

Abstract
Objective:
To determine the effectiveness of a computer-based intervention designed to increase sit-stand desk usage and help reverse workplace physical inactivity.
Background:
Sit-stand desks have been successful in reducing workplace sedentary behavior, but the challenge remains for an effective method to increase the usage in order to experience the health and productivity benefits.
Method:
Data collection (1-year field study with 194 workers) used a novel method of computer software that continuously recorded objective electric sit-stand desk usage, while taking into account the time a worker spends away from their desk (breaks, meetings). During the baseline period, all workers’ desk usage was recorded by the software, and the intervention period consisted of software reminders and real-time feedback to all workers to change desk positions. Pooled means were calculated to determine desk usage patterns, and effect sizes and pairwise mean differences were analyzed to test for intervention significance.
Results:
The intervention doubled desk usage by increasing ~1 change to ~2 changes per work day. There was a 76% reduction in workers who never used the sit-stand function of the desk. Medium to large effect sizes from the intervention were observed in all three primary outcome measures (desk in sitting/standing position and desk position changes per work day).
Conclusion:
These findings demonstrate an effective intervention that increased postural transitioning and interrupted prolonged inactivity while remaining at the workstation.
Application:
The methods and results in this research study show that we can quantify an increase in desk usage and collect aggregate data continuously.
Keywords: workplace ergonomics, software, workstation, work measurement
Background
Obesity occurs when energy intake is exceeded by energy expenditure (EE; Levine et al., 2005). Physical inactivity can lead to an increased risk of obesity, and levels are classified by the following MET (metabolic equivalent) activity intensity: light (< 3 METs), moderate (3–6 METs), and vigorous (> 6 METs; Blair & Brodney, 1999; Pate et al., 1995). Although recommendations only exist for moderate to vigorous activity (150 min per week), adults are not meeting these recommendations. They also spend increased time in a seated or reclined position at work, known as sedentary behavior (≤ 1.5 METs; McCrady & Levine, 2009; World Health Organization, 2010).
The lack of physical activity at work is an ergonomic and emerging risk. Ergonomic improvements and physical activity at work can prevent neck disorders and reduce the incidence of low back pain (European Agency for Safety and Health at Work, 2005). Prolonged bouts of sitting time (> 20–30 min) are associated with higher levels of fasting insulin and increased risk of type-2 diabetes and are positively correlated with waist circumference and the prevalence of obesity (Gupta et al., 2016; Healy, Matthews, Dunstan, Winkler, & Owen, 2011; Healy et al., 2008). Frequently interrupting prolonged sitting can reduce metabolic risk independent of moderate/vigorous physical activity levels and can improve postprandial glucose metabolism, triglyceride levels, BMI, and waist circumference (Bergouignan et al., 2016; Hamilton, Healy, Dunstan, Zderic, & Owen, 2008; Honda et al., 2016). The EE for a postural transition (sit-to-stand or stand-to-sit) is 35% and 28% higher than that of sitting and standing, respectively (Júdice, Hamilton, Sardinha, Zderic, & Silva, 2016). Additionally, the EE increases for a postural transition as the weight increases (Hatamoto, Yamada, Higaki, & Tanaka, 2016). Thus, increasing postural transitioning may be an important interventional target for overweight or obese individuals who should be increasing their EE.
It has been theorized, in rodent models, that bones sense changes in body mass and as a result, can alter appetite and diet intake to return the body to its previous weight (Jansson et al., 2018). The body’s “gravitostat” is the bones’ sensor that can be triggered by body weight bearing down on bones. During prolonged sitting time, most body weight is supported by seat cushions, which leaves bones unaware of how much weight is being taken on by the bones (Jansson et al., 2018). Therefore, if sitting time can be reduced, bones could have a better sense of body weight and can signal reduced appetite and diet intakes that would result in weight loss. Sit-stand desks have been used to reduce occupational sedentary behavior and improve BMI and productivity (Dutta, Koepp, Stovitz, Levine, & Pereira, 2014; Wendel, Benden, Zhao, & Jeffrey, 2016; Garrett et al., 2016). The intention of the desks is to disrupt prolonged periods of sitting and standing time. Most require worker action to change desk positions. Due to the responsibility placed on the worker to change desk positions, there have been compliance and usage issues, which have led to minimal health and productivity benefits (Wilks, Mortimer, & Nylén, 2006). Health behavior change constructs (self-monitoring and goal setting) have shown to be effective components of promoting physical activity but have yet to be adopted to test effectiveness of sit-stand desks to change behavior (Pearson, 2012).
A statement from Public Health England and the Active Working Community Interest Company says that desk-based workers should aim to “initially progress towards accumulating at least 2 hr/day of standing and light activity during working hours, eventually progressing to a total accumulation of 4 hr/day” (Buckley et al., 2015). To date, there is currently no quantitative study, conducted over time, to determine whether workers are meeting this recommendation. Therefore, the purpose of this study was to determine the effectiveness of a health behavior change intervention designed to increase sit-stand desk usage and help reverse workplace physical inactivity. Continuous, objective data were collected on the time desks were in a sitting and standing position during computer use for 194 workers during a 1-year time period in three naturalistic work settings. Computer reminders were used to increase movement at the workstation.
Method
Participants
Participants were adult workers at a government group in Australia (Comcare) where office work included computer-based tasks and other work (meetings, reading, conference calls). During the 1-year data collection period, 624 workers had recorded data. The eligibility criteria for this secondary analysis was ≥ 20 active computer use (ACU) hr and ≥ 5 work days per worker (equivalent to at least 1 work week) for each of the following time periods: 3 months baseline, first 3 months of the intervention, and the last 3 months of the intervention. These criteria ensured the entire cohort of workers completed the study from the beginning to the end. Out of 624 workers, 194 workers were eligible for this analysis (n =194). From an organizational level, all workers were provided electric sit-stand desks in 2012. Three out of seven office sites nationally (Canberra, Melbourne, and Sydney) were randomly selected to have workers included in this study. Recruitment for this study occurred from a management level. All workers who had a sit-stand desk for at least 1 year were invited to be a part of the study through management meetings. All data were collected through computer software (described later), de-identified by Comcare, and provided to Texas A&M University researchers for secondary analyses. Texas A&M Institutional Review Board approved the secondary analyses protocol, and the workers provided consent to their employer. Due to this secondary analysis, the researchers were not able to obtain demographic information on the workers (age, gender).
Data Collection
The data were collected for a 1-year time period. The study consisted of two phases: baseline (3 months) and intervention (9 months). Prior to the start of the study, each worker’s electric sit-stand desk had a cable (Linak® USB2LIN06 USB connector cable, Linak®, Denmark) that connected the desk to the USB port of the desktop PC connected to their desktop PC. Software (Wellnomics® Sit Stand version 1.0, Wellnomics LTD., New Zealand) was installed on all workers’ desktop PCs. The cables and software were installed for all workers in all three office locations in October 2016. After the installation, each worker placed the desk in a sitting and standing position, based on recommended ergonomic heights (Cook & Burgess-Limerick, 2003), and the software recorded the heights.
The validated sit-stand software worked in conjunction with the cable to record data continuously on the times the desks were in each position (sitting or standing) during active computer use (Blangsted, Hansen, & Jensen, 2004). Inactive computer use was defined as the duration, greater than 30 s, during which there was no keyboard or mouse use. Once the worker resumed any keyboard/mouse activity, active computer use time began and the software recorded the desk position along with the duration the desk was in that position.
For the baseline phase (November 1, 2016, through January 31, 2017), the software was placed into monitor only mode. In monitor only mode, the software recorded continuous data, during active computer use (ACU), for the time desks were in a sitting (Sit-ACU) or standing position (Stand-ACU) and desk position changes per work day. The software informed the workers that the software was placed into monitor only mode.
For the intervention phase (February 1, 2017, through November 24, 2017), the software was placed in software reminders mode, every worker received computer software reminders to change desk positions, and the outcome measures were continuously recorded. For this study, the default setting for the frequency of the reminders was set to 30 min sitting and 20 min standing (ex: after 30 min of Sit-ACU, the worker would receive a reminder to change the desk to a standing position; after 20 min of Stand-ACU, the worker would receive a reminder to change the desk to a sitting position). This default setting was based on musculoskeletal medicine research, which suggests postural transitions every 20–30 min, as well as evidence showing that interrupting long bouts of sitting time (> 30 min) provides metabolic benefits (Atlas & Deyo, 2001; Dunstan et al., 2012; Gallagher, Campbell, & Callaghan, 2014; Ryan, Dall, Granat, & Grant, 2011).
During the intervention, a reminder arrow (pointed up or down based on their current desk position) to change desk positions appeared on the workers’ computer monitor displays. The workers had the option to change their desk position, postpone the reminders, or ignore them. Workers could change the frequency of the reminders or choose to not receive any computer reminders. Further, they could interact with the prompt, as it provided real-time statistics in order to monitor individual progress for that day, week, or month. The prompt displayed the following metrics: stand-ACU, the percentage of the desk was in a standing position, and average number of desk position changes per work day. The primary outcome measures for this study were sit/stand-ACU and desk position changes per work day.
Analysis
The analysis was conducted using SPSS 22 (IBM SPSS Statistics). Pairwise comparisons analysis was conducted to determine the mean differences between baseline and the intervention using means, SD, and histograms. We tested for significance of the intervention using effect size (using Cohen’s d), paired two sample for means t test (ACU and Sit/Stand ACU) and nonparametric tests using the Wilcoxon signed-rank test (desk position changes per hour and work day). The overall pooled means were calculated for every month of data collection period to determine usage patterns before and after the intervention. Due to 1 week of company holiday period in December, any data during this time period was excluded from this secondary analysis. The linear relationship and slope were calculated using the pairwise mean differences of each outcome measure with relevance to computer usage to determine the changes made from the intervention.
Results
For the baseline phase, the 194 workers had an average of 163 ACU hr and 40 work days recorded per worker. For the intervention phase, the average data recorded was 637 ACU hr and 159 work days per worker. Pairwise comparisons of difference in outcome measure means are shown in Table 1. All three primary outcome measures had a significant change (p < .05) from baseline to intervention, with medium to large effect sizes (Cohen’s d) observed in each outcome (Sit-ACU: 0.48, Stand-ACU: 0.41, Desk position changes per work day: 0.68).
Table 1:
Overall Group Means and Pairwise Comparisons From Baseline to Intervention Pooled Across 1 Year
| Variable | Baseline M (SD) | Intervention M (SD) | Pairwise M difference (SD) | Effect size (Cohen’s d) |
|---|---|---|---|---|
| ACU | 4.03 (0.93) hrs | 3.87 (0.86) hrs | −0.16 (0.61) hr | |
| Sit-ACU | 3.61 (1.14) hrs | 3.27 (0.97) hrs | −0.34* (0.71) hr | 0.48 |
| Stand-ACU | 0.42 (0.72) hr | 0.60 (0.68) hr | 0.18* (0.44) hr | 0.41 |
| Desk position changes per work day** | 1.04 (1.54)changes | 2.31 (2.37) changes | 1.27* (1.88) changes | 0.68 |
p < .05.
Wilcoxon signed rank test.
Figure 1 illustrates the effect from baseline to intervention for every month of the study. From the baseline phase compared with the end of the study, all outcome measures increased, indicating the intervention was successful.
Figure 1.
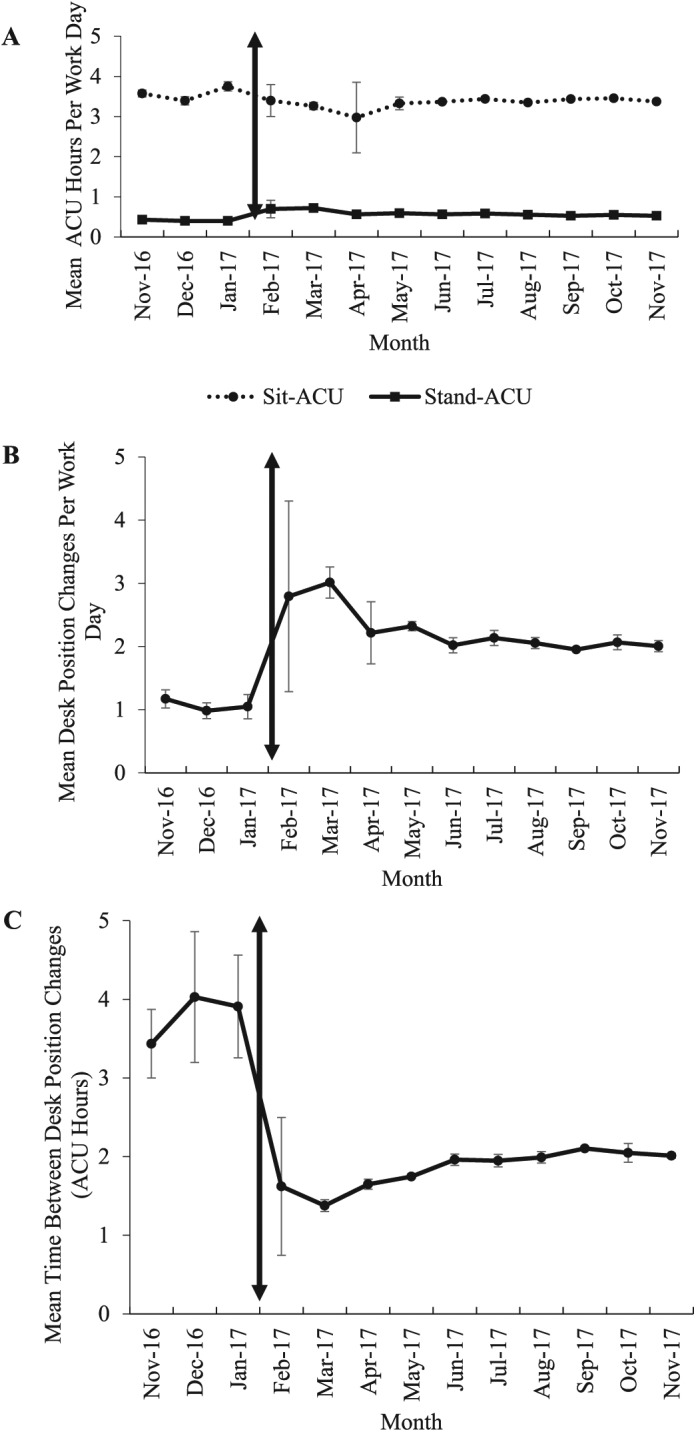
Overall pooled outcome measure means for all workers by each month. The double-arrowed vertical line represents the start of the intervention. Means of Sit/Stand-ACU (A), Desk position changes per work day (B), and Time between desk position changes (C) show health behavior change for each outcome measure. Data from company holiday period (January 1, 2017–January 7, 2017) was excluded for these graphs. Error bars indicate 95% confidence intervals.
A significant linear relationship was observed with the pairwise mean differences for the duration of computer usage (2, 3, 4, 5 mean ACU hr per work day) for all three outcome measures (Sit-ACU: slope = −0.37, p < .0001, Stand-ACU: slope = 0.09, p < .05, Desk position changes per work day: slope 0.33, p < .05). The largest increases in Sit- and Stand-ACU were seen in the workers who used the computer, on average, for 5 hr/work day (39 min reduced and 25 min increased, respectively). The largest increases for desk position changes per work day were seen by the workers who used the computer, on average, for 5 hr/work day (increased by 2.56 desk position changes).
The frequency of desk position changes per work day increased for workers from the baseline to the intervention (Figure 2). The largest subpopulation of workers with increases comprised those who had a mean of ≥ 3 desk position changes per work day. Out of 194 workers, these group of 20 workers (baseline) increased to 83 workers (intervention), or a 330% increase in workers who completed ≥ 3 desk position changes per work day. Another significant measure was the workers who never made any desk position changes. From the baseline to the intervention phase, this group of 33 workers reduced to only seven workers, which is equivalent to a 76% decrease in workers who never made any desk position changes. Further, the overall average desk position compliance (rate at which workers would change their desk position when provided a software reminder) was 61%.
Figure 2.
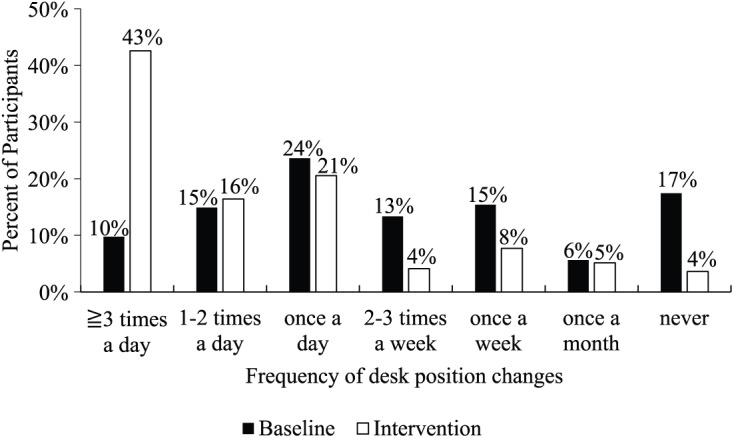
Frequency of desk position changes for all workers from baseline to intervention.
The time desks were in a sitting or standing position was related to the ACU time. As a result, it is important to look at the Sit/Stand-ACU as a percent of computer use (Figure 3). For the baseline phase, 26% of the workers never had their desk in a standing position. After the intervention, this was reduced to only 9% of the workers, indicating that the software reminders made workers use their desk in the standing position more often.
Figure 3.
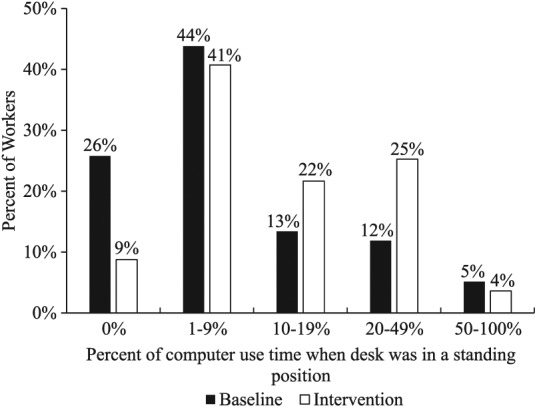
The percent of workers based on the percent of computer use time when the desks were in a standing position.
Discussion
The computer-based behavioral intervention was effective at increasing sit-stand desk utilization. To date, studies using sit-stand desks with computer reminders have met the primary intention of reducing sitting time while increasing standing time and position changes with office workers (Barbieri et al., 2017; Donath, Faude, Schefer, Roth, & Zahner, 2015; Evans et al., 2012; Swartz et al., 2014). However, these short-term studies have not taken into account the time individuals are absent from the workstation (meetings, breaks, lunch). This study was able to account for time spent only at the workstation, which is an important factor when determining the effect of a physical activity intervention designed for sit-stand desks. Additionally, this is the first study to collect continuous and objective sit-stand desk usage data while engaging workers with their habits for a 1-year time period. The intervention accomplished this goal without requiring workers to leave their desk or wear sensors. This is important to note when designing a long-term, sustainable method that can be used in a naturalistic work environment. Therefore, the results from this study provide a novel, effective behavioral intervention toward monitoring and reversing worker physical inactivity.
Overall, the workers reduced their proportion of desk sitting time (90% to 82%) and increased their desk standing time (10% to 18%). Approximately one fourth of the workers never had their desk in a standing position during computer use during the baseline period. After the intervention, only 9% of the workers were left in this category. The findings from each outcome measure were statistically significant (p < .05) with medium to large effect sizes, revealing that this intervention had a positive impact on addressing the workers’ sedentary behavior. Further, the workers increased their sit-to-stand desk transition frequency with the help of the software reminders. During the baseline phase, the workers averaged ~1 desk position change per work day. After the intervention, the workers averaged ~2 changes per work day. Likewise, the average time a desk was in a position before a change significantly reduced from ~3.79 to 1.85 hrs (51% reduction).
There was a significant relationship with the changes made on all three outcome measures in relation to computer use. The workers who spent a longer time using the computer (5 hr/day) made the largest increases in desk sitting/standing time and desk changes per work day. This finding shows that higher duration computer users have the ability to show the greatest changes in their desk usage habits and responded well to the behavioral intervention. Given that breaking up prolonged bouts of being in the same position and postural transitioning have a greater energy expenditure than sitting/standing, the data from the intervention could be used to target subpopulations (overweight/obese individuals, high-duration computer users) who need to increase their movement throughout the work day (Júdice et al., 2016).
In order to engage workers with their health behavior change, the software interface provided each worker real-time feedback on their desk usage (self-monitoring) and the option to change the frequency of the reminders (goal setting). For this study, we used a reminder default setting of 20 min standing for every 30 min sitting, based on previous research recommendations (Atlas & Deyo, 2001; Dunstan et al., 2012; Gallagher et al., 2014; Ryan et al., 2011). The ratio of sit-to-stand time can vary based on occupational settings and work tasks. For example, workers who spend less time at their workstation may have a different compliance level with the reminders. The compliance to default settings should be evaluated on different types of office workers. Aggressive strategies to increase the frequency of changing position reminders could be used as an approach by upper management to motivate teams of employees by setting organizational desk usage goals.
Based on monthly observations for the 1-year time period, the intervention was most effective for the first ~3 months. A longitudinal, randomized study should be conducted to add more health behavior change constructs after a 3-month period to see whether effects can be sustained beyond 3 months. Gamification elements (weekly reports/leaderboards, reward points, badges) may be an option in some workplaces to motivate workers to remain engaged with their physical activity health behavior change (Paredes, Tewrai, & Canny, 2013). A final key takeaway for employers from this research was that no change was detected in active computer time after the successful sedentary behavior intervention. Future studies may evaluate quality of work output in addition to using this new time measure.
Limitations and Strengths
A study strength was the inclusion requirement of steady-state sit-stand desk users (had desk for ≥ 1 year). Therefore, the study design was not affected by an adoption phase for the desks. Second, the organization provided desks to the office sites 4 years prior to the study, which eliminates the possibility of volunteerism bias. A limitation was all workers in this study were previously using a stretch-break software (Wellnomics® Workpace®) that would remind them to take a break from their workstation (i.e., walk around the floor, stretch break, take a flight of stairs). Because workers had a previous exposure to computer software that prompted them to take a break, their acceptance to comply with this computer-based intervention could vary. It is important to address that due to security concerns, the software had to be approved by the government group’s information technology department. This process took several steps until final approval was given. Even though the process for approval was extensive and challenging, this software, as a data collection method, is better for long-term, large-scale research and requires low maintenance/costs. For future research, conducting similar behavioral interventions could cause new risks to arise or other risks present in the workplace could increase.
Blind studies involving interventions may be ideal, but it is impossible to hide a standing desk versus a seated desk from a worker. Furthermore, while we preferred a control group continue without software intervention, the company would not allow anyone to be without the intervention, so the rollout of a perceived benefit had to be for all employees at the same time. This brings up two clear examples of how in situ studies stray from theoretical experimental design goals. The authors believe the robustness of the conclusions in this case far exceed the limitations posed by employers when interacting with real workers in genuine work situations.
Conclusion
These findings reveal an effective intervention using computer technology combined with electric sit-stand desks that will increase movement during the workday. Because we can now quantify and increase postural transitioning and desk usage (continuously), future research should use this health behavior intervention to study the effect of increased workday movement on biomarkers, diet intake, and employee health costs/injury data. With the methods and results from this research, we can identify and target high-risk individuals to change their health behaviors.
Key Points
● We were able to account for time when a worker steps away from their workstation for job tasks (meeting, breaks, etc.) and record data based on the presence of a worker at their desk.
● With these research findings, we can now use this sustainable intervention to help high-risk, sedentary workers (obese/overweight, high computer use) who should be increasing their energy expenditure by using the methods and behavioral intervention from this study in order to change their health behaviors.
● We can now quantify increased electric sit-stand desk usage, which in turn will help us structure future research studies to understand the effect of the desks on biomarkers and workplace health.
Acknowledgments
This project was funded in part by the Office Ergonomics Research Committee Grant M1501491, Linak, and Wellnomics LTD.
Biography
Pankaj Parag Sharma received his DrPH in epidemiology & environmental health from Texas A&M University School of Public Health in 2018.
Ranjana K. Mehta is an assistant professor in the Industrial and Systems Engineering department at Texas A&M University in College Station. She received her PhD in industrial and systems engineering from Virginia Tech in 2011.
Adam Pickens is an assistant professor in the Department of Environmental & Occupational Health at Texas A&M University, School of Public Health in College Station. He received his PhD in industrial engineering from Texas Tech University in 2006.
Gang Han is an associate professor in the Department of Epidemiology and Biostatistics at Texas A&M University, School of Public Health in College Station. He received his PhD in statistics from Ohio State University in 2005.
Mark Benden is the department head and an associate professor in the Department of Environmental & Occupational Health at Texas A&M University, School of Public Health in College Station. He received his PhD in Interdisciplinary Engineering from Texas A&M University in 2005.
Footnotes
ORCID iD: Pankaj Parag Sharma  https://orcid.org/0000-0003-4528-8610
https://orcid.org/0000-0003-4528-8610
References
- Atlas S. J., Deyo R. A. (2001). Evaluating and managing acute low back pain in the primary care setting. Journal of General Internal Medicine, 16(2), 120–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barbieri D. F., Mathiassen S. E., Srinivasan D., Dos Santos W. M., Inoue R. S., Siqueira A. A. G., . . .Oliveira A. B. (2017). Sit–stand tables with semi-automated position changes: A new interactive approach for reducing sitting in office work. IISE Transactions on Occupational Ergonomics and Human Factors, 5(1), 39–46. [Google Scholar]
- Bergouignan A., Latouche C., Heywood S., Grace M. S., Reddy-Luthmoodoo M., Natoli A. K., . . .Kingwell B. A. (2016). Frequent interruptions of sedentary time modulates contraction- and insulin-stimulated glucose uptake pathways in muscle: Ancillary analysis from randomized clinical trials. Scientific Reports, 6, 32044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blair S. N., Brodney S. (1999). Effects of physical inactivity and obesity on morbidity and mortality: Current evidence and research issues. Medicine and Science in Sports and Exercise, 31, S646–S662. [DOI] [PubMed] [Google Scholar]
- Blangsted A. K., Hansen K., Jensen C. (2004). Validation of a commercial software package for quantification of computer use. International Journal of Industrial Ergonomics, 34(3), 237–241. [Google Scholar]
- Buckley J. P., Hedge A., Yates T., Copeland R. J., Loosemore M., Hamer M., . . .Dunstan D. W. (2015). The sedentary office: A growing case for change towards better health and productivity. Expert statement commissioned by Public Health England and the Active Working Community Interest Company. British Journal of Sports Medicine. doi: 10.1136/bjsports-2015-094618 [DOI] [PubMed] [Google Scholar]
- Cook C., Burgess-Limerick R. (2003). Guidelines for computer workstations. Ergonomics Australia, 17(1), 19–37. [Google Scholar]
- Donath L., Faude O., Schefer Y., Roth R., Zahner L. (2015). Repetitive daily point of choice prompts and occupational sit-stand transfers, concentration and neuromuscular performance in office workers: An RCT. International Journal of Environmental Research and Public Health, 12(4), 4340–4353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunstan D. W., Kingwell B. A., Larsen R., Healy G. N., Cerin E., Hamilton M. T., . . .Owen N. (2012). Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care, 35(5), 976–983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dutta N., Koepp G. A., Stovitz S. D., Levine J. A., Pereira M. A. (2014). Using sit-stand workstations to decrease sedentary time in office workers: A randomized crossover trial. International Journal of Environmental Research and Public Health, 11(7), 6653–6665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- European Agency for Safety and Health at Work. (2005). Report: Expert forecast on emerging physical risks related to occupational safety and health. Luxembourg: Office for Official Publications of the European Communities. [Google Scholar]
- Evans R. E., Fawole H. O., Sheriff S. A., Dall P. M., Grant P. M., Ryan C. G. (2012). Point-of-choice prompts to reduce sitting time at work: A randomized trial. American Journal of Preventive Medicine, 43(3), 293–297. [DOI] [PubMed] [Google Scholar]
- Gallagher K. M., Campbell T., Callaghan J. P. (2014). The influence of a seated break on prolonged standing induced low back pain development. Ergonomics, 57(4), 555–562. [DOI] [PubMed] [Google Scholar]
- Garrett G., Benden M., Mehta R., Pickens A., Peres S. C., Zhao H. (2016). Call center productivity over 6 months following a standing desk intervention. IIE Transactions on Occupational Ergonomics and Human Factors, 4(2–3), 188–195. [Google Scholar]
- Gupta N., Hallman D. M., Mathiassen S. E., Aadahl M., Jørgensen M. B., Holtermann A. (2016). Are temporal patterns of sitting associated with obesity among blue-collar workers? A cross sectional study using accelerometers. BMC Public Health, 16(1), 148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamilton M. T., Healy G. N., Dunstan D. W., Zderic T. W., Owen N. (2008). Too little exercise and too much sitting: Inactivity physiology and the need for new recommendations on sedentary behavior. Current Cardiovascular Risk Reports, 2(4), 292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatamoto Y., Yamada Y., Higaki Y., Tanaka H. (2016). A novel approach for measuring energy expenditure of a single sit-to-stand movement. European Journal of Applied Physiology, 116(5), 997–1004. [DOI] [PubMed] [Google Scholar]
- Healy G. N., Dunstan D. W., Salmon J., Cerin E., Shaw J. E., Zimmet P. Z., Owen N. (2008). Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care, 31(4), 661–666. [DOI] [PubMed] [Google Scholar]
- Healy G. N., Matthews C. E., Dunstan D. W., Winkler E. A., Owen N. (2011). Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 2003–06. European Heart Journal, 32(5), 590–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Honda T., Chen S., Yonemoto K., Kishimoto H., Chen T., Narazaki K., . . .Kumagai S. (2016). Sedentary bout durations and metabolic syndrome among working adults: A prospective cohort study. BMC Public Health, 16(1), 888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansson J. O., Palsdottir V., Hägg D. A., Schéle E., Dickson S. L., Anesten F., . . .Cone R. D. (2018). Body weight homeostat that regulates fat mass independently of leptin in rats and mice. Proceedings of the National Academy of Sciences, 115(2), 427–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Júdice P. B., Hamilton M. T., Sardinha L. B., Zderic T. W., Silva A. M. (2016). What is the metabolic and energy cost of sitting, standing and sit/stand transitions? European Journal of Applied Physiology, 116(2), 263–273. [DOI] [PubMed] [Google Scholar]
- Levine J. A., Lanningham-Foster L. M., McCrady S. K., Krizan A. C., Olson L. R., Kane P. H., . . .Clark M. M. (2005). Interindividual variation in posture allocation: Possible role in human obesity. Science, 307(5709), 584–586. [DOI] [PubMed] [Google Scholar]
- McCrady S. K., Levine J. A. (2009). Sedentariness at work: How much do we really sit? Obesity, 17(11), 2103–2105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paredes P., Tewari A., Canny J. (2013). Design principles for the conceptualization of games for health behavior change. CHI 2013, Paris. [Google Scholar]
- Pate R. R., Pratt M., Blair S. N., Haskell W. L., Macera C. A., Bouchard C., . . .Kriska A. (1995). Physical activity and public health: A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA, 273(5), 402–407. [DOI] [PubMed] [Google Scholar]
- Pearson E. S. (2012). Goal setting as a health behavior change strategy in overweight and obese adults: A systematic literature review examining intervention components. Patient Education and Counseling, 87(1), 32–42. [DOI] [PubMed] [Google Scholar]
- Ryan C. G., Dall P. M., Granat M. H., Grant P. M. (2011). Sitting patterns at work: Objective measurement of adherence to current recommendations. Ergonomics, 54(6), 531–538. [Google Scholar]
- Swartz A. M., Rote A. E., Welch W. A., Maeda H., Hart T. L., Cho Y. I., Strath S. J. (2014). Prompts to disrupt sitting time and increase physical activity at work, 2011–2012. Preventing Chronic Disease, 11, E73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wendel M. L., Benden M. E., Zhao H., Jeffrey C. (2016). Stand-biased versus seated classrooms and childhood obesity: A randomized experiment in Texas. American Journal of Public Health, 106(10), 1849–1854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilks S., Mortimer M., Nylén P. (2006). The introduction of sit–stand worktables: Aspects of attitudes, compliance and satisfaction. Applied Ergonomics, 37(3), 359–365. [DOI] [PubMed] [Google Scholar]
- World Health Organization. (2010). Global recommended levels of physical activity adults.