

Abstract
The facelift has significantly evolved over the past several decades. What was once considered a skin only operation is now a sophisticated, elegant procedure that requires meticulous preoperative analysis, understanding of underlying anatomically based aging changes, and extreme attention to detail. According to the American Society of Plastic Surgeons, 125,697 facelifts were performed in 2017. It is not surprising that given these advances that facial rejuvenation surgery is still a very common procedure with a high degree of patient satisfaction despite the increase in nonsurgical facial aging treatments. With an improved understanding of facial anatomy including the facial retaining ligaments and intervening superficial and deep fat compartments, the modern facelift requires an anatomically targeted approach. Furthermore, the modern facelift surgeon must achieve consistently excellent results with reasonably little downtime while being aware of methods to improve the safety of this popular elective procedure. Hematoma is the most common complication after rhytidectomy with an incidence between 0.9% and 9%, with a higher incidence in males. Other potential complications include seroma, nerve injury, skin flap necrosis, siaolocele as a consequence of submandibular gland debulking, and skin flap rhytid and hairline distortion. This review aims to discuss safe, consistent, and reproducible methods to achieve success with facelift.
BACKGROUND
The facelift has significantly evolved over the past several decades. What was once considered a skin only operation is now a sophisticated, elegant procedure that requires meticulous preoperative analysis, understanding of underlying anatomically based aging changes, and extreme attention to detail. According to the American Society of Plastic Surgeons, 125,697 facelifts were performed in 2017.1 It is not surprising that given these advances that facial rejuvenation surgery is still a very common procedure with a high degree of patient satisfaction2 despite the increase in nonsurgical facial aging treatments.1
With an improved understanding of facial anatomy including the facial retaining ligaments and intervening superficial and deep fat compartments,3–5 the modern facelift requires an anatomically targeted approach. Furthermore, the modern facelift surgeon must achieve consistently excellent results with reasonably little downtime while being aware of methods to improve the safety of this popular elective procedure. Hematoma is the most common complication after rhytidectomy with an incidence between 0.9% and 9%, with a higher incidence in males.6–12 Other potential complications include seroma, nerve injury, skin flap necrosis, siaolocele as a consequence of submandibular gland debulking, and skin flap rhytid and hairline distortion. This review aims to discuss safe, consistent, and reproducible methods to achieve success with facelift.
ANATOMY
The superficial musculoaponeurotic system (SMAS) is the investing fascia of the facial mimetic muscles and is continuous with the platysma inferiorly and galea superiorly.13–15 Laterally, the SMAS is firmly adherent to the parotid–masseteric fascia where it is known as the immobile SMAS. The facial retaining ligaments transmit through the SMAS to the overlying skin, either originating from the periosteum (zygomatic and mandibular retaining ligaments) or from underlying muscle fascia (masseteric and cervical retaining ligaments).5,14 These retaining ligaments also serve as barriers between the superficial and deep facial fat compartments with neurovascular structures, or “facial danger zones,” located between these retaining ligaments.3,4,16–18
AGING CHANGES
Facial aging changes occur due to a combination of soft tissue deflation, decent, and ligamentous laxity, resulting in predictable aging patterns and radial expansion of the face.19 Skeletal regression, particularly in the inferolateral orbital rim and alveolar ridges, contributes to loss of midfacial support and loss of overall facial height.20–22 Furthermore, the gradual loss of skin elasticity and dermal thinning contributes to rhytid formation and can be exacerbated by smoking and ultraviolet radiation exposure.23
Accordingly, modern facelift techniques should be tailored to address the underlying culprits of facial aging. Soft tissue decent and ligamentous laxity are corrected by SMAS repositioning and ligamentous release. The architecture of the facial fat compartments has been previously detailed (Fig. 1).3,4 Fat grafting directly treats facial fat compartment deflation.24,25 Therefore, the modern facelift should involve a “Lift-and-Fill” approach.25
Fig. 1.
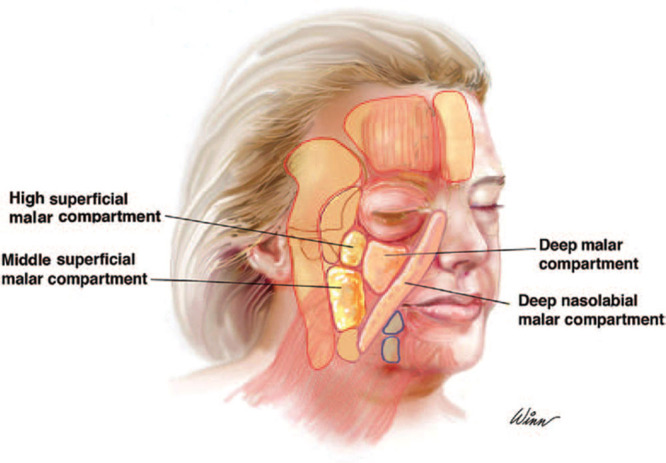
Facial fat compartments. Fat grafting of the labeled fat compartments is critical in the “lift-and-fill” face lift technique. Reprinted with permission from Plast Reconstr Surg. 2014;133:756e–767e)
FACIAL ANALYSIS AND PREOPERATIVE PLANNING
On examination, facial horizontal fifths and vertical thirds are analyzed to determine overall facial balance, making note of any asymmetries. The relationship between facial length, midfacial width, and overall fullness is critical as this guides the customized surgical intervention which, depending on asymmetries in the individual patient, may vary on each side (Fig. 2).26 The neck, décolletage, and skin elasticity and quality are evaluated. The patient is asked to provide photographs from youth to better assess areas of volume loss and changes that have occurred with time. Standardized facial photographs are obtained and essential for preoperative planning, patient counseling, and medicolegal purposes. It is important to note if the patient would benefit from ancillary procedures including brow lift, blepharoplasty, rhinoplasty, lip lift, genioplasty, and skin resurfacing procedures to improve facial aesthetic harmony.
Fig. 2.
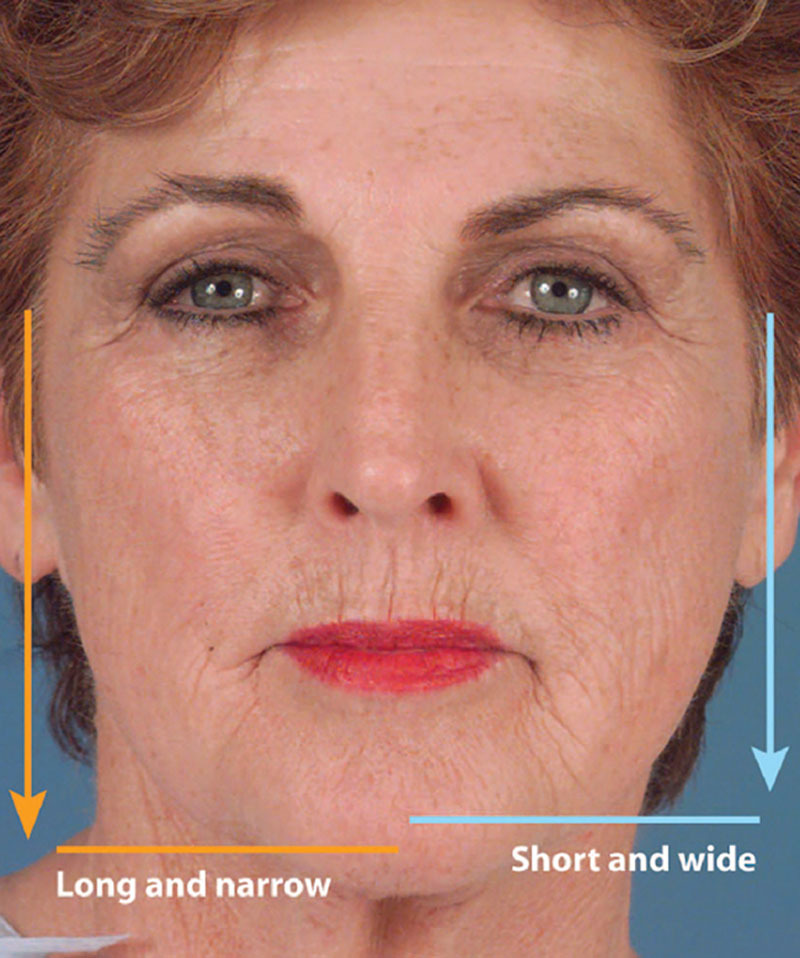
Preoperative analysis for the individualized component facelift. Anteroposterior view is used to determine midface width, height, and overall facial shape and soft-tissue distribution. Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
A thorough patient history and physical examination are performed. A full list of medications and supplements must be reviewed to ensure no consumption of blood thinners. Any patient over 50 requires an electrocardiogram (EKG) in addition to full laboratory testing which includes blood counts, coagulation profile, and even electrolytes as it has been shown certain medications can cause potentially serious electrolyte disturbances perioperatively.27 Particular attention is paid to a history of hypertension and nicotine product use. If present, hypertension must be medically optimized and necessary medical clearances are obtained before surgery. The patient must cease nicotine product use for a minimum of 3 months before surgery to decrease the risk of skin flap necrosis. In smokers, urine nicotine metabolites are tested 1 month before surgery to confirm abstinence. Furthermore, the history of nonsurgical treatments including neuromodulators, fillers, and energy-based devices is noted as the authors have observed increased scarring in these patients during dissection.
INCISION PLANNING
Temporal Incision
The distance between the lateral orbital rim and the anterior temporal hairline is assessed (Fig. 3). Skin redundancy and the anticipated amount of temporal skin excision is determined. If the estimated postoperative lateral orbital rim to anterior hairline distance is ≤5cm (ie minimal temporal skin resection), then the temporal portion of the incision can be concealed behind the hairline. If the anticipated distance is >5cm, then a prehairline incision is chosen to prevent postsurgical sideburn distortion.28,29
Fig. 3.
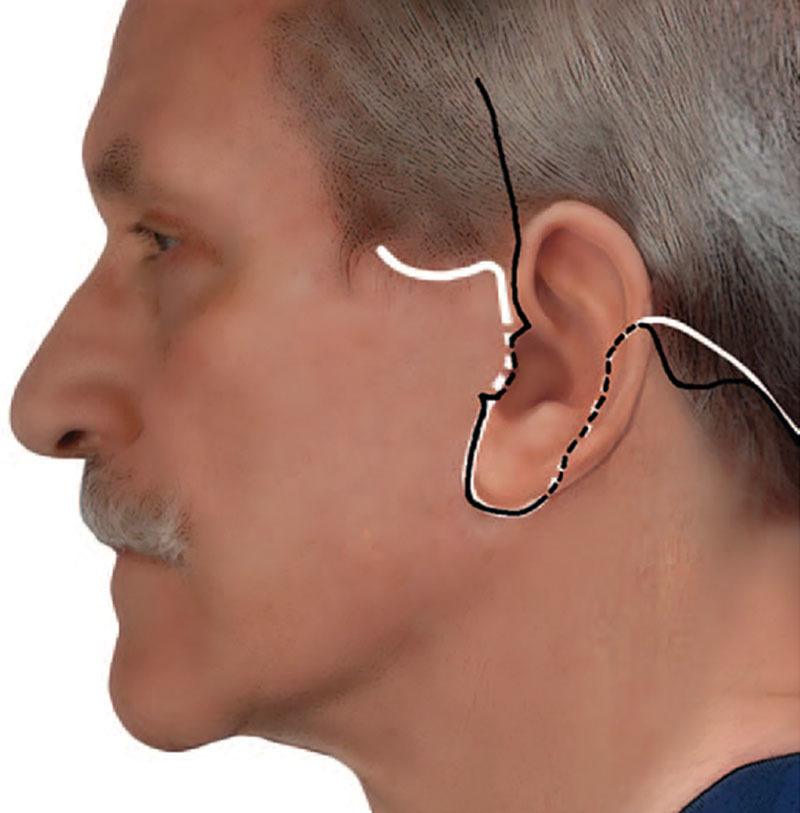
The rhytidectomy incision. White line, incision used by R.J.R.; black line, incision used by J.M.S.. Reprinted with permission from Plast Reconstr Surg. 2017;139:295–307.
Preauricular Incision
The incision follows the ear–cheek junction curvature, except for the tragus, where a choice is made between a pre or intertragal incision. A pretragal incision may be appropriate if there is a prominent preauricular crease, a tall vertical tragus, or prominent lateral cheek hair follicles. Otherwise, the majority of patients are best served by an intertragal incision to prevent postsurgical skin color and texture mismatch of the tragus and lateral cheek. Along the ear lobule, the incision is made 1 mm caudal to the cheek–lobule junction to prevent distortion of the interface between these anatomic units.
Retroarticular Incision
The incision continues into the retroauricular sulcus and is carried cephalically up to the midear. The decision to either carry the incision posteriorly into the scalp or inferiorly along the occipital hairline at the junction of the thin and thick hair is based on the estimated skin resection.29 If >2 cm of retroauricular skin resection is anticipated, then the incision is made along the occipital hairline to prevent a step off in the occipital hairline.
Submental Incision
The decision to open the neck is determined preoperatively based on the presence of cervical skin laxity and is accessed via a 3–4 cm incision marked 1–2 cm posterior to the submental crease.30 Surgical maneuvers are tailored to the individual patient. Considerations include the amount and location of excess cervical adiposity, the presence of jowling, severity of dynamic and static platysmal banding, and the distance between the medial platysmal borders (< or >2 cm; Fig. 4).31 Other authors advocate a more aggressive lateral platysmaplasty while avoiding a submental incision.32,33 Because the success of a modern facelift is often judged by the quality of the neck contour correction, in the authors experience, there is a low threshold to open the neck as doing so allows the ability to tighten via midline platysmaplasty, sculpt subplatysmal contents, and reduce the incidence of recurrent platysmal bands.34
Fig. 4.
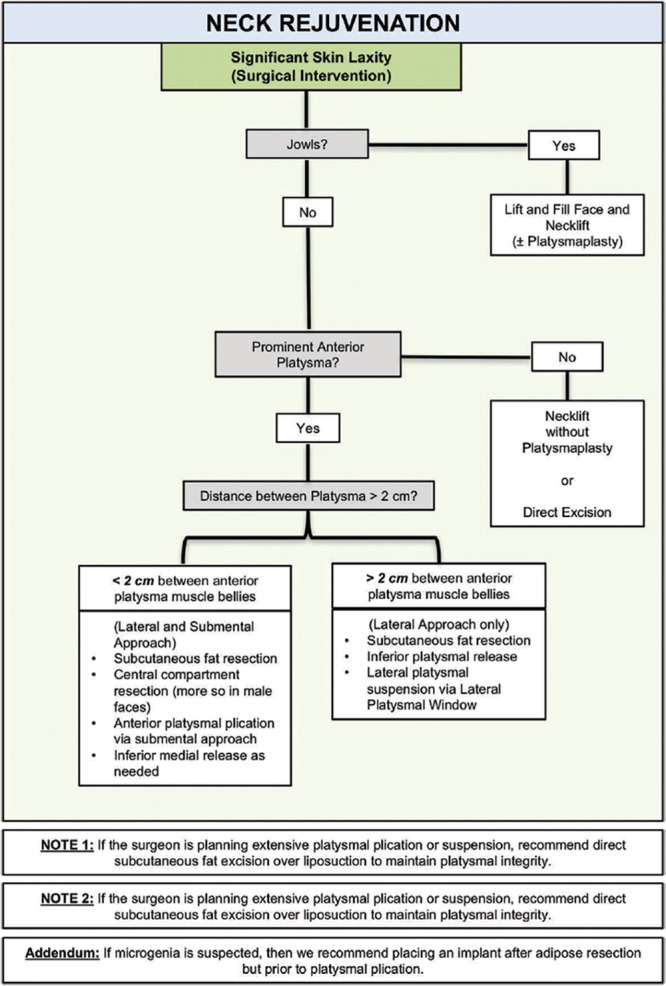
Neck rejuvenation algorithm for patients with moderate to severe skin laxity. Reprinted with permission from Plast Reconstr Surg. 2017;140:405e–414e.
ANESTHESIA AND PERIOPERATIVE MANAGEMENT
Hypertension is a controllable risk factor for hematoma;35,36 therefore, strict multimodal blood pressure control is essential to minimize complications (Fig. 5).37 Anxiety, pain, nausea, and vomiting are preemptively managed (Fig. 6). All patients receive 2 mg of midazolam in the preoperative holding area. Males and patients with a history of hypertension undergo placement of a 0.2-mg clonidine transdermal patch—in all other patients, a 0.1-mg clonidine patch is placed.
Fig. 5.
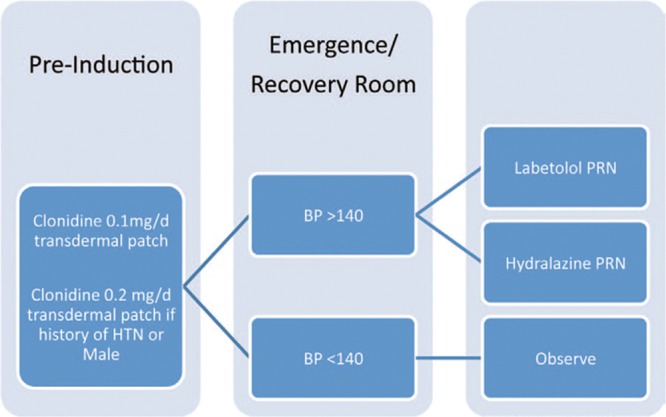
Hypertension management algorithm. HTN, hypertension; BP, blood pressure; PRN, as needed. Reprinted with permission from Plast Reconstr Surg. 2015;135:723–730.
Fig. 6.
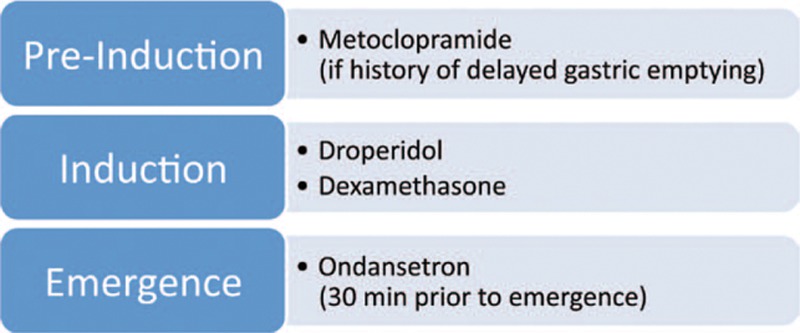
Nausea and vomiting prevention algorithm. Reprinted with permission from Plast Reconstr Surg. 2015;135:723–730.
General anesthesia is preferred. The endotracheal tube is placed midline and not secured, as it is monitored closely intraoperatively. Nitrous oxide is avoided due to an increased risk of postoperative nausea. Inhalational anesthetics are also avoided due to their propensity to cause vasodilation.37 Dexamethasone (8 mg IV) is given after induction for both edema and nausea management, and 4 mg of IV ondansetron is given 30 minutes before emergence. Sequential compression devices are placed, and an indwelling urinary catheter is inserted. The face is widely prepped with ophthalmic betadine and 2 g IV cefazolin is given 30 minutes before incision. As previously described by the senior author (R.J.R.), venous blood is drawn upon induction to extract platelet-rich plasma.6 The platelet-rich plasma is then drawn into a 10-cm3 dual-port sprayer syringe, with the second syringe containing an activating thrombin solution. Before skin closure, the activated platelet-rich/thrombin mixture is sprayed between the skin flap and underlying SMAS to help decrease ecchymosis and edema.6,38 The facelift incisions are then marked as previously described, based on preoperative assessment for optimal scar concealment and to minimize hairline distortion.
FILLING OF THE FACIA FAT COMPARTMENTS
Fat grafting is performed at the beginning of the procedure to ensure meticulous injection and to minimize fat graft contamination. For details regarding the senior author’s (R.J.R) technique, please refer to our prior article by Pezeshk et al.24 Nasolabial fold correction and restoration of youthful malar projection are by means of anatomically targeted fat grafting to the deep malar, deep nasolabial malar, and the high and middle superficial malar fat compartments (Fig. 1). Typically, 1–3 ml of fat are injected per compartment.25 Additionally, perioral, earlobe, temple fat grafting is performed if indicated.
INDIVIDUALIZED SKIN FLAP ELEVATION
A 22-guage spinal needle is used to inject 80–120 ml of infiltrate solution per side for the purpose of hemostasis and hydrodissection of the tissue planes. The infiltrate solution consists of 30 ml of 0.5% lidocaine and 1.5 ml of epinephrine (1:1,000) mixed with 300 ml of normal saline.6 The needle is inserted along the marked facelift incisions to prevent additional flap trauma, with the solution infiltrated in the subcutaneous plane. The endpoint for infiltration is moderate and uniform skin turgor of the facial tissues. Ten minutes are allowed to elapse after infiltration before incision for optimal hemostatic effect.
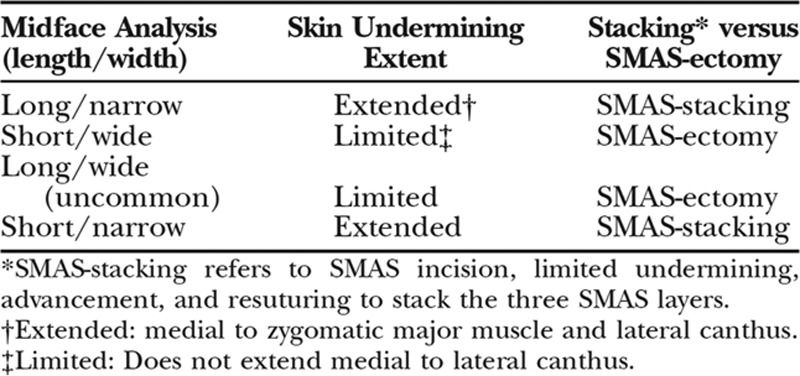
The marked facelift incisions are then completed with a 15 blade and the skin flaps are raised in the subcutaneous plane with facelift scissors. At least 3 mm of subcutaneous fat is left on the skin to maintain flap vascularity and to prevent contour irregularities. The extent of skin undermining is individualized to the shape and width of the patients face (Fig. 7)26,35,39 and is ultimately determined intraoperatively once the SMAS maneuvers have been completed to confirm skin redraping without puckering. Limited skin flap elevation is performed in faces with mild skin laxity and wide malar width. In contrast, long faces with narrow bimaxillary width, jowling, and redundancy medial to the lateral canthus require extended skin undermining for more complete release of the mandibular septum, zygomatic, and masseteric retaining ligaments for proper skin redraping and medial SMAS advancement (Fig. 8).26,39 Of note, medial perioral dissection is avoided as this results in postoperative deformities with facial animation due to dissociation of the skin with the underlying facial musculature.29,39
Fig. 7.

Individualized component facelift—undermining and SMASectomy vs SMAS-stacking. Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
Fig. 8.
Area of subcutaneous skin flap undermining indicated in red. Reprinted with permission from Plast Reconstr Surg. 2006;118:1251–1263.
OPEN TREATMENT OF THE NECK
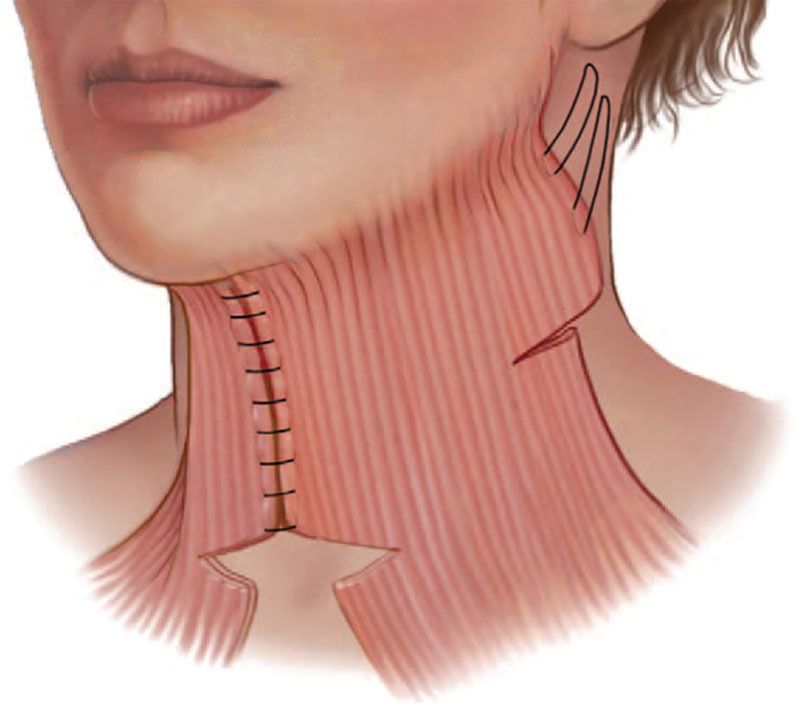
If the decision is made to open the neck, the submental incision is opened, and the facial/neck skin subcutaneous planes are connected. The senior author (R.J.R) has abandoned submental liposuction due to the high incidence of contour irregularities. In the appropriately selected patient, the authors perform preplatysmal and central subplatysmal fat resection under direct vision.30 On a technical note, preplatysmal fat is resected from lateral to medial as it is easy to inadvertently enter the subplatysmal plane with a medial approach. The medial platysma borders are plicated with figure-of-eight 4-0 Mersilene from the inferior mandibular border down to the level of the thyroid cartilage, followed by a 2-cm inferior transverse platysma myotomy (Fig. 9).34 Some authors advocate for more aggressive subplatysmal surgery including submandibular gland resection and digastric shaving28,40; however, a steep learning curve is required, and notable complications include marginal mandibular nerve palsy, salivary leak, and hematoma with potentially life-threatening airway compromise41; therefore, the senior author refrains from other subplatysmal procedures to minimize potential complications. In the scenario of prominent submandibular glands, 10 units of Botox (Allergan, Inc., Irvine, Calif.) are directly injected into the gland intraoperatively and then at 6–8 weeks postoperatively to promote submandibular gland atrophy.34
Fig. 9.
Inferomedial platysma is transected, platysmal midline stitches are placed, and a lateral platysmal window is performed. Reprinted with permission from Plast Reconstr Surg. 2006;118:1251–1263.
The sequence of SMAS/lateral platysmaplasty and medial platysmaplasty is debated by some authors. Of note, proponents of SMAS maneuvers before medial platysmaplasty believe that medial platysmaplasty “locks down” the SMAS and limits lateral SMAS correction.42 However, the authors prefer to complete the medial platysmaplasty first, as they have not noticed subsequent restriction in lateral SMAS correction.
LATERAL PLATYSMAL WINDOW AND SMAS MANEUVERS
A 2-cm lateral subplatysmal “window” is made approximately 1 finger breadth below the mandibular angle and 1 cm anterior to the SCM border to avoid the great auricular nerve.30,43 The lateral platysma flap is secured to the mastoid fascia with 2 figure-of-eight spanning 3-0 Mersilene sutures (Ethicon, Inc., Somerville, N.J.).
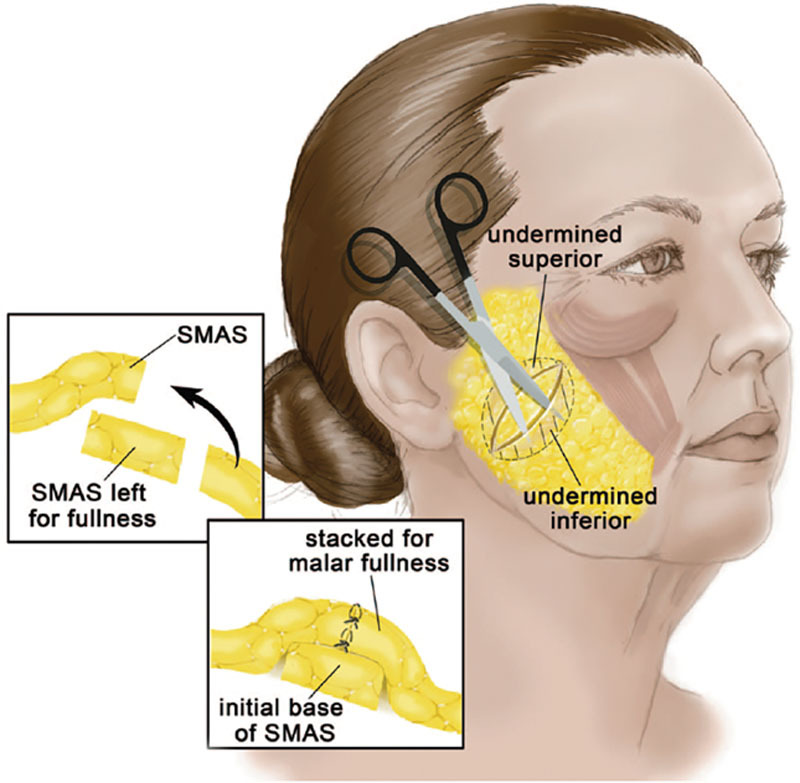
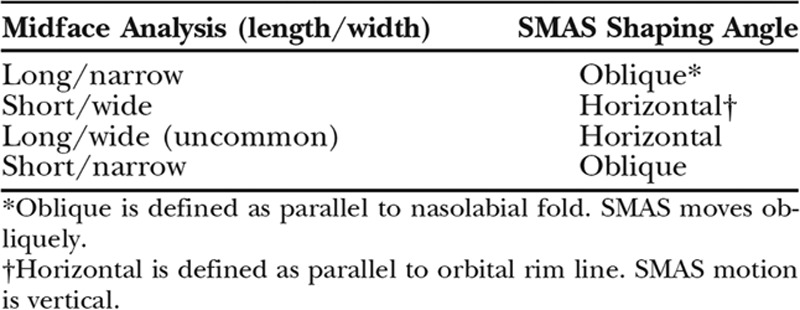
The decision of which SMAS technique to use is somewhat a topic of debate, including SMAS plication,44 SMASectomy,10,45 extended SMAS flap,19 high SMAS,46,47 and deep plane32,48 techniques. Despite the plethora of available techniques, the authors feel that the most reproducible, safe, and efficient techniques are SMAS-stacking for patients that need volume (ie long and narrow faces; Fig. 10) or SMASectomy for patients that need tissue debulking (ie wide, heavy faces; Fig. 11).26 In narrow faces, the long axis of SMASectomy or stacking is performed obliquely along a line from the lateral canthus to the gonial angle to improve midfacial width. However, a more horizontal vector is used in wide faces to improve submalar hollowing and avoid further midfacial widening (Figs. 12 and 13). The SMAS is secured with figure-of-eight 3-0 Mersilene (Ethicon, Inc., Somerville, N.J.), followed by running 4-0 Mersilene (Ethicon, Inc.) to prevent SMAS irregularities.
Fig. 10.
SMAS-stacking. SMAS incision and plication serve to stack tissue in the direction that the SMAS is lifted. The SMAS base remains while limited proximal and distal SMAS undermining allows the surgeon to create a 3-layered construct. This is beneficial in narrow faces that need more fullness in the malar region. This orientation of the SMAS-stacking will dictate where this augmentation is produced. Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
Fig. 11.
The oblique SMASectomy. SMAS movement is directed perpendicular to the nasolabial fold. This is beneficial for the narrower facial side. (Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
Fig. 12.
Horizontal SMASectomy. SMASectomy is oriented horizontally so that the SMAS moves in a vertical direction. This recruits more tissue superiorly, therefore increasing medial malar fullness while creating relative submalar hollowing. This technique is used for the wide midface so that excessive width is not recruited laterally, where it is not needed. Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
Fig. 13.
Individualized component facelift—SMAS shaping. Reprinted with permission from Plast Reconstr Surg. 2009;123:1050–1063.
SKIN REDRAPING AND CLOSURE
The skin flaps are redraped along a posterosuperior vector—care is taken not to recruit cervical rhytids onto the face, as iatrogenic rhytid displacement is a telltale sign of a poorly executed facelift. As previously described, the final extent of skin flap undermining is completed to assure the absence of skin puckering. Gauze moistened with a 3% tranexamic acid solution is placed beneath the skin flaps and allowed to sit for 3–5 minutes to help reduce bleeding, bruising, and edema.49–51
The tranexamic acid-soaked gauze is removed, and the skin flaps are then conservatively trimmed and inset with minimal tension. Platelet-rich plasma/thrombin mixture is spayed between the skin and SMAS layers. A closed suction drain is placed in the neck via a stab incision in the occipital scalp. Sparing 3-0 Monocryl (Ethicon, Inc.) deep dermal sutures are used, followed by 5-0 Nylon (Ethicon, Inc.) interrupted skin sutures. Staples are used on the incisions in hair-bearing areas. It is important to highlighting that if a intertragal approach is performed, the tragal skin flap is defatted, and the surgeon must be cognizant of the need for additional skin to account for the pretragal concavity—failure to account for this will result in “tenting” of the skin flap in the pretragal area and tension on the tragus, leading to tragal eversion and exposure of the auditory canal. The submental incision is closed with a running external 5-0 Nylon suture (Ethicon, Inc.). Avoidance of tension on the skin closure is paramount to avoid postoperative scar widening and auricular distortion.
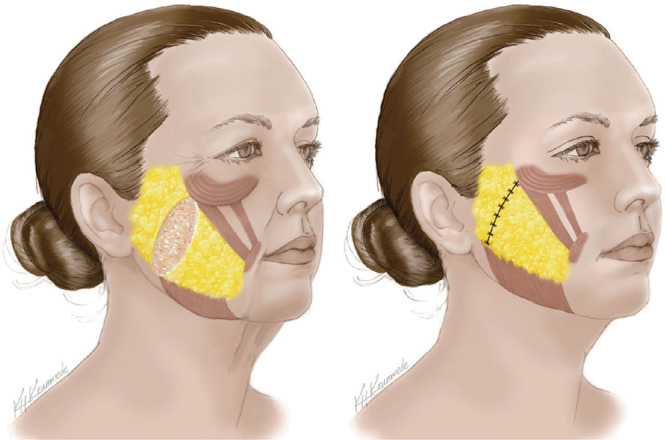
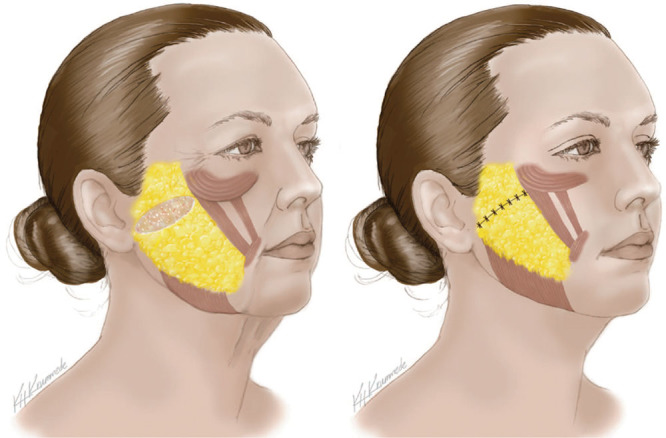
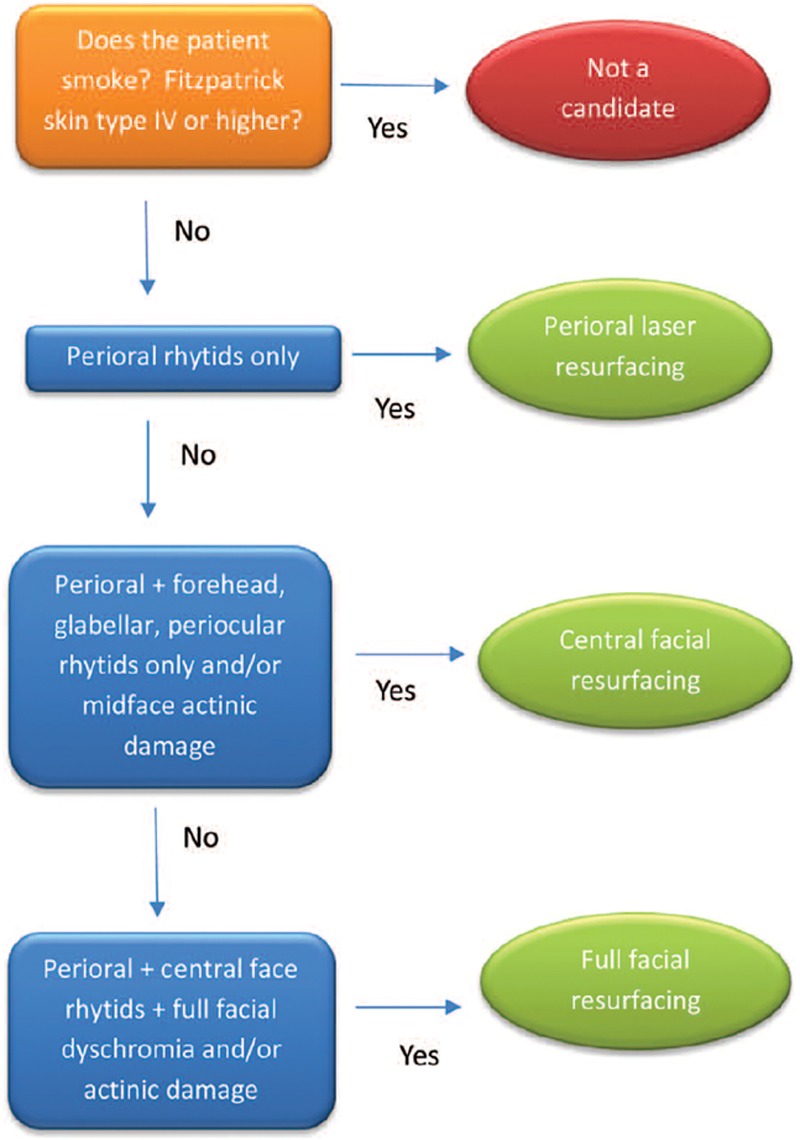
In patients who benefit from skin resurfacing (Fig. 14), the senior author (R.J.R.) has demonstrated that laser resurfacing and facelifting can be safely performed concomitantly after skin closure.52 In these patients, 500 mg of acyclovir 4 times daily for 7 days is commenced the day before surgery. Profile dual-mode erbium–aluminum–garnet (Sciton, Inc., Palo Alto, Calif.) laser is used with 2 passes with 50% overlap over nonundermined areas, and one oblique angle pass over undermined areas. Pre, intra, and postoperative considerations are essential to optimize safety and wound healing after skin resurfacing (Fig. 15).
Fig. 14.
Algorithm for face lift combined with laser resurfacing. Reprinted with permission from Plast Reconstr Surg. 2015;136:27–38.
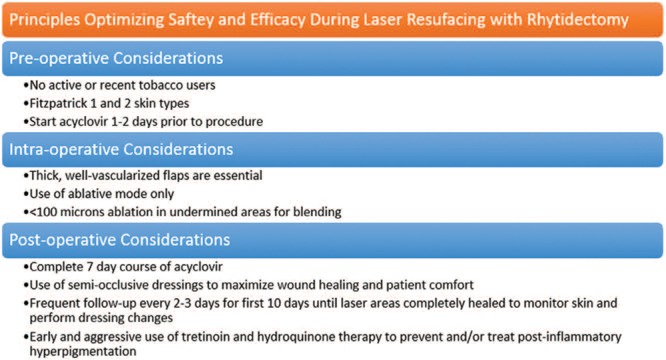
Fig. 15.
Principles optimizing safety and efficacy during laser resurfacing during laser resurfacing with rhytidectomy. Reprinted with permission from Plast Reconstr Surg. 2015;136:27–38.
Xeroform gauze and bacitracin are placed over the incisions followed by gauze then a kerlix head wrap and stockinette head dressing. The surgeon must be cognizant of the inelasticity of gauze dressings and anticipate a degree of postoperative edema; therefore, the kerlix wrap must be loosely applied to avoid pressure on the skin flaps.
POSTOPERATIVE MANAGEMENT
Patients are kept overnight with strict postoperative blood pressure, pain, and nausea management to prevent hematoma. The surgical dressings are changed the first postoperative day, and the neck drain is removed. The patient is allowed to return to regular activity 6 weeks after surgery and kept on a low-sodium diet for 1 month. Although the data are conflicting,53,54 a single 8 mg dose of intraoperative dexamethasone is given for both nausea prevention and to potentially decrease facial edema in the immediate postoperative period. However, available evidence at this time does not support the use of postoperative steroid use.55,56 An exception is in patients who undergo laser skin resurfacing, who are started on a methylprednisolone dose pack taper on postoperative day 1.
SPECIAL CONSIDERATIONS
The Male Patient
According to the 2017 American Society of Plastic Surgeons statistics, 11,719 or 9% of all facelifts were performed in males.1 While many similarities exist with the approach to the female patient, the male patient requires special considerations (Figs. 16 and 17).57 Furthermore, male patients are counseled to avoid vasoactive medications (eg, Viagra; Pfizer, New York, N.Y.) for 4 weeks postoperatively.
Fig. 16.
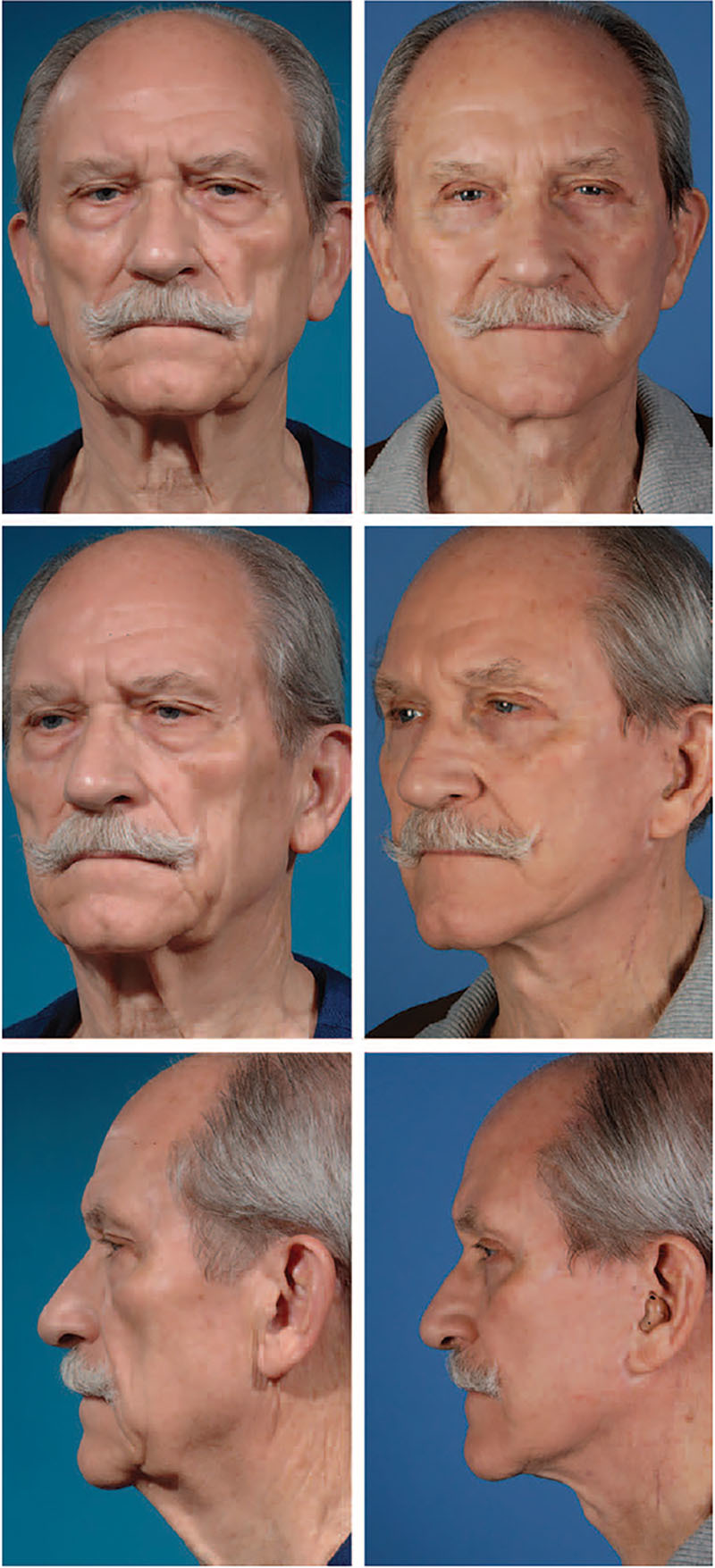
Photographs obtained preoperatively (A) and 18 months postoperatively (B) of a 75-year-old man who underwent SMASectomy and plication with deep malar fat augmentation. Reprinted with permission from Plast Reconstr Surg. 2017;139:295–307.
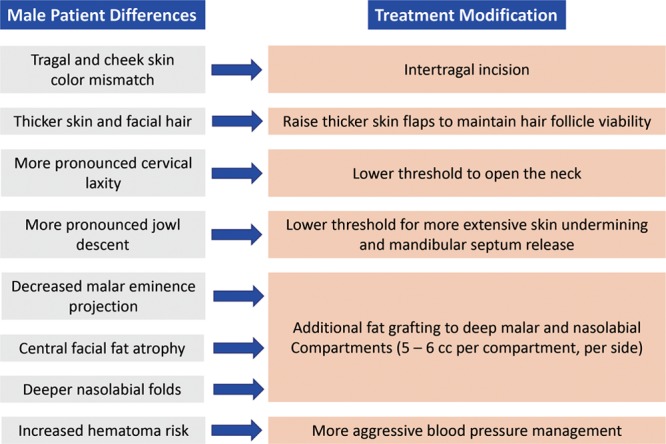
Fig. 17.
Differences and treatment modifications in male rhytidectomy.
Secondary and Tertiary Facelifts
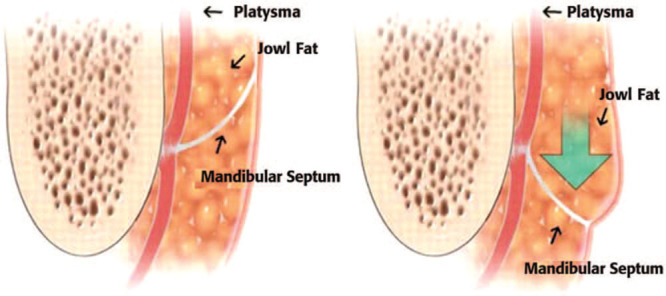
The secondary and tertiary facelift patients tend to be older and often present with iatrogenic deformities from their prior rhytidectomy (Fig. 18). Furthermore, secondary facelifts require more volumization and minimal, if any, skin excision. Pixie ear deformity (ie, tethered appearing and anteriorly rotated lobule) is common and requires anatomic posterior lobule rotation, scar excision and avoidance of skin flap tension. Other deformities include sideburn distortion and the “windswept” deformity. Skin flap elevation is more difficult due to scarring of the tissue planes, making the use of infiltrating solution evermore critical for hydrodissection.58 The senior author (R.J.R) endorses the “five Rs” of secondary facelift which include resection of prior scar, release of the SMAS, reshaping via tissue stacking and volumization, and skin release and redraping to correct depressions, “windswept” and J-deformities.59
Fig. 18.
Laxity and descent of the mandibular septum leading to jowl formation. Reprinted with permission from Plast Reconstr Surg. 2013;132339–350.
MANAGEMENT OF COMPLICATIONS
Hematoma
Prompt recognition is paramount as large hematomas can result in skin flap necrosis and airway compromise. Although smaller hematomas are not life threatening, failure to evacuate these results in scarring and contour irregularities that are difficult to treat secondarily. Large hematomas require return to the operating room. Small hematomas can be aspirated with a 16-guage needle 5–7 days after surgery in clinic, once the hematoma has liquified.
Seroma
Use of a closed neck drain helps avoid most seromas as they usually occur the most gravity-dependent areas. A chin strap is also used as a compression garment to close dead space.60 If a seroma occurs, it should be serially drained by aspiration until resolved. For persistent areas of induration and if the seroma cannot be aspirated, injections of Kenalog 10 mg/ml diluted with 1% lidocaine injections are used.
Recurrent Platysmal Bands
Recurrent banding is most common medially. A low threshold for a submental incision and medial platysmal plication helps to decrease the incidence of recurrent platysmal bands. Despite appropriate operative interventions, platysmal bands may still recur. In these patients, either reoperation or Botox (Allergan, Inc., Irvine, Calif.) can be used.34
Persistent/Recurrent Jowling
Persistent jowling can result from insufficient mandibular retaining ligament release and jowl fat pad lipodystrophy (Fig. 16). Extended skin undermining with release of the mandibular retaining ligament, with direct fat excision if necessary, is critical in patients with prominent jowls.61 Targeted liposuction and/or fat grafting is used for secondary jowl bulges or jawline scalloping, respectively.34
Skin Necrosis
Avoiding surgery in high-risk patients (ie, nicotine product users) and maintaining at least 3 mm of fat on the skin flap undersurface prevent the majority of cases. Exacerbating factors such as excess skin tension is avoided and hematoma, if present, must be promptly addressed. Nitroglycerin ointment can be applied in the operating room over compromised appearing areas. Otherwise, areas of necrosis are conservatively managed with daily cleaning and triple antibiotic ointment application until the ischemic margins fully declare themselves and the eschar falls off. Areas that have healed by secondary intention can be addressed at a later date with scar revision.
Marginal Mandibular Nerve Palsy
Conservative management is used. Neuropraxia is the most common culprit and expected to resolve within 3 months of surgery. Contralateral depressor angularis oris neurotoxin injection can be used as a temporizing measure to improve smile symmetry.
Sialocele
The senior author (R.J.R.) avoids submandibular gland surgery as this risks sialocele formation and bleeding complications. Salivary leaks can be managed by serial aspiration, anticholinergics, and neurotoxin injection.
CONCLUSIONS
The modern facelift is a sophisticated operation that focuses on treating targeted areas of facial aging using an individualized and detailed approach to the SMAS, skin, and fat compartments. Maximizing patient safety and consistency is the key to this operation to deliver high patient satisfaction.
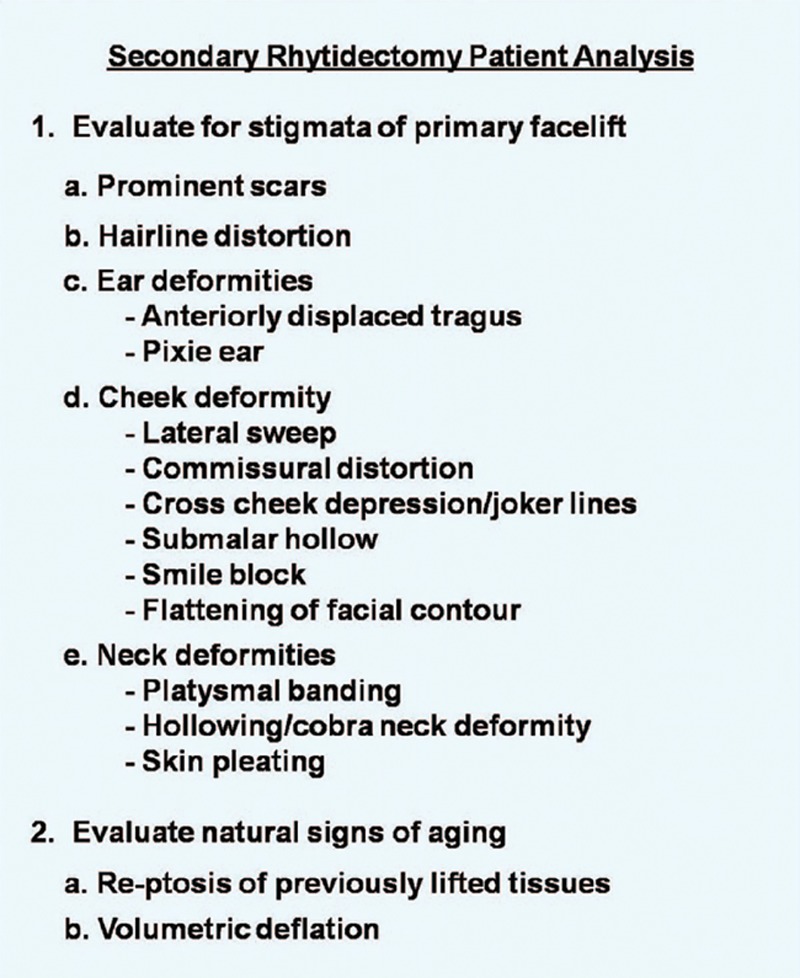
Fig. 19.
Secondary rhytidectomy patient analysis. Reprinted with permission from Plast Reconstr Surg. 2012;130:1370–1378.
Footnotes
Published online 7 June 2019.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.ASPS. 2017 Plastic Surgery Statistics Report, American Society of Plastic Surgeons, Available at https://www.plasticsurgery.org/documents/News/Statistics/2017/plastic-surgery-statistics-full-report-2017.pdf. Accessed October 14, 2018.
- 2.Sinno S, Schwitzer J, Anzai L, et al. Face-lift satisfaction using the FACE-Q. Plast Reconstr Surg. 2015;136:239–242. [DOI] [PubMed] [Google Scholar]
- 3.Rohrich RJ, Pessa JE. The fat compartments of the face: anatomy and clinical implications for cosmetic surgery. Plast Reconstr Surg. 2007;119:2219–2227; discussion 2228–2231. [DOI] [PubMed] [Google Scholar]
- 4.Schaverien MV, Pessa JE, Rohrich RJ. Vascularized membranes determine the anatomical boundaries of the subcutaneous fat compartments. Plast Reconstr Surg. 2009;123:695–700. [DOI] [PubMed] [Google Scholar]
- 5.Alghoul M, Codner MA. Retaining ligaments of the face: review of anatomy and clinical applications. Aesthet Surg J. 2013;33:769–782. [DOI] [PubMed] [Google Scholar]
- 6.Costa CR, Ramanadham SR, O’Reilly E, et al. The role of the superwet technique in face lift: an analysis of 1089 patients over 23 years. Plast Reconstr Surg. 2015;135:1566–1572. [DOI] [PubMed] [Google Scholar]
- 7.Griffin JE, Jo C. Complications after superficial plane cervicofacial rhytidectomy: a retrospective analysis of 178 consecutive facelifts and review of the literature. J Oral Maxillofac Surg. 2007;65:2227–2234. [DOI] [PubMed] [Google Scholar]
- 8.Beer GM, Goldscheider E, Weber A, et al. Prevention of acute hematoma after face-lifts. Aesthetic Plast Surg. 2010;34:502–507. [DOI] [PubMed] [Google Scholar]
- 9.Berner RE, Morain WD, Noe JM. Postoperative hypertension as an etiological factor in hematoma after rhytidectomy. Prevention with chlorpromazine. Plast Reconstr Surg. 1976;57:314–319. [DOI] [PubMed] [Google Scholar]
- 10.Baker D. Rhytidectomy with lateral SMASectomy. Facial Plast Surg. 2000;16:209–213. [DOI] [PubMed] [Google Scholar]
- 11.Straith RE, Raju DR, Hipps CJ. The study of hematomas in 500 consecutive face lifts. Plast Reconstr Surg. 1977;59:694–698. [DOI] [PubMed] [Google Scholar]
- 12.Perkins SW, Williams JD, Macdonald K, et al. Prevention of seromas and hematomas after face-lift surgery with the use of postoperative vacuum drains. Arch Otolaryngol Head Neck Surg. 1997;123:743–745. [DOI] [PubMed] [Google Scholar]
- 13.Mitz V, Peyronie M. The superficial musculo-aponeurotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg. 1976;58:80–88. [DOI] [PubMed] [Google Scholar]
- 14.Furnas DW. The retaining ligaments of the cheek. Plast Reconstr Surg. 1989;83:11–16. [DOI] [PubMed] [Google Scholar]
- 15.Stuzin JM, Baker TJ, Gordon HL. The relationship of the superficial and deep facial fascias: relevance to rhytidectomy and aging. Plast Reconstr Surg. 1992;89:441–459; discussion 450. [PubMed] [Google Scholar]
- 16.Pessa JE, Rohrich RJ. Facial Topography. Clinical Anatomy of the Face. 2012St. Louis, Mo.: Quality Medical Publishing. [Google Scholar]
- 17.Roostaeian J, Rohrich RJ, Stuzin JM. Anatomical considerations to prevent facial nerve injury. Plast Reconstr Surg. 2015;135:1318–1327. [DOI] [PubMed] [Google Scholar]
- 18.Alghoul M, Bitik O, McBride J, et al. Relationship of the zygomatic facial nerve to the retaining ligaments of the face: the Sub-SMAS danger zone. Plast Reconstr Surg. 2013;131:245e–252e. [DOI] [PubMed] [Google Scholar]
- 19.Stuzin JM. Neligan PC. Facelift: The extended SMAS technique in facial rejuvenation. In: Plastic Surgery. 2012;Vol II:3rd ed Philadelphia: Elsevier; 238–256. [Google Scholar]
- 20.Pessa JE. An algorithm of facial aging: verification of Lambros’s theory by three-dimensional stereolithography, with reference to the pathogenesis of midfacial aging, scleral show, and the lateral suborbital trough deformity. Plast Reconstr Surg. 2000;106:479–488; discussion 489. [DOI] [PubMed] [Google Scholar]
- 21.Pessa JE, Chen Y. Curve analysis of the aging orbital aperture. Plast Reconstr Surg. 2002;109:751–755; discussion 756. [DOI] [PubMed] [Google Scholar]
- 22.Pessa JE, Desvigne LD, Lambros VS, et al. Changes in ocular globe-to-orbital rim position with age: implications for aesthetic blepharoplasty of the lower eyelids. Aesthetic Plast Surg. 1999;23:337–342. [DOI] [PubMed] [Google Scholar]
- 23.Kligman LH. Photoaging. Manifestations, prevention, and treatment. Clin Geriatr Med. 1989;5:235–251. [PubMed] [Google Scholar]
- 24.Pezeshk RA, Small KH, Rohrich RJ. Filling the facial compartments during a face lift. Plast Reconstr Surg. 2015;136:704–705. [DOI] [PubMed] [Google Scholar]
- 25.Rohrich RJ, Ghavami A, Constantine FC, et al. Lift-and-fill face lift: integrating the fat compartments. Plast Reconstr Surg. 2014;133:756e–767e. [DOI] [PubMed] [Google Scholar]
- 26.Rohrich RJ, Ghavami A, Lemmon JA, et al. The individualized component face lift: developing a systematic approach to facial rejuvenation. Plast Reconstr Surg. 2009;123:1050–1063. [DOI] [PubMed] [Google Scholar]
- 27.Levine SM, Sinno S, Cannavo D, et al. Selective serotonin reuptake inhibitor-induced hyponatremia and the plastic surgery patient. Plast Reconstr Surg. 2017;139:1481–1488. [DOI] [PubMed] [Google Scholar]
- 28.Marten TJ. High SMAS facelift: combined single flap lifting of the jawline, cheek, and midface. Clin Plast Surg. 2008;35:569, vi–603, vi. [DOI] [PubMed] [Google Scholar]
- 29.Marten TJ, Elyassnia D. Neligan PC. Secondary deformities and the secondary facelift. In: Plastic Surgery. 2012;Vol II:3rd ed Philadelphia: Elsevier; 277–312. [Google Scholar]
- 30.Narasimhan K, Stuzin JM, Rohrich RJ. Five-step neck lift: integrating anatomy with clinical practice to optimize results. Plast Reconstr Surg. 2013;132:339–350. [DOI] [PubMed] [Google Scholar]
- 31.Gassman AA, Pezeshk R, Scheuer JF, III, et al. Anatomical and clinical implications of the deep and superficial fat compartments of the neck. Plast Reconstr Surg. 2017;140:405e–414e. [DOI] [PubMed] [Google Scholar]
- 32.Mustoe TA, Rawlani V, Zimmerman H. Modified deep plane rhytidectomy with a lateral approach to the neck: an alternative to submental incision and dissection. Plast Reconstr Surg. 2011;127:357–370. [DOI] [PubMed] [Google Scholar]
- 33.Pelle-Ceravolo M, Angelini M, Silvi E. Treatment of anterior neck aging without a submental approach: lateral skin-platysma displacement, a new and proven technique for platysma bands and skin laxity. Plast Reconstr Surg. 2017;139:308–321. [DOI] [PubMed] [Google Scholar]
- 34.Narasimhan K, Ramanadham S, O’Reilly E, et al. Secondary neck lift and the importance of midline platysmaplasty: review of 101 cases. Plast Reconstr Surg. 2016;137:667e–675e. [DOI] [PubMed] [Google Scholar]
- 35.Grover R, Jones BM, Waterhouse N. The prevention of haematoma following rhytidectomy: a review of 1078 consecutive facelifts. Br J Plast Surg. 2001;54:481–486. [DOI] [PubMed] [Google Scholar]
- 36.Abboushi N, Yezhelyev M, Symbas J, et al. Facelift complications and the risk of venous thromboembolism: a single center’s experience. Aesthet Surg J. 2012;32:413–420. [DOI] [PubMed] [Google Scholar]
- 37.Ramanadham SR, Costa CR, Narasimhan K, et al. Refining the anesthesia management of the face-lift patient: lessons learned from 1089 consecutive face lifts. Plast Reconstr Surg. 2015;135:723–730. [DOI] [PubMed] [Google Scholar]
- 38.Brown SA, Appelt EA, Lipschitz A, et al. Platelet gel sealant use in rhytidectomy. Plast Reconstr Surg. 2006;118:1019–1025. [DOI] [PubMed] [Google Scholar]
- 39.Rohrich RJ, Narasimhan K. Long-term results in face lifting: observational results and evolution of technique. Plast Reconstr Surg. 2016;138:97–108. [DOI] [PubMed] [Google Scholar]
- 40.Connell BF, Shamoun JM. The significance of digastric muscle contouring for rejuvenation of the submental area of the face. Plast Reconstr Surg. 1997;99:1586–1590. [PubMed] [Google Scholar]
- 41.Mendelson BC, Tutino R. Submandibular gland reduction in aesthetic surgery of the neck: review of 112 consecutive cases. Plast Reconstr Surg. 2015;136:463–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bucky L. Facelift, how deep how wide. Paper presented at: American Society of Plastic Surgeons “The Meeting”; September 30, 2018; Chicago, IL. [Google Scholar]
- 43.Pezeshk RA, Sieber DA, Rohrich RJ. Neck rejuvenation through the lateral platysma window: a key component of face-lift surgery. Plast Reconstr Surg. 2017;139:865–866. [DOI] [PubMed] [Google Scholar]
- 44.Robbins LB, Brothers DB, Marshall DM. Anterior SMAS plication for the treatment of prominent nasomandibular folds and restoration of normal cheek contour. Plast Reconstr Surg. 1995;96:1279–1287; discussion 1288. [DOI] [PubMed] [Google Scholar]
- 45.Baker DC. Lateral SMASectomy. Plast Reconstr Surg. 1997;100:509–513. [DOI] [PubMed] [Google Scholar]
- 46.Barton FE., Jr. The “high SMAS” face lift technique. Aesthet Surg J. 2002;22:481–486. [DOI] [PubMed] [Google Scholar]
- 47.Barton FE, Jr, Hunt J. The high-superficial musculoaponeurotic system technique in facial rejuvenation: an update. Plast Reconstr Surg. 2003;112:1910–1917. [DOI] [PubMed] [Google Scholar]
- 48.Hamra ST. The deep-plane rhytidectomy. Plast Reconstr Surg. 1990;86:53–61; discussion 62. [PubMed] [Google Scholar]
- 49.Brown S, Yao A, Taub PJ. Antifibrinolytic agents in plastic surgery: current practices and future directions. Plast Reconstr Surg. 2018;141:937e–949e. [DOI] [PubMed] [Google Scholar]
- 50.Butz DR, Geldner PD. The use of tranexamic acid in rhytidectomy patients. Plast Reconstr Surg Glob Open. 2016;4:e716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Rohrich RJ, Cho MJ. The role of tranexamic acid in plastic surgery: review and technical considerations. Plast Reconstr Surg. 2018;141:507–515. [DOI] [PubMed] [Google Scholar]
- 52.Scheuer JF, 3rd, Costa CR, Dauwe PB, et al. Laser resurfacing at the time of rhytidectomy. Plast Reconstr Surg. 2015;136:27–38. [DOI] [PubMed] [Google Scholar]
- 53.Hoefflin SM. Decreasing prolonged swelling and pain associated with deep plane face lifts. Plast Reconstr Surg. 1992;90:1125. [DOI] [PubMed] [Google Scholar]
- 54.Owsley JQ, Weibel TJ, Adams WA. Does steroid medication reduce facial edema following face lift surgery? A prospective, randomized study of 30 consecutive patients. Plast Reconstr Surg. 1996;98:1–6. [DOI] [PubMed] [Google Scholar]
- 55.da Silva EM, Hochman B, Ferreira LM. Perioperative corticosteroids for preventing complications following facial plastic surgery. Cochrane Database Syst Rev. 2014;2(6):CD009697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Pulikkottil BJ, Dauwe P, Daniali L, et al. Corticosteroid use in cosmetic plastic surgery. Plast Reconstr Surg. 2013;132:352e–360e. [DOI] [PubMed] [Google Scholar]
- 57.Rohrich RJ, Stuzin JM, Ramanadham S, et al. The modern male rhytidectomy: lessons learned. Plast Reconstr Surg. 2017;139:295–307. [DOI] [PubMed] [Google Scholar]
- 58.Rasko YM, Beale E, Rohrich RJ. Secondary rhytidectomy: comprehensive review and current concepts. Plast Reconstr Surg. 2012;130:1370–1378. [DOI] [PubMed] [Google Scholar]
- 59.Beale EW, Rasko Y, Rohrich RJ. A 20-year experience with secondary rhytidectomy: a review of technique, longevity, and outcomes. Plast Reconstr Surg. 2013;131:625–634. [DOI] [PubMed] [Google Scholar]
- 60.Knize DM. Limited incision submental lipectomy and platysmaplasty. Plast Reconstr Surg. 2004;113:1275–1278. [DOI] [PubMed] [Google Scholar]
- 61.Stuzin JM. MOC-PSSM CME article: face lifting. Plast Reconstr Surg. 2008;121(Suppl 1):1–19. [DOI] [PubMed] [Google Scholar]