

Abstract
Background:
Knee laxity in the setting of anterior cruciate ligament injury is often assessed through physical examination using the Lachman, pivot-shift, and anterior drawer tests. The degree of laxity noted on these examinations may influence treatment decisions and prognosis.
Hypothesis:
Increased pre-operative knee laxity is associated with increased risk of revision ACL reconstruction, increased risk of contralateral ACL reconstruction, and poorer patient-reported outcomes at six years postoperative.
Study design:
Cohort study.
Methods:
2333 patients who underwent primary isolated ACL reconstruction without additional ligament injury were identified. Patients reported by the operating surgeons to have an International Knee Documentation Committee Grade D Lachman, anterior drawer, or pivot-shift examination were classified as having a high-grade laxity. Multiple logistic regression models were utilized to evaluate whether having high-grade pre-operative laxity was predictive of increased odds of undergoing subsequent revision or contralateral ACL reconstruction within six years of the index procedure, controlling for patient age, sex, Marx activity level, level of competition, and graft type. Multiple linear regression modeling was used to evaluate whether having high-grade pre-operative laxity was predictive of poorer IKDC or KOOS-QOL scores at 6 years postoperative, controlling for baseline score, patient age, ethnicity, sex, BMI, marital status, smoking status, sport participation, competition level, Marx activity rating score, graft type, and articular cartilage and meniscus status.
Results:
High-grade Lachman was noted in 334 patients (14.3%), high-grade pivot-shift was noted in 617 patients (26.5%), and high-grade anterior drawer was noted in 233 patients (10.0%). Six year revision and contralateral ACL reconstruction data were available for 2129 patients (91.6%). High-grade pre-reconstruction Lachman was associated with significantly increased odds of ACL graft revision (OR=1.76, p = 0.02) and contralateral ACL reconstruction (OR=1.68, p = 0.019). High-grade pre-reconstruction pivot-shift was associated with significantly increased odds of ACL graft revision (OR=1.75, p = 0.002) but not with significantly increased odds of contralateral ACL reconstruction (OR=1.30, p = 0.19). High-grade pre-reconstruction laxity was associated with statistically significantly lower 6-year IKDC (β = −2.26, p = 0.003), KOOS-QOL (β = −2.67, p = 0.015), and Marx Activity score (β = −0.54, p = 0.020), but these differences do not approach clinically relevant differences in patient-reported outcomes.
Conclusion:
High-grade pre-operative knee laxity is predictive of increased odds of revision ACL reconstruction and contralateral ACL reconstruction 6 years following ACL reconstruction. Poorer patient-reported outcome scores in the high-grade laxity group were also noted but the difference did not reach a level of clinical relevance.
Introduction
Physical examination using the Lachman,28 pivot-shift,4, 12 and anterior drawer tests16 is frequently utilized by the treating physician to diagnose an anterior cruciate ligament (ACL) injury. These physical examination tests often reveal increased laxity when the ACL is ruptured, but the degree of increased laxity varies greatly among patients. The information that variability in laxity among ACL-injured patients may provide in regards to decisions and prognosis has not been extensively evaluated.
The presence a relatively high degree of knee laxity in a patient’s knee after sustaining an ACL injury may indicate the presence of concomitant injuries in addition to the ACL tear.15 Prior work has demonstrated that injury to the menisci15, 19 as well as patient factors such as age and sex15 are associated with increased knee laxity prior to reconstruction.19 In addition to these factors, increased laxity may also be associated with increased risk of capsular injury, particularly in the anterolateral aspect of the knee.27, 29 Patients with high-grade pre-reconstruction laxity (defined as a Lachman or anterior drawer examination greater than 10mm different from the contralateral side or a 3+ pivot-shift) have been previously shown to be at increased risk to undergo revision ACL reconstruction within two years,14 but longer term effects and the relationship between increased knee laxity and risk of subsequent contralateral ACL injury are unknown.
The purpose of this study was to determine whether high-grade laxity of the injured knee as assessed by the surgeon during an exam under anesthesia prior to ACL reconstruction is predictive of subsequent ACL revision risk, contralateral ACL reconstruction risk, and patient-reported outcomes following ACL reconstruction. The hypothesis tested was that increased pre-operative knee laxity would be predictive of increased risk of subsequent revision ACL reconstruction, increased risk of subsequent contralateral ACL reconstruction, and poorer patient-reported outcomes at six years postoperative.
Methods
Patients
Between 2002 and 2008, 2859 patients who underwent ACL reconstruction were identified and enrolled in a prospective outcome study. All patients underwent intra-articular ACL reconstruction without associated extra-articular reconstructions or lateral tenodeses. All patients underwent the same rehabilitation protocol.32 For the current study, those undergoing revision surgery (321) or simultaneous bilateral reconstructions (13), as well as those with associated grade 2 or 3 collateral ligament injuries (167) or PCL tears (25) were excluded, leaving 2333 patients who were eligible for inclusion (Figure 1). Institutional Review Board approval was obtained at participating institutions.
Figure 1.
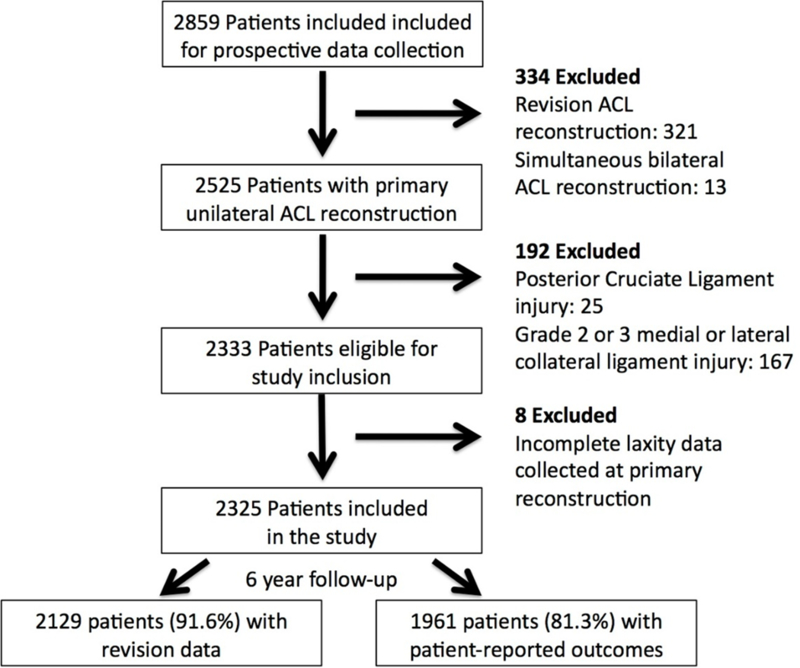
Flow chart for patient selection.
Data Extraction
Prospective data collection included patient age, sex, ethnicity, marital status, and body mass index [BMI]; smoking status; knee laxity during examination under anesthesia prior to ACL reconstruction; sport at injury; level of competition; graft type; data regarding meniscus and articular cartilage status; pre-operative and 6 year postoperative subjective International Knee Documentation Committee (IKDC),8 Knee injury and Osteoarthritis Outcome Score Knee-Related Quality of Life (KOOS-QOL),24 and Marx activity rating scores;18 the incidence of subsequent revision ACL reconstruction within six years of the index surgery; and the incidence of subsequent contralateral ACL reconstruction within six years of the index surgery. Ethnicity was classified as white, black, other, or unknown and marital status was documented as single, married, or other. Patients were classified as either a recent smoker (current smoker or quit within 6 months of study consent) or not a recent smoker (nonsmoker or quit greater than 6 months prior to study consent). It was documented whether the patient was playing a sport at injury and if so the sport was classified as football, soccer, basketball, or other. Level of sport competition was recorded as competitive (high school, club, collegiate, or professional) or recreational. Graft type was classified as patellar tendon autograft, hamstring tendon autograft, quadriceps autograft, or allograft (this category included hybrid grafts containing both autograft and allograft material). Medial and lateral meniscus status was recorded as it was at the end of the index procedure as intact, partial meniscectomy, meniscus repair, or untreated stable tear. Articular cartilage status was classified according to the modified Outerbridge Classification22 in each of the three compartments (medial, lateral, patellofemoral). Due to poor reported inter-rater agreement between grade 2 and 3 lesions,17 the grade for each compartment was dichotomized based on the worst score in that compartment as minimal (modified Outerbridge 0 or 1) or significant (modified Outerbridge 2, 3, or 4) cartilage injury. Knee laxity was reported according to the IKDC classification system.6 High-grade laxity was defined as a Lachman or anterior drawer examination greater than 10mm different from the contralateral side or a 3+ pivot-shift.
Statistics
Multiple logistic regression modeling was used to evaluate whether high-grade pre-reconstruction laxity was predictive of risk of subsequent revision ACL reconstruction. Other variables evaluated as potential confounders or effect modifiers included patient age, sex, ethnicity, smoking status, marital status, and BMI; Marx activity rating score at reconstruction; sport at injury; level of competition; graft type; medial and lateral meniscus status; and articular cartilage status. Given the number of surgeons in the study, surgeon could not be included in the model due to lack of power. A separate analysis did demonstrate no significant effect of surgeon on graft failure risk. A forward selection modeling procedure was utilized with variables sequentially added to the model and kept in the model if they resulted in a change in the odds ratio of the variable of interest of greater than 0.05. The final model included patient age, sex, BMI, Marx activity rating score, sport, graft type, medial meniscus treatment, and lateral meniscus treatment. Due to the small number of patients (3), patients who received quadriceps autografts were excluded from this analysis. Based on the 16 degrees of freedom required to model these potential predictor variables, the 146 “events” (revision ACL reconstructions) recorded during the 6 year follow-up period provided sufficient power for this analysis. The analysis was repeated using the presence of high-grade laxity on at least two of the three examinations (Lachman, high-grade pivot-shift, and high-grade anterior drawer) and the presence of high-graft laxity on all three examinations as the primary independent variable. Finally, the same model was utilized to evaluate whether the presence of high-grade laxity was a predictor of subsequent contralateral ACL injury (n=156 “events”). Consideration was given to the possibility of significant interaction terms. Based on clinical relevance, the interactions between graft type and each measure of laxity were modeled and no significant interactions were noted. These terms were therefore not included in the models. In addition, due to concern regarding variation in laxity assessment among surgeons, a separate logistic regression was performed to evaluate whether surgeon was a significant predictor of revision risk, controlling for known predictors of revision in this dataset (age and graft type). Surgeon was not a predictor of revision risk and was not included in any further models.
Multiple linear regression modeling was used to evaluate whether high-grade pre-reconstruction laxity was predictive of subjective IKDC score or KOOS-QOL at six years postoperative, controlling for baseline score; patient age, sex, ethnicity, smoking status marital status, and BMI; Marx activity rating score at reconstruction; sport at injury; level of competition; graft type; medial and lateral meniscus status; and articular cartilage status. The presence of interactions between all included predictors was evaluated and no significant interactions were identified. The analysis was repeated using the presence of high-grade laxity on at least two of the three examinations (Lachman, high-grade pivot-shift, and high-grade anterior drawer) and the presence of high-grade laxity on all three examinations as the primary independent variable.
Results
Pre-reconstruction laxity data were available for 2325 patients (99.7%). Patient characteristics at the time of surgery are described in Table 1. In total, 743 of 2325 patients (32.0%) were noted to have high-grade laxity on at least one physical examination test. High-grade pivot-shift was most frequently identified (617 patients, 26.5%), with high-grade Lachman (334 patients, 14.4%) and high-grade anterior drawer (233 patients, 10.0%) also identified. The proportion of patients noted to have high-grade laxity varied among the 17 surgeons (Table 2), but was not dependent on volume of reconstructions performed.
Table 1:
Patient Characteristics (n = 2325 patients)
| Age (Mean ± SD) | 26.7 ± 11.1 years |
|---|---|
| Sex | Male: 1302 (56.0%) Female: 1023 (44.0%) |
| Ethnicity | White: 1929 (83.0%) Black: 195 (8.4%) Other: 193 (8.3%) Unknown/not reported: 8 (0.3%) |
| Marital Status | Single: 1500 (64.5%) Married: 656 (28.2%) Other: 84 (3.6%) Unknown/not reported: 85 (3.7%) |
| Body Mass Index | 25.5 ± 4.9 kg/m2 |
| Smoking Status | Nonsmoker: 2033 (87.4%) Smoker: 280 (12.0%) Unknown/not reported: 12 (0.6%) |
| Sport at Injury | Basketball: 508 (21.8%) Football: 299 (12.9%) Soccer: 372 (16.0%) Other: 791 (34.0%) None: 355 (15.3%) |
| Level of Competition | Competitive: 917 (39.4%) Recreational: 1394 (60.0%) Unknown/not reported: 14 (0.6%) |
| Graft Type | BTB Autograft: 1037 (44.7%) Hamstring Autograft: 881 (37.9%) Quadriceps Autograft: 3 (0.1%) Allograft: 404 (17.4%) |
| Medial Meniscus Status | Intact: 1389 (59.7%) Meniscectomy: 431 (18.5%) Repaired: 371 (16.0%) Stable Untreated Tear: 130 (5.6%) Unknown: 3 (0.1%) |
| Lateral Meniscus Status | Intact: 1217 (52.3%) Meniscectomy: 688 (29.6%) Repaired: 163 (7.0%) Stable Untreated Tear: 257 (11.1%) |
| Medial Articular Cartilage Status (Modified Outerbridge) | Grade 0 or 1: 1796 (77.2%) Grade2, 3, or 4: 529 (22.8%) |
| Lateral Articular Cartilage Status (Modified Outerbridge) |
Grade 0 or 1: 1835 (78.9%) Grade2, 3, or 4: 490 (21.2%) |
| Patellofemoral Articular Cartilage Status (Modified Outerbridge) |
Grade 0 or 1: 1858 (79.9%) Grade2, 3, or 4: 467 (20.1%) |
Table 2:
Percentage of Patients with High-Grade Pre-operative Laxity
| Surgeon | Lachman | Anterior Drawer |
Pivot-Shift | Any measure |
|---|---|---|---|---|
| 1 (n = 79) | 17.7% | 5.1% | 11.4% | 22.8% |
| 2 (n = 11) | 9.1% | 0.0% | 9.1% | 18.2% |
| 3 (n = 36) | 0.0% | 2.8% | 11.1% | 11.1% |
| 4 (n = 510) | 15.5% | 14.3% | 16.9% | 23.2% |
| 5 (n = 116) | 36.2% | 10.3% | 16.4% | 38.8% |
| 6 (n = 122) | 4.1% | 0.0% | 3.3% | 4.1% |
| 7 (n = 23) | 17.4% | 8.7% | 47.8% | 47.8% |
| 8 (n = 130) | 8.5% | 0.8% | 20.8% | 25.4% |
| 9 (n = 429) | 25.9% | 24.1% | 43.8% | 46.6% |
| 10 (n = 14) | 7.1% | 0.0% | 21.4% | 35.7% |
| 11 (n = 78) | 19.2% | 12.8% | 5.1% | 19.2% |
| 12 (n = 19) | 0.0% | 0.0% | 0.0% | 0.0% |
| 13 (n = 127) | 0.8% | 0.0% | 1.6% | 2.4% |
| 14 (n = 350) | 5.4% | 2.9% | 68.9% | 69.4% |
| 15 (n = 34) | 73.5% | 34.3% | 5.7% | 73.5% |
| 16 (n = 230) | 4.4% | 3.5% | 5.6% | 6.5% |
| 17 (n = 31) | 0.0% | 0.0% | 6.5% | 6.5% |
Six-year revision data were available for 2129 patients (91.6%) and patient-reported outcomes were available for 1961 patients (84.3%). ACL graft revision was performed in 147 patients (6.9%), including 94 patients who underwent revision within the first two years following primary ACL reconstruction and 53 patients who underwent revision surgery between 2 and 6 years following primary ACL reconstruction. In the multiple logistic regression model, identification of high-grade pre-reconstruction laxity on at least one physical examination test was predictive of significantly increased odds of subsequent ACL graft revision (OR=1.73, 95% CI: 1.19 – 2.51, p = 0.004). High-grade pivot-shift (OR=1.75, p = 0.002) and Lachman (OR=1.76, p = 0.020) were also predictive of increased revision risk, while the relationship between high-grade anterior drawer and revision surgery was not statistically significant (OR=1.60, p = 0.098) (Table 3). The absence of significant interactions between predictor variables demonstrates that none of the co-variates included in the model affect failure risk in patients in the high-grade laxity group differently than in those patients without increased laxity.
Table 3:
Relationships between high-grade pre-reconstruction knee laxity and revision ACL surgery within 6 years post-op
| High-grade laxity | Odds Ratio | 95% Confidence Interval |
Significance |
|---|---|---|---|
| 3+ Pivot-shift | 1.75 | 1.19 – 2.54 | p = 0.002 |
| Lachman > 10mm | 1.76 | 1.10 – 2.80 | p = 0.020 |
| Anterior Drawer > 10mm | 1.60 | 0.92 – 3.32 | p = 0.098 |
| Any one of the above | 1.73 | 1.19 – 2.51 | p = 0.004 |
Subsequent contralateral ACL reconstructions were performed in 156 patients (7.3%), including 68 patients who underwent contralateral ACL reconstruction within the first two years following primary ACL reconstruction and 88 patients who underwent contralateral ACL reconstruction between 2 and 6 years following primary ACL reconstruction. In the multiple logistic regression model, only the presence of a high-grade pre-reconstruction Lachman was predictive of significantly increased odds of contralateral ACL reconstruction (OR=1.68, 95% CI: 1.09 – 2.69, p = 0.019). High-grade pivot-shift (OR=1.30, p = 0.16) and anterior drawer (OR=1.14, p = 0.64) were not predictive of increased odds of contralateral ACL reconstruction (Table 4).
Table 4:
Relationships between high-grade pre-reconstruction knee laxity and contralateral ACL reconstruction within 6 years post-op
| High-grade laxity | Odds Ratio | 95% Confidence Interval |
Significance |
|---|---|---|---|
| 3+ Pivot-shift | 1.30 | 0.89 – 1.88 | p = 0.16 |
| Lachman > 10mm | 1.68 | 1.09 – 2.69 | p = 0.019 |
| Anterior Drawer > 10mm | 1.14 | 0.65 – 2.00 | p = 0.64 |
| Any one of the above | 1.37 | 0.96 – 1.95 | p = 0.08 |
The mean 6-year IKDC score was 82.6 ± 16.2, the mean KOOS-QOL score was 75.3 ± 22.2, and the mean 6-year Marx activity score was 7.4 ± 5.0. The mean IKDC score was 80.9 ± 17.5 in the high-grade laxity group and 83.3 ± 15.7 in the group without high-grade laxity. The mean 6-year KOOS-QOL score was 73.2 ± 23.2 in the high-grade laxity group and 76.3 ± 21.6 in the group without high-grade laxity. The mean 6-year Marx activity score was 7.0 ± 5.1 in the high-grade laxity group and 7.6 ± 5.0 in the group without high-grade laxity. Controlling for baseline score; patient age, sex, ethnicity, smoking status marital status, and BMI; Marx activity rating score at reconstruction; sport at injury; level of competition; graft type; medial and lateral meniscus status; and articular cartilage status, the presence of high-grade pre-reconstruction laxity was predictive of significantly lower 6-year IKDC (β = −2.26, p = 0.003), KOOS-QOL (β = −2.67, p = 0.015), and Marx Activity score (β = −0.54, p = 0.020) (Table 5). When excluding patients who underwent a subsequent revision or contralateral ACL reconstruction from the analysis, the presence of high-grade pre-reconstruction laxity remained predictive of significantly lower 6-year IKDC (β = −1.86, p = 0.021), with a trend toward lower 6-year KOOS-QOL (β = −2.03, p = 0.070) and Marx activity level (β = −0.56, p = 0.077)
Table 5:
Relationships between high-grade pre-reconstruction knee laxity and patient-reported outcomes and activity level at 6 years postoperative
| High-grade laxity | Regression Coefficient (β) |
95% Confidence Interval |
Significance |
|---|---|---|---|
| Subjective IKDC Score | |||
| 3+ Pivot-shift | −1.52 | −3.12 to 0.06 | p = 0.06 |
| Lachman > 10mm | −0.62 | −2.66 to 1.40 | p = 0.54 |
| Anterior Drawer > 10mm | −1.12 | −3.50 to 1.24 | p = 0.35 |
| At least one of the above | −2.26 | −3.77 to −0.75 | p = 0.003 |
| KOOS-QOL | |||
| 3+ Pivot-shift | −1.53 | −3.80 to 0.73 | p = 0.18 |
| Lachman > 10mm | −1.87 | −4.77 to 1.02 | p = 0.20 |
| Anterior Drawer > 10mm | −0.96 | −4.35 to 2.43 | p = 0.58 |
| At least one of the above | −2.67 | −4.81 to −0.53 | p = 0.015 |
| Marx Activity Score | |||
| 3+ Pivot-shift | −0.38 | −0.86 to −0.10 | p = 0.12 |
| Lachman > 10mm | −0.56 | −1.18 to 0.06 | p = 0.077 |
| Anterior Drawer > 10mm | −0.47 | −1.20 to 0.24 | p = 0.20 |
| At least one of the above | −0.54 | −1.00 to − 0.09 | p = 0.02 |
IKDC = International Knee Documentation Committee
KOOS-QOL = Knee injury and Osteoarthritis Outcome Score - Knee-Related Quality of Life
Discussion
The most important finding of this study is that the presence of high-grade pre-operative knee laxity was predictive of significantly increased odds of subsequent revision ACL surgery within 6 years. The presence of high-grade pre-operative Lachman was also predictive of an increased risk of subsequent contralateral ACL reconstruction within 6 years of the initial ACL injury, while a high-grade pivot-shift or anterior drawer demonstrated no such relationship. Previous work has demonstrated high-grade pre-operative laxity to be associated with increased risk of revision ACL reconstruction at 2 years.14
The increased risk of subsequent graft tears and contralateral ACL tears in the high-grade laxity patient population makes this population an important group for further study. An important question when considering the treatment of these patients is whether the increased risk of subsequent injury in the high-grade laxity group is related to knee-specific (injury) factors or patient factors. This study provides insight into this question through the separate analyses of the risk of revision ACL reconstruction and contralateral ACL reconstruction. In this cohort, high-grade pre-reconstruction Lachman was predictive of increased odds of subsequent revision ACL reconstruction and contralateral ACL reconstruction, while high-grade pivot-shift was only predictive of increased odds of revision ACL reconstruction. The finding that high-grade pivot-shift affected the risk of subsequent revision ACL reconstruction but not contralateral ACL reconstruction may indicate that knee specific injury factors are at play. Patients with a high-grade pivot-shift may represent a subset of patients in whom to study the efficacy of double bundle ACL reconstruction or ancillary stabilization procedures that could augment standard intra-articular ACL reconstruction. Some authors have suggested double bundle reconstruction or additional augmentation procedures in such patients to control high-grade laxity may improve outcomes.13, 21 The extra-articular procedures in particular have seen increased interest in recent years25 following widespread discussion of the anatomy and function of the anterolateral ligament complex of the knee,1, 29 but consistent, high-quality data regarding surgical indications and outcomes are still lacking.
In contrast, patients with a high-grade Lachman demonstrated similarly increased odds of both subsequent revision ACL reconstruction and contralateral ACL reconstruction. These relationships may be related to the drivers of high-grade Lachman and pivot-shift findings, including generalized ligamentous laxity and associated injuries. Previous work has demonstrated that generalized joint laxity may be associated with increased risk of ACL injury, particularly in females.20 Recent work has also demonstrated that patients generalized ligamentous laxity as determined by a modified Beighton score had increased risk of both ACL graft and contralateral ACL injury within 6 years of ACL reconstruction.11 Further work is needed to better understand these relationships.
This study also demonstrated a small, but statistically significant negative effect of high-grade pre-operative laxity on patient-reported outcomes 6 years following ACL reconstruction. However, the 2 to 3 point decreases in outcome score do not approach the clinically significant differences established for the subjective IKDC (10 points) and KOOS-QOL scores (8–10 points).31 These difference do represent a change from the 2 year data from this same cohort14 and others3, 7 in which pre-reconstruction laxity had no impact on 2-year patient reported outcome scores. Were this trend to continue with further follow-up, the differences in patient-reported outcomes could become clinically relevant, but the currently exhibited differences are not clinically relevant.
The reason for poorer patient-reported outcomes in the high-grade pre-operative laxity group is not clear. As reported above, this group does include a higher proportion of patients who underwent subsequent revision or contralateral ACL reconstruction, potentially affecting patient-reported outcomes. However, a repeat analysis of patient-reported outcome score that excluded these patients still noted poorer patient-reported outcomes in the high-grade pre-operative laxity group. Another possibility is that patients with high-grade pre-operative laxity are more likely to develop osteoarthritis than those with less laxity. Prior work has demonstrated that the presence of high-grade pre-operative laxity is associated with more chronic ACL tears as well as generalized ligamentous laxity.15 Recent cross-sectional data indicate that generalized ligamentous laxity is associated with increased risk of knee osteoarthritis.5 Six year patient-reported outcome data is likely too early to detect the onset of osteoarthritis in many patients. Longer follow-up and radiographic evaluation is necessary to evaluate the impact of high-grade pre-operative laxity on osteoarthritis risk.
The strengths of this study include a sample size sufficient for performance of a logistic regression analysis and prospective data collection, which resulted in a very complete dataset. The physical examination tests utilized in the study to assess pre-reconstruction laxity are in broad clinical use, making the findings relevant to the day-to-day practice of orthopaedic surgeons, and physical examination was performed under anesthesia in all cases - liming the impact of guarding on resutls. Seventeen different surgeons at multiple sites were involved in data collection, making the resulting data broadly generalizable.
There are limitations inherent to this study that must be considered. Primarily, quantitative instruments were not used to assess pre-reconstruction laxity. Rather, knee laxity was assessed by the treating physician using the IKDC classification system. Previous studies in conscious patients have demonstrated some variability in inter-rater reliability when classifying laxity in ACL deficient knees with this system 9, 10, 23, 30 and variability in the proportions of patients with high-grade pre-operative laxity was noted across surgeons in this study. It is not known whether these differences represent variation among surgeons or differences in their individual patient populations. The fact that the examinations were performed under anesthesia in the current study likely improves reliability introduced by patients’ guarding,26 particularly in regards to the pivot-shift.2 While certainly less quantitative than instrumented assessments of laxity that are sometimes utilized in the research setting, these assessments represent the method of laxity assessment most frequently used by surgeons when they make treatment decisions, making the data quite relevant. The numbers in this study preclude the inclusion of surgeon in the logistic regression models, however, the additional analysis that demonstrated that surgeon was not a significant predictor of revision risk suggests that the relationships between high-grade laxity and outcome identified in this study are driven by true differences in patient knee laxity rather than differences in examination technique by surgeons. A further limitation is the lack of a formal assessment of generalized ligamentous laxity (such as a Beighton score) in this patient population. Such data could provide additional insight into risk factors for graft failure or contralateral ACL injury as discussed above. The use of revision ACL reconstruction as a surrogate for graft failure is a further limitation, and may lead to underestimation of graft failure risk; however, this outcome was selected given its clear nature and an inability to assess all patients via MRI or physical examination to identify graft failures that did not undergo additional reconstructive surgery. An additional limitation is the absence of data regarding persistent knee laxity following ACL reconstruction. Data regarding the persistence of laxity at follow-up could provide insight into the reasons for the increased failure risk in the high-grade laxity population and inform potential treatment options. Finally, graft type was selected by surgeons based on factors not documented in this study. Because some surgeons may have beliefs regarding the performance of certain graft types in patients with high-grade laxity, the distribution of patients with high-grade laxity among graft types may not be consistent. The fact that no significant interactions were noted between graft type and measures of high-grade laxity suggests that the impact of any such differences on the findings of the study is minimal.
Conclusion
High-grade pre-operative knee laxity is predictive of increased odds of revision ACL reconstruction and contralateral ACL reconstruction 6 years following ACL reconstruction. Poorer patient-reported outcome scores in the high-grade laxity group were also noted but the difference did not reach a level of clinical relevance.
What is known about the subject:
High-grade pre-reconstruction laxity is associated with increased revision risk at 2 years following ACL reconstruction
What this study adds to existing knowledge:
High-grade pre-reconstruction Lachman is associated with significantly increased odds of revision and contralateral ACL surgery, while increased pivot-shift is associated only with increased revision ACL risk at 6 years post-operative.
Contributor Information
Robert Magnussen, Department of Orthopaedic Surgery, The Ohio State University Wexner Medical Center, 2835 Fred Taylor Drive, Columbus, OH 43202 USA.
Emily K. Reinke, Sports Medicine, Orthopaedic Surgery Research, Duke University Medical Center, Duke Sports Science Institute, DUMC Box 3615, 3475 Erwin Road, Durham, NC 27705.
Laura J. Huston, Vanderbilt University.
Timothy E. Hewett, Department of Orthopaedic Surgery, Mayo Clinic, Rochester, MN, USA.
Kurt P. Spindler, Department of Orthopaedics, Cleveland Clinic Foundation, 5555 Transportation Blvd. Garfield Heights, OH 44125.
References
- 1.Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. Anatomy of the anterolateral ligament of the knee. J Anat. 2013;223(4):321–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Donaldson WF 3rd, Warren RF, Wickiewicz T. A comparison of acute anterior cruciate ligament examinations. Initial versus examination under anesthesia. Am J Sports Med. 1985;13(1):5–10. [DOI] [PubMed] [Google Scholar]
- 3.Eitzen I, Holm I, Risberg MA. Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br J Sports Med. 2009;43(5):371–376. [DOI] [PubMed] [Google Scholar]
- 4.Galway HR, MacIntosh DL. The lateral pivot shift: a symptom and sign of anterior cruciate ligament insufficiency. Clin Orthop Relat Res. 1980(147):45–50. [PubMed] [Google Scholar]
- 5.Gurer G, Bozbas GT, Tuncer T, Unubol AI, Ucar UG, Memetoglu OI. Frequency of joint hypermobility in Turkish patients with knee osteoarthritis: a cross sectional multicenter study. Int J Rheum Dis. 2016. [DOI] [PubMed] [Google Scholar]
- 6.Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993;1(3–4):226–234. [DOI] [PubMed] [Google Scholar]
- 7.Heijne A, Ang BO, Werner S. Predictive factors for 12-month outcome after anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 2009;19(6):842–849. [DOI] [PubMed] [Google Scholar]
- 8.Irrgang JJ, Anderson AF, Boland AL, et al. Development and validation of the international knee documentation committee subjective knee form. Am J Sports Med. 2001;29(5):600–613. [DOI] [PubMed] [Google Scholar]
- 9.Johnson DS, Ryan WG, Smith RB. Does the Lachman testing method affect the reliability of the International Knee Documentation Committee (IKDC) Form? Knee Surg Sports Traumatol Arthrosc. 2004;12(3):225–228. [DOI] [PubMed] [Google Scholar]
- 10.Lange T, Freiberg A, Droge P, Lutzner J, Schmitt J, Kopkow C. The reliability of physical examination tests for the diagnosis of anterior cruciate ligament rupture--A systematic review. Man Ther. 2015;20(3):402–411. [DOI] [PubMed] [Google Scholar]
- 11.Larson CM, Bedi A, Dietrich ME, et al. Generalized Hypermobility, Knee Hyperextension, and Outcomes After Anterior Cruciate Ligament Reconstruction: Prospective, Case-Control Study With Mean 6 Years Follow-up. Arthroscopy. 2017;33(10):1852–1858. [DOI] [PubMed] [Google Scholar]
- 12.Larson RL. Physical examination in the diagnosis of rotatory instability. Clin Orthop Relat Res. 1983(172):38–44. [PubMed] [Google Scholar]
- 13.Lerat JL, Mandrino A, Besse JL, Moyen B, Brunet-Guedj E. [Effect of external extra-articular ligament plasty on the results of anterior cruciate ligament reconstruction with patellar tendon, a 4 years follow-up]. Rev Chir Orthop Reparatrice Appar Mot. 1997;83(7):591–601. [PubMed] [Google Scholar]
- 14.Magnussen RA, Reinke EK, Huston LJ, Group M, Hewett TE, Spindler KP. Effect of High-Grade Preoperative Knee Laxity on Anterior Cruciate Ligament Reconstruction Outcomes. Am J Sports Med. 2016;44(12):3077–3082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Magnussen RA, Reinke EK, Huston LJ, Group M, Hewett TE, Spindler KP. Factors Associated With High-Grade Lachman, Pivot Shift, and Anterior Drawer at the Time of Anterior Cruciate Ligament Reconstruction. Arthroscopy. 2016;32(6):1080–1085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Malanga GA, Andrus S, Nadler SF, McLean J. Physical examination of the knee: a review of the original test description and scientific validity of common orthopedic tests. Arch Phys Med Rehabil. 2003;84(4):592–603. [DOI] [PubMed] [Google Scholar]
- 17.Marx RG, Connor J, Lyman S, et al. Multirater agreement of arthroscopic grading of knee articular cartilage. Am J Sports Med. 2005;33(11):1654–1657. [DOI] [PubMed] [Google Scholar]
- 18.Marx RG, Stump TJ, Jones EC, Wickiewicz TL, Warren RF. Development and evaluation of an activity rating scale for disorders of the knee. Am J Sports Med. 2001;29(2):213–218. [DOI] [PubMed] [Google Scholar]
- 19.Musahl V, Citak M, O’Loughlin PF, Choi D, Bedi A, Pearle AD. The effect of medial versus lateral meniscectomy on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med. 2010;38(8):1591–1597. [DOI] [PubMed] [Google Scholar]
- 20.Myer GD, Ford KR, Paterno MV, Nick TG, Hewett TE. The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am J Sports Med. 2008;36(6):1073–1080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Noyes FR, Barber SD. The effect of an extra-articular procedure on allograft reconstructions for chronic ruptures of the anterior cruciate ligament. J Bone Joint Surg Am. 1991;73(6):882–892. [PubMed] [Google Scholar]
- 22.Outerbridge RE. The etiology of chondromalacia patellae. 1961. Clin Orthop Relat Res. 2001(389):5–8. [DOI] [PubMed] [Google Scholar]
- 23.Peeler J, Leiter J, MacDonald P. Accuracy and reliability of anterior cruciate ligament clinical examination in a multidisciplinary sports medicine setting. Clin J Sport Med. 2010;20(2):80–85. [DOI] [PubMed] [Google Scholar]
- 24.Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)--development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28(2):88–96. [DOI] [PubMed] [Google Scholar]
- 25.Sonnery-Cottet B, Thaunat M, Freychet B, Pupim BH, Murphy CG, Claes S. Outcome of a Combined Anterior Cruciate Ligament and Anterolateral Ligament Reconstruction Technique With a Minimum 2-Year Follow-up. Am J Sports Med. 2015;43(7):1598–1605. [DOI] [PubMed] [Google Scholar]
- 26.Tanaka M, Vyas D, Moloney G, Bedi A, Pearle AD, Musahl V. What does it take to have a high-grade pivot shift? Knee Surg Sports Traumatol Arthrosc. 2012;20(4):737–742. [DOI] [PubMed] [Google Scholar]
- 27.Terry GC, Norwood LA, Hughston JC, Caldwell KM. How iliotibial tract injuries of the knee combine with acute anterior cruciate ligament tears to influence abnormal anterior tibial displacement. Am J Sports Med. 1993;21(1):55–60. [DOI] [PubMed] [Google Scholar]
- 28.Torg JS, Conrad W, Kalen V. Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med. 1976;4(2):84–93. [DOI] [PubMed] [Google Scholar]
- 29.Vincent JP, Magnussen RA, Gezmez F, et al. The anterolateral ligament of the human knee: An anatomic and histologic study. Knee Surg Sports Traumatol Arthrosc. 2012;20(1):147–152. [DOI] [PubMed] [Google Scholar]
- 30.Wiertsema SH, van Hooff HJ, Migchelsen LA, Steultjens MP. Reliability of the KT1000 arthrometer and the Lachman test in patients with an ACL rupture. Knee. 2008;15(2):107–110. [DOI] [PubMed] [Google Scholar]
- 31.Wright RW. Knee injury outcomes measures. J Am Acad Orthop Surg. 2009;17(1):31–39. [DOI] [PubMed] [Google Scholar]
- 32.Wright RW, Haas AK, Anderson J, et al. Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON Guidelines. Sports Health. 2015;7(3):239–243. [DOI] [PMC free article] [PubMed] [Google Scholar]