

Abstract
A prominent coved or saddle-shaped ST-segment elevation followed by T wave changes in V1-V3 and in the absence of other identifiable cause is termed as Brugada pattern. This pattern in the presence of documented ventricular arrhythmias or its symptoms (syncope, seizure) or significant family for sudden cardiac death or abovementioned ECG changes is called Brugada syndrome. Here we present a comprehensive literature review on the precipitation factors of Brugada syndrome/pattern by various stimuli, its presentation, associations, management and outcomes. We are also presenting a unique case of Brugada pattern where the patient’s Brugada pattern was unmasked at an extreme old age by infection.
Keywords: cardiovascular medicine, arrhythmias
Background
The burden of Brugada syndrome is not well studied as it is very rare; however, the prevalence of asymptomatic Brugada pattern appears to vary among different populations ranging between 0.1% and 1% depending on the population.1 2 Highest reported prevalence was in the city of Japan that is about 0.7% and 1.0%; however, in USA, these numbers were 0.4% and 0.012% in two different reports.3 Most studies have focused on regional distribution and ECG patterns of the Brugada syndrome or Brugada pattern. There has been no review to unmask the possible precipitating factors, management and outcome of this potentially fatal clinical condition. In this study, we reviewed and analysed 65 patients and given a comprehensive review.
Case presentation
An 82-year-old man with a medical history of advanced Parkinson’s disease, prior left cerebellar infarct and swallowing dysfunction presented to the hospital with generalised weakness and loss of appetite for a few days. Review of systems was significant for productive cough that had started the night before presentation, along with non-bloody diarrhoea in the preceding week. His blood pressure was 141/67, with a heart rate of 75. He was saturating 93% while breathing ambient air and was afebrile. He was unable to contribute to the history due to lethargy. An ECG showed normal sinus rhythm and an intraventricular conduction delay (figure 1).
Figure 1.
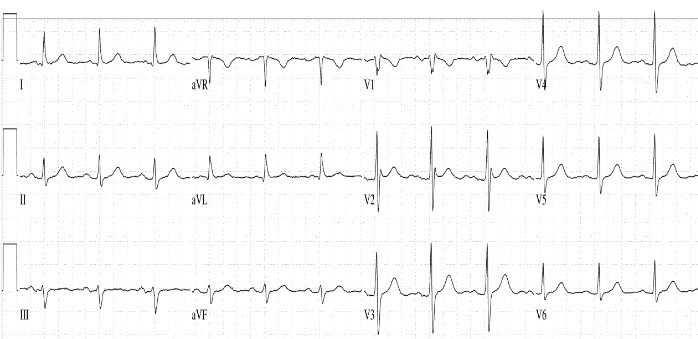
ECG showing normal sinus rhythm and no signs of ischaemia.
Within few hours of admission, he mounted a fever of 102 F. He suddenly became hypoxic and complained of chest pain to his nurse. A rapid response team was called. Vitals were now a blood pressure of 99/54 mm Hg, heart rate of 111 beats/min, temperature of 102.9°F (39.3°C) and saturating 94% on 4 L of oxygen via nasal cannula.
Investigations
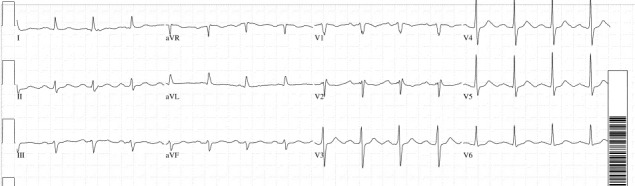
His blood work was unremarkable for any abnormality. His serum potassium 4.5 mEq/L, Mg 2.3 mg/dL. His renal and liver functions were also normal. An ECG was obtained that showed sinus tachycardia with prolonged PR interval along with new ST-segment elevations in leads V1 and V2, with reciprocal ST depressions in the inferior leads (figure 2). Patient was now very lethargic and not complaining of any chest pain. Repeat ECG within few minutes revealed worsening ST elevations in V1 and V2 with concurrent worsening of the reciprocal changes.
Figure 2.

ECG showing coved ST-segment elevation with T wave inversion in V1 and V2 consistent with type 1 Brugada pattern.
ST elevation mycoardial infarction (STEMI) alert was called and left heart catheterisation revealed no obstructive coronary disease (figures 3 and 4). Ventriculogram showed normal EF with no regional wall motion abnormalities. His ECG changes continued to evolve with post catheterisation ECG showing downsloping ST elevations in V1 and V2, ultimately having ECG returning to normal (figure 5).
Figure 3.
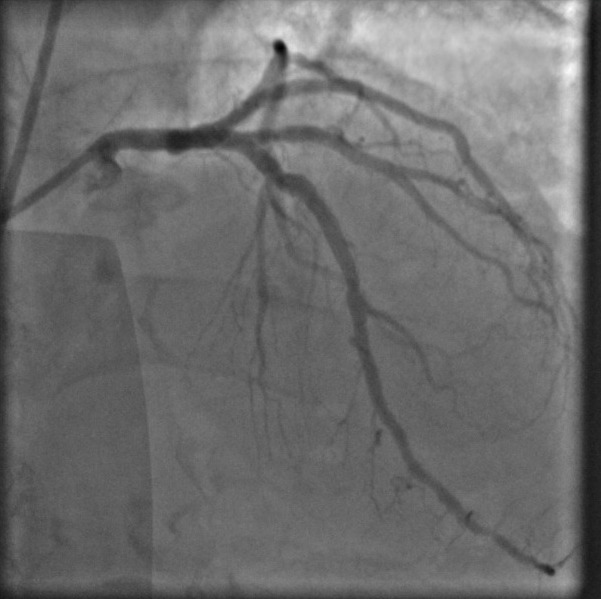
Left coronary artery on angiography is clean with no obstruction.
Figure 4.

Right coronary artery on angiography does not show any obstruction.
Figure 5.
ECG shows resolution of the ST elevation.
A D-dimer was added on to his admission labs and found to be elevated at more than 5250 ng/mL (normal 0–230 ng/mL). CT scan ruled out pulmonary embolism but showed multifocal infiltrates and raised suspicion for aspiration as debris was seen in the trachaea along with a distended oesophagus. CT scan of the head did not reveal any new abnormalities and urinalysis was unremarkable.
Differential diagnosis
The differential diagnosis included coronary artery disease and pulmonary embolism which were excluded by unremarkable coronary angiography and CT scan. The reason for high D-dimers in our patient was twofold, his pneumonia and increased age. Increased age has been noted to be associated with high D-dimers levels. The patient was on carbidopa–levodopa for Parkinson’s disease (Sinemet), but not on any drug such as digoxin, quinidine, tricyclics which can cause ST-segment changes. Other differentials were the long PR interval, early repolarisation, acute pericarditis, non-specific physiologic phenomena, such as ingestion of food, postural changes, emotional stress, hyperventilation, or central nervous system injuries, abnormalities in left ventricular wall motion, electrolyte disturbances, use of drugs or heart failure.4
Treatment
He was then admitted to the general medical floor and started on antibiotics for coverage of community-acquired pneumonia and aspiration pneumonia. During the episode of ST-segment changes a rectal aspirin was given, and percutaneous intervention (PCI) alert was activated.
Outcome and follow-up
His blood pressure, fever and respiratory status improved after a few days on antibiotics. His mental status improved slowly and returned to baseline in a few days. His further hospital stay was complicated by faecal impaction which was treated successfully. He was found to be aspirating on swallow evaluation and after discussions regarding goals of care, he eventually received a gastrostomy tube for feeding before discharge. An ECG later in the course was similar to his admission ECG without any ST changes. Given patient’s waxing and waning neurological status and recurrent aspirations, his family opted for comfort-directed care and he was discharged to home hospice. Unfortunately, the genetic testing could not be performed due to his condition and the family was also unavailable.
Discussion
Brugada syndrome was first recognised in 1992 by the professor of cardiology Dr Brugada. It is the constellation of specific ECG patterns in addition to history of sustained ventricular arrhythmias or patient may experience syncope or sudden cardiac death. Asymptomatic ECG patterns are termed as Brugada pattern and these patterns can be persistently present or they are unmasked by a number of different stimuli. Some of the triggers for Brugada pattern are the infection, fever, toxins and medications especially flecainide and procainamide.5
We did a comprehensive literature search using different Medical Subject Heading (MeSH) terms and reviewed all the available literature on unmasking or new onset of Brugada pattern and Brugada syndrome. Our search revealed a total of 65 cases as mentioned in online supplementary table 1.6–70 The mean age of the reported patients was 42 years (1.5–80) with 85% (n=60) males and 15% (n=11) females. These patients were admitted to the hospital for reasons other than their arrhythmia. Fever was present on admission in 100% of the patients. Other signs included cough in 21%, sore throat in 12%, chest pain in 11%, syncope in 10%, abdominal pain and diarrhoea in 5% of the patient population. The ultimate reason or diagnosis which led to the unmasking of Brugada pattern was mostly found to be pneumonia in 31% (n=21) and upper respiratory tract infections in 7% (n=5) of the patients. Less common causes included cholecystitis, tonsillitis and pharyngitis, each affecting 4% (n=3) of the patients. Each of the infection, cellulitis and malaria affected 3% (n=2) of the patients. Only one patient had asthma, haemophagocytic syndrome, sepsis, syncope and ventricular fibrillation each. More than 60% patients had no reported comorbidities. Comorbidities in rest of the patient population included smoking 11% (n=8), dyslipidaemia 4% (n=3), hypertension 5% (n=4) while each of myasthenia, alcoholism and HIV infection affected one patient. There was an incidence of positive family history of Brugada pattern in about 13% (n=9) patients. Brugada pattern without symptoms was present in 62% (n=40) while Brugada syndrome was revealed in 38% (n=25) of the patients. Management in most of the asymptomatic Brugada pattern patients was directed towards treating the underlying cause. Pneumonia in all 31% cases was managed with antibiotics and malaria in 2% cases was managed with antimalarials. About 17% (n=7) of the patients with Brugada pattern and 76% (n=19) of the patients with Brugada syndrome ended up getting implantable cardioverter-defibrillator (ICD) which added up to 38% (n=26) of the total population with ICD. Interestingly more than 77% patients had a successful resolution of ECG changes and symptoms after the treatment of the inciting triggers and they were discharged in stable condition. Only two patients succumbed to the arrhythmias which could be attributed to the old age and extensive comorbidities in the setting of Brugada pattern. There was no mention of outcome in about 20% patients. Compared with other subjects included in the literature review, our patient was unique in term of his age and never had a cardiovascular disease or other mentioned comorbidities. His initial ECG was normal and the transient Brugada pattern was completely reversed in 1 day during the same hospitalisation with treatment of underlying condition. It is important to note that our patient is the first reported case where the Brugada pattern revealed itself at this age; the oldest age reported as per our review was 80 years by Pontollio. The number of cases presented after 70 years age was less than 1% in this review. This highlights the fact that ST elevation in old age could be benign Brugada pattern rather than coronary artery disease in the appropriate clinical settings.
bcr-2019-229829supp001.pdf (65.9KB, pdf)
Patients with Brugada pattern on ECG without any history of syncope or cardiac arrest carry 8% risk of new arrhythmic events in the first 27 months.71 These high-risk patients with normal baseline ECG can be diagnosed by provocative testing such as administration of sodium channel blockers (flecainide or procainamide).72 Fever may also serve as a good provocative test to elicit the Brugada pattern.73 Our findings are consistent with previous studies showing that Brugada pattern is about 20 times more common in febrile patients as compared with afebrile patients. Interestingly, these patients can remain asymptomatic upto a 30 months of follow-up.73
The pathogenesis of Brugada pattern is complex and about 21 different genetic mutations have been described including sodium channel SCN genes and right ventricular abnormalities.72 74 However, only 30%–35% of patients with this pattern actually have mutations on genetic testing, highlighting that there are other mechanisms involved in the pathogenesis.72 Due to these observations, it is recommended to do ECG screening rather than genetic testing to the patient’s family members.
Brugada syndrome is diagnosed with combination of ECG patterns and clinical presentation. Brugada pattern on ECG may present with three different patterns. Type 1 is 2 mm coved ST segment or J point elevation followed by negative T wave. Type 2 is saddleback appearance of T wave with at least 1 mm elevation of ST segment or 2 mm elevation of J point followed by positive or biphasic T wave.5 Type 3 is either coved or saddleback appearance with >1 mm ST-segment elevation.5 6 Three types of clinical criteria used to diagnose the disease include data from family history (ECG type 1 pattern at any age or sudden cardiac death in family members with less than 45 years of age), ventricular arrhythmias (polymorphic ventricular tachycardia or ventricular fibrillation) and symptoms of arrhythmias (syncope, seizures). Combination of type 1 Brugada pattern and at least one of the clinical criteria is definitive for Brugada syndrome while type 2 or type 3 pattern on ECG with at least one clinical criterion is suggestive of Brugada syndrome.5 In our patient, type 1 pattern was present with coved ST-segment elevation and T wave inversion on leads V1 and V2. This pattern made him high risk for Brugada syndrome. In 2013 consensus statement was issued by three major heart societies that in the presence of clinically significant symptoms and ECG changes whether in response to provocative testing or spontaneously should mark the diagnosis of Brugada syndrome.75 Our patient’s ECG showed type 1 Brugada pattern but he did not have clinical symptoms or family history to label it as Brugada syndrome.
Brugada pattern is managed by treating the triggering factor, avoiding the responsible toxins and medications while patients being labelled as Brugada syndrome based on ECG pattern and clinical presentation of family history should have an automatic implantable cardioverter defibrillator (AICD) placed to avoid sudden cardiac death.75 For patients who refuse AICD or have recurrent AICD shocks due to arrhythmias, low-dose quinidine or amiodarone should be started. If patients develop side effects or become intolerant to these medications, radiofrequency catheter ablation can significantly reduce the arrhythmias burden.76 Patients with the Brugada ECG pattern who experience atrial fibrillation have a higher risk of future ventricular tachyarrhythmias and sudden cardiac deaths.
Learning points.
Physicians should have a high index of suspicion for Brugada pattern even at the extreme of ages with no family history of sudden cardiac deaths.
It is important to rule out coronary artery disease before labelling any patient with Brugada pattern.
Careful distinction should be made between Brugada pattern and Brugada syndrome based on clinical presentation and family history.
This comprehensive review summarised the demographic and clinical trend of the disease with a very reassuring outcome provided the inciting event is tackled in time.
AICD placement should be offered to every patient with Brugada pattern on ECG if criterion for Brugada syndrome is being fulfilled.
Footnotes
Contributors: SR performed data extraction and helped in references. HA managed the case and wrote presentation. WU wrote discussion. AA reviewed the article. GG did a critical review and supervision.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Next of kin consent obtained.
References
- 1. Gehi AK, Duong TD, Metz LD, et al. Risk stratification of individuals with the Brugada electrocardiogram: a meta-analysis. J Cardiovasc Electrophysiol 2006;17:577–83. 10.1111/j.1540-8167.2006.00455.x [DOI] [PubMed] [Google Scholar]
- 2. Miyasaka Y, Tsuji H, Yamada K, et al. Prevalence and mortality of the Brugada-type electrocardiogram in one city in Japan. J Am Coll Cardiol 2001;38:771–4. 10.1016/S0735-1097(01)01419-X [DOI] [PubMed] [Google Scholar]
- 3. Patel SS, Anees S, Anees SS, et al. Prevalence of a Brugada pattern electrocardiogram in an urban population in the United States. Pacing Clin Electrophysiol 2009;32:704–8. 10.1111/j.1540-8159.2009.02354.x [DOI] [PubMed] [Google Scholar]
- 4. Hanna EB, Glancy DL. ST-segment elevation: Differential diagnosis, caveats. Cleve Clin J Med 2015;82:373–84. 10.3949/ccjm.82a.14026 [DOI] [PubMed] [Google Scholar]
- 5. Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 2005;111:659–70. 10.1161/01.CIR.0000152479.54298.51 [DOI] [PubMed] [Google Scholar]
- 6. Bernardo MH, Tiyyagura SR. A Case of Type I and II Brugada Phenocopy Unmasked in a Patient with Normal Baseline Electrocardiogram (ECG). Am J Case Rep 2018;19:21–4. 10.12659/AJCR.906464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Nagy SZ, Chan CF. Brugada syndrome unmasked by febrile illness in a previously healthy male patient with history of syncope. Heart 2012;98:1610 10.1136/heartjnl-2012-302379 [DOI] [PubMed] [Google Scholar]
- 8. Vieira MB, Gaibino N, Pignatelli A, et al. Fever-triggered Brugada syndrome in an adult patient presenting with hemophagocytic syndrome induced by Chlamydophila pneumoniae. BMJ Case Rep 2015;2015:bcr2014208863 10.1136/bcr-2014-208863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Mendes SL, Elvas L, Ramos D, et al. Fever in an elderly patient unmasks Brugada syndrome. Rev Port Cardiol 2017;36:317–8. 10.1016/j.repc.2016.07.014 [DOI] [PubMed] [Google Scholar]
- 10. Sharma AK, Lama L, Heist EK. Brugada pattern induced by fever. Indian Heart J 2015;67:159–60. 10.1016/j.ihj.2015.02.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Madeira M, Caetano F, Providência R, et al. Fever-induced type 1 Brugada pattern. Rev Port Cardiol 2015;34:287.e1–287.e7. 10.1016/j.repc.2014.10.002 [DOI] [PubMed] [Google Scholar]
- 12. López-Caleya JF, Fernández-Diéguez MO, Martín-Rodrigo L, et al. [Brugada type I associated with cellulitis: Review and update]. Semergen 2016;42:e22–4. 10.1016/j.semerg.2015.01.016 [DOI] [PubMed] [Google Scholar]
- 13. Boda S, Mishra PC, Naik BS. Diagnosis of Brugada syndrome during fever: a case report from a tertiary care centre. J Assoc Physicians India 2014;62:617. [PubMed] [Google Scholar]
- 14. Martins J, Braga C, Arantes C, et al. Syncope in a febrile state: A case report of Brugada syndrome. Revista Portuguesa de Cardiologia 2014;33:801.e1–801.e6. 10.1016/j.repce.2014.07.002 [DOI] [PubMed] [Google Scholar]
- 15. Washington CH, Issaranggoon na ayuthaya S, Makonkawkeyoon K, et al. A 9-year-old boy with severe diphtherial infection and cardiac complications. BMJ Case Rep 2014;2014:bcr2014206085 10.1136/bcr-2014-206085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Mody P, Pandey A, Joglar J. Fever-Induced Electrocardiographic Changes. J Gen Intern Med 2015;30:136–7. 10.1007/s11606-014-2992-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Domínguez-Lenogue S, Amoros-García R, Sierra-Bergua B, et al. [A fever that exposed: presentation of 2 cases of Brugada syndrome]. Semergen 2014;40:347–9. 10.1016/j.semerg.2013.12.002 [DOI] [PubMed] [Google Scholar]
- 18. Juhasz Z, Tiszlavicz L, Kele B, et al. Sudden cardiac death from parvovirus B19 myocarditis in a young man with Brugada syndrome. J Forensic Leg Med 2014;25:8–13. 10.1016/j.jflm.2014.04.018 [DOI] [PubMed] [Google Scholar]
- 19. Picetti E, Zoerle T, Cattani L, et al. Fever and Brugada syndrome: a dangerous combination. Minerva Anestesiol 2014;80:512–3. [PubMed] [Google Scholar]
- 20. Meggiolaro M, Zorzi A, El Maghawry M, et al. Brugada ECG disclosed by acute malaria: is it all about fever and propofol? J Clin Anesth 2013;25:483–7. 10.1016/j.jclinane.2013.02.012 [DOI] [PubMed] [Google Scholar]
- 21. Mirijello A, Addolorato G, Landolfi R. Brugada electrocardiographic findings in an 80-year-old man. Case Rep Child Meml Hosp Chic 2013;2013:bcr2013010226 10.1136/bcr-2013-010226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Pontillo D, Patruno N. Brugada syndrome ECG pattern and fever: too warm is bad. J Cardiovasc Med 2015;16 Suppl 1:S4 10.2459/JCM.0b013e3283600a3e [DOI] [PubMed] [Google Scholar]
- 23. Kumar V, Patel N, Van Houzen N, et al. Brugada-type electrocardiographic changes induced by fever. Circulation 2013;127:2145–6. 10.1161/CIRCULATIONAHA.112.000901 [DOI] [PubMed] [Google Scholar]
- 24. Zhou Y, Wang J, Li X, et al. ST-T-wave alternans in Brugada electrocardiogram type I pattern during the resolution of febrile states: case report-online article. Cardiovasc J Afr 2013;24:1–3. [DOI] [PubMed] [Google Scholar]
- 25. Gandhi S, Kuo A, Smaggus A. The management of Brugada syndrome unmasked by fever in a patient with cellulitis. Case Rep Child Meml Hosp Chic 2013;2013:bcr2013009063 10.1136/bcr-2013-009063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Noris M, Carrillo A, Campuzano O, et al. Syncope and polymorphic ventricular tachycardia in the setting of a febrile illness. J Electrocardiol 2013;46:666–9. 10.1016/j.jelectrocard.2013.01.006 [DOI] [PubMed] [Google Scholar]
- 27. Shea Y-fung, Mok M-yeeM, Fang JX. Transient Brugada electrocardiogram pattern associated with Tenchkoff catheter exit site infection. Nephrology 2013;18:239–40. 10.1111/nep.12016 [DOI] [PubMed] [Google Scholar]
- 28. Yalin K, Gölcük E, Bilge AK, et al. Brugada type 1 electrocardiogram unmasked by a febrile state following syncope. Turk Kardiyol Dern Ars 2012;40:155–8. 10.5543/tkda.2012.01725 [DOI] [PubMed] [Google Scholar]
- 29. Wynne J, Littmann L. Brugada electrocardiogram associated with pulmonary embolism. Int J Cardiol 2013;162:e32–e33. 10.1016/j.ijcard.2012.05.059 [DOI] [PubMed] [Google Scholar]
- 30. Traub D, Fonseka N, Priori S. ST-segment elevation in the setting of a febrile illness. Ann Noninvasive Electrocardiol 2011;16:303–7. 10.1111/j.1542-474X.2011.00445.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. De Marco S, Giannini C, Chiavaroli V, et al. Brugada syndrome unmasked by febrile illness in an asymptomatic child. J Pediatr 2012;161:769–769.e1. 10.1016/j.jpeds.2012.04.034 [DOI] [PubMed] [Google Scholar]
- 32. Barra S, Providência R, Nascimento J. Fever outperforms flecainide test in the unmasking of type 1 Brugada syndrome electrocardiogram. EP Europace 2013;15:394 10.1093/europace/eus175 [DOI] [PubMed] [Google Scholar]
- 33. Grogan SP, Cube RP, Edwards JA. Brugada syndrome unmasked by fever. Mil Med 2011;176:946–9. 10.7205/MILMED-D-10-00458 [DOI] [PubMed] [Google Scholar]
- 34. Zaidi AN. An Unusual Case of Brugada Syndrome in a 10-year-old Child with Fevers. Congenit Heart Dis 2010;5:594–8. 10.1111/j.1747-0803.2010.00382.x [DOI] [PubMed] [Google Scholar]
- 35. Johnson JM, Thomas TM, Wilson CM, et al. A 24-year-old man with subjective fever and syncope. J Emerg Nurs 2010;36:336–7. 10.1016/j.jen.2009.12.008 [DOI] [PubMed] [Google Scholar]
- 36. Labra González R, Casares Medrano J, Sánchez Castaño Ángel José, et al. Síndrome de Brugada asintomático precipitado por una infección por el virus de la gripe pandémica (H1N1) 2009. Medicina Clínica 2011;136:226–7. 10.1016/j.medcli.2010.01.023 [DOI] [PubMed] [Google Scholar]
- 37. Ozben B, Caymaz O, Erdoğan O. Fever-induced precordial ST-segment elevation in a young man. Turk Kardiyol Dern Ars 2010;38:35–7. [PubMed] [Google Scholar]
- 38. Alla VM, Suryanarayana PG, Kaushik M. Temperature Twist. Am J Med 2010;123:127–30. 10.1016/j.amjmed.2009.10.004 [DOI] [PubMed] [Google Scholar]
- 39. Lacunza J, San Román I, Moreno S, et al. Heat stroke, an unusual trigger of Brugada electrocardiogram. Am J Emerg Med 2009;27:634.e1–634.e3. 10.1016/j.ajem.2008.09.036 [DOI] [PubMed] [Google Scholar]
- 40. Serletis-Bizios A, Azevedo ER, Singh SM. Unmasking of Brugada syndrome during a febrile episode. Can J Cardiol 2009;25:239 10.1016/S0828-282X(09)70079-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Patanè S, Marte F, La Rosa FC, et al. Revelation of Brugada electrocardiographic pattern during a febrile state. Int J Cardiol 2010;140:e19–e21. 10.1016/j.ijcard.2008.11.069 [DOI] [PubMed] [Google Scholar]
- 42. Shalev A, Zeller L, Galante O, et al. Symptomatic Brugada unmasked by fever. Isr Med Assoc J 2008;10:548. [PubMed] [Google Scholar]
- 43. Shinohara T, Takahashi N, Saikawa T, et al. Brugada syndrome with complete right bundle branch block disclosed by a febrile illness. Intern Med 2008;47:843–6. 10.2169/internalmedicine.47.0791 [DOI] [PubMed] [Google Scholar]
- 44. Hanazawa K, Tamura T, Doi T, et al. [Severe arrythmic events triggered by fever in a case of Brugada syndrome]. Nihon Naika Gakkai Zasshi 2007;96:2516–8. 10.2169/naika.96.2516 [DOI] [PubMed] [Google Scholar]
- 45. Ambardekar AV, Lewkowiez L, Krantz MJ. Mastitis unmasks Brugada syndrome. Int J Cardiol 2009;132:e94–e96. 10.1016/j.ijcard.2007.07.154 [DOI] [PubMed] [Google Scholar]
- 46. Ott P, Freund NS. Brugada-pattern EKG in a febrile patient. J Emerg Med 2007;33:281–2. 10.1016/j.jemermed.2007.02.052 [DOI] [PubMed] [Google Scholar]
- 47. Skinner JR, Chung SK, Nel CA, et al. Brugada syndrome masquerading as febrile seizures. Pediatrics 2007;119:e1206–e1211. 10.1542/peds.2006-2628 [DOI] [PubMed] [Google Scholar]
- 48. Gavrielatos G, Letsas KP, Pappas LK, et al. Brugada electrocardiographic pattern induced during febrile state with marked leukocytosis. Pacing Clin Electrophysiol 2007;30:135–6. 10.1111/j.1540-8159.2007.00589.x [DOI] [PubMed] [Google Scholar]
- 49. Sovari AA, Prasun MA, Kocheril AG, et al. Brugada syndrome unmasked by pneumonia. Tex Heart Inst J 2006;33:501. [PMC free article] [PubMed] [Google Scholar]
- 50. Unlu M, Bengi F, Amasyali B, et al. Brugada-like electrocardiographic changes induced by fever. Emerg Med J 2007;24:e4 10.1136/emj.2006.041202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Karakitsos D, Patrianakos A, Poularas J, et al. Brugada-like electrocardiographic pattern unmasked by fever in a critical care patient. Acta Anaesthesiol Scand 2006;50:1038–9. 10.1111/j.1399-6576.2006.01091.x [DOI] [PubMed] [Google Scholar]
- 52. Suzuki T, Kohsaka S. Brugada-type electrocardiographic changes in a febrile patient of african descent. Am J Med Sci 2006;332:97–9. 10.1097/00000441-200608000-00010 [DOI] [PubMed] [Google Scholar]
- 53. Keller D, Huang H, Zhao J, et al. A novel SCN5A mutation, F1344S, identified in a patient with Brugada syndrome and fever-induced ventricular fibrillation. Cardiovasc Res 2006;70:521–9. 10.1016/j.cardiores.2006.02.030 [DOI] [PubMed] [Google Scholar]
- 54. Wakita R, Watanabe I, Okumura Y, et al. Brugada-like electrocardiographic pattern unmasked by fever. Jpn Heart J 2004;45:163–7. 10.1536/jhj.45.163 [DOI] [PubMed] [Google Scholar]
- 55. Kusaka K, Yamakawa J, Kawaura K, et al. Brugada-like electrocardiographic changes during influenza infection. J Int Med Res 2003;31:244–6. 10.1177/147323000303100313 [DOI] [PubMed] [Google Scholar]
- 56. Patruno N, Pontillo D, Achilli A, et al. Electrocardiographic pattern of Brugada syndrome disclosed by a febrile illness: clinical and therapeutic implications. Europace 2003;5:251–5. 10.1016/S1099-5129(03)00029-1 [DOI] [PubMed] [Google Scholar]
- 57. Ortega-Carnicer J, Benezet J, Ceres F, et al. Fever-induced ST-segment elevation and T-wave alternans in a patient with Brugada syndrome. Resuscitation 2003;57:315–7. 10.1016/S0300-9572(03)00057-1 [DOI] [PubMed] [Google Scholar]
- 58. Mok NS, Priori SG, Napolitano C, et al. A newly characterized SCN5A mutation underlying Brugada syndrome unmasked by hyperthermia. J Cardiovasc Electrophysiol 2003;14:407–11. [DOI] [PubMed] [Google Scholar]
- 59. Kum LC, Fung JW, Sanderson JE. Brugada syndrome unmasked by febrile illness. Pacing Clin Electrophysiol 2002;25:1660–1. [DOI] [PubMed] [Google Scholar]
- 60. Porres JM, Brugada J, Urbistondo V, et al. Fever unmasking the Brugada syndrome. Pacing Clin Electrophysiol 2002;25:1646–8. 10.1046/j.1460-9592.2002.01646.x [DOI] [PubMed] [Google Scholar]
- 61. Morita H, Nagase S, Kusano K, et al. Spontaneous T wave alternans and premature ventricular contractions during febrile illness in a patient with Brugada syndrome. J Cardiovasc Electrophysiol 2002;13:816–8. 10.1046/j.1540-8167.2002.00816.x [DOI] [PubMed] [Google Scholar]
- 62. Saura D, García-Alberola A, Carrillo P, et al. Brugada-like electrocardiographic pattern induced by fever. Pacing Clin Electrophysiol 2002;25:856–9. 10.1046/j.1460-9592.2002.t01-1-00856.x [DOI] [PubMed] [Google Scholar]
- 63. Das A, Gupta A, Das S. ST segment elevations in a patient with neutropenic fever. Eur J Intern Med 2017;40:e7–e8. 10.1016/j.ejim.2016.12.004 [DOI] [PubMed] [Google Scholar]
- 64. Tessitore E, Ramlawi M, Tobler O, et al. Brugada Pattern Caused by a Flecainide Overdose. J Emerg Med 2017;52:e95–e97. 10.1016/j.jemermed.2016.10.045 [DOI] [PubMed] [Google Scholar]
- 65. Porto AG, Dametto E, Piazza R, et al. Atypical electrocardiographic presentation of Brugada syndrome. Int J Cardiol 2016;223:651–3. 10.1016/j.ijcard.2016.08.125 [DOI] [PubMed] [Google Scholar]
- 66. Stankovic I, Janicijevic A, Neskovic AN. Transient left ventricular dysfunction during fever-induced Brugada-like electrocardiographic pattern. Europace 2016;18:1607 10.1093/europace/euw042 [DOI] [PubMed] [Google Scholar]
- 67. Khalid N, Chhabra L, Kluger J. Pyrexia-induced Brugada phenocopy. J Ayub Med Coll Abbottabad 2015;27:228–31. [PubMed] [Google Scholar]
- 68. Singla A, Coats W, Flaker GC. A 46-year-old man with fever, ST-segment elevation. Cleve Clin J Med 2011;78:286–8. 10.3949/ccjm.77a.10099 [DOI] [PubMed] [Google Scholar]
- 69. Baranchuk A, Simpson CS. Brugada syndrome coinciding with fever and pandemic (H1N1) influenza. Can Med Assoc J 2011;183:582 10.1503/cmaj.100016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Siniorakis E, Arvanitakis S, Psatheris G, et al. Recurrence of fever-related Brugada pattern and right ventricular functional correlates. Int J Cardiol 2011;148:370–2. 10.1016/j.ijcard.2010.09.069 [DOI] [PubMed] [Google Scholar]
- 71. Brugada J, Brugada R, Antzelevitch C, et al. Long-term follow-up of individuals with the electrocardiographic pattern of right bundle-branch block and ST-segment elevation in precordial leads V1 to V3. Circulation 2002;105:73–8. 10.1161/hc0102.101354 [DOI] [PubMed] [Google Scholar]
- 72. Juang J-MJ, Horie M. Genetics of Brugada syndrome. J Arrhythm 2016;32:418–25. 10.1016/j.joa.2016.07.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Junttila MJ, Gonzalez M, Lizotte E, et al. Induced Brugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Circulation 2008;117:1890–3. 10.1161/CIRCULATIONAHA.107.746495 [DOI] [PubMed] [Google Scholar]
- 74. Priori SG, Napolitano C, Gasparini M, et al. Natural history of Brugada syndrome: insights for risk stratification and management. Circulation 2002;105:1342–7. [DOI] [PubMed] [Google Scholar]
- 75. Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm 2013;10:1932–63. 10.1016/j.hrthm.2013.05.014 [DOI] [PubMed] [Google Scholar]
- 76. Kusumoto FM, Bailey KR, Chaouki AS, et al. Systematic review for the 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018;72:1653–76. 10.1016/j.jacc.2017.10.052 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bcr-2019-229829supp001.pdf (65.9KB, pdf)