53) | 60 (24.79) | 82 (30.60) | 143 (28.26) | 295 (32.24) | 171 (35.19) |
| Education | |||||||
| In college | 1038 (37.60) | 128 (35.16) | 56 (23.73) | 103 (39.31) | 232 (46.59) | 311 (33.99) | 208 (42.80) |
| College graduate | 965 (34.95) | 169 (46.43) | 101 (42.80) | 78 (29.77) | 140 (28.11) | 331 (36.17) | 146 (30.04) |
| No college | 758 (27.45) | 67 (18.41) | 79 (33.41) | 81 (30.92) | 126 (25.30) | 273 (29.84) | 132 (27.16) |
| Location | |||||||
| Albuquerque | 191 (6.78) | 17 (4.62) | 13 (5.33) | 24 (8.89) | 35 (6.81) | 62 (6.67) | 40 (8.15) |
| Los Angeles | 546 (19.38) | 66 (17.93) | 49 (20.08) | 41 (15.19) | 105 (20.43) | 184 (19.78) | 101 (20.57) |
| Nashville | 343 (12.18) | 36 (9.78) | 27 (11.07) | 32 (11.85) | 78 (15.18) | 105 (11.29) | 65 (13.24) |
| Oklahoma | 498 (17.68) | 63 (17.12) | 38 (15.57) | 98 (36.30) | 83 (16.15) | 120 (12.90) | 96 (19.55) |
| San Diego | 445 (15.80) | 65 (17.66) | 37 (15.16) | 20 (7.41) | 54 (10.51) | 204 (21.94) | 65 (13.24) |
| San Francisco | 543 (19.28) | 91 (24.73) | 70 (28.69) | 38 (14.07) | 77 (14.98) | 192 (20.65) | 75 (15.27) |
| Tucson | 251 (8.91) | 30 (8.15) | 10 (4.10) | 17 (6.30) | 82 (15.95) | 63 (6.77) | 49 (9.98) |
| Binge drinking in the last 30 days | 2290 (86.91) | 308 (89.02) | 196 (85.22) | 217 (86.11) | 437 (89.55) | 733 (85.23) | 399 (86.93) |
Association Between Anti-Tobacco Industry Attitudes and Smoking Cessation Predictors
Results from multivariate logistic regressions are found in Table 2. After adjusting for other covariates, anti-tobacco industry attitudes were positively associated with both having an intention to quit and attempting to quit. Accordingly, participants had 1.37 greater odds of intent to quit (adjusted odds ratio, AOR = 1.37, 95% confidence interval [CI] = 1.24–1.52), and 1.14 greater odds to have made at least one attempt to quit (AOR = 1.14, 95% CI = 1.03–1.27) for each unit increase in their anti-tobacco industry attitude scores.
Table 2:
Factors Associated With Intention to Quit and Attempt to Quit Among all Study Participants.
| Variable | Intention to Quit AOR (95% CI) |
Attempt to Quit AOR (95% CI) |
|---|---|---|
| Anti-tobacco industry attitudes | 1.37*** (1.24–1.52) | 1.14* (1.03–1.27) |
| Peer crowd groups | ||
| Young Professional | Ref | Ref |
| Homebody | 1.39 (0.91–2.12) | 1.11 (0.75–1.67) |
| Country | 1.25 (0.82–1.90) | 0.96 (0.65–1.43) |
| Partier | 0.92 (0.64–1.33) | 1.03 (0.73–1.44) |
| Hipster | 1.14 (0.82–1.59) | 1.20 (0.89–1.61) |
| Hip Hop | 1.45* (1.00–2.10) | 1.00 (0.71–1.41) |
| Demographic factors | ||
| Age | 1.03 (0.99–1.07) | 0.99 (0.95–1.03) |
| Gender (female vs male) | 1.19 (0.98–1.46) | 1.24* (1.03–1.49) |
| Race (other vs non-Hispanic white) | 1.00 (0.82–1.22) | 0.92 (0.76–1.11) |
| Education (in/graduated from college vs No college) | 0.94 (0.76–1.16) | 0.86 (0.70–1.06) |
| Location | ||
| Albuquerque | Ref | Ref |
| Los Angeles | 0.76 (0.51–1.13) | 0.97 (0.66–1.43) |
| Nashville | 0.77 (0.50–1.20) | 0.99 (0.65–1.50) |
| Oklahoma | 0.7 (0.47–1.06) | 1.1 (0.74–1.64) |
| San Diego | 0.77 (0.51–1.18) | 0.71 (0.48–1.07) |
| San Francisco | 0.55** (0.36–0.84) | 0.83 (0.56–1.23) |
| Tucson | 0.78 (0.49–1.24) | 0.8 (0.51–1.26) |
| Smoking-related factors | ||
| Attempt to quit in the last year | 6.58*** (5.40–8.01) | Not Applicable |
| Intention to quit in the next 6 months | Not Applicable | 6.56*** (5.38–7.99) |
| Smoke within 30 minutes of waking | 1.1 (0.85–1.42) | 0.70** (0.55–0.89) |
| Average cigarette smoked per day | 0.99 (0.97–1.00) | 1.02* (1.00–1.03) |
| Binge drinking in the last 30 days | 1.02 (0.76–1.36) | 0.73* (0.56–0.95) |
Notes: AOR, adjusted odds ratio; 95%CI = 95% confidence interval;
P < 0.05
P < 0.01
P < 0.001
In addition, the 2 outcomes were strongly correlated with each other. Participants who attempted to quit in the last year had 6.58 times the odds of having intention to quit in the next 6 months (AOR = 6.58,95% CI = 5.40–8.01) and vice versa. The Hip Hop group was more likely to have intentions to quit compared to the Young Professional group (AOR = 1.45, 95% CI = 1.00–2.10). Participants who were female (vs male; AOR = 1.24, 95% CI = 1.03–1.49) or smoked more cigarettes per day (AOR = 1.02, 95% CI = 1.00–1.03) were more likely to attempt to quit smoking, while smoking within 30 minutes of waking (AOR = 0.70, 95% CI = 0.55–0.89) and binge drinking (AOR = 0.73, 95% CI = 0.56–0.95) reduced the odds of attempting to quit.
Differential Associations Between Anti-Tobacco Industry Attitudes and Intention to Quit Across Peer Crowds
The interaction between anti-tobacco industry attitudes and peer crowd was only significant for intention to quit, but not for having made a quit attempt (data not shown). Differential associations between anti-tobacco industry attitudes and intention to quit across peer crowds are displayed in Figure 1. Among the 6 peer crowds, there was a significant positive association between anti-tobacco industry attitudes and intention to quit in 4 groups (Table 3). The adjusted odds ratios were highest for Homebody (AOR = 1.90, 95% CI = 1.29–2.81), followed by Hipster (AOR = 1.41, 95% CI = 1.16–1.72), Partier (AOR = 1.38, 95% CI = 1.07–1.79), and Hip Hop (AOR = 1.35, 95% CI = 1.04–1.77). For the other covariates, attempt to quit was consistently associated with intention to quit for all 6 peer crowd groups, while average cigarettes smoked per day was negatively associated with intention quit only for the Country group (AOR = 0.93, 95% CI = 0.88–0.99); and gender (female vs male) was positively associated with intention quit only for Young Professionals (AOR = 2.12, 95% CI = 1.13–3.99).
Figure 1.
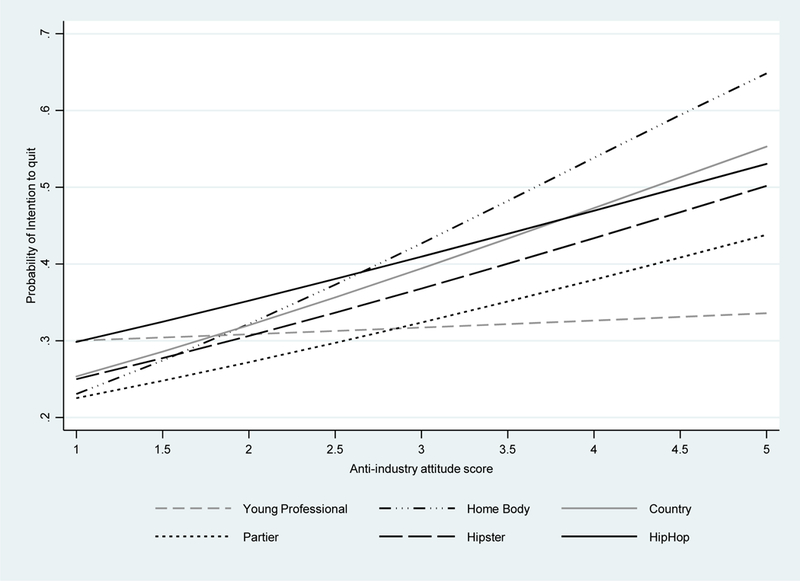
Differential associations between anti-tobacco industry attitudes and intention to quit across young adult peer crowds.
Table 3:
Differential Associations Between Anti-Tobacco Industry Attitudes and Intention to Quit Across Young Adult Peer Crowds.a
| Significant Variables, AOR (95% CI) |
Young Professional, N = 368 |
Homebody, N = 244 |
Country, N = 270 |
Partier, N = 514 |
Hipster, N = 930 |
Hip Hop, N = 49l |
|---|---|---|---|---|---|---|
| Independent variable | ||||||
| Anti-tobacco industry attitudes | 1.13 | 1.90b | 1.52 | 1.38c | 1.41d | 1.35c |
| (0.84 – 1.53) | (1.29 – 2.81) | (1.00 – 2.32) | (1.07 – 1.79) | (1.16 – 1.72) | (1.04 – 1.77) | |
| Significant Covariates | ||||||
| Gender (Female vs. Male) | 2.12c (1.13–3.99) |
|||||
| Attempt to quit in the last year | 6.82d | 7.97d | 15.79d | 5.12d | 7.47d | 5.41d |
| (3.81–12.22) | (3.69–17.19) | (7.20–34.62) | (3.14–8.37) | (5.30–10.54) | (3.42–8.56) | |
| Average cigarettes smoked per day | 0.93c (1.13– 0.99) |
|||||
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Only significant variables with P < .05 in the multivariate analyses are shown. All models were adjusted for demographic characteristics, binge drinking, and smoking-related factors.
P < .01.
P < .05.
P < .001.
Robustness Analyses Among Complete Data (Listwise Deletion)
Robustness analyses showed similar results but slightly larger adjusted odds ratios. Anti-tobacco industry attitudes were still associated with intention to quit (AOR = 1.50, 95% CI = 1.30–1.73) and attempt to quit (AOR = 1.38, 95% CI = 1.20–1.59). The positive impact of anti-tobacco industry attitudes also differed across peer crowds only for intention to quit. However, the significance and magnitude of AORs in subgroup analyses were slightly different from the results from the imputed data set with significant associations for Homebody (AOR = 2.43, 95% CI = 1.38–4.27), Country (AOR = 2.87, 95% CI = 1.28–6.42), Partier (AOR = 1.46, 95% CI = 1.00–2.11), and Hipster (AOR = 1.46, 95% CI = 1.13–1.88).
Discussion
This study examined the impact of anti-tobacco industry attitudes on intentions to quit and quit attempts among young adult smokers. Consistent with previous research,8,9,11,14,35 we found significant positive relationships between anti-tobacco industry attitudes and both smoking cessation predictors. The current study replicates these relationships among a more current sample of bar patrons in 7 cities, and provides further evidence that anti-tobacco industry messages may promote intention to quit and quit attempts among young adult smokers. While the positive impact of anti-tobacco industry attitudes on intention to quit is found in our study and others (eg, the “truth” national campaign,14 the 2002 California tobacco survey,8 and the 2005 national panel survey11), the effect sizes differ across studies. These differences could be due to variations in assessments of the anti-industry attitudes and adjustments for different covariates in the data analyses across studies. Furthermore, our study focused on a high-risk population of young adult bar patrons, and found fewer respondents reported intention to quit smoking in the next 6 months (33.17%) and having made a least one quit attempt in the last year (40.48%) than those reported from the 2011 National Young Adult Health Survey (64.4% and 60.6%, respectively).36 Likewise, our sample also reported lower anti-industry attitude scores than the general young adult population.3 Taken together, interventions to promote anti-smoking attitudes and smoking cessation should prioritize the bar population.
While prior studies have shown the relationship between antitobacco industry attitudes and tobacco use cessation,10 few have explored moderating factors, and even fewer within the young adult population, an important target for the industry.6 Our study extends the literature by exploring how this relationship differs across 6 young adult peer crowds. We found positive associations for 4 crowds (Hipster, Hip Hop, Homebody, and Partier), but not the Country and Young Professional crowds. This intriguing finding suggests that peer crowd identity may moderate the relationship between anti-industry attitudes and intention to quit. In practice, anti-industry messages may promote cessation among certain peer crowds, particularly some high-risk groups (eg, Hipster, Hip Hop, and Partier), while it may not be effective for the Country and Young Professional groups.
In the early 2000s, the “truth” campaign contributed to the significant reduction of adolescent and young adult’s tobacco use rates across the United States.37 However, smoking rates among rural youths and young adults did not decrease at the same rate as those among their urban and suburban peers.38 Since the Country peer crowd is more common in rural areas, our findings may help explain why the campaign focused on anti-industry messaging was less successful in these areas. Formative research focus groups with Country teens and young adults have found that this peer crowd has strong procorporate values and prioritizes individual responsibility (J. W. Jordan, MA, personal communication, May 27, 2018). When shown ads focused on anti-industry messages, participants often responded with confusion about what the industry has to do with their personal decision to smoke. In contrast, the lack of an association within the Young Professionals peer crowd is harder to understand. One possible explanation is that since Young Professional young adults have the lowest tobacco use rate across all peer crowds,3,17 those who are motivated by anti-industry attitudes may have already quit due to exposure to campaigns like “truth,” and the remaining Young Professional smokers might require a different message. Future research should further explore potential alternate messages that may more effectively motivate these peer crowds to quit smoking.
Collectively, our findings suggest that anti-tobacco industry messages that are tailored based on peer crowd affiliation may be an effective approach to promote intention to quit smoking among young adult bar patrons. Developing anti-industry messages that resonate with unique peer crowd values can enhance the relatability and relevance of health communication materials. Since each peer crowd has its own values and attitudes that influence how messages are processed and retained,16,39 tobacco control practitioners should tailor anti-industry messages appropriately. For example, the Commune anti-tobacco campaign, targeting Hipsters in California, focused on working with local artists to expose specific industry practices that affect issues Hipsters are passionate about, such as animal testing, environmental protection, and world hunger.22 Since Hipsters value many of these issues, the Commune campaign is able to deliver more in-depth messaging showing Hipsters how smoking goes against their beliefs. In contrast, messaging to the Hip Hop peer crowd may be more powerful by focusing on the tobacco industry’s targeting of minority populations, particularly with menthol products21 (see Figure 2). In addition, practitioners should be open to the possibility that anti-industry messages will not align with the values of some audiences, despite the success these messages have had with other populations. As the tobacco industry has demonstrated with their own advertising, one message does not fit all.
Figure 2.

Examples of peer crowd-tailored anti-tobacco industry messaging: Hipster ads (top row) emphasizing environmental and social impact of tobacco production; and Hip Hop ads (bottom row) emphasizing minority community targeting. Both strategies may utilize adbusting (left column).
Several limitations should be considered. First, due to the cross-sectional design, we cannot establish temporal or causal relationships between anti-tobacco industry attitudes and smoking cessation predictors. Second, our self-reported data is subject to recall and socially desirability biases. Third, our bar sample and the nonrandom city selection process within the context of a larger intervention study may restrict the generalizability of our results to other populations or locations.
In conclusion, anti-tobacco industry attitudes are significantly associated with smoking cessation predictors, with different impacts for intention to quit by peer crowd affiliation. Integrating anti-industry content into tailored peer crowd interventions to promote intention to quit smoking may be a relevant strategy to reduce tobacco use among some of the highest risk young adults.
So What.
What is Already Known on This Topic?
Although tobacco industry denormalization and peer crowd targeting are important strategies to decrease young adult smoking, the impact of anti-tobacco industry attitudes on smoking cessation predictors among different peer crowds has not been examined.
What Does This Article Add?
This study found that there is a differential relationship between anti-industry attitudes and intention to quit smoking across 6 young adult peer crowds, suggesting that peer crowd affiliation may moderate the relationship between anti-industry attitudes and intention to quit.
What Are the Implications for Health Promotion Practice or Research?
Developing health communication messages that resonate with unique peer crowd values can enhance the relevance of public health campaigns. Integrating anti-industry content into tailored peer crowd interventions to promote intention to quit smoking may be a relevant strategy to reduce tobacco use among some of the highest risk young adults.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Cancer Institute at NIH (Grant Number U01-CA154240 and T32 113710).
Footnotes
Declaration of Conflicting Interests
References
- 1.Kasza KA, Ambrose BK, Conway KP, et al. Tobacco-product use by adults and youths in the United States in 2013 and 2014. N Engl J Med. 2017;376(4):342–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Villanti AC, Gaalema DE, Tidey JW, Kurti AN, Sigmon SC, Higgins ST. Co-occurring vulnerabilities and menthol use in U. S. Young adult cigarette smokers: findings from wave 1 of the PATH Study, 2013–2014. Prev Med. 2018;117:43–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ling PM, Holmes LM, Jordan JW, Lisha NE, Bibbins-Domingo K. Bars, nightclubs, and cancer prevention: new approaches to reduce young adult cigarette smoking. Am J Prev Med. 2017; 53(3S1):S78–S85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jiang N, Ling PM. Impact of alcohol use and bar attendance on smoking and quit attempts among young adult bar patrons. Am J Public Health. 2013;103(5):e53–e61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hendlin Y, Anderson SJ, Glantz SA. ‘Acceptable rebellion’: marketing hipster aesthetics to sell Camel cigarettes in the US. Tob Control. 2010;19(3):213–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ling PM, Glantz SA. Why and how the tobacco industry sells cigarettes to young adults: evidence from industry documents. Am J Public Health. 2002;92(6):908–916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zucker D, Hopkins RS, Sly DF, Urich J, Kershaw JM, Solari S. Florida’s “truth” campaign: a counter-marketing, anti-tobacco media campaign. J Public Health Manag Pract. 2000;6(3):1–6. [DOI] [PubMed] [Google Scholar]
- 8.Ling PM, Neilands TB, Glantz SA. The effect of support for action against the tobacco industry on smoking among young adults. Am J Public Health. 2007;97(8):1449–1456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hammond D, Fong GT, Zanna MP, Thrasher JF, Borland R. Tobacco denormalization and industry beliefs among smokers from four countries. Am J Prev Med. 2006;31(3):225–232. [DOI] [PubMed] [Google Scholar]
- 10.Malone RE, Grundy Q, Bero LA. Tobacco industry denormalisation as a tobacco control intervention: a review. Tob Control. 2012;21(2):162–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ling PM, Neilands TB, Glantz SA. Young adult smoking behavior: a national survey. Am J Prev Med. 2009;36(5):389–394. e382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hershey JC, Niederdeppe J, Evans WD, et al. The theory of “truth”: how counterindustry campaigns affect smoking behavior among teens. Health Psychol. 2005;24(1):22–31. [DOI] [PubMed] [Google Scholar]
- 13.Farrelly MC, Nonnemaker J, Davis KC, Hussin A. The influence of the national truth campaign on smoking initiation. Am J Prev Med. 2009;36(5):379–384. [DOI] [PubMed] [Google Scholar]
- 14.Richardson AK, Green M, Xiao H, Sokol N, Vallone D. Evidence for truth(R): the young adult response to a youth-focused anti-smoking media campaign. Am J Prev Med. 2010;39(6): 500–506. [DOI] [PubMed] [Google Scholar]
- 15.Vallone D, Cantrell J, Bennett M, et al. Evidence of the Impact of the truth FinishIt Campaign. Nicotine Tob Res. 2018;20(5): 543–551. [DOI] [PubMed] [Google Scholar]
- 16.Moran MB, Walker MW, Alexander TN, Jordan JW, Wagner DE. Why peer crowds matter: incorporating youth subcultures and values in health education campaigns. Am J Public Health. 2017;107(3):389–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lisha NE, Jordan JW, Ling PM. Peer crowd affiliation as a segmentation tool for young adult tobacco use. Tob Control. 2016; 25(suppl 1):i83–i89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sussman S, Pokhrel P, Ashmore RD, Brown BB. Adolescent peer group identification and characteristics: a review of the literature. Addict Behav. 2007;32(8):1602–1627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ling PM, Glantz SA. Using tobacco-industry marketing research to design more effective tobacco-control campaigns. JAMA. 2002;287(22):2983–2989. [DOI] [PubMed] [Google Scholar]
- 20.Hafez N, Ling PM. Finding the Kool Mixx: how Brown & Williamson used music marketing to sell cigarettes. Tob Control. 2006;15(5):359–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Walker MW, Navarro MA, Hoffman L, Wagner DE, Stalgaitis CA, Jordan JW. The Hip Hop peer crowd: an opportunity for intervention to reduce tobacco use among at-risk youth. Addict Behav. 2018;82:28–34. [DOI] [PubMed] [Google Scholar]
- 22.Ling PM, Lee YO, Hong J, Neilands TB, Jordan JW, Glantz SA. Social branding to decrease smoking among young adults in bars. Am J Public Health. 2014;104(4):751–760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fallin A, Neilands TB, Jordan JW, Hong JS, Ling PM. Wreaking “havoc” on smoking: social branding to reach young adult “partiers” in Oklahoma. Am J Prev Med. 2015;48(1 suppl 1): S78–S85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kalkhoran S, Lisha NE, Neilands TB, Jordan JW, Ling PM. Evaluation of bar and nightclub intervention to decrease young adult smoking in new Mexico. J Adolesc Health. 2016;59(2): 222–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moran MB, Murphy ST, Sussman S. Campaigns and cliques: variations in effectiveness of an antismoking campaign as a function of adolescent peer group identity. J Health Commun. 2012; 17(10):1215–1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Comello M Conceptualizing the intervening roles of identity in communication effects In: America Rodriguez LLR, ed. Identity and Communication: New Agendas in Communication. New York, NY: Routledge; 2013:168–188. [Google Scholar]
- 27.Muhib FB, Lin LS, Stueve A, et al. A venue-based method for sampling hard-to-reach populations. Public Health Rep. 2001; 116(suppl 1):216–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lisha NE, Neilands TB, Jordan JW, Holmes LM, Ling PM. The social prioritization index and tobacco use among young adult bar patrons. Health Educ Behav. 2016;43(6):641–647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Graham JW, Taylor BJ, Olchowski AE, Cumsille PE. Planned missing data designs in psychological research. Psychol Methods. 2006;11(4):323–343. [DOI] [PubMed] [Google Scholar]
- 30.Jordan JW, Stalgaitis CA, Charles J, Madden PA, Radhakrishnan AG, Saggese D. Peer crowd identification and adolescent health behaviors: results from a statewide representative study [published online February 1, 2018]. Health Educ Behav. 2018:1090198118759148. [DOI] [PubMed] [Google Scholar]
- 31.Yao T, Ong MK, Max W, et al. Responsiveness to cigarette prices by different racial/ethnic groups of US adults. Tob Control. 2018; 27(3):301–309. [DOI] [PubMed] [Google Scholar]
- 32.Moons KG, Donders RA, Stijnen T, Harrell FE Jr. Using the outcome for imputation of missing predictor values was preferred. J Clin Epidemiol. 2006;59(10):1092–1101. [DOI] [PubMed] [Google Scholar]
- 33.Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Weinberger AH, Pilver CE, Hoff RA, Mazure CM, McKee SA. Changes in smoking for adults with and without alcohol and drug use disorders: longitudinal evaluation in the US population. Am J Drug Alcohol Abuse. 2013;39(3):186–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kushnir V, Selby P, Cunningham JA. Association between tobacco industry denormalization beliefs, tobacco control community discontent and smokers’ level of nicotine dependence. Addict Behav. 2013;38(7):2273–2278. [DOI] [PubMed] [Google Scholar]
- 36.Villanti AC, Bover Manderski MT, Gundersen DA, Steinberg MB, Delnevo CD. Reasons to quit and barriers to quitting smoking in US young adults. Fam Pract. 2016;33(2): 133–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Farrelly MC, Davis KC, Haviland ML, Messeri P, Healton CG. Evidence of a dose-response relationship between “truth” anti-smoking ads and youth smoking prevalence. Am J Public Health. 2005;95(3):425–431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bonnie RJ, Stratton K, Kwan LY. Public Health Implications of Raising the Minimum Age of Legal Access to Tobacco Products Washington, DC: Board on Population Health and Public Health Practice; Institute of Medicine; 2015. [PubMed] [Google Scholar]
- 39.Moran MB, Sussman S. Translating the link between social identity and health behavior into effective health communication strategies: an experimental application using antismoking advertisements. Health Commun. 2014;29(10):1057–1066. [DOI] [PMC free article] [PubMed] [Google Scholar]