

Abstract
Objective:
To compare respiratory-triggered DIfferential Subsampling with Cartesian Ordering (rtDISCO) and breath held Liver Acquisition with Volume Acquisition (LAVA) image quality.
Methods:
In this IRB-approved, HIPAA-compliant prospective study, 25 subjects underwent T1 imaging with rtDISCO and LAVA prior to and following intravenous contrast. Three readers scored individual series and side-by-side comparisons for motion and noise. Eight clinical tasks were qualitatively assessed.
Results:
As individual series, readers rated rtDISCO images as more degraded by motion on both pre- (mean rtDISCO score=2.7, LAVA=1.6; p<0.001) and post-contrast images (rtDISCO=2.4, LAVA=1.8; p<0.001). Readers preferred LAVA images based on motion on both pre- (mean preference=−1.2; p<0.001) and post-contrast images (mean preference=−0.7; p<0.001) on side-by-side assessment. There was no preference between sequences for 6/8 clinical tasks on post-contrast images.
Conclusions:
Readers preferred LAVA with respect to motion but not noise; there was no preference in the majority of tested clinical tasks.
Keywords: Motion, Noise, LAVA, DISCO, magnetic resonance imaging
Introduction
Dynamic contrast enhanced imaging, consisting of pre- and post-contrast T1-weighted imaging in multiple contrast phases, is used to detect and characterize a variety of abnormalities in the abdomen.1–4 Three-dimensional (3D) spoiled gradient recalled echo (SPGR) with fat suppression (LAVA; General Electric, Milwaukee, WI, USA), has a typical temporal resolution of 15–20 seconds and is performed within a single breath hold.5,6 The Cartesian acquisition and regular sampling for k-space filling in this sequence makes it susceptible to respiratory motion and ghosting artifacts.7–9 In patients with limited breath holding capacity, a respiratory triggered data acquisition, in which data acquisition is timed to the patient’s breathing cycle, has been shown to decrease motion artifacts, but scan duration may suffer, as images are only acquired during an acceptable respiratory window.10,11 In addition, irregular patient breathing or mis-timing of the acquisitions can result in greater ghosting artifacts.
DIfferential Sub-sampling with Cartesian Ordering (DISCO) offers high spatial and temporal resolution dynamic contrast enhanced imaging by combining a dual-echo spoiled gradient recalled echo in steady state (SPGR) sequence with a k-space undersampling technique.5 K-space is sampled elliptically, with the central k-space segment sampled with each ellipse while outer k-space segment is undersampled in a pseudo-random fashion.5 The temporal resolution of DISCO can be as short as 4–5 seconds. In patients with limited or no breath hold capacity, the temporal resolution of DISCO and motion artifact suppression offered by the undersampling could make a respiratory-triggered acquisition useful for contrast-enhanced imaging.
The purpose of this study was to compare respiratory-triggered DIfferential Subsampling with Cartesian Ordering (rtDISCO) and breath held Liver Acquisition with Volume Acquisition (LAVA) image quality with respect to motion and noise in abdominal MRI obtained in inpatients, who may have lower breath holding capacity than outpatients.
Materials and Methods
This was an institutional review board-approved, Health Insurance Portability and Accountability Act compliant prospective study. Written informed consent was obtained from all subjects.
Subjects
Twenty-five subjects undergoing clinical liver MRI as an inpatient at our institution (12 males, 13 females; mean age 58 years ± 13 years) were prospectively enrolled. Indications for imaging included chronic liver disease (n=12), pain/biliary obstruction (n=10), and oncologic workup (n=3).
MRI
Imaging was performed on a 1.5T MRI system (MR450W, General Electric, Milwaukee, Wisconsin) with the subjects supine, using an 18-channel phased-array body coil centered over the upper abdomen combined with the table-mounted spine matrix. Axial T1-weighted (T1w) imaging of the abdomen was performed with rtDISCO (free breathing with respiratory triggering) and LAVA (breath held) prior to and following the intravenous administration of gadobenate dimeglumine (Bracco Diagnostics, Princeton, NJ) at 2 mL/sec in the equilibrium phase. Coronal imaging in the equilibrium phase was also performed with both rtDISCO and LAVA sequences. Pulse sequence parameters for rtDISCO axial images included: TR=5.3 ms; TE=2.4 ms; flip angle=12°; pixel bandwidth=326 Hz/pixel; image matrix of 256 × 192 with 68 slices; and acquisition time=21 s. Pulse sequence parameters for LAVA axial images included: TR=6.0 ms; TE=3.1 ms; flip angle=12°; pixel bandwidth=326 Hz/pixel; image matrix of 256 × 192 with 68 slices; and acquisition time=17.3 s. For the rtDISCO sequence, patients were instructed to breath quietly and calmly.
Individual Series Analysis
The axial and coronal rtDISCO and LAVA images were de-identified and randomized. Three abdominal radiologists, with 1–6 years of post-fellowship experience, independently reviewed the rtDISCO and LAVA images as individual series, blinded to acquisition scheme for each image set. Readers recorded their assessment of image quality in terms of both image motion and image noise from 1 (no degradation) to 5 (highly degraded). Readers then qualitatively assessed each image set for focal liver, adrenal and renal lesions, portal vein patency, gallbladder and pancreatic margins, and common duct and peritoneal thickening. For each assessment, a confidence level from 1 (no confidence) to 5 (high confidence) was recorded.
Side-by-Side Analysis
The axial and coronal rtDISCO and LAVA images were then de-identified and randomized pairwise, such that the images were presented to reviewers as a pair, but in random order. Three abdominal radiologists independently reviewed the rtDISCO and LAVA images side-by-side, blinded to the acquisition scheme for each image set. Readers recorded their preference between images in terms of both motion and image noise. Readers then recorded their preference between images for presence of focal liver, adrenal and renal lesions, portal vein patency, gallbladder and pancreatic margins, and common duct and peritoneal thickening. After recording these preferences for all image pairs, results were de-randomized to yield a scale of: −2 – strongly prefer LAVA; −1 – somewhat prefer LAVA; 0 – no preference; +1 – somewhat prefer rtDISCO; +2 – strongly prefer rtDISCO.
Statistical Analysis
All statistical analyses were performed using R software (version 3.4.3 [2017]). Inter-reader agreement for continuous variables was assessed using the intra-class correlation coefficient (ICC), and inter-reader agreement for discrete variables was assessed using Fleiss’ kappa. Based on the ICC or kappa value, agreement was interpreted as poor (0.01–0.2), fair (0.21–0.4), moderate (0.41–0.6), good (0.61–0.8), or very good (0.81–0.1). For individual series assessments and side-by-side assessments, mixed-effects linear models were used to assess reader confidence scores and reader preference scores. rtDISCO versus LAVA and series were treated as fixed effects, and reader and patient were treated as random effects. Multiple testing corrections were performed using Tukey’s honest significance difference test. P-values less than 0.05 were considered statistically significant.
Results
Individual Series Analysis
Overall, among three readers, inter-reader agreement for motion was good (ICC: 0.73, 95% Confidence Interval [CI]: 0.66–0.79. Agreement for noise was fair (ICC: 0.35, 95% CI: 0.25–0.45). For each of the clinical tasks, agreement was moderate to good (ICC: 0.53–0.68).
For the axial unenhanced assessment, readers rated rtDISCO images as more degraded by motion (mean rtDISCO=2.7, mean LAVA=1.6; p<0.001). There was no preference between series with respect to image noise (mean rtDISCO score=2.2, LAVA=2.3; p=0.57). There was a preference for LAVA for 7/8 clinical tasks on the unenhanced images. For focal liver lesions, the mean confidence score for rtDISCO was 3.6, compared to 4.1 for LAVA (p<0.001). Similar results were seen for gallbladder margin (rtDISCO=3.7, LAVA=4.1; p<0.05), common duct thickness (rtDISCO=2.7, LAVA=3.1; p<0.05), pancreatic margin (rtDISCO=3.6, LAVA=4.3 p<0.001), adrenal glands (rtDISCO=4.0, LAVA=4.6; p<0.001), renal lesions (rtDISCO=3.9, LAVA=4.5; p<0.001) and peritoneal thickening (rtDISCO=3.5, LAVA=4.1; p<0.001). For assessment of the portal vein, there was no difference between series (rtDISCO=2.8, LAVA=3.0; p=0.13).
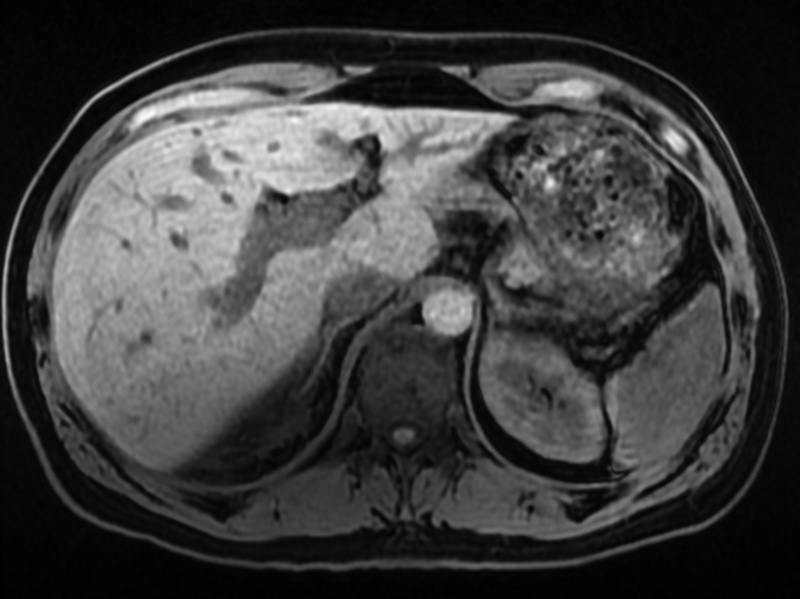
On the axial equilibrium phase assessment, readers rated rtDISCO images as more degraded by motion (mean rtDISCO score=2.4, LAVA=1.8; p<0.001) (Table 1). There was no preference with respect to image noise (mean rtDISCO score=1.8, LAVA=1.7; p=0.82), and no preference was found between series with respect to the clinical tasks (Table 1) (Fig. 1).
Table 1.
Individual series analysis for axial equilibrium phase datasets.
| Motion | Noise | Liver Lesions | Portal Vein | Gall-bladder | Common Duct | Pancreas | Adrenal | Renal | Perito-neum | |
|---|---|---|---|---|---|---|---|---|---|---|
| Reader 1 | ||||||||||
| rtDISCO | 2.5 | 1.8 | 4.3 | 4.1 | 4.2 | 3.6 | 3.9 | 3.7 | 4.6 | 4.3 |
| LAVA | 1.7 | 1.7 | 4.4 | 4.6 | 4.6 | 4.2 | 4.4 | 4.3 | 4.6 | 4.6 |
| Reader 2 | ||||||||||
| rtDISCO | 2.3 | 1.5 | 4.2 | 4.2 | 4.5 | 3.8 | 4.2 | 4.5 | 4.9 | 4.5 |
| LAVA | 1.8 | 1.4 | 4.5 | 4.3 | 4.6 | 4.0 | 4.4 | 4.6 | 4.8 | 4.4 |
| Reader 3 | ||||||||||
| rtDISCO | 2.3 | 2.2 | 4.2 | 3.9 | 4.3 | 3.3 | 4.0 | 4.0 | 4.8 | 4.6 |
| LAVA | 1.9 | 2.1 | 4.6 | 4.2 | 4.3 | 3.5 | 3.9 | 4.1 | 4.6 | 4.4 |
| Mean | ||||||||||
| rtDISCO | 2.4 | 1.8 | 4.2 | 4.1 | 4.3 | 3.6 | 4.0 | 4.1 | 4.7 | 4.4 |
| LAVA | 1.8 | 1.7 | 4.5 | 4.4 | 4.5 | 3.9 | 4.2 | 4.3 | 4.6 | 4.5 |
| p-Value | <0.001 | 0.82 | 0.13 | 0.08 | 0.53 | 0.13 | 0.35 | 0.08 | 0.94 | 0.94 |
Note: For image motion and image noise, ratings ranged from 1 (no degradation) to 5 (highly degraded). For each clinical task, readers rated confidence from 1 (no confidence) to 5 (high confidence).
Fig. 1.


38-year-old female with metastatic colon adenocarcinoma. (A) Axial T1w (LAVA) in the equilibrium phase. In the individual series review, all three readers rated the image has having minimal motion; two of the readers rated the image has having no significant noise, while one reader rated the image as having minimal noise. (B) Axial T1w (rtDISCO) in the equilibrium phase. In the individual series review, one reader rated the image as having moderate motion and minimal noise, while the other two readers rated the image as having minimal motion and no noise.
On the coronal equilibrium phase assessment, there was no preference between the rtDISCO and LAVA images with respect to image motion (rtDISCO=1.7, LAVA=1.9; p=0.21), image noise (rtDISCO=2.3, LAVA=2.2; p=0.57), or any of the clinical tasks (p>0.35).
Side-by-Side Analysis
Overall, among three readers, inter-reader agreement for motion was good (ICC: 0.71, 95% CI: 0.60–0.79. Agreement for noise was fair (ICC: 0.29, 95% CI: 0.14–0.44). For each of the clinical tasks, agreement was moderate to very good (ICC: 0.48–0.90).
For side-by-side assessments, readers preferred LAVA images based on motion on both pre- (mean preference=−1.2; p<0.001) and post-contrast axial images (mean preference=−0.7; p<0.001). On the coronal post-contrast images, slight preference for rtDISCO with respect to motion was not statistically significant (mean preference=0.4; p=0.08) (Table 2).
Table 2.
Side-by-side reader preferences for motion and noise on axial pre- and post-contrast datasets and for clinical tasks on axial equilibrium phase images.
| Reader 1 | Reader 2 | Reader 3 | Mean | p-value | |
|---|---|---|---|---|---|
| Motion – Pre-Contrast | −1.4 | −1 | −1.3 | −1.2 | <0.001 |
| Motion – Post-Contrast | −0.8 | −0.5 | −0.7 | −0.7 | <0.001 |
| Noise – Pre-Contrast | −1.1 | .1 | −0.3 | −0.4 | 0.15 |
| Noise – Post-Contrast | −1.1 | 0.0 | −0.7 | −0.6 | 0.04 |
| Focal Liver Lesions | −1.1 | −0.4 | −0.8 | −0.8 | 0.003 |
| Portal Vein | −0.8 | −0.4 | −0.7 | −0.6 | 0.01 |
| Gallbladder | −0.1 | 0.4 | 0.3 | 0.2 | 0.67 |
| Common duct | −0.8 | −0.1 | −0.3 | −0.4 | 0.12 |
| Pancreatic margin | −0.7 | −0.1 | 0.0 | −0.3 | 0.39 |
| Adrenal glands | −0.6 | 0.0 | 0.2 | −0.2 | 0.68 |
| Renal lesions | −0.7 | 0.1 | 0.0 | −0.2 | 0.58 |
| Peritoneal thickening | −0.9 | −0.1 | −0.5 | −0.5 | 0.08 |
Note: After recording preferences for all image pairs, results were de-randomized to yield a scale of: −2 – strongly prefer LAVA; −1 – somewhat prefer LAVA; 0 – no preference; +1 – somewhat prefer rtDISCO; +2 – strongly prefer rtDISCO.
On pre-contrast axial images, there was no significant preference with respect to image noise (mean preference=−0.4; p=0.15). On post-contrast axial images, there was a slight preference for LAVA images based on image noise (mean preference=−0.6; p=0.04) (Table 2) (Fig. 2). On the coronal post-contrast images, there was no preference with respect to noise (mean preference=−0.2; p=0.71).
Fig. 2.
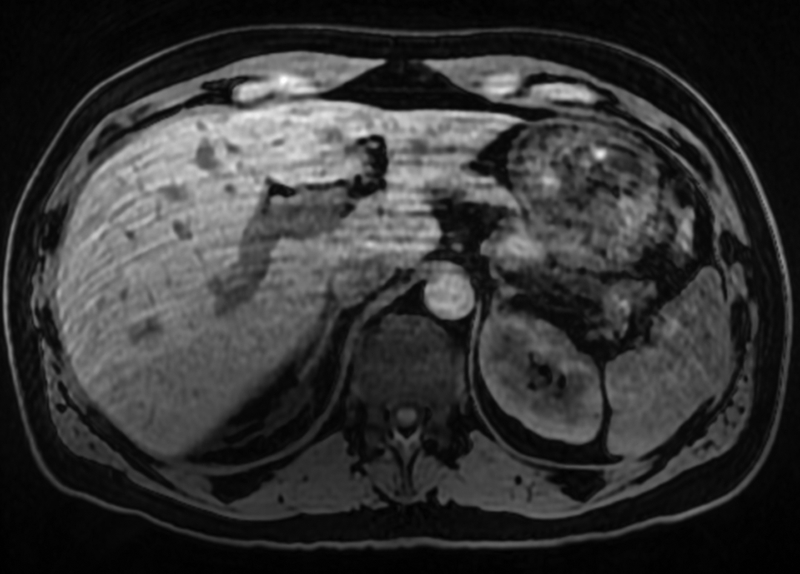
42-year-old male with abnormal liver function tests. (A) Axial T1w (LAVA) without IV contrast and (B) axial T1w (rtDISCO) without IV contrast. In the side-by-side analysis, all three readers strongly preferred the LAVA image (A) with respect to motion. Two readers mildly preferred the LAVA image (A) with respect to noise, while the third reader had no preference between the images for noise.
On pre-contrast axial images, there was a preference for the LAVA images for the detection of liver lesions (mean preference=−1.1; p<0.001), common duct (mean preference=−0.7; p=0.006), pancreatic margin (mean preference=−0.7; p=0.006), and renal lesions (mean preference=−0.7; p=0.01). There was no preference for gallbladder (mean preference=−0.3; p=0.45), adrenal gland (mean preference=−0.4; p=0.08), and peritoneal thickening (mean preference=−0.08; p=0.93). There was a preference for rtDISCO with respect to the portal vein (mean preference=0.8; p<0.001).
On axial equilibrium phase images, there was a preference for LAVA for assessment for focal liver lesions and portal vein patency. Mean score for focal liver lesion preference was −0.8 (p<0.005) and mean score for portal vein assessment was −0.6 (p<0.01). There was no significant preference between sequences for the other 6 clinical tasks on post-contrast images (Table 2).
On coronal equilibrium phase images, there was no preference with regard to motion (mean preference=0.4; p=0.08), noise (mean preference=−0.2; p=0.71), or any of the clinical tasks (mean preference between 0.1 and 0.4; p>0.2).
Discussion
In this study, multiple readers compared a respiratory-triggered DISCO acquisition and a breath hold LAVA acquisition of the upper abdomen prior to and following IV contrast administration in inpatients. Readers preferred the breath hold LAVA images compared to rtDISCO with respect to motion but not for noise, and there was no preference in the majority of tested clinical tasks. These findings suggest that applying respiratory triggering to this rapid image acquisition technique does not improve motion artifact over a breath hold acquisition; however, the difference in subjective motion assessment may not affect diagnostic confidence.
In our investigation, we found that on both individual series and side-by-side evaluation, readers preferred the breath hold LAVA images compared to rtDISCO with respect to motion. Previous authors have found similar findings when comparing navigated acquisition to breath-hold acquisitions. Young, et al., compared a respiratory triggered 3D SPGR T1w sequence to breath-hold and free breathing sequences and found that the image quality of the respiratory triggered acquisition was improved compared to the free breathing acquisition, but was inferior to the breath-hold acquisition.11 The authors concluded that the residual motion artifact may be due to the small range of motion in the acceptable window or inaccuracies in sensing the diaphragm. The authors also found a significant increase in scanning time, thereby limiting dynamic contrast enhanced imaging. Vasanawala et al. reported similar findings and suggested that motion artifact in the respiratory triggered acquisition resulted from accepting acquired data during 40% of the respiratory cycle; motion artifacts might have been reduced by narrowing the acceptance window to a smaller portion of the respiratory cycle.10 In a study of delayed phase, non-dynamic imaging, image quality was improved with navigated T1w images compared to breath hold T1w in the hepatobiliary phase.12
Chandarana et al. have evaluated methods of altering k-space sampling. A study comparing radial “stack-of-stars” k-space sampling with conventional T1w imaging found no difference between radial free breathing T1w and breath hold T1w with respect to overall image quality and respiratory motion artifact, but did find lower hepatic vessel clarity.8 In another study, Chandarana, et al., found that a radial acquisition with “stack-of-stars” had higher scores for image quality and respiratory motion artifact and more lesions were identified compared to a regular Cartesian acquisition in pediatric patients.13 In our study, readers preferred the breath hold Cartesian LAVA images compared to rtDISCO images with k-space subsampling with respect to motion; however, there was no preference between image sets in the majority of clinical tasks.
With the limited sampling of outer k-space segment, there is some concern that image noise could be adversely affected.5 In addition, since the DISCO sequence is often parameterized with higher spatial resolution than conventional LAVA, signal to noise ratio may be further affected.14 We matched spatial resolution and pixel bandwidth between sequences to account for the latter effect and found no difference in image noise between the rtDISCO or the LAVA acquisitions. In addition, there was no reader preference in the majority of the tested clinical tasks between the two sequences.
There are limitations to this investigation. While this was a prospective study of hospital inpatients, only a small number of patients were included and no clinical assessment of the patient’s breath hold ability was made. We chose inpatient status as a surrogate for reduced breath holding capacity, but the low mean motion scores suggest that even in this patient population, breath holding was not severely impaired. Pre-contrast and late dynamic phase imaging was acquired with both LAVA and rtDISCO for comparison, but arterial phase and portal venous phase imaging could not be performed with both sequences. Reader preferences for various clinical tasks and features were assessed, but a limited number of patients had focal lesions, and further investigation is needed to compare clinical tasks such as lesion detection and characterization between the two sequences.
In conclusion, readers preferred LAVA compared to rtDISCO with respect to motion but not noise, and there was no reader preference in the majority of tested clinical tasks in inpatients undergoing contrast-enhanced abdominal MRI.
Acknowlegements:
Research reported in this publication was supported by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002553. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Grant Support: National Center For Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR002553.
An institutional research grant from General Electric Healthcare supported this research.
References
- 1.Hussain SM, Reinhold C, Mitchell DG. Cirrhosis and lesion characterization at MR imaging. Radiographics 2009;29:1637–52. [DOI] [PubMed] [Google Scholar]
- 2.Chavhan GB, Babyn PS, Vasanawala SS. Abdominal MR imaging in children: motion compensation, sequence optimization, and protocol organization. Radiographics 2013;33:703–19. [DOI] [PubMed] [Google Scholar]
- 3.Chavhan GB, Shelmerdine S, Jhaveri K, Babyn PS. Liver MR Imaging in Children: Current Concepts and Technique. Radiographics 2016;36:1517–32. [DOI] [PubMed] [Google Scholar]
- 4.Semelka RC, Martin DR, Balci C, Lance T. Focal liver lesions: comparison of dual-phase CT and multisequence multiplanar MR imaging including dynamic gadolinium enhancement. J Magn Reson Imaging 2001;13:397–401. [DOI] [PubMed] [Google Scholar]
- 5.Saranathan M, Rettmann DW, Hargreaves BA, Clarke SE, Vasanawala SS. DIfferential Subsampling with Cartesian Ordering (DISCO): a high spatio-temporal resolution Dixon imaging sequence for multiphasic contrast enhanced abdominal imaging. J Magn Reson Imaging 2012;35:1484–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Li XH, Zhu J, Zhang XM, et al. Abdominal MRI at 3.0 T: LAVA-Flex compared with conventional fat suppression T1-weighted images. J Magn Reson Imaging 2014;40:58–66. [DOI] [PubMed] [Google Scholar]
- 7.Zaitsev M, Maclaren J, Herbst M. Motion artifacts in MRI: A complex problem with many partial solutions. J Magn Reson Imaging 2015;42:887–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chandarana H, Block TK, Rosenkrantz AB, et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol 2011;46:648–53. [DOI] [PubMed] [Google Scholar]
- 9.Morelli JN, Runge VM, Ai F, et al. An image-based approach to understanding the physics of MR artifacts. Radiographics 2011;31:849–66. [DOI] [PubMed] [Google Scholar]
- 10.Vasanawala SS, Iwadate Y, Church DG, Herfkens RJ, Brau AC. Navigated abdominal T1-W MRI permits free-breathing image acquisition with less motion artifact. Pediatric radiology 2010;40:340–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Young PM, Brau AC, Iwadate Y, et al. Respiratory navigated free breathing 3D spoiled gradient-recalled echo sequence for contrast-enhanced examination of the liver: diagnostic utility and comparison with free breathing and breath-hold conventional examinations. AJR Am J Roentgenol 2010;195:687–91. [DOI] [PubMed] [Google Scholar]
- 12.Yoon JH, Lee JM, Lee ES, et al. Navigated three-dimensional T1-weighted gradient-echo sequence for gadoxetic acid liver magnetic resonance imaging in patients with limited breath-holding capacity. Abdom Imaging 2015;40:278–88. [DOI] [PubMed] [Google Scholar]
- 13.Chandarana H, Block KT, Winfeld MJ, et al. Free-breathing contrast-enhanced T1-weighted gradient-echo imaging with radial k-space sampling for paediatric abdominopelvic MRI. Eur Radiol 2014;24:320–6. [DOI] [PubMed] [Google Scholar]
- 14.Inoue Y, Hata H, Nakajima A, Iwadate Y, Ogasawara G, Matsunaga K. Optimal techniques for magnetic resonance imaging of the liver using a respiratory navigator-gated three-dimensional spoiled gradient-recalled echo sequence. Magn Reson Imaging 2014;32:975–80. [DOI] [PubMed] [Google Scholar]