

Supplemental Digital Content is available in the text.
Keywords: angioplasty, drug-coated balloons, paclitaxel, peripheral artery disease
Abstract
Background:
While randomized trials have demonstrated the superiority of drug-coated balloon (DCB) angioplasty versus standard percutaneous transluminal angioplasty (PTA) in patients with femoropopliteal peripheral artery disease, the long-term durability of DCB angioplasty remains uncertain.
Methods and Results:
IN.PACT SFA is a prospective, multicenter, randomized single-blinded trial (Randomized Trial of IN.PACT Admiral Paclitaxel-Coated Percutaneous Transluminal Angioplasty [PTA] Balloon Catheter vs Standard PTA for the Treatment of Atherosclerotic Lesions in the Superficial Femoral Artery [SFA] and/or Proximal Popliteal Artery [PPA]) that enrolled 331 subjects with symptomatic (Rutherford 2–4) femoropopliteal lesions. Subjects were randomly assigned 2:1 to the IN.PACT Admiral DCB or PTA. Assessments through 5 years included freedom from clinically driven target lesion revascularization, the primary safety end point, and major adverse events. Through 5 years, patients treated with the IN.PACT Admiral DCB demonstrated a sustained treatment effect with superior freedom from clinically driven target lesion revascularization when compared with PTA (Kaplan-Meier estimate of 74.5% versus 65.3%; log-rank P=0.020). The primary safety composite was achieved in 70.7% of subjects in the DCB and 59.6% in the PTA groups (P=0.068). The major adverse event rate was 42.9% for DCB and 48.1% for PTA (P=0.459). There were no device- or procedure-related deaths in either group as adjudicated by an independent and blinded Clinical Events Committee.
Conclusions:
The IN.PACT SFA randomized trial demonstrates that the IN.PACT Admiral DCB continues to perform better than PTA through 5 years with higher freedom from clinically driven target lesion revascularization. The sustained safety and effectiveness profile of this DCB supports its use as a preferred treatment choice compared with PTA for femoropopliteal lesions.
Clinical Trial Registration:
URL: https://www.clinicaltrials.gov. Unique identifier: NCT01175850 (IN.PACT SFA phase I) and NCT01566461 (IN.PACT SFA phase II).
WHAT IS KNOWN
Compared with percutaneous transluminal angioplasty, treatment with a drug-coated balloon provides superior clinical benefit through early and mid-term follow-up. However, long-term outcomes remain uncertain.
WHAT THE STUDY ADDS
Outcomes from this large randomized trial are the first statistically powered 5-year follow-up data after angioplasty with a drug-coated balloon in patients with femoropopliteal atherosclerotic lesions and demonstrate a lower rate of repeat interventions when compared with percutaneous transluminal angioplasty.
These results provide evidence about the 5-year safety profile of the IN.PACT Admiral drug-coated balloon compared with percutaneous transluminal angioplasty for patients with peripheral artery disease.
See Editorial by Banerjee and Shishehbor
Paclitaxel-based drug-coated balloons (DCB) have shown promise for the treatment of peripheral artery disease (PAD). Several randomized clinical trials have demonstrated superior performance of paclitaxel-based DCBs compared with standard percutaneous transluminal angioplasty (PTA) for femoropopliteal peripheral artery lesions.1–6 A large prospective nonrandomized study has also shown DCB angioplasty to be effective for complex femoropopliteal lesions, including long lesions, chronic total occlusions, and in-stent restenosis.7–10 DCB angioplasty offers the advantage of ease of use, simplicity, and reduction in the need for stenting. There are now 3 DCB platforms approved by the Food and Drug Administration for commercial use in the United States and many more available worldwide.11 Despite the clinical benefits of DCB angioplasty demonstrated in clinical trials, the long-term safety and effectiveness of paclitaxel-coated balloons are unknown. There are no long-term data available beyond 3 years for any of the commercially available DCBs,4 and only one small study has reported 5-year outcomes after DCB angioplasty.12
The IN.PACT SFA trial (Randomized Trial of IN.PACT Admiral Paclitaxel-Coated Percutaneous Transluminal Angioplasty [PTA] Balloon Catheter vs Standard PTA for the Treatment of Atherosclerotic Lesions in the Superficial Femoral Artery [SFA] and/or Proximal Popliteal Artery [PPA]) evaluated the safety and effectiveness of the IN.PACT Admiral DCB (Medtronic, Dublin, Ireland) compared with standard PTA for the treatment of patients with symptomatic femoropopliteal artery disease. Early and mid-term results from the IN.PACT SFA trial demonstrated superior primary patency and a reduction in clinically driven target lesion revascularization (CD-TLR) with DCB compared with PTA.1,2,4 In the current report, we
describe the final 5-year outcomes from the IN.PACT SFA randomized trial.
Methods
The data, analytic methods, and study materials may be made available to other researchers on request from the sponsor.
Study Design
The IN.PACT SFA trial was a prospective, multicenter, multinational, randomized, single-blind trial that was conducted in 2 consecutive phases. Three hundred thirty-one (331) subjects were enrolled between September 2010 and April 2011 (IN.PACT SFA phase I) and between April 2012 and January 2013 (IN.PACT SFA phase II). Eligible subjects were randomized in a 2:1 ratio to treatment with the IN.PACT Admiral DCB (n=220) or PTA (n=111) groups. Details of the IN.PACT SFA trial design and outcomes up to 3 years have been described previously.1,2,4
Subjects were followed for a total of 60 months according to the following schedule: 30 days and 6, 12, 24, 36, 48, and 60 months. Subjects underwent duplex ultrasonography or angiographic evaluations at 30 days and 6, 12, 24, and 36 months. Assessments at 48 and 60 months included the occurrence of reintervention, adverse events, and health status. Informed consent was obtained from all subjects before enrollment. An institutional review board or ethics committee approved all protocols at each trial site. The trial was conducted in accordance with the Declaration of Helsinki, good clinical practice guidelines, and applicable laws as specified by all relevant governmental bodies.
An independent and blinded Clinical Events Committee (CEC; The Baim Institute for Clinical Research, formerly HCRI, Boston, MA) reviewed and adjudicated all major adverse events through the 60-month follow-up period. The CEC included interventional and noninterventional clinicians with pertinent expertise who were not participants in the trial and did not have conflicts of interest. Oversight of clinical sites was provided by an independent data safety monitoring board.
End Points and Definitions
Assessment through 60 months included freedom from CD-TLR, defined as reintervention at the target lesion due to symptoms or a decrease in the ankle-brachial index by ≥20% or >0.15 when compared with post-procedure baseline ankle-brachial index or toe-brachial index, which was allowed in cases of incompressible vessels in the IN.PACT SFA phase II. The composite safety end point was defined as freedom from device- and procedure-related death through 30 days and freedom from target limb major amputation and clinically driven target vessel revascularization (CD-TVR) through 60 months. The rate of major adverse events (a composite of death from any cause, CD-TVR, target limb major amputation, and thrombosis) was evaluated through 60 months. Additional end points included the rate of each individual component of the major adverse event composite. Primary patency, defined as freedom from CD-TLR and freedom from restenosis (duplex ultrasonography peak systolic velocity ratio ≤2.4), was analyzed through 36 months per study protocol.
Statistics
Analyses were based on the intent-to-treat principle. Baseline demographics and clinical characteristics were summarized on a per subject basis; lesion characteristics were summarized on a per lesion basis. For baseline characteristics, continuous variables were described as mean±SD and were compared by Student t tests; dichotomous and categorical variables were described as counts and proportions and were compared by the Fisher exact test or Cochran–Mantel–Haenszel modified ridit scores, respectively. Outcome analyses were performed at a subject level. The Kaplan-Meier method was used to evaluate time to event data for freedom from CD-TLR and freedom from all-cause death through the 60-month follow-up period. The difference in the survival curves between treatment groups was assessed using the log-rank test. For other outcomes, proportion rates were reported, and the Fisher exact test was used to compare between treatment groups for binary outcomes, and the Wilcoxon rank-sum test or Student t test was used for continuous outcomes.
To demonstrate the treatment effects within several selected clinical element subgroups, a forest plot of freedom from CD-TLR through 60 months was prepared.
Statistical analyses were performed using SAS (SAS Institute, NC) version 9.4. The level of statistical significance was set at P<0.05.
Results
In the IN.PACT SFA trial, 331 subjects were randomized to either DCB (n=220) or PTA (n=111). At 60 months follow-up, 155 subjects in the DCB arm and 88 subjects in the PTA arm were eligible for evaluation (Figure 1). The 60-month follow-up compliance rates were 94.8% (147/155) for the DCB group and 96.6% (85/88) for the PTA group. As reported previously,4 demographic, clinical, and lesion characteristics were well matched between treatment groups at baseline (Table I in the Data Supplement). The mean age of subjects in the DCB and PTA groups were 67.5±9.5 and 68.0±9.2 years (P=0.612), respectively. The mean lesion length was 8.9±4.9 cm in the DCB and 8.8±5.1 cm in the PTA groups (P=0.815). Total occlusions were treated in 25.8% and 19.5% (P=0.222) of subjects in the DCB and PTA arms, respectively (Table I in the Data Supplement).
Figure 1.
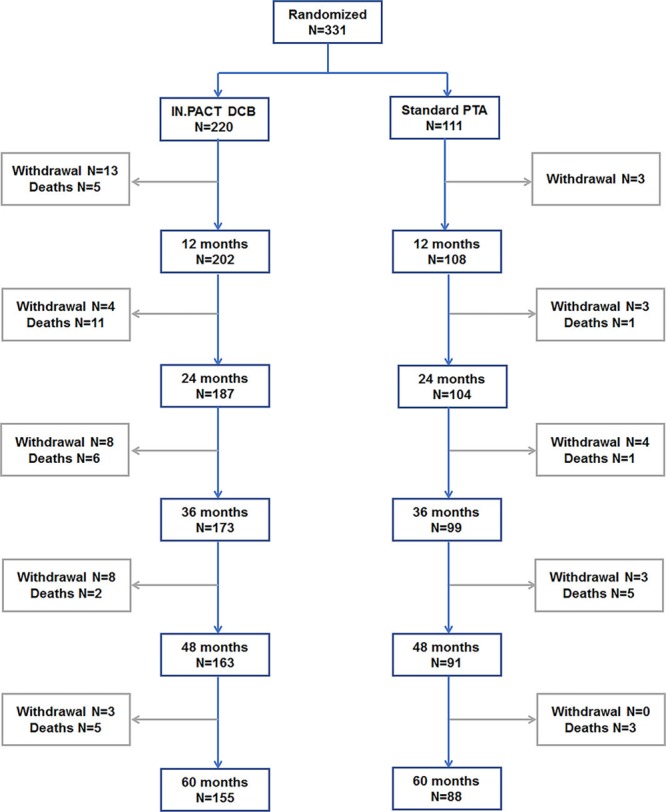
Subject flow chart in the IN.PACT SFA trial though 60 mo. Three hundred thirty-one subjects were randomized 2:1 into groups that received angioplasty with a paclitaxel drug-coated balloon (DCB) or a standard percutaneous transluminal angioplasty (PTA). Subjects were followed for 5 y. IN.PACT SFA indicates Randomized Trial of IN.PACT Admiral Paclitaxel-Coated Percutaneous Transluminal Angioplasty (PTA) Balloon Catheter vs Standard PTA for the Treatment of Atherosclerotic Lesions in the Superficial Femoral Artery (SFA) and/or Proximal Popliteal Artery (PPA).
Effectiveness Outcomes Through 60 Months
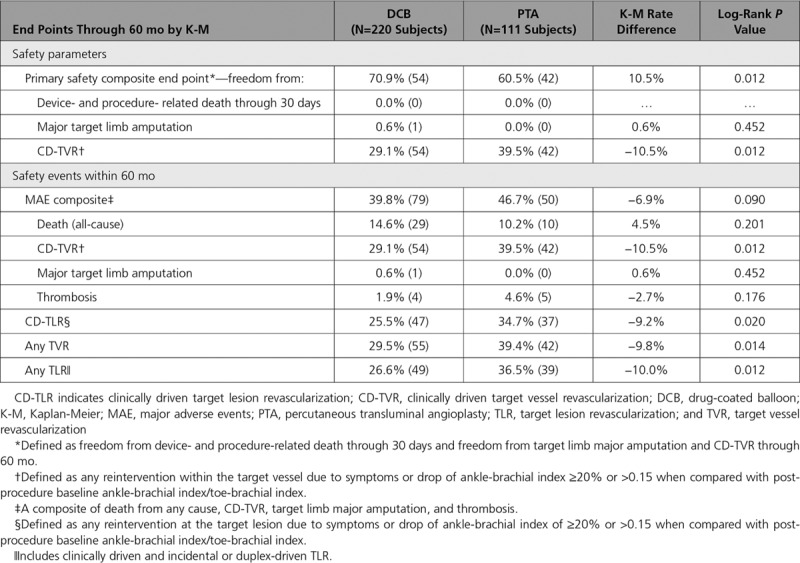
The Kaplan-Meier estimate of freedom from CD-TLR was significantly higher with DCB than PTA (74.5% versus 65.3%; log-rank P=0.020) through 60 months (Figure 2). The proportion rates of CD-TLR observed at 60 months were 25.5% and 35.6% in the DCB and PTA arms, respectively (P=0.080, Table 1). Kaplan-Meier estimates of CD-TLR through 60 months were 25.5% and 34.7% for the DCB and PTA arms, respectively (log-rank P=0.020, Table 2)
Figure 2.
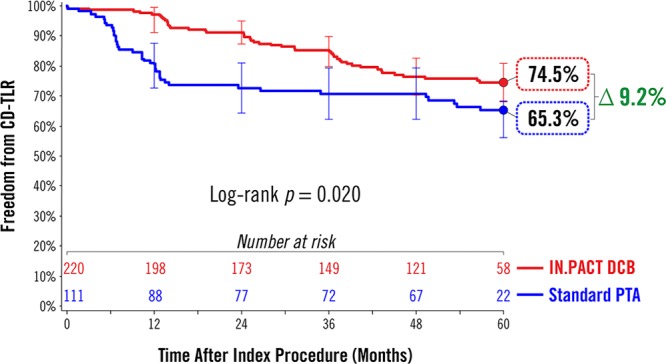
Treatment effect of a drug-coated balloon (DCB) in femoropopliteal lesions at 60 mo. Freedom from clinically driven target lesion revascularization (CD-TLR) by Kaplan-Meier estimate was significantly higher in the DCB group than in the percutaneous transluminal angioplasty (PTA) group (74.5% vs 65.3%; log-rank P=0.020) at 60 mo. Bars represent 95% CI. All target lesion revascularization events were adjudicated by the independent and blinded Clinical Events Committee.
Table 1.
Safety and Effectiveness Results at 60 Months
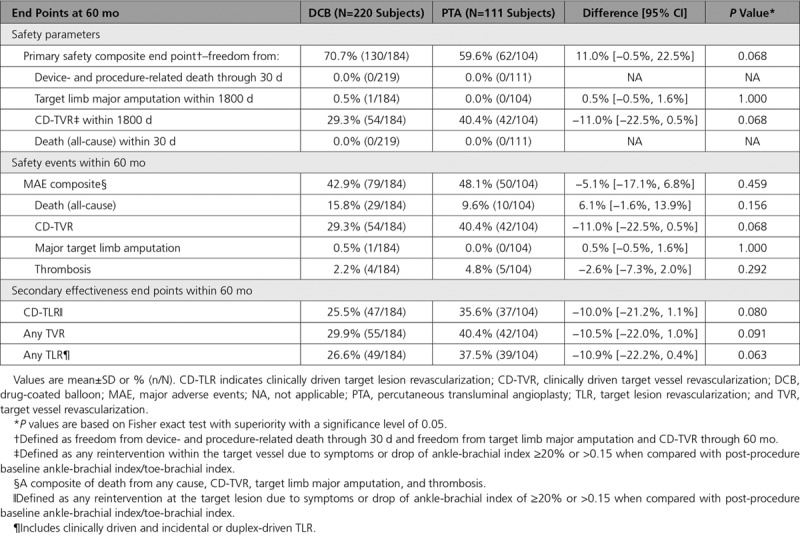
Table 2.
Safety and Effectiveness Results Through 60 Months by Kaplan-Meier Estimate
A post hoc analysis was performed to compare freedom from CD-TLR through 60 months in subgroups defined by the baseline demographic or clinical characteristics (Figure 3). In the nondiabetic subgroup, Kaplan-Meier estimates of freedom from CD-TLR through 60 months were 77.1% for DCB and 66.3% for PTA (log-rank P=0.046), respectively (Figure 3A). In the diabetic subgroup, the Kaplan-Meier estimate of freedom from CD-TLR through 60 months was 70.3% in DCB versus 64.4% in PTA (log-rank P=0.243; Figure 3B).
Figure 3.
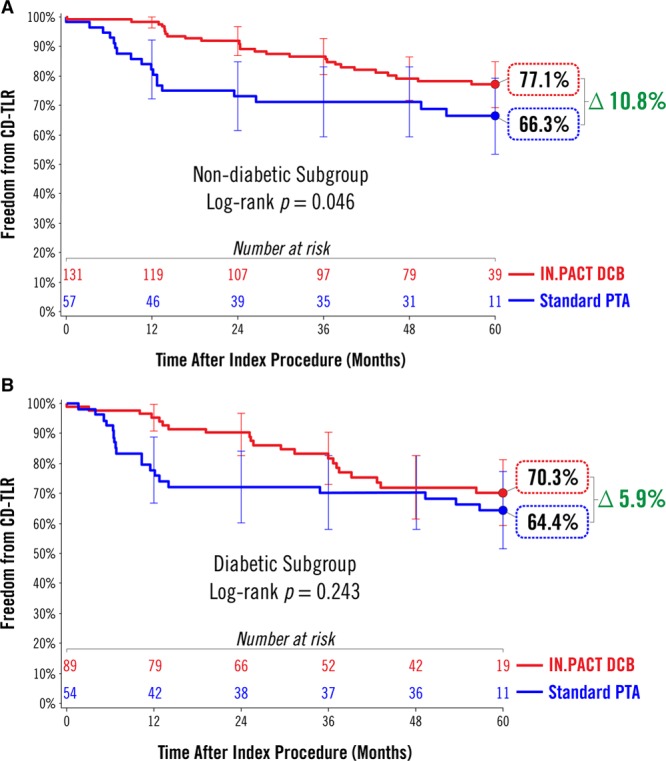
Subgroup analysis of freedom from clinically driven target lesion revascularization (CD-TLR) by Kaplan-Meier estimate at 60 mo. A, Freedom from CD-TLR was significantly higher in the drug-coated balloon (DCB) group than percutaneous transluminal angioplasty (PTA; 77.1% vs 66.3%; P=0.046) in the nondiabetic subgroup. B, Freedom from CD-TLR was numerically higher in the DCB group than PTA but not statistically significant (70.3% vs 64.4%; P=0.243) in the diabetic subgroup. Bars represent 95% CI. All target lesion revascularization events were adjudicated by the independent and blinded Clinical Events Committee.
Post hoc analyses of other subgroup categories are presented in a forest plot (Figure 4). Through 60 months, freedom from CD-TLR favored DCB treatment over PTA across numerous clinical and anatomic subgroups, including Rutherford category 4, patient age ≥75, female sex, lesion length ≥10 cm, and total occlusions.
Figure 4.
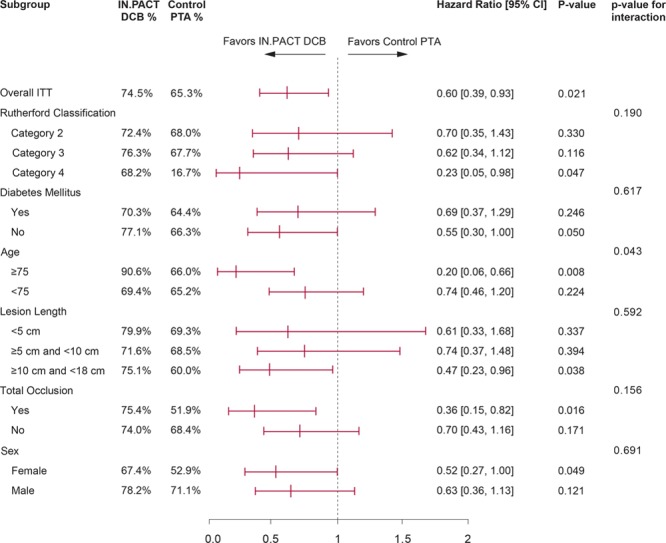
Post hoc analysis of freedom from clinically driven target lesion revascularization (CD-TLR) at 60 mo. Forest plot shows CD-TLR based on Kaplan-Meier estimate in key subgroups at 60 mo. Subjects with Rutherford category 4, nondiabetic, age greater than 75 y, longer lesion length (≥10 cm and ≤18 cm), total occlusion and female sex favored drug-coated ballon (DCB), while both DCB and percutaneous transluminal angioplasty (PTA) performed nonsignificantly in remaining subgroups. P value of hazard ratio between DCB and PTA was calculated using Cox Proportion Hazards model for each subgroup. Treatment-by-subgroup interactions were tested using a Cox proportional hazards model containing the main effects of treatment (IN.PACT DCB and Control PTA), subgroup and the treatment-by-subgroup interaction. ITT indicates intent-to-treat.
Safety Outcomes Through 60 Months
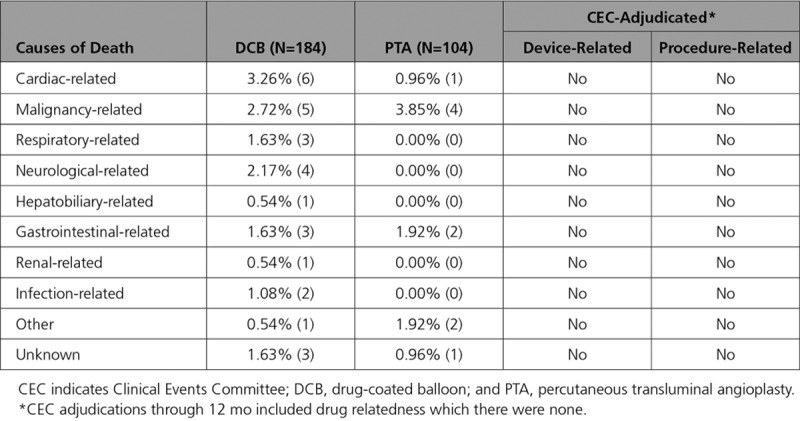
Safety outcomes through 60 months are reported in Tables 1 and 2. The primary safety composite end point within 60 months was achieved in 70.7% (130/184) of subjects in the DCB group and 59.6% (62/104) of subjects in the PTA group (P=0.068). The all-cause mortality rate was 13.5% (39/288) for all subjects and was not significantly different between the DCB arm and the PTA arm (15.8% versus 9.6%; P=0.156, Table 1). These rates were consistent with the Kaplan-Meier estimates of freedom from all-cause death in the DCB and PTA arms (Table 2 and Figure I in the Data Supplement). There was no procedure- or device-related death in this study as adjudicated by the CEC (Table 3). Additional analyses were performed to examine the effect of paclitaxel dose on survival. The results demonstrated that there was no correlation between mean paclitaxel dose and mortality rate (Figures II and III in the Data Supplement). Causes of deaths included cardiac-, malignancy-, neurological-, respiratory-, hepatobiliary-, renal-, infection-, or gastrointestinal-related events, and other/unknown (Table 3).
Table 3.
Causes of Death Through 60 Months
Major adverse events composite rates were 42.9% (79/184) in the DCB group and 48.1% (50/104) in the PTA (P=0.459, Table 1). Vessel thrombosis occurred in 2.2% (4/184) of the patients with DCB and 4.8% (5/104) in the patients with PTA (P=0.292, Table 1). These findings were consistent with Kaplan-Meier estimates (Table 2). One major target limb amputation was reported in the entire IN.PACT SFA trial. A 79-year-old male patient in the DCB group underwent an above-the-knee amputation of the treated limb 3.5 years after DCB for popliteal artery occlusion. He was noted to have restenosis at the popliteal artery site as well as severe lesions in the common femoral artery and SFA. He underwent successful balloon angioplasty of all lesions but developed progressive gangrenous necrosis leading to amputation.
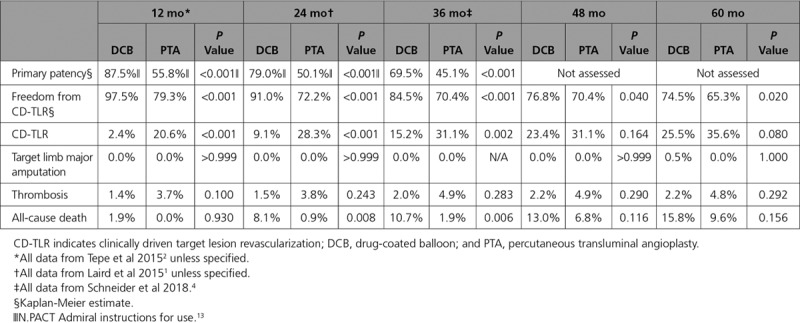
A summary of the safety and effectiveness outcomes through 5 years in the IN.PACT SFA trial1,2,4,13 is reported in Table 4.
Table 4.
Final Report—IN.PACT SFA Trial Through 60 Months
Discussion
In this final report from the IN.PACT SFA randomized trial, a paclitaxel-coated DCB was shown to provide superior outcomes compared with PTA through 5 years in subjects with symptomatic femoropopliteal artery disease. Five-year freedom from CD-TLR was superior following DCB, though the incremental benefit of DCB over PTA has narrowed over time. These results support the hypothesis that short-term exposure to paclitaxel, an antiproliferative drug indicated to inhibit neointimal hyperplasia, provides long-term benefit with regard to avoidance of target lesion revascularization that persists for up to 5 years.
In recent years, there has been tremendous innovation in endovascular therapies for lower extremity PAD, and a wide variety of approaches have been used, including bare-metal stents (BMS), covered stents, atherectomy, drug-eluting stents (DES), and DCB.14,15 Despite this proliferation of endovascular therapies for PAD, there are limited comparative data regarding these devices and only a few randomized studies have reported long-term (5 years) results.12,16–18 There are inherent difficulties in comparing outcomes across device trials, given the differences in study end points, definitions, vascular territories included, patient demographics, and lesion characteristics. Nonetheless, outcomes found in the DCB group of femoropopliteal trials are superior to those reported for PTA and other endovascular interventions in the same vascular bed, and DCB have a Class 1 recommendation per the newly released SCAI Guidelines (The Society for Cardiovascular Angiography and Interventions).14,15,19,20 In the literature, only 2 contemporary endovascular device studies evaluating drug-eluting platforms for the treatment of femoropopliteal artery disease (THUNDER trial [Local Taxane With Short Exposure for Reduction of Restenosis in Distal Arteries] and Zilver PTX Randomized trial [Evaluation of the Zilver PTX Drug-Eluting Stent in the Above-the-Knee Femoropopliteal Artery]) have reported target lesion revascularization (TLR)/freedom from TLR through 5 years.12,16 The 5-year freedom from TLR rate was 79% for a DCB in the THUNDER trial,12 compared with a freedom from CD-TLR rate of 74.5% for the DCB arm in the present study. In the Zilver PTX Randomized trial, the 5-year freedom from TLR was 83.1% for the Zilver PTX DES.16 It should be noted that the mean lesion length in the DCB arm of IN.PACT SFA was 8.9 cm compared with 6.6 cm in the Zilver PTX Randomized trial and 7.4 cm for the DCB arm in THUNDER trial. The slightly higher 5-year freedom from TLR seen with Zilver PTX comes at the cost of a permanent metallic implant and the risk of problematic in-stent restenosis.21,22
Throughout the 5-year follow-up period, all major adverse events, including TLR and TVR, were adjudicated by an independent and blinded CEC in the IN.PACT SFA trial. The results demonstrated a durable safety profile for DCB with low thrombosis rates and only one amputation through 5 years in this PAD population. There was a trend towards a higher number of patients achieving the primary safety composite end point in the DCB arm as compared with PTA. While at 2 and 3 years follow-up there was a significantly higher mortality observed in the DCB arm,1,4 this was no longer statistically significant at 4 and 5 years albeit a numerically higher rate in the DCB group. Causes of death were varied, age-appropriate for this treatment population, and adjudicated by the CEC to not be related to the study device and procedure. A recent summary-level meta-analysis reported an association between paclitaxel devices (DCB and DES) and mortality23; however, 5 more-recent meta-analyses (3 of which include patient-level data) have contradicted these findings.24–28 The supplemental paclitaxel dose analysis results concurred with the latter 5 meta-analyses. There was no correlation between the paclitaxel dose effect on survival status analysis (Figure II in the Data Supplement) or mortality rate across trials with varying mean paclitaxel dosing (Figure III in the Data Supplement).
A post hoc analysis was performed evaluating outcomes in important subgroups (Figure 4). Results in challenging lesions (longer lesions and total occlusion), advanced PAD (Rutherford category 4) or high-risk patients (age older than 75 years) favored DCB over PTA. Of particular interest is the apparent independent relationship between lesion length and CD-TLR through 5 years in subjects treated with DCB, though the small number of subjects means this deserves further study. Recent data from prospective as well as retrospective registries/studies also demonstrated that DCB angioplasty provides consistent clinical benefit in cohorts of long lesions,7,29 in-stent restenosis,8 and other complex lesions.9,30,31 Although only short-term outcomes (1 and 2 years) are available for these registries/studies; these results provide additional evidence that DCB is a viable treatment option for complex lesion/patient cohorts. Previously, we reported a superior treatment effect of DCB in patients with diabetes mellitus as compared with PTA.1 Although freedom from CD-TLR was numerically higher in diabetic patients treated with DCB, there was no statistically significant difference between these 2 treatment groups at 5 years.
In the current study, women treated with DCB had a better outcome as compared with women treated with PTA. A similar result was also observed in the THUNDER trial at 5 years.12 These encouraging findings highlight the promise of DCB for improving outcomes in women with symptomatic femoropopliteal disease, although further study is required.
Limitations
As in any clinical trial, the number of subjects that are available for evaluation is gradually reduced as the length of the follow-up period increases. Subjects were randomized in a 2:1 ratio to the DCB or PTA group resulting in fewer patients in the PTA arm. Another limitation of this study is that core lab-adjudicated duplex ultrasonography assessments were not performed at 4 and 5 years, hence patency rates were reported through 3 years only. The present study was not powered to resolve statistically any differences in mortality between the 2 treatment arms. Finally, the results of this trial were restricted to certain patient populations that would fit the enrollment criteria and cannot be generalized to all patients with femoropopliteal artery disease.
Conclusions
The IN.PACT SFA randomized trial demonstrates that the IN.PACT Admiral DCB continues to perform better than PTA through 5 years with higher freedom from CD-TLR. The sustained safety and effectiveness profile of this DCB supports its use as a preferred treatment choice compared with PTA for femoropopliteal lesions.
Acknowledgments
The IN.PACT SFA investigators would like to recognize and thank the patients who were involved with this clinical study for their participation and contribution. The authors would like to acknowledge the following individuals/team for their contributions: Eric Fernandez, MD and Kathleen Cahill, MS for technical review; Sangeeta Yendrembam, PhD for medical writing assistance; and the IN.PACT SFA clinical team for thorough and meticulous study coordination.
Sources of Funding
The study was supported by Medtronic.
Disclosures
Dr Laird is a consultant and advisory board member for Abbott Vascular, Bard, Boston Scientific, and Medtronic. Dr Schneider is consultant and advisory board member to Medtronic. Dr Jaff is a noncompensated advisor for Abbott Vascular and Boston Scientific; advisor for BiotroniK, Medtronic, Philips, Vactronix, and Vascular Therapies. Dr Brodmann has received speaking honoraria from Bard Peripheral Vascular, Biotronik, Medtronic, Spectranetics, and VIVA Physicians and is a consultant for Bard Peripheral Vascular, Biotronik, Medtronic, and Spectranetics. Dr Zeller has received speaking honoraria from Abbott Vascular, Bard Peripheral Vascular, Biotronik, Boston Scientific Corp, Cook Medical, Cordis Corp, GLG, Gore & Associates, Medtronic, Philips, Spectranetics, Straub Medical, TriReme, Veryan, and VIVA Physicians; is a consultant for Abbott Vascular, Bard Peripheral Vascular, Boston Scientific Corp, Cook Medical, Gore & Associates, Medtronic, and Spectranetics, and his clinic has received study funds or funds for research or clinical trials from 480 Biomedical, Abbott Vascular, B. Braun, Bard Peripheral Vascular, Bayer Pharma, Biotronik, Caveo Med, Contego Medical, Cook Medical, CSI, Gore & Associates, Innova, Intact Vascular, Medtronic, Mercator, Philips, Pluristem, Shockwave, Spectranetics, Terumo, TriReme, and Veryan. Dr Metzger is a proctor for Abbott and Endologix Symposia and received honoraria from Boston Scientific, CSI, Gore and Medtronic. Dr Krishnan is a consultant to Abbott and Medtronic. Dr Scheinert is advisor/consultant for Abbott, Bayer, Boston Scientific, Cook Medical, Cardionovum, CR Bard, Gardia Medical/Allium, Medtronic, Philips, and Upstream Peripheral Technologies. Dr Micari is an advisory board member to Boston Scientific Corp and Medtronic. Dr Wang and M. Masters are full-time employees of Medtronic. Dr Tepe has received research grants from Bard, Biotronik, Boston Scientific, Gore and Medtronic, and is a compensated advisory board member for B Braun and Medtronic.
Supplementary Material
Footnotes
The Data Supplement is available at https://www.ahajournals.org/doi/suppl/10.1161/CIRCINTERVENTIONS.118.007702.
References
- 1.Laird JR, Schneider PA, Tepe G, Brodmann M, Zeller T, Metzger C, Krishnan P, Scheinert D, Micari A, Cohen DJ, Wang H, Hasenbank MS, Jaff MR IN.PACT SFA Trial Investigators. Durability of treatment effect using a drug-coated balloon for femoropopliteal lesions: 24-month results of IN.PACT SFA. J Am Coll Cardiol. 2015;66:2329–2338. doi: 10.1016/j.jacc.2015.09.063. doi: 10.1016/j.jacc.2015.09.063. [DOI] [PubMed] [Google Scholar]
- 2.Tepe G, Laird J, Schneider P, Brodmann M, Krishnan P, Micari A, Metzger C, Scheinert D, Zeller T, Cohen DJ, Snead DB, Alexander B, Landini M, Jaff MR IN.PACT SFA Trial Investigators. Drug-coated balloon versus standard percutaneous transluminal angioplasty for the treatment of superficial femoral and popliteal peripheral artery disease: 12-month results from the IN.PACT SFA randomized trial. Circulation. 2015;131:495–502. doi: 10.1161/CIRCULATIONAHA.114.011004. doi: 10.1161/CIRCULATIONAHA.114.011004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Iida O, Soga Y, Urasawa K, Saito S, Jaff MR, Wang H, Ookubo H, Yokoi H MDT-2113 SFA Japan Investigators. Drug-coated balloon vs standard percutaneous transluminal angioplasty for the treatment of atherosclerotic lesions in the superficial femoral and proximal popliteal arteries: one-year results of the MDT-2113 SFA Japan randomized trial. J Endovasc Ther. 2018;25:109–117. doi: 10.1177/1526602817745565. doi: 10.1177/1526602817745565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schneider PA, Laird JR, Tepe G, Brodmann M, Zeller T, Scheinert D, Metzger C, Micari A, Sachar R, Jaff MR, Wang H, Hasenbank MS, Krishnan P IN.PACT SFA Trial Investigators. Treatment effect of drug-coated balloons is durable to 3 years in the femoropopliteal arteries: long-term results of the IN.PACT SFA randomized trial. Circ Cardiovasc Interv. 2018;11:e005891. doi: 10.1161/CIRCINTERVENTIONS.117.005891. doi: 10.1161/CIRCINTERVENTIONS.117.005891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Krishnan P, Faries P, Niazi K, Jain A, Sachar R, Bachinsky WB, Cardenas J, Werner M, Brodmann M, Mustapha JA, Mena-Hurtado C, Jaff MR, Holden AH, Lyden SP. Stellarex drug-coated balloon for treatment of femoropopliteal disease: twelve-month outcomes from the randomized ILLUMENATE pivotal and pharmacokinetic studies. Circulation. 2017;136:1102–1113. doi: 10.1161/CIRCULATIONAHA.117.028893. doi: 10.1161/CIRCULATIONAHA.117.028893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rosenfield K, Jaff MR, White CJ, Rocha-Singh K, Mena-Hurtado C, Metzger DC, Brodmann M, Pilger E, Zeller T, Krishnan P, Gammon R, Müller-Hülsbeck S, Nehler MR, Benenati JF, Scheinert D LEVANT 2 Investigators. Trial of a paclitaxel-coated balloon for femoropopliteal artery disease. N Engl J Med. 2015;373:145–153. doi: 10.1056/NEJMoa1406235. doi: 10.1056/NEJMoa1406235. [DOI] [PubMed] [Google Scholar]
- 7.Scheinert D, Micari A, Brodmann M, Tepe G, Peeters P, Jaff MR, Wang H, Schmahl R, Zeller T IN.PACT Global Study Investigators. Drug-coated balloon treatment for femoropopliteal artery disease. Circ Cardiovasc Interv. 2018;11:e005654. doi: 10.1161/CIRCINTERVENTIONS.117.005654. doi: 10.1161/CIRCINTERVENTIONS.117.005654. [DOI] [PubMed] [Google Scholar]
- 8.Brodmann M, Keirse K, Scheinert D, Spak L, Jaff MR, Schmahl R, Li P, Zeller T IN.PACT Global Study Investigators. Drug-coated balloon treatment for femoropopliteal artery disease: The IN.PACT Global Study de novo in-stent restenosis imaging cohort. JACC Cardiovasc Interv. 2017;10:2113–2123. doi: 10.1016/j.jcin.2017.06.018. doi: 10.1016/j.jcin.2017.06.018. [DOI] [PubMed] [Google Scholar]
- 9.Ansel GM, Brodmann M, Keirse K, Micari A, Jaff MR, Rocha-Singh K, Fernandez EJ, Wang H, Zeller T IN.PACT Global Study Investigators. Drug-coated balloon treatment of femoropopliteal lesions typically excluded from clinical trials: 12-month findings from the IN.PACT Global Study. J Endovasc Ther. 2018;25:673–682. doi: 10.1177/1526602818803119. doi: 10.1177/1526602818803119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Micari A, Brodmann M, Keirse K, Peeters P, Tepe G, Frost M, Wang H, Zeller T IN.PACT Global Study Investigators. Drug-coated balloon treatment of femoropopliteal lesions for patients with intermittent claudication and ischemic rest pain: 2-year results from the IN.PACT Global Study. JACC Cardiovasc Interv. 2018;11:945–953. doi: 10.1016/j.jcin.2018.02.019. doi: 10.1016/j.jcin.2018.02.019. [DOI] [PubMed] [Google Scholar]
- 11.Kansal A, Long CA, Patel MR, Jones WS. Endovascular treatment of femoro-popliteal lesions. Clin Cardiol. 2019;42:175–183. doi: 10.1002/clc.23098. doi: 10.1002/clc.23098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tepe G, Schnorr B, Albrecht T, Brechtel K, Claussen CD, Scheller B, Speck U, Zeller T. Angioplasty of femoral-popliteal arteries with drug-coated balloons: 5-year follow-up of the THUNDER trial. JACC Cardiovasc Interv. 2015;8(1 pt A):102–108. doi: 10.1016/j.jcin.2014.07.023. doi: 10.1016/j.jcin.2014.07.023. [DOI] [PubMed] [Google Scholar]
- 13.IN.PACT™ Admiral™ Instructions for Use. https://www.accessdata.fda.gov/cdrh_docs/pdf14/P140010S037c.pdf. Accessed January 4, 2019.
- 14.Katsanos K, Spiliopoulos S, Karunanithy N, Krokidis M, Sabharwal T, Taylor P. Bayesian network meta-analysis of nitinol stents, covered stents, drug-eluting stents, and drug-coated balloons in the femoropopliteal artery. J Vasc Surg. 2014;59:1123–1133.e8. doi: 10.1016/j.jvs.2014.01.041. doi: 10.1016/j.jvs.2014.01.041. [DOI] [PubMed] [Google Scholar]
- 15.Jaff MR, Nelson T, Ferko N, Martinson M, Anderson LH, Hollmann S. Endovascular interventions for femoropopliteal peripheral artery disease: a network meta-analysis of current technologies. J Vasc Interv Radiol. 2017;28:1617–1627.e1. doi: 10.1016/j.jvir.2017.08.003. doi: 10.1016/j.jvir.2017.08.003. [DOI] [PubMed] [Google Scholar]
- 16.Dake MD, Ansel GM, Jaff MR, Ohki T, Saxon RR, Smouse HB, Machan LS, Snyder SA, O’Leary EE, Ragheb AO, Zeller T Zilver PTX Investigators. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation. 2016;133:1472–1483. doi: 10.1161/CIRCULATIONAHA.115.016900. discussion 1483. doi: 10.1161/CIRCULATIONAHA.115.016900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shammas NW, Shammas GA, Arikat L, Shammas AN, Darrow A, Banerjee A, Rudy B. Five-year freedom from target-lesion revascularization using excimer laser ablation therapy in the treatment of in-stent restenosis of femoropopliteal arteries. J Invasive Cardiol. 2017;29:207–208. [PubMed] [Google Scholar]
- 18.Kruse RR, Poelmann FB, Doomernik D, Burgerhof HG, Fritschy WM, Moll FL, Reijnen MM. Five-year outcome of self-expanding covered stents for superficial femoral artery occlusive disease and an analysis of factors predicting failure. J Endovasc Ther. 2015;22:855–861. doi: 10.1177/1526602815610583. doi: 10.1177/1526602815610583. [DOI] [PubMed] [Google Scholar]
- 19.Koifman E, Lipinski MJ, Buchanan K, Yu Kang W, Escarcega RO, Waksman R, Bernardo NL. Comparison of treatment strategies for femoro-popliteal disease: a network meta-analysis. Catheter Cardiovasc Interv. 2018;91:1320–1328. doi: 10.1002/ccd.27484. doi: 10.1002/ccd.27484. [DOI] [PubMed] [Google Scholar]
- 20.Feldman DN, Armstrong EJ, Aronow HD, Gigliotti OS, Jaff MR, Klein AJ, Parikh SA, Prasad A, Rosenfield K, Shishehbor MH, Swaminathan RV, White CJ. SCAI consensus guidelines for device selection in femoral-popliteal arterial interventions. Catheter Cardiovasc Interv. 2018;92:124–140. doi: 10.1002/ccd.27635. doi: 10.1002/ccd.27635. [DOI] [PubMed] [Google Scholar]
- 21.Sobieszczyk P. In-stent restenosis after femoropopliteal interventions with drug-eluting stents: same but different? JACC Cardiovasc Interv. 2016;9:835–837. doi: 10.1016/j.jcin.2016.02.015. doi: 10.1016/j.jcin.2016.02.015. [DOI] [PubMed] [Google Scholar]
- 22.Iida O, Takahara M, Soga Y, Hirano K, Yamauchi Y, Zen K, Kawasaki D, Nanto S, Yokoi H, Uematsu M ZEPHYR Investigators. The characteristics of in-stent restenosis after drug-eluting stent implantation in femoropopliteal lesions and 1-year prognosis after repeat endovascular therapy for these lesions. JACC Cardiovasc Interv. 2016;9:828–834. doi: 10.1016/j.jcin.2016.01.007. doi: 10.1016/j.jcin.2016.01.007. [DOI] [PubMed] [Google Scholar]
- 23.Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Karnabatidis D. Risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the leg: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2018;7:e011245. doi: 10.1161/JAHA.118.011245. doi: 10.1161/JAHA.118.011245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Albrecht T, Ukrow A, Werk M, Tepe G, Zeller T, Meyer DR, Kutschera M, Speck U, Waliszewski M. Impact of patient and lesion characteristics on drug-coated balloon angioplasty in the femoropopliteal artery: a pooled analysis of four randomized controlled multicenter trials. Cardiovasc Intervent Radiol. 2019;42:495–504. doi: 10.1007/s00270-018-2137-3. doi: 10.1007/s00270-018-2137-3. [DOI] [PubMed] [Google Scholar]
- 25.Schneider PA, Laird JR, Doros G, Gao Q, Ansel G, Brodmann M, Micari A, Shishehbor MH, Tepe G, Zeller T. Mortality not correlated with paclitaxel exposure: an independent patient-level meta-analysis [published online January 25, 2019]. J Am Coll Cardiol. doi: 10.1016/j.jacc.2019.01.013. doi: 10.1016/j.jacc.2019.01.013. [DOI] [PubMed] [Google Scholar]
- 26.Secemsky EA, Kundi H, Weinberg I, Jaff MR, Krawisz A, Parikh SA, Beckman JA, Mustapha J, Rosenfield K, Yeh RW. Association of survival with femoropopliteal artery revascularization with drug-coated devices [published online February 12, 2019]. JAMA Cardiol. doi: 10.1001/jamacardio.2019.0325. doi: 10.1001/jamacardio.2019.0325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Anantha-Narayanan M, Shah SM, Jelani QU, Garcia S, Ionescu C, Regan C, Mena-Hurtado C. Drug-coated balloon versus plain old balloon angioplasty in femoropopliteal disease: an updated meta-analysis of randomized controlled trials [published online March 6, 2019]. Catheter Cardiovasc Interv. doi: 10.1002/ccd.28176. doi: 10.1002/ccd.28176. [DOI] [PubMed] [Google Scholar]
- 28.Albrecht T, Schnorr B, Kutschera M, Waliszewski MW. Two-year mortality after angioplasty of the femoro-popliteal artery with uncoated balloons and paclitaxel-coated balloons-a pooled analysis of four randomized controlled multicenter trials [published online March 6, 2019]. Cardiovasc Intervent Radiol. doi: 10.1007/s00270-019-02194-w. doi: 10.1007/s00270-019-02194-w. [DOI] [PubMed] [Google Scholar]
- 29.Micari A, Nerla R, Vadalà G, Castriota F, Grattoni C, Liso A, Russo P, Pantaleo P, Roscitano G, Cremonesi A. 2-year results of paclitaxel-coated balloons for long femoropopliteal artery disease: evidence from the SFA-Long Study. JACC Cardiovasc Interv. 2017;10:728–734. doi: 10.1016/j.jcin.2017.01.028. doi: 10.1016/j.jcin.2017.01.028. [DOI] [PubMed] [Google Scholar]
- 30.Schmidt A, Piorkowski M, Görner H, Steiner S, Bausback Y, Scheinert S, Banning-Eichenseer U, Staab H, Branzan D, Varcoe RL, Scheinert D. Drug-coated balloons for complex femoropopliteal lesions: 2-year results of a real-world registry. JACC Cardiovasc Interv. 2016;9:715–724. doi: 10.1016/j.jcin.2015.12.267. doi: 10.1016/j.jcin.2015.12.267. [DOI] [PubMed] [Google Scholar]
- 31.Teymen B, Akturk S, Akturk U, Tdjani M. Comparison of drug-eluting balloon angioplasty with self-expanding interwoven nitinol stent deployment in patients with complex femoropopliteal lesions. Vascular. 2018;26:54–61. doi: 10.1177/1708538117719580. doi: 10.1177/1708538117719580. [DOI] [PubMed] [Google Scholar]