

Abstract
Background
The information for the impact of air pollutants on the severity of chronic obstructive pulmonary disease (COPD) and hospital admissions in Bulgaria is scarce. The aim of the study is to assess the relationship between some ambient air pollution and exacerbations levels as well as hospital admissions of patients with COPD in Bulgaria.
Methods
A multi-center, prospective, one-year observational study was conducted among 426 COPD patients. Data from pollution monitoring are collected from the Executive Environment Agency (EEA).
Results
The results showed that the pollution with sulfur dioxide (SO2) is less than limit concentrations recommended by the European Union and World Health Organization (WHO), while the pollution with PM exceeds limits values of WHO two times. The mean rate of exacerbations in selected towns are between 0.5–3, the number of exacerbations with hospitalization are between 0.2–1.8 and length of hospital stay is between 1–14 days.
Conclusions
The study confirms that air pollution leads to increased number of exacerbations and hospital stay. The patients with mild level of COPD have 0.86 exacerbations and 2.61 days in hospital per year, while in case of very severe COPD these values increase 4 times. Outside pollutions lead to worsening of the disease severity and hospitalizations due to a higher rate of COPD exacerbations.
Keywords: Air pollution, particulate matter, chronic obstructive pulmonary disease (COPD), exacerbations, hospital stay
Introduction
Air pollution has a wide variety of harmful effects on humans. The levels of pollutants are high in urban areas due to the concentration of pollution sources from traffic, industry, power plants and households (1,2). In 2014, 92% of the world population was living in places exposed to air pollutants with levels considered dangerous by World Health Organization (WHO) (3).
Commonly measured pollutants are gaseous air pollutants sulfur dioxide (SO2), ozone (O3), carbon oxide (CO), nitrogen dioxide (NO2) and particle matters with size 10 microns (PM10) and 2.5 microns (PM2.5). PMs are the major causes of acute and chronic respiratory diseases (4). Worldwide, it is estimated that PM causes about 25% of lung cancer mortality, 8% of chronic obstructive pulmonary disease (COPD) mortality, and about 15% of ischaemic heart disease and stroke (5). The pollutants are associated with those diseases and have effects even at short-term low levels of exposure fluctuations (4,6,7).
COPD is a progressive disease associated with a chronic inflammatory process in the airways and the lungs, resulting in respiratory disturbance, reduced quality of life and increased mortality (8). During the disease the airflow obstruction and exacerbation frequencies associated with poorer health status are high, which lead to increased hospitalizations, morbidity and mortality (9). Exacerbations of existing COPD are defined as “a short-term episodes during which the normal inflammatory process is enhanced” (9). Mechanisms of acute exacerbation of respiratory symptoms in COPD are investigated in a number of studies (10,11). Exacerbations are associated with predominantly airway inflammation, a systemic inflammatory response or viral infection (11). The potential mechanisms of exacerbations also depend on circulating particles into the blood stream which create vascular dysfunction with potential systemic effects, air pollutant-related oxidative stress which damage the epithelium of the airways and reduce the immune response (12). COPD patients have also more particle deposits in the lung (12).
The relationships between levels of ambient air pollution and an increase in COPD exacerbations and hospitalizations has been investigated by many authors (8,9,13-16). There is scarce information for the effects of different pollutants on the severity of COPD and hospital admissions in Bulgaria although it is the most polluted country in Europe in terms of PM10 for 2012, followed by Poland and Slovakia. The percentage of population in Bulgaria exposed to excessive PM10 levels in 2012 is close to 90% while in the EU it is above 38% (17).
Fine particle pollution remains a major problem in some large cities in Bulgaria (18). The diseases of respiratory system have significant economic and social burden and are one of the major reasons for hospitalization in the country (19,20). It is known that 9.7% of hospitalized patients in the country suffered from COPD (21). The number of hospitalizations for COPD patients between 2013–2014 years in BG are 13,600–15,240. Hospitalization rate due to COPD exacerbations remains relatively stable among 18–19%. There are data for COPD disease in high-risk groups such as smokers (22,23). Pharmaco-economic studies about pharmacotherapy of COPD is published in the literature (24,25). The relationship between air pollution level, ambient temperature and exacerbations in COPD patients in one city was studied but there is no information about the global pollution in the country (19). That was the reason to focuss our attention on this problem.
The aim of the study is to assess the association between some ambient air pollutants and exacerbations levels as well as and hospital admissions of patients with COPD in Bulgaria.
Our ultimate goal is to assess the progress of COPD and present the trend of the severity of the illness in a period of four years following the chosen cohort of patients. In this context we focus our study on the relationship between exposure to major air pollutions (PM10 and SO2) and exacerbations levels as well as hospital admissions of COPD patients at the beginning of the period under consideration.
Methods
Study population
According to experts from the Bulgarian Society of Pulmonary Diseases, the total number of COPD patients in Bulgaria is about 480,000, but records from the National Health Insurance Fund showed that only part of them are diagnosed with COPD (81,218 patients for 2014) and obtained reimbursed medicines (25,26). A multi-center, prospective, one-year observational study was performed. The study period was between April 2015 and May 2016 and included 426 patients recruited from 16 towns across the country. A general population was stratified according to the residence of the surveyed persons. There are five strata: living in Sofia-town, Northwestern, Northeastern, Southwest and Southeast Bulgaria. A sample size of 405 COPD patients was considered nationally representative. Sample sizes for every stratum were determined based on estimated number of COPD patients and the number of citizens in every region. Statistical calculations were prepared with the standard error 5% and the probability 99%. The target values of patients for five strata were 180 people from Sofia, 30 from Northwestern, 77 from Northeastern, 29 from Southwest and 89 from Southeast Bulgaria. The final volume of the sample was 426. The actual number of COPD patients consist of 143 people from Sofia, 38 from Northwestern, 76 from Northeastern, 58 from Southwest and 111 from Southeast Bulgaria (27).
Patient recruitment
COPD patients in Bulgaria are registered by a pulmonologist who perform spirometry and manage their therapy. Patients are obliged to visit their pulmonologist at least twice per year, but in case of emergencies specialists’ visits could be more frequently. The selection of patients was accomplished as every fifth person who visited a pulmonologist in the span of the period under consideration (April 2015 and May 2016) and agreed to participate in the study. The information about patients’ age, gender and disease duration, combined assessment of COPD per GOLD guidelines 2015, spirometry data and treatment were recorded in a registration form by the pulmonologist. The patients who participated in the study were followed between April 2015 and May 2016 and information about hospital emergency room visits, number of exacerbations and treatment were included in their registration form. Combined assessment of COPD was based on patient characteristics (demographic data, symptoms), degree of bronchial obstruction (measured through spirometry), number and severity of exacerbations per year, degree of dyspnea according to physical activity (mMRC), and results from COPD Assessment Test (CAT) for assessing quality of life (28).
Environmental data
Sixteen towns were included in the study which are situated near the pollution sources like industry, solid fuel combustion and power plants where the level of PM and other pollution is high. The analyses of air pollution were performed for every town. The pollution level in chosen cities for particulate matter PM10 and level of air pollution with SO2 was described based on data from pollution monitoring, collected by the Executive Environment Agency (EEA) (29). If in some town more than one station exists in the assessment of daily exposure to pollution the values were averaged. The information on the state of atmospheric air from all monitoring stations is received at a central dispatch point in the EEA. The data is real-time in the National Database and is preliminary. The daily average values of particulate matter and sulfur dioxide were calculated and then averaging over every month. The final data is published in the quarterly bulletins issued by the EEA after verification. The averaged value of the pollutants for observed period was used. The concentration limits of pollutants are the same as those accepted by EU according to Regulation of the Ministry of Environment and Waters and the Ministry of Health (30). The methodology of the assessment of pollution is similar like those described by Choi et al. 2018 (31).
Statistical analysis
Data were analyzed using MedCalc ver.17.9.7 (MedCalc Software). Data for number of exacerbations, hospital stay, and air pollutions are reported as mean ± SD using descriptive statistics. The association between the incidence rate of PM10 or SO2 concentration and number of exacerbations or hospital stay was analyzed using linear and non-linear regression analyses.
Results
The COPD hospitalization and emergency visits as well as lung function and respiratory symptoms was investigated according to methodology described in the study of Heinrich & Schikowski (8), The potential vulnerability of COPD patients to air pollution was assessed by documenting over on one-year period. Out of the 426 patients 296 were men (69.48%) and 130 were women (30.52%). Average patient age was 66.66±9.08 years (27).
The durability of COPD was evaluated to be between 5.5 and 15 years. The average duration of disease was 9.56±6.09 years. The relationship between durability and the number of exacerbations is presented in Figure 1 The number of exacerbations are at least one for about 90% of patients. For up to 10 years of durability of COPD the number of exacerbations is between 0.5 and 2.7 but when durability is over 10 years the exacerbations are over 1.5 per year minimum which correspond to severe and very severe state of COPD. The correlation between number of exacerbations and the days in hospitalizations was also established and it is high with r2=0.62 (Figure 2). Number of exacerbations increases with worsening of patient health and are proportional to hospital admissions. The exacerbations were divided into two groups due to severity—with and without admission to hospital. The numbers of exacerbations with hospital admission per patient per year are proportional to days in hospital with high correlation coefficient of r2=0.98 (Figure 3). Patients from stage A and B according to GOLD stay in hospital between 2–4 days, while patients with more than one exacerbations (stage C and D)—between 8–14 days.
Figure 1.
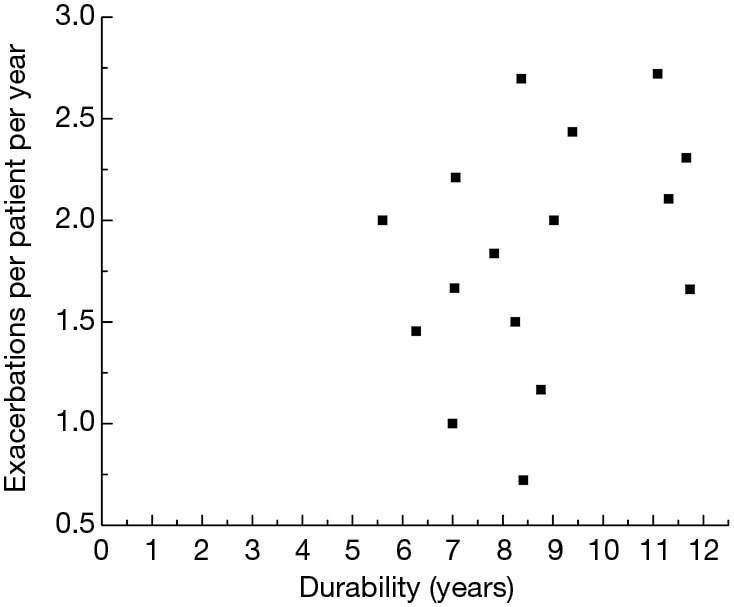
The durability and number of exacerbations per patient per year.
Figure 2.
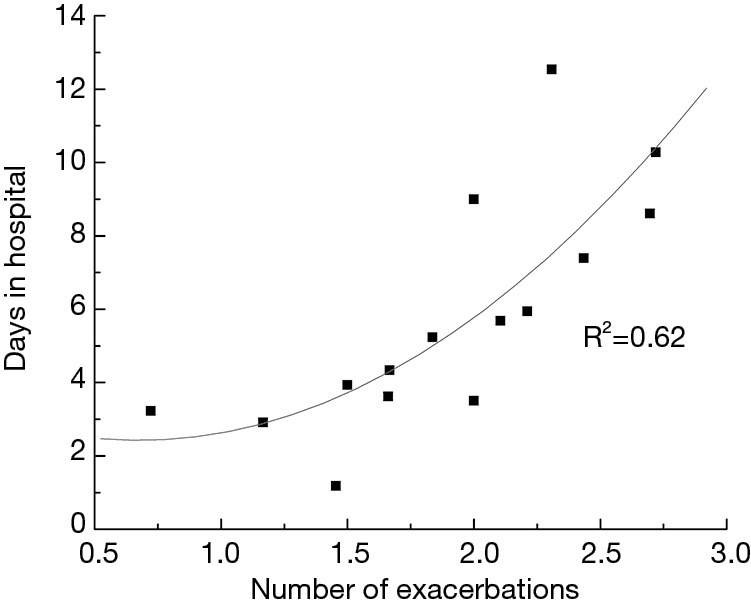
The correlation between number of exacerbations and hospital admissions.
Figure 3.
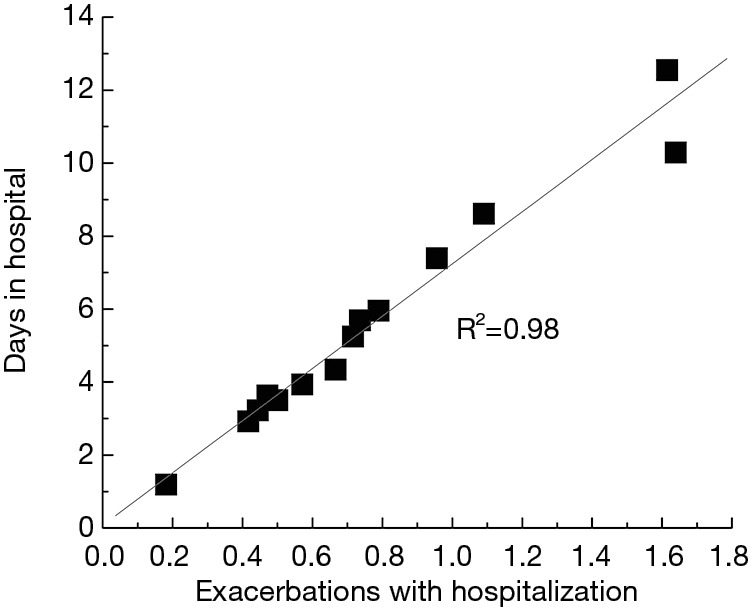
The numbers of exacerbations with hospital admission per patient per year.
The number of exacerbations, exacerbations with hospitalization and stay in a hospital were presented according to severity of COPD (Table 1). The severity of COPD leads to increased number of exacerbations and days of hospital stay. The patients with mild COPD have 0.87 exacerbations and 2.61 days in hospital per year, while the values for patients with very severe COPD are 3.6 and 13 days in hospital per year respectively.
Table 1. The number of exacerbations, severe exacerbations which need admission to hospital and stay in hospital.
| Severity | Exacerbations | Days in hospital | Severe exacerbations which need stay in hospital |
|---|---|---|---|
| Mild | 0.87±0.03 | 2.61±0.17 | 0.22±0.02 |
| Moderate | 1.28±0.01 | 3.71±0.04 | 0.52±0.01 |
| Severe | 2.73±0.01 | 7.26±0.05 | 0.94±0.01 |
| Very severe | 3.59±0.02 | 12.79±0.15 | 1.77±0.02 |
The average air pollution of the cities was calculated for one-year period (April 2015–May 2016) and for year 2010 also for the purposes of comparison.
During the investigated period the values of PM10 is changing in interval (33.66–65.48 µg/m3). The mean pollution with PM10 is 41.54±8.77 µg/m3. The towns were divided according to the level of air pollution in two groups. Those with PM10 under 40 µg/m3—group A and towns which limit of concentration is over 40 µg/m3—group B.
The average value for towns in group A was 34.99±2.61 µg/m3 and for towns in group B was 46.63±8.03 µg/m3. The number of exacerbations was presented according to pollution with PM10 (Figure 4). The results show that the average number of exacerbations are more than 1 in all but two towns. In places where the pollution with PM10 is under 40 µg/m3 the average number of exacerbations per patient per year is 1.8±0.07, severe exacerbations which lead to hospital admission are 0.68±0.06 and days in hospital are 4.96±0.36. There is an increase in the number of exacerbations (1.8±0.07 vs. 1.97±0.04) and days in hospital (4.96±0.36 vs. 5.94±0.13) with increasing of pollution with PM10. The number of severe exacerbations with hospital admission (0.68±0.06 vs. 0.66±0.02) do not increase with PM10 pollution because they depend on administration mainly. The obtained results are not significantly different because of the close values of pollution levels with PM10 (34.99±2.61 vs. 46.63±8.03 µg/m3) (Figure 4).
Figure 4.

Exacerbations per patient according to level of pollution. (A) PM10; (B) SO2.
The results about ambient pollution showed that SO2 is in the range of 3.72–20.17 µg/m3. The average pollution with SO2 is 10.54±3.07 µg/m3. The towns which pollution with PM10 is under 40 µg/m3 the average pollution with SO2 was 10.41±1.92 µg/m3 and the level of SO2 in the towns from group B is 10.64±4.22 µg/m3 for SO2. All towns, except one have mean value of SO2 under 20 µg/m3.
The established annual trends for pollutant SO2 and PM10 showed a decrease in the emissions and improvement of air quality in Bulgaria in the last 5 years. Mean values of PM10 decreases on average with 7.2 µg/m3. The mean pollution with PM10 for investigated towns for 2010 is 49.81±11.11 µg/m3 while the mean pollution for 2015 is 41.54±8.77 µg/m3. The differences between polluted and non-polluted towns become closer. In 2010 this was 35.32±1.49 vs. 50.98±9.85 µg/m3 while in 2015 was 34.99±2.61 vs. 46.63±8.03 µg/m3. In all but one town the air became less polluted.
Discussion
The pollutants contribute strongly to smog formation and air pollution with the growth of urban centers and climate change (8). In areas with a high content of SO2 in the ambient air, the concentration of dust is also high and we investigated this fact for BG towns. The mean weekly levels of PM10 were found to correlate with the mean weekly levels of SO2 (19). The content of SO2 in the air of all towns under consideration is under the limit of 20 µg/m3.
The pollution with PM10 in the country is very close to the EU limit value—40 µg/m3. In only two towns the pollution is more than 20% higher than the mean annual value of 41.54±8.77 µg/m3. However, there are no towns in BG where PM10 levels are below the annual WHO air quality guideline level of 20 µg/m3. In the recent decade a decrease in the emissions of the main atmospheric pollutants and improvement of the air quality in the country was reported probably because of accepted restrictions by the local authorities and applied integrated policies to reduce dust emissions and to use cleaner modes of transport. However, in some populated areas—predominantly large cities, pollution remains still a major problem (18).
The systematic reviews and original research papers that focused on the exacerbation and progression of COPD in relation to exposure to ambient air pollutants showed that air pollution leads to exacerbations and hospitalization and as a consequence to reduced pulmonary function (9,13,14). Systematic reviews and meta-analysis from 26 papers published between 1995 and 2015 reported that the risks for COPD mortality and COPD hospital admission, ranging between 2% and 3%, increase with elevation of PM2.5 or PM10 levels (8). COPD hospitalization and emergency room visits were affected by an exposure to SO2. An increase per 10 µg/m3 for SO2 leads to 2.1% more emergency room visits (9). Another meta-analysis, which combines 59 studies, revealed a short-term effect of all pollutants on the levels of COPD exacerbation (16). Choi et al. also concluded that air pollution increases the incidence of events such as COPD-hospitalizations and exacerbations (31). Our study supports those results with the relation between the exacerbations with hospitalization and air pollution.
Hospitalization and exacerbation rates are also dependent on the disease severity, the presence of previous comorbidities, a history of exacerbation and treatment of the patient (32). The annual rate of COPD exacerbations has been estimated from 9 studies in the work of Seemungal et al. (15). The exacerbations are between 0.5 to 3.5 per patient per year. Albert et al. after screening in clinical trial a total of 1,577 subjects reported that the frequency of exacerbations was 1.48–1.83 per patient-year according to the prescribed treatment (33). We also obtained similar results 0.87–3.59 exacerbations rate per patients per year or average exacerbations per patient per year are 2.23±0.02.
Patients who have acute exacerbations of COPD, as compared with patients with COPD who do not have acute exacerbations, have an increased risk of death, a more rapid decline in lung function, and reduced quality of life. Most of the patients from our cohort are between 61–80 years (68.78%) and have lived with the disease for 11–20 years. A total of 86.6% of patients in cohort have acute exacerbations and were accepted in hospital.
A study included 234 hospitals in the UK showed an in-hospital mortality of 7% and a 90-day mortality of 15% following admission for COPD exacerbations (34). The acute exacerbations of COPD were found to be independent indicators of a poor prognosis. The patients with the greatest mortality risk were those with three or more acute COPD exacerbations (HR 4.13, 95% CI: 1.80 to 9.41) (35). According to our study the average exacerbations with hospitalization which are considered acute exacerbations per patient per year are 0.866±0.01. On total 30.7% (131 patients) has 3 and more exacerbations per year and 72.4% of them have 3 or 4 exacerbations per year. These are the patients with greatest mortality risk.
The average admission rate in hospital for COPD is about 200 per 100,000 people per year (36). The admission rate for North Macedonia, Romania, and Turkey is more than 200 per 100,000 patients (36). In our country this admission rate is unknown but 9.7% of hospitalized patients in the country suffered from COPD which means that about 22,000 patients were hospitalized in 2015 (21). Hospitalization rates range from as low as 2.61 to12.79 per patient per year while mean stay in hospital is 6.52 days.
The study confirms that severity of the COPD leads to increased number of exacerbations and hospital-stay. Patients with mild level of COPD have 0.86 exacerbations and 2.61 days in hospital per year, while for very severe COPD patients these values increase almost 4 times. Krachunov et al. reported that the frequency of acute exacerbations of COPD correlated with: NO, SO2 and PM10 (19). The numbers of hospital stay after exacerbations are in the range of 0.4–1.67 per patients per year which increase with pollution with PM10. It has been found that patients with GOLD stage D have five-fold higher hospitalization than hospitalizations of patients with GOLD stage A and nearly three-fold higher admission to hospital compared to stage B patients.
Limitations
The study has some limitations. The pollution with PM2.5, carbon monoxide CO and NO was not considered because the reports of EEA for these pollutants did not include information from some chosen towns. The mortality rate after admission to hospital with acute exacerbations of COPD was not included in this study. It worth to be estimated how the mortality risk increases with the frequency of severe acute exacerbations.
We intend to assess the progress of COPD and present the trend of the severity of the illness in a period of four years. Thus we will see an impact of changing PM10 exposure on respiratory health. The presented results describe only the state of the art at the beginning of investigation. The second part of our research will include the trend of severity of illness assessing the decline of FEV1 per increment of 10 µg/m3 PM10.
Conclusions
Our study is the first Bulgarian one, which presents results by extracting data from representative sample of COPD-patients observed for a period of one year. The relationship between air pollution, number of hospitalizations and different stages of COPD were investigated for the selected towns over entire country area. The main strength of the study is the assessments of air pollution status of the chosen towns and its association with the severity of COPD in Bulgaria. The study confirms that with the increase of COPD severity and the degree of pollution the numbers of exacerbations and hospital stay increase.
Acknowledgments
Funding: This study was financed by the National Science Fund in Bulgaria (Contract DFNI B-02/12 from December 12, 2014).
Ethical Statement: The Bulgarian National Science Fund approved the study (No. B02-12/12.12.2014). Every patient was acquainted with the study design and purposes and provided informed consent.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.WHO air quality guidelines: past, present and future. Copenhagen: WHO Regional Office for Europe; 2017. [Google Scholar]
- 2.Krzyzanowski M, Apte J, Bonjour S, et al. Air pollution in the mega-cities. Curr Envir Health Report 2014;1:185-91. 10.1007/s40572-014-0019-7 [DOI] [Google Scholar]
- 3.WHO factsheets. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/
- 4.Abe KC, Miraglia SG. Health impact assessment of air pollution in São Paulo, Brazil. Int J Environ Res Public Health 2016;13. doi: . 10.3390/ijerph13070694 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.WHO report 2012. Available online: https://www.who.int/gho/phe/outdoor_air_pollution/en/
- 6.Tamayo-Uria I, Altzibar JM, Mughini-Gras L, et al. Exacerbations of chronic obstructive pulmonary disease (COPD): An ecological study in the basque country, Spain (2000-2011). COPD 2016;13:726-33. 10.1080/15412555.2016.1182145 [DOI] [PubMed] [Google Scholar]
- 7.Chen R, Huang W, Wong C, et al. Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: The China air pollution and health effects study (CAPES). Environmental Research 2012;118:101-6. 10.1016/j.envres.2012.07.003 [DOI] [PubMed] [Google Scholar]
- 8.Heinrich J, Schikowski T. COPD patients as vulnerable subpopulation for exposure to ambient air pollution. Curr Environ Health Rep 2018;5:70-6. 10.1007/s40572-018-0178-z [DOI] [PubMed] [Google Scholar]
- 9.DeVries R, Kriebel D, Sama S. Low level air pollution and exacerbation of existing COPD: a case crossover analysis. Environ Health 2016;15:98-107. 10.1186/s12940-016-0179-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Roca M, Verduri A, Corbetta L, et al. Mechanisms of acute exacerbation of respiratory symptoms in chronic obstructive pulmonary disease. Eur J Clin Invest 2013;43:510-21. 10.1111/eci.12064 [DOI] [PubMed] [Google Scholar]
- 11.Wedzicha J. Mechanisms of chronic obstructive pulmonary disease exacerbations. Ann Am Thorac Soc 2015;12 Suppl 2:S157-9. 10.1513/AnnalsATS.201507-427AW [DOI] [PubMed] [Google Scholar]
- 12.Li XY, Gilmour PS, Donaldson K, et al. Free radical activity and pro-inflammatory effects of particulate air pollution (PM10) in vivo and in vitro. Thorax 1996;51:1216-22. 10.1136/thx.51.12.1216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ko FW, Hui DS. Outdoor air pollution: impact on chronic obstructive pulmonary disease patients. Curr Opin Pulm Med 2009;15:150-7. 10.1097/MCP.0b013e32832185ee [DOI] [PubMed] [Google Scholar]
- 14.Garshick E. Effects of short- and long-term exposures to ambient air pollution on COPD. Eur Respir J 2014;44:558-61. 10.1183/09031936.00108814 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Seemungal TA, Hurst JR, Wedzicha JA. Exacerbation rate, health status and mortality in COPD - a review of potential interventions. Int J Chron Obstruct Pulmon Dis 2009;4:203-23. 10.2147/COPD.S3385 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Annesi-Maesano I. Air Pollution and Chronic Obstructive Pulmonary Disease Exacerbations: When Prevention Becomes Feasible. Am J Respir Crit Care Med 2019;199:547-8. 10.1164/rccm.201810-1829ED [DOI] [PubMed] [Google Scholar]
- 17.WHO for PM Available online: http://www.euro.who.int/__data/assets/pdf_file/0006/189051/Health-effects-of-particulate-matter-final-Eng.pdf
- 18.Report for health in BG (in Bulgarian). Available online: www.ncphp.government.bg/files/doklad_zdrave-17-10.pdf
- 19.Krachunov I, Ivanov Y. Particulate matter and respiratory health. Thorac Med 2014;6:8-17. [Google Scholar]
- 20.Tachkov K, Kamusheva M, Pencheva V, et al. Evaluation of the economic and social burden of chronic obstructive pulmonary disease (COPD). Biotechnol Biotec Eq 2017;31:855-61. [Google Scholar]
- 21.Penyovska P, Kyuchukova S, Dimova A. Hospital care in Bulgaria – trends in expenditure and activity. Health Economics and Management (in Bulgarian) 2018;67:3-10. 10.14748/hem.v67i1.5023 [DOI] [Google Scholar]
- 22.Pavlov P, Ivanov Y, Glogovska P, et al. COPD morbidity among smokers – an epidemiological study. Thorac Med 2011;3:50-3. [Google Scholar]
- 23.Pavlov P, Ivanov Y, Glogovska P, et al. New epidemiological data about COPD in Pleven region. Thorac Med 2012;2:44-50. [Google Scholar]
- 24.Tachkov K, Dimitrova M, Mitov K, et al. Pharmaco-economic studies of pharmacotherapy of COPD. Social Medicine 2017;2-3:20-8. [Google Scholar]
- 25.Ivanov Y, Nikolaev I, Nemeth I. Real-life evaluation of COPD treatment in a Bulgarian population: a 1-year prospective, observational, noninterventional study. Int J Chron Obstruct Pulmon Dis 2018;13:653-63. 10.2147/COPD.S153969 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Available online: www.nhif.bg
- 27.Kamusheva M, Dimitrova M, van Boven J, et al. Clinical characteristics, treatment patterns and socio-economic burden of COPD in Bulgaria. J Med Econ 2017;20:503-9. 10.1080/13696998.2017.1279620 [DOI] [PubMed] [Google Scholar]
- 28.GOLD 2016. Available online: http://goldcopd.org/
- 29.Reports of EEA (2016). Available online: http://eea.government.bg/airq/bulletin.jsp
- 30.Limit concentration regulation Nº 12/2010 г. of the Ministry of Environment and Waters. Available online: http://eea.government.bg/bg/legislation/air/Naredba_12_Normi_KAV.pdf
- 31.Choi J, Oh JY, Lee YS, et al. Harmful impact of air pollution on severe acute exacerbation of chronic obstructive pulmonary disease: particulate matter is hazardous. Int J Chron Obstruct Pulmon Dis 2018;13:1053-9. 10.2147/COPD.S156617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Haider M, Shafqat M, Zafar M. Impact of air pollution on severe acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis 2018;13:2101-3. 10.2147/COPD.S170691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Albert RK, Connett J, Bailey WC, et al. Azithromycin for Prevention of Exacerbations of COPD. N Engl J Med 2011;365:689-98. 10.1056/NEJMoa1104623 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Connolly MJ, Lowe D, Anstey K, et al. Admissions to hospital with exacerbations of chronic obstructive pulmonary disease: effect of age related factors and service organization. Thorax 2006;61:843-8. 10.1136/thx.2005.054924 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925-31. 10.1136/thx.2005.040527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.European Lung white book, Available online: https://www.erswhitebook.org/chapters/chronic-obstructive-pulmonary-disease/