

Abstract
Objectives:
The aim of this study was to evaluate the most commonly used body composition tools in clinical practice, such as anthropometry and electrical bioimpedance, and compare it with deuterium oxide.
Methods:
An exploratory cross-sectional study was conducted on women aged 100 years or above at home. Body composition was determined by measuring skinfolds (Jackson and Pollock and Durnin and Womersley equations), by bioimpedance, and by the deuterium oxide method.
Results:
Body mass index values were lower than 22 kg/m2 in 64% of the subjects. When the various methods used were compared with deuterium oxide, there was better agreement for the determination of fat mass than lean mass. For fat mass, agreement was better when using bioimpedance (Lin’s coefficient = 0.70), whereas for lean mass, agreement was better using the Durnin and Womersley equation (Lin’s coefficient = 0.51).
Conclusion:
It is possible to use bioimpedance and skinfolds to evaluate fat mass and lean mass, respectively, in centenarians.
Keywords: Centenarians, body composition, women, deuterium oxide, aging
Introduction
Demographic aging has been the topic of several studies because of its impact on various aspects of today’s society. From the standpoint of the Health Sciences, there is a strong relationship between healthy life habits, diet, active social life, and the practice of regular physical activity with a successful aging process.1
Despite the worldwide aging of the population, the prevalence of centenarians is very low (approximately 1 in 10,000 persons) and, consequently, the traditional population sampling methods are difficult to apply in the study of centenarians and are inviable for the obtention of large samples.2
Survival during extremely advanced age is more influenced by variables related to functional and nutritional status than by variables representing risk factors for age-associated chronic diseases.3 Centenarians are a poorly studied population group. Understanding the changes in body composition associated with aging and their effects is extremely important for the healthcare and nutritional support of the older population.4
With the increase in the number of older people and, consequently, centenarians, the search for methods that can identify changes in body composition in a practical and easy way in clinical practice is fundamental.5 We know that the methods presently available are imprecise and have both advantages and disadvantages. In centenarians, this may be even more critical, as there are no adequate references for this age group.
Several methods are available for the assessment of body composition; among them, deuterium oxide dilution is highly accurate and precise and is considered to be the gold standard for the determination of total body water. In addition, it is minimally invasive and can be used in any clinical situation.6 Dual X-ray absorptiometry (DXA) assessment is considered to be a reference method for the evaluation of body composition.7 However, it is often difficult to take centenarians to the reference center for the realization of the DXA, due to difficulties of locomotion.
Bioelectrical impedance analysis (BIA) is a widely used method, but it has limitations related to quantification of total body water.5 BIA overestimates lean mass (LM)8 and underestimates fat mass (FM) in lean subjects.
In view of the above considerations, the objective of this study was to assess the body composition of centenarian women using deuterium oxide dilution and to compare the results with those obtained by more easily accessible and low-cost methods as anthropometry and BIA. The hypothesis was that these simpler methods would be accurate and therefore useful for clinical practice in this special population.
Methods and materials
An exploratory cross-sectional study was conducted on centenarian women residing in a medium-sized city in Brazil (Ribeirão Preto, State of São Paulo). The study was approved by the local Research Ethics Committee (HCFMRP USP) on 9 April 2012 (protocol no. 9032012).
Inclusion and exclusion criteria
The centenarians were selected using the database of the Health Secretary Office of the Municipality of the city. The families were first contacted by telephone in order to authorize and schedule a home visit. The criteria for inclusion were being 100 years old or above and living in the city of Ribeirão Preto. The age was proven by the presentation of a birth or marriage certificate or general registration. The subjects were assessed at home in view of restricted mobility being present in many cases. All subjects and/or the persons responsible for them gave written informed consent to participate in the study. Some study subjects had no decisional capacity to provide informed consent because of very low cognitive status (eight women with advanced dementia). In those cases, the persons responsible for them agreed to their participation and this option was authorized by the Research Ethics Committee. Centenarians with acute diseases within 30 days before the clinical evaluation were excluded from the study. The clinical evaluation was performed by a geriatrician.
A convenience sample was used, since the goal was to study as many centenarian women as possible. The study involved a representative sample of the centenarians residing in a city with about 600,000 inhabitants (24 of the 58 identified in the 2010 census, 7.2% of the individuals aged 65 years or above9).
Anthropometry
The following anthropometric measurements were obtained: weight, height, waist circumference (WC), hip circumference (HC), calf circumference (CC), and arm circumference (AC) of the dominant arm.
For weight determination, the subjects were instructed to wear light clothing and no shoes and were examined preferably under fasting conditions and with an empty bladder (in the morning). A digital scale with a capacity of 180 kg (Model Glass 3; G-Tech, Sao Paulo, Brazil) was used for weight measurement.
The weight of disabled women was estimated using the Chumlea equations, which require several anthropometric measurements10
Height was measured with the subjects barefoot, standing erect, and looking at the horizon. Body height was measured as the distance between the vertex and the plantar region. The stadiometer used for the measurements was an inextensible vertical bar with 0.5 cm graduation marks. For bedridden subjects, height was estimated starting at knee height, as proposed by Chumlea et al.10
Body mass index (BMI) was calculated as weight/height2 (BMI = kg/m2) and was classified according to the stratifications proposed by Lipschitz,11 where values below 22 kg/m2 indicate underweight and the range between 24 and 29 kg/m2 indicates eutrophy.
The circumferences were measured using a 200-cm-long flexible and inextensible anthropometric tape with accuracy to one decimal place (Sanny, American Medical do Brasil Ltd, Sao Paulo, Brazil). The 50th percentile values obtained in the Brazilian SABE (Health, Well-Being, and Aging) survey were adopted as reference values.12
WC and HC
WC was measured at the smallest diameter between the iliac crest and the last floating rib, which is the narrowest part of the trunk, and HC was measured at the maximum diameter of the buttocks.13
AC
AC was determined with the subject in the sitting position and the arm hanging loosely at her side, at the mid-portion of the arm between the elbow and the shoulder.13
CC
CC was determined with the subject standing up (when possible) with the feet apart in such a way that body weight would be equally distributed on each foot. An inextensible tape was used to measure the largest circumference of the calf.14
The three methods for the assessment of body composition (skinfolds, BIA, and deuterium oxide method) were applied on the same day.
Skinfolds
The skinfolds were measured using a Lange adipometer (Santa Cruz, CA, USA) with a 0–60 mm scale and a ±1 mm precision, on the right side of the body. The sites assessed were biceps, triceps, subscapular, suprailiac, and thigh according to the 1988 standardization of Lohman et al.14 The National Health and Nutrition Examination Survey (NHANES) 50th percentile up to 74.9 years was adopted as reference to skinfolds.15
Each skinfold was measured in triplicate and the mean value was calculated. Body density was calculated using the following equations:
Jackson and Pollock equation16
*Skinfolds (triceps + suprailiac + thigh)
2. Durnin and Womersley equation17
**Skinfolds (triceps + biceps + subscapular + suprailiac).
The Siri equation18 was used to determine the percentage of body fat (%BF) in the two equations
FM was calculated with the following equation
And LM was calculated with the following equation
Electrical BIA
After 8 h of sleep and under fasting conditions, each subject was submitted to tetrapolar, 800 µA, and 50 kH BIA (Model 450; Biodynamics, Seattle, WA, USA). The electrodes were positioned on the ipsilateral surface of the wrist and ankle and on the distal line of the carpal and metacarpal bones of the dominant dimidium.19 Three subjects were not submitted to the examination due to the presence of a pacemaker, a factor that contraindicates the examination, and one subject died before the test.
Deuterium oxide
For the assessment of body composition by the deuterium oxide method, the subjects were instructed to fast for an overnight period of 10–12 h. After the anthropometric measurements and BIA at the home of each volunteer, basal saliva (at least 1 mL) was collected. Next, the volunteer received a standard dose of 90 g of a 7% dilution of 99.9% deuterium oxide (Cambridge Isotope Laboratories, Inc., Tewksbury, MA, USA), followed by 50-mL natural water for complete deuterium intake and for mouth washing. A new saliva sample was collected 3 h after deuterium intake, and all samples were stored at −10°C until analysis.
In all, 20 out of the 24 subjects had saliva samples collected, since 4 subjects had scarce saliva and/or presented dementia syndromes that impeded saliva collection. Some subjects were not collaborative, and the help of caregivers was of fundamental importance. When the participant was unable to deliver saliva correctly into the flask, we placed a cotton bud in her oral cavity and, after it became saturated, we placed it inside a syringe and compressed it to expel the saliva into the tube.
Deuterium enrichment in the saliva samples was determined by isotope ratio mass spectrometer (ANCA 20-22; Sercon, Cheshire, UK) after equilibrium with 20% hydrogen by the platinum–aluminum catalyzer method.
Statistical analysis
An exploratory analysis was first applied to the data using descriptive statistics (mean and median) and variability (standard deviation (SD)) with the aid of the SPSS 17.0.2 software.
Bland–Altman graphs for the determination of the distribution of body composition data obtained by the various methods and the Lin’s coefficients for the assessment of agreement between the methods were constructed using the MedCal® software, Version 9.1.10.1. The Lin’s coefficient ranges from −1 to 1 and is used to assess the level of agreement between two measurements. Levels closer to 1 indicate better agreement between methods.
Results
The study was conducted on 24 centenarian women with a mean age of 101.1 ± 2.0 years. Of the total, 25% were bedridden and only 37.5% had normal cognition. They had 3.7 ± 1.7 comorbidities, and the number of medications in use was 5.3 ± 3.5.
Table 1 presents the anthropometric data of the subjects. The BMI values were lower than 22 kg/m2 in 16 subjects (64%).
Table 1.
Anthropometric measurements applied to centenarian women (n = 22).
| Mean | SD | |
|---|---|---|
| Height (cm) | 148.4 | 6.0 |
| Weight (kg) | 46.4 | 9.8 |
| BMI (kg/m2) | 21.2 | 5.0 |
| Arm circumference (cm) | 22.3 | 2.7 |
| Waist circumference (cm) | 79.0 | 7.5 |
| Hip circumference (cm) | 90.0 | 6.0 |
| Calf circumference (cm) | 28.6 | 2.3 |
| Biceps (mm) | 7.2 | 3.6 |
| Triceps (mm) | 10.1 | 3.7 |
| Subscapular (mm) | 10.3 | 3.3 |
| Suprailiac (mm) | 8.5 | 3.6 |
| Thigh (mm) | 17.5 | 8.0 |
| Phase angle (degree) | 4.3 | 1.2 |
| Resistance (ohm) | 728 | 111 |
| Reactance (ohm) | 54 | 16 |
SD: standard deviation; BMI: body mass index.
All subjects had AC values lower than 29 cm and only 3 women (12.5%) had WC values of 86 cm or more. CC was less than 32 cm in 18 centenarians (90%). All subjects had a tricipital skinfold of less than 24 mm.
Table 2 presents the body composition data of the subjects obtained by the deuterium oxide method, BIA, and by the Jackson and Pollock16 the Durnin and Womersley17 equations.
Table 2.
Body composition of centenarian women (n = 20) determined by the deuterium oxide method, bioelectrical impedance, and by the Jackson and Pollock16 and the Durnin and Womersley17 equations.
| Deuterium |
BIA |
Durnin and Womersley |
Jackson and Pollock |
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| LM (kg) | 31.1 | 3.7 | 27.0 | 5.9 | 32.5 | 3.3 | 33.5 | 3.0 |
| LM (%) | 69.5 | 8.5 | 57.5 | 8.6 | 72.3 | 4.2 | 74.8 | 7.0 |
| FM (kg) | 14.0 | 4.8 | 20.2 | 7.0 | 12.6 | 3.1 | 12.0 | 4.3 |
| FM (%) | 30.5 | 8.5 | 42.5 | 8.6 | 27.7 | 4.2 | 25.2 | 7.0 |
BIA: bioelectrical impedance analysis; SD: standard deviation; LM: lean mass; FM: fat mass.
Figures 1–6 illustrate the distribution of the body composition parameters of the subjects according to the methods applied.
Figure 1.
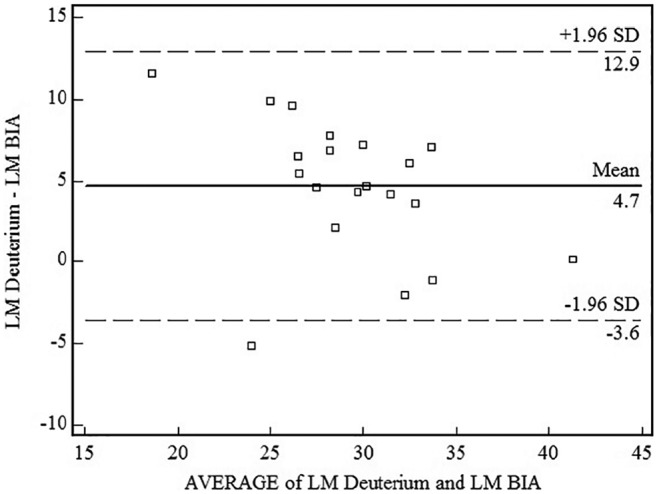
Bland–Altman graph for lean mass (LM) determined by the deuterium oxide method and by bioelectrical impedance analysis (BIA).
Figure 2.
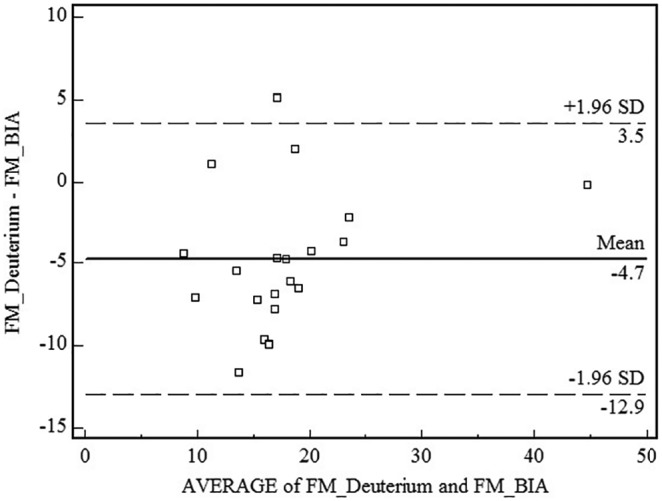
Bland–Altman graph for fat mass (FM) determined by the deuterium oxide method and by bioelectrical impedance analysis (BIA).
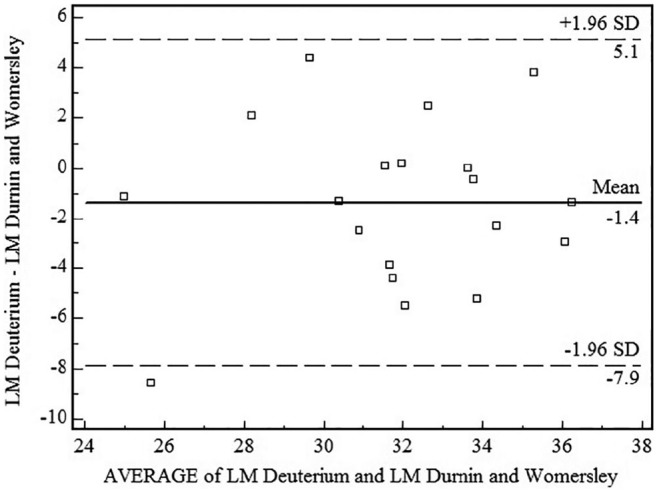
Figure 3.
Bland–Altman graph for lean mass (LM) determined by the deuterium oxide method and by the Durnin and Womersley equation.17
Figure 4.
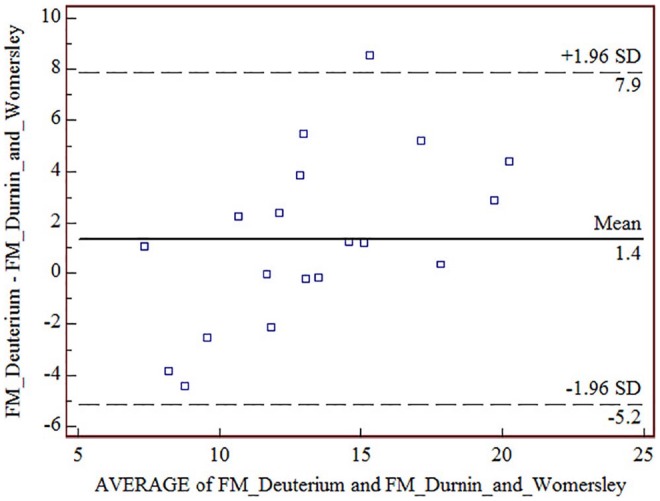
Bland–Altman graph for fat mass (FM) determined by the deuterium oxide method and by the Durnin and Womersley equation.17
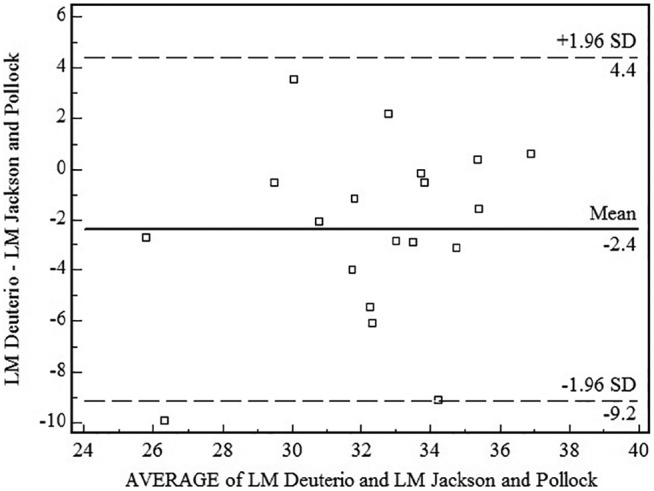
Figure 5.
Bland–Altman for lean mass (LM) determined by the deuterium oxide method and by the Jackson and Pollock equation.16
Figure 6.
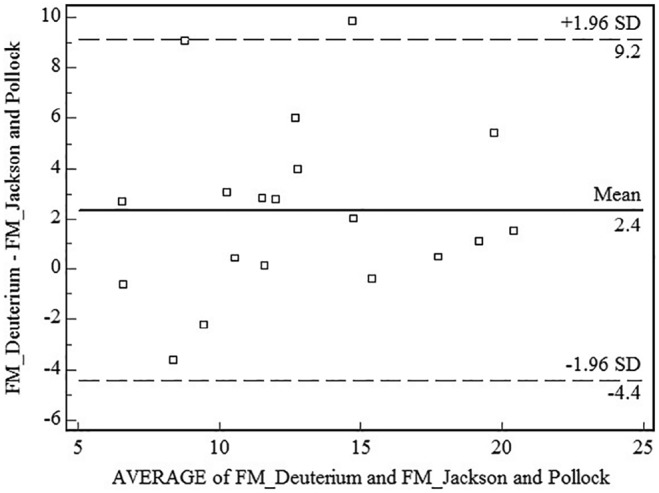
Bland–Altman graph for fat mass (FM) determined by the deuterium oxide method and by the Jackson and Pollock equation.16
Table 3 shows that, when the various methods used were compared with the deuterium oxide method, there was better agreement for the determination of FM than for the determination of LM. For FM, agreement was better when using BIA, whereas for LM, agreement was better when using the Durnin and Womersley equation.17
Table 3.
Agreement between the following methods for the assessment of body composition: deuterium oxide dilution, bioelectrical impedance, and anthropometry.
| Lin’s coefficient | 95% CI | |
|---|---|---|
| FM deuterium × FM BIA | 0.70 | 0.47–0.84 |
| LM deuterium × LM BIA | 0.46 | 0.18–0.66 |
| FM deuterium × FM Jackson and Pollock16 | 0.68 | 0.38–0.85 |
| LM deuterium × LM Jackson and Pollock16 | 0.37 | 0.02–0.64 |
| FM deuterium × FM Durnin and Womersley17 | 0.62 | 0.34–0.80 |
| LM deuterium × LM Durnin and Womersley17 | 0.51 | 0.13–0.76 |
CI: confidence interval; FM: fat mass; BIA: bioelectrical impedance analysis; LM: lean mass.
Discussion
Although the relevance of studying body composition in older individuals has been well demonstrated, few studies have analyzed the body composition of centenarians, with women representing the great majority of persons in this age range.20
Stable isotopes, deuterium oxide in this case, have advantages and disadvantages. Among the advantages, there is a minimal risk to health even when it is used in newborns and pregnant women, high precision for the determination of body water, and the possibility of sample storage without tracer loss and reuse of the same sample for further analysis. Among the disadvantages are high cost, time-consuming sample preparation, complex analysis, and the impossibility of determining retention directly.21
The results obtained follow the model of two-compartment body composition (LM and FM), which does not permit the assessment of body water distribution in different compartments or of BF distribution. For this reason, the method should not be applied to subjects with edema, decompensated heart failure, or other conditions involving changes in body water volume.22
Studies have demonstrated that the determination of LM and FM by BIA may be affected by the nutritional status of older persons. Vilaça et al.22 demonstrated that the agreement of body composition assessed by BIA with that assessed by DXA was worse in malnourished than in healthy subjects.23 BIA tends to overestimate LM and to underestimate FM in malnourished older subjects.
In this study, we did not select the subjects according to their nutritional status, but most of them had low weight. When agreement between BIA and deuterium oxide was assessed, it was found to be better in the determination of FM than of LM. This agreement would possibly be greater if verified in healthier subjects.
The BIA method could not be applied to three subjects (9.7%) due to the presence of a heart pacemaker, and one subject died before the examination. The BIA method was of easy execution and comfortable for the centenarians, being practical, painless, and user-friendly. The single-frequency BIA method was chosen over the multifrequency BIA, because the latter is more expensive, although it is referred to be more accurate.24 The objective of this work was to evaluate low-cost methods.
Skinfolds were also measured, for being the most frequently used method for the determination of BF due to its low cost and relatively simple use compared with other methods.22 Although validated equations are available in Brazil, there is a predominant use of the Jackson and Pollock16 and the Durnin and Womersley17 equations.15,25,26 In a previous study, the specific and generalized Durnin and Womersley17 equations underestimated BF percentage measured by hydrostatic weighing among subjects aged up to 72 years. We have no references of body composition equations for the centenarian population.
Among elderly women with a mean age of 70 years, FM percentage was about 40% when assessed by the deuterium, Jackson and Pollock,16 and Durnin and Womersley17 methods, as opposed to about 30% for the centenarian women studied here.27 Thus, centenarian women seem to have a lower fat percentage than 70-year-old women.
In the same study,27 the agreement between the deuterium and the anthropometric methods was better for FM, as observed in this study. However, the agreement between these methods in the measurement of FM seems to be better for non-centenarian older persons than for centenarians. This study demonstrated that the equations used showed moderate- to-strong agreement with the deuterium method, as also observed in studies conducted on distinct populations.28
Many of the centenarians studied here had difficulty in locomotion and 25% of them were assessed on bed. So, the DXA assessment was not possible to use. The objective of the study was to use the most commonly used body composition tools in clinical practice, such as BIA, and compare it with deuterium oxide, which despite being a sophisticated technique, allows the collection of biological material anywhere.
Skinfold percentile tables are available15 but they usually include values up to the age of 75 years, which would not serve as parameters for the present sample. Although this reference is old, it is still the most used in clinical practice to verify alterations of body composition by the anthropometry method. If we use the SABE table,12 which includes Brazilian older people aged 86 years or above, the 50th percentile will be 18 cm, and all centenarians studied here had values below this. Based on these existing tables, we found that the measured skinfolds, such as the tricipital fold, were below the 50th percentile in all the women evaluated.
One limitation of this study was the small sample size. However, the study involved a representative sample of the centenarians (41.4%) residing in a medium-sized city with a total of 58 centenarians identified in the 2010 census.9 The data we found may differ from those obtained in countries with a higher level of development; however, our main objective was to compare different methods of assessing body composition in the same centenarian individuals.
Concluding, when different methods for the assessment of body composition were applied to centenarian women, there was better agreement in the determination of FM than in the determination of LM. Bioimpedance had better agreement with the deuterium dilution method in the assessment of FM and the Durnin and Womersley equation17 in the assessment of LM. Although further studies are needed for the development of more specific tools for the assessment of body composition in very old people, BIA and skinfolds may be used for the evaluation of FM and LM, respectively.
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval: Ethical approval for this study was obtained from the Research Ethics Committee of the University Hospital, Faculty of Medicine of Ribeirão Preto (HCFMRP USP) on 9 April 2012 (protocol no. 9032012).
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the University of São Paulo (NAPENV) and by the Foundation for the Support of São Paulo State’s Research (FAPESP-MCT/CNPq-PRONEX Process: 2011/50768-7).
Informed consent: Written informed consent was obtained from all subjects before the study or from their legally authorized representatives (in cases where the subjects did not have the decisional capacity to provide informed consent).
ORCID iD: Nereida KC Lima  https://orcid.org/0000-0002-7139-8883
https://orcid.org/0000-0002-7139-8883
Trial registration: This study is not a randomized clinical trial, as it was not registered.
References
- 1. Guralnik JM, Kaplan GA. Predictors of healthy aging: prospective evidence from the Alameda county study. Am J Public Health 1989; 79(6): 703–708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. NIA Aging and Genetic Epidemiology Working Group. Genetic epidemiologic studies on age-specified traits. Am J Epidemiol 2000; 152: 1003–1008. [DOI] [PubMed] [Google Scholar]
- 3. Gueresi P, Troiano L, Minicuci N, et al. The MALVA (MAntova LongeVA) study: an investigation on people 98 years of age and over in a province of Northern Italy. Exp Gerontol 2003; 38(10): 1189–1197. [DOI] [PubMed] [Google Scholar]
- 4. Ahmed T, Haboubi N. Assessment and management of nutrition in older people and its importance to health. Clin Interv Aging 2010; 5: 207–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Pereira da, Silva A, Matos A, Valente A, et al. Body composition assessment and nutritional status evaluation in men and women Portuguese centenarians. J Nutr Health Aging 2016; 20(3): 256–266. [DOI] [PubMed] [Google Scholar]
- 6. Pfrimer K, Moriguti JC, Lima NK, et al. Bioelectrical impedance with different equations versus deuterium oxide dilution method for the inference of body composition in healthy older persons. J Nutr Health Aging 2012; 16(2): 124–127. [DOI] [PubMed] [Google Scholar]
- 7. Guglielmi G, Ponti F, Agostini M, et al. The role of DXA in sarcopenia. Aging Clin Exp Res 2016; 28(6): 1047–1060. [DOI] [PubMed] [Google Scholar]
- 8. Aleman-Mateo H, Rush E, Esparza-Romero J, et al. Prediction of fat-free mass by bioelectrical impedance analysis in older adults from developing countries: a cross-validation study using the deuterium dilution method. J Nutr Health Aging 2010; 14(6): 418–426. [DOI] [PubMed] [Google Scholar]
- 9. Brazilian Institute of Geography and Statistics (IBGE), www.cidades.ibge.gov.br; http://www.ibge.gov.br/home/estatistica/populacao/censo2010/
- 10. Chumlea WC, Guo S, Roche AF, et al. Prediction of body weight for the nonambulatory elderly from anthropometry. J Am Diet Assoc 1988; 88(5): 564–568. [PubMed] [Google Scholar]
- 11. Lipschitz DA. Screening for nutritional status in the elderly. Prim Care 1994; 21(1): 55–67. [PubMed] [Google Scholar]
- 12. Almeida MF, Marucci MF, Gobbo LA, et al. Anthropometric changes in the Brazilian cohort of older adults: SABE survey (health, well-being, and aging). J Obes 2013; 2013: 695496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Hure AJ, Collins CE, Giles WB, et al. Protocol for the women and their children’s health (WATCH) study: a cohort of pregnancy and beyond. J Epidemiol 2012; 22(3): 267–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lohman TG, Roche AF, Martorell R. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics, 1988. [Google Scholar]
- 15. Frisancho AR. New standards of weight and body composition by frame size and height for assessment of nutritional status of adults and the elderly. Am J Clin Nutr 1984; 40(4): 808–819. [DOI] [PubMed] [Google Scholar]
- 16. Jackson AS, Pollock ML. Generalized equations for predicting body density of men. Br J Nutr 1978; 40(3): 497–504. [DOI] [PubMed] [Google Scholar]
- 17. Durnin JVGA, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr 1974; 32(1): 77–97. [DOI] [PubMed] [Google Scholar]
- 18. Siri WE. Body composition from fluid spaces and density: analysis of methods. In: Brozek J, Henschel A. (eds) Techniques for measuring body composition. Washington, DC: National Academy of Sciences, National Research Council, 1961, pp. 223–243. [Google Scholar]
- 19. Baumgartner R, Chumlea WC, Roche AF. Estimation of body composition from bioelectric impedance of body segments. Am J Clin Nutr 1989; 50(2): 221–226. [DOI] [PubMed] [Google Scholar]
- 20. Campos AC, Ferreira EF, Vargas AM, et al. Healthy aging profile in octogenarians in Brazil. Rev Lat Am Enfermagem 2016; 29(24): e2724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Bila WC, Mariano RM, Silva VR, et al. Applications of deuterium oxide in human health. Isotopes Environ Health Stud 2017; 6: 1–17. [DOI] [PubMed] [Google Scholar]
- 22. Vilaça KH, Paula FJ, Ferriolli E, et al. Body composition assessment of undernourished older subjects by dual-energy x-ray absorptiometry and bioelectric impedance analysis. J Nutr Health Aging 2011; 15(6): 439–443. [DOI] [PubMed] [Google Scholar]
- 23. Aniteli TM, Florindo AA, Pereira RMR, et al. Development of an equation for measurement of body fat mass of elderly women with osteoporosis or osteopenia through skin fold thickness using dual energy X-ray absorptiometry as a reference. Rev Bras Med Esporte 2006; 12(6): 366–370. [Google Scholar]
- 24. Martinoli R, Mohamed EI, Maiolo C, et al. Total body water estimation using bioelectrical impedance: a meta-analysis of the data available in the literature. Acta Diabetol 2003; 40(Suppl. 1): S203–S206. [DOI] [PubMed] [Google Scholar]
- 25. Petroski EL, Pires-Neto CS. Validity of anthropometric equations for the estimation of body density in men. Rev Bras Ativ Fis Saude 1996; 1: 5–14. [Google Scholar]
- 26. Fonseca PH, Marins JC, Silva AT. Validation of anthropometric equations for the estimation of body density in professional soccer players. Rev Bras Med Esporte 2007; 13: 153–156. [Google Scholar]
- 27. Carneiro JAO, Vilaça KHC, Pfrimer K, et al. Evaluation of body composition of eutrophic young women and eutrophic and overweight elderly women using the deuterium oxide method and different anthropometric equations. Rev Nutr 2015; 28(5): 465–473. [Google Scholar]
- 28. Yao M, Roberts SB, Ma G, et al. Field methods for composition assessment are valid in healthy Chinese adults. J Nutr 2002; 132(2): 310–317. [DOI] [PubMed] [Google Scholar]