

Abstract
Children with specific learning disorders (SLDs) face a unique set of socio-emotional challenges as a result of their academic difficulties. Although a higher prevalence of anxiety in children with SLD is often reported, there is currently no research on cognitive mechanisms underlying this anxiety. One way to elucidate these mechanisms is to investigate attentional bias to threatening stimuli using a dot-probe paradigm. Our study compared children ages 9–16 with SLD (n=48) to typically-developing (TD) controls (n=33) on their attentional biases to stimuli related to general threats, reading, and stereotypes of SLD. We found a significant threat bias away from reading-related stimuli in the SLD, but not TD group. This attentional bias was not observed with the general threat and stereotype stimuli. Further, children with SLD reported greater anxiety compared to TD children. These results suggest that children with SLD experience greater anxiety, which may partially stem from reading specifically. The finding of avoidance rather than vigilance to reading stimuli indicates the use of more top-down attentional control. This work has important implications for therapeutic approaches to anxiety in children with SLD and highlights the need for attention to socio-emotional difficulties in this population. Future research is needed to further investigate the cognitive aspects of socio-emotional difficulties in children with SLD, as well as how this may impact academic outcomes.
INTRODUCTION
An estimated 5–15% of school-aged children are diagnosed with a Specific Learning Disorder (SLD; American Psychiatric Association, 2013). SLD is characterized by underperformance in reading, writing, and/or mathematics that is unexpected given a child’s IQ and adequate schooling. SLD is neurobiological in origin (Xia, Hancock, & Hoeft, 2017), and a large body of literature has documented cognitive risk factors associated with SLD (Moll, Göbel, Gooch, Landerl, & Snowling, 2016). The majority of SLD occurs in the reading domain, yet comorbidity rates between the different SLDs are high. For example, SLD in reading co-occurs with SLD in math at a rate of 30 to 70% (Willcutt et al., 2013). Individuals with SLD often experience poor math and reading outcomes (Dandache, Wouters, & Ghesquière, 2014; Shalev, Manor, & Gross-Tsur, 2005), and consequently have higher rates of school dropout and lower college attendance than those without SLD (Morrison & Cosden, 1997; Murray, Goldstein, Nourse, & Edgar, 2000).
In addition to academic difficulties, children with SLD may experience psychological maladjustment including anxious symptomatology. A recent meta-analysis reported that approximately 70% of students with SLD experience higher levels of anxiety than their non-SLD peers (Nelson & Harwood, 2011). In a large dataset of 36,984 individuals, 20% of young people with SLD reported a comorbid anxiety disorder compared to 10% of their peers without SLD (Wilson, Deri Armstrong, Furrie, & Walcot, 2009). In explaining the higher prevalence of anxiety in children with SLD, most theorists propose that anxiety develops as a secondary consequence of repeated school failure (Carroll, Maughan, Goodman, & Meltzer, 2005). Anxiety might also develop as a result of stereotype threat, the fear of confirming a negative stereotype about one’s group (Spencer, Logel, & Davies, 2016). Although the existence of stereotype threat has yet to be investigated in this population, research shows that students with SLD often feel stigmatized as a result of their diagnosis, which may result in stereotype threat (Shifrer, 2013). This stigma may come from the label of SLD – while a formal diagnosis might comfort children in providing an explanation for their difficulties, it can also make them feel ostracized. Indeed, a longitudinal study found that individuals with SLD seemed less concerned with “the day-to-day technical problems of the disability,” and more frustrated with “the stigma attached to it by their culture,” including feeling “different” from their peers in school (Higgins, Raskind, Goldberg, & Herman, 2002). Children with SLD in one study, for instance, reported concerns about being perceived as “stupid,” “lazy”, or “careless” by their peers because of their academic struggles (Riddick, 2001). This worry about what others think may lead some children to try to conceal their SLD, leading to considerable stress (Pachankis, 2007) that might magnify as their SLD progresses and develops. This stress may be further caused or exacerbated by the increased parental stress and family conflict observed in families of children with SLD (L. Dyson, 2010; L. L. Dyson, 2003; Karande, Kumbhare, Kulkarni, & Shah, 2009). Whether from academics or stereotype threat, this anxiety experienced by students with SLD may then interrupt key cognitive processes involved in learning, leading to further underperformance in school. If left untreated, anxious symptoms and psychopathology might contribute to further socio-emotional risk, such as the increased suicide rates that are observed in the SLD population (Wilson et al., 2009).
Despite evidence for a higher rate of anxiety in SLD and its serious implications, the hypothesized mechanisms behind anxiety in this population are understudied. Current research consists largely of self-, parent-, or teacher-reports of anxiety in children with SLD, without investigations into its cognitive underpinnings. One approach for studying anxiety in other populations involves examining attentional bias to negative or threatening stimuli, which is hypothesized to cause and perpetuate anxiety (Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & Van Ijzendoorn, 2007). Indeed, studies show that anxious children demonstrate hypervigilance toward threat-related stimuli (see (Dudeney, Sharpe, & Hunt, 2015) for meta-analysis) – this bias is commonly evaluated with a dot-probe task. The dot probe compares response times to probes in spatial proximity to threatening or neutral stimuli to quantify a threat-related attentional bias (MacLeod, Mathews, & Tata, 1986). This task has been used to ascertain attentional bias in a variety of child populations, including those with depression (Joormann, Talbot, & Gotlib, 2007; Neshat-Doost, Moradi, Taghavi, Yule, & Dalgleish, 2000; Taghavi, Neshat-Doost, Moradi, Yule, & Dalgleish, 1999), post-traumatic stress disorder (Bertó et al., 2017; Briggs‐Gowan et al., 2015; Dalgleish, Moradi, Taghavi, Neshat-Doost, & Yule, 2001), autism spectrum disorder (Hollocks, Ozsivadjian, Matthews, Howlin, & Simonoff, 2013; May, Cornish, & Rinehart, 2015; Moore, Heavey, & Reidy, 2012; Zhao, Zhang, Fu, & Maes, 2016), Williams syndrome (Dodd & Porter, 2010; McGrath et al., 2016), asthma (Dudeney et al., 2017; Lowther, Newman, Sharp, & McMurray, 2016), and a range of anxiety disorders (Hunt, Keogh, & French, 2007; Salum et al., 2013; Sylvester, Hudziak, Gaffrey, Barch, & Luby, 2016; Vasey, Daleiden, Williams, & Brown, 1995; Waters, Henry, Mogg, Bradley, & Pine, 2010).
One relevant area of design in dot-probe research is whether the task content is generally threatening or specific to a disorder or population. For example, dot-probe studies with children with asthma have included asthma-related words (e.g., dust, cough, allergic; Dudeney et al., 2017), and studies with depressed children include depression-related words (e.g., crying, bully, lonely; Neshat-Doost et al., 2000). Determining whether attentional bias is due to threats in general or disorder-specific content has implications for cognitive models of anxiety. Attention to threat regardless of its specific content might indicate a more generic attention control dysfunction or amygdala hypersensitivity. Conversely, content specificity in attentional bias may signal more schema-driven processing involving learning and memory (Pergamin-Hight, Naim, Bakermans-Kranenburg, van IJzendoorn, & Bar-Haim, 2015). This distinction has implications for therapeutic approaches for SLD populations. If children with SLD show attentional biases toward general threat stimuli, then treatments for general anxiety such as cognitive behavioral therapy are likely to be applicable to SLD. If, however, the underpinnings of anxiety are content-specific to children with SLD, more tailored interventions may be merited. Furthermore, adopting the approach that anxiety is specific to the SLD experience, it is unclear whether this is due to academic difficulties or struggles with the social stigma of SLD.
Another important consideration is the directionality of the attentional bias, which has been found to vary as a result of task characteristics and clinical psychopathology. According to the vigilance-avoidance pattern, attention may initially be oriented toward threatening information (vigilance), and subsequently be directed away from it (avoidance; Mogg, Bradley, Miles, & Dixon, 2004). The initial vigilance is hypothesized to represent more bottom-up processing, where attention is automatically captured by salient stimuli (e.g. a bright flash of lightning). In contrast, avoidance may represent engagement of more top-down cognitive mechanisms, meaning attention is voluntarily guided towards or away from certain stimuli in a goal-directed manner (e.g., looking for a friend’s yellow hat in a crowd; Aue, Hoeppli, Piguet, Sterpenich, & Vuilleumier, 2013; Cisler & Koster, 2010; Ferri, Schmidt, Hajcak, & Canli, 2013). Avoidance rather than vigilance to threat has been observed with longer stimulus duration times (>500ms) in the dot-probe task (Koster, Crombez, Verschuere, Van Damme, & Wiersema, 2006; Mogg et al., 2004; Waters, Bradley, & Mogg, 2014), presumably capturing the later stage of controlled attentional processing. Other research has shown that bias direction may vary with specific clinical characteristics. Bias away from threat has been found in individuals exposed to severe life-threatening risks (Bar-Haim et al., 2010) or trauma (Pine et al., 2005). Recent work more applicable to the current study has shown that there is dissociation between fear and distress disorders in orienting to threat. Children with distress disorders (e.g. generalized anxiety) tend to be vigilant to threat, whereas children with fear disorders (e.g. specific phobia) tend to avoid threatening information, regardless of stimulus duration (Salum et al., 2013; Waters et al., 2014). Importantly, the attentional bias direction has predicted response to treatment in children and adults with anxiety (M. Price, Tone, & Anderson, 2011; Waters, Mogg, & Bradley, 2012). Thus, determining the direction of attentional bias has important implications for elucidating the cognitive mechanisms underlying and clinical implications of anxiety in children with SLD.
The current study was designed to address a gap in the literature by examining mechanisms of anxiety in children with SLD compared to typically-developing (TD) controls matched on age, gender, and vocabulary (often used as a proxy for verbal IQ). Self-report measures were used to compare the groups on anxiety. A linguistic dot-probe paradigm was employed to evaluate attentional bias with words associated with general threats, reading, and stereotypes of SLD. Reading stimuli was chosen for several reasons: the majority of SLDs occur in the domain of reading, reading is involved in nearly every academic subject, and attentional bias has yet to be investigated with reading (though it has with math and school/academics more broadly). These and the stereotype stimuli were developed using focus groups. The overall aim was to compare children with SLD and TD children on self-report measures of anxiety, distinguish between general and content-specific attentional bias to threat, and determine attentional bias direction. This study is the first to examine attentional bias to threat in children with SLD, and has implications for understanding and treating anxiety and related socio-emotional issues in this population.
Consistent with literature documenting increased anxious symptomatology in children with SLD, we hypothesized that children with SLD would score higher than their TD counterparts on anxiety. Regarding attentional bias, we could not make strong predictions as there are no previous studies examining this construct in an SLD population. However, a recent meta-analysis showed that content specific to a disorder evokes more attentional bias than general threat stimuli (Pergamin-Hight et al., 2015). Combining this finding with the theory that anxiety is a secondary consequence of SLD, we predicted that an attentional bias with reading stimuli (e.g. book, read) and stereotype stimuli (e.g. disabled, slow; both content specific to SLD) but not general threat stimuli (e.g. bomb, kill) would be shown. In regards to directionality of the biases, vigilance would represent engagement of more bottom-up mechanisms and clinical similarity of anxiety in children with SLD to distress disorders. Avoidance would indicate more top-down processing and resemblance to fear disorders. We did not have strong predictions as to directionality given the scarcity of research on mechanisms of anxiety in children with SLD – thus, this aspect of our study was exploratory. Finally, we hypothesized that attentional bias with the general threat stimuli only would be correlated with self-reported anxiety, since our anxiety measure was not specific to distress from reading or stereotype consciousness.
METHOD
Participants
Participants were children between the ages of 9–16. Children with SLD (n=50) were recruited from private schools for students with SLD in the San Francisco Bay Area. Two participants from this group were excluded in processing steps due to lack of usable data, (total n=48). Although independent diagnoses of SLD were not obtained for all students, schools indicated that all children in the SLD group had received a formal diagnosis from the school psychologist – these diagnoses were collected and used in reporting below. Diagnoses were further confirmed by examining neuropsychological reports from the school psychologist when they were made available to the first author (n=3). Additionally, independent neuropsychological testing of a subsample of students (n=9) was conducted with our staff psychologist which provided confirmation of reported diagnoses (total n=12 independent confirmation of diagnoses). Of our analysis sample (n=48), 42 students (87.5%) had an SLD with impairment in reading (reading disorder; RD), and the remaining 6 students (12.5%) had an SLD with impairment in math only (mathematics disorder; MD). Of the students with RD, 24 had a diagnosis of RD only, 11 had comorbid RD and writing disorder (WD), and 7 had comorbid RD, WD, and MD. There were 26 students (54.2%) of the analysis sample who had a comorbid diagnosis of ADHD. The occurrences of comorbid diagnoses in our SLD sample is reflective of the heterogeneity observed within SLD populations as a whole (see Hendren, Haft, Black, White, & Hoeft, 2018).
The control group of TD children (n=33) was recruited from one private school in the San Francisco Bay Area, as well as from the community through online advertisements. Exclusion criteria for the TD group included current or past diagnosis of any anxiety or neurodevelopmental disorder. We excluded children with these diagnoses as the purpose of the study was to investigate group differences in attentional bias in those with versus without an SLD diagnosis. We therefore wanted group differences to be attributable to the SLD diagnosis and label, rather than to group differences in anxiety diagnoses. Groups were matched on age, gender, and vocabulary level – participant characteristics are summarized in Table 1.
Table 1.
Comparison of SLD and TD controls on demographics and measures.
| Overall | Children with SLD | Controls | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Measures | n | Mean | SD | n | Mean | SD | n | Mean | SD | t | p |
| Age, years | 81 | 11.7 | 1.9 | 48 | 11.4 | 1.5 | 33 | 12.1 | 2.4 | −1.562 | .121 |
| Vocabulary (S) | 101 | 10.9 | 99 | 10.0 | 104 | 11.7 | −1.846 | .069 | |||
| Word Reading (S) | 95 | 16.9 | 89 | 14.7 | 105 | 15.1 | −4.806 | <.001 | |||
| Anxiety (T) ◊ | 54 | 10.1 | 56 | 10.7 | 51 | 8.6 | 2.056 | .043 | |||
Note.
S = Standard Scores; ≤ 70 = Extremely Low, 71–79 = Low, 80–89 = Low Average, 90–110 = Average, 111–120 = High Average, 121–129 = Superior, ≥ 130 = Very Superior
T = T Scores; < 60 = Within Normal Limits, 60–69 = At-Risk, ≥ 70 = Clinically Significant
5 children in the SLD group and 1 child in the Control group had Anxiety scores in the clinically significant range.
Study protocol was approved through the University of California San Francisco Institutional Review Board (Study #16–20551), and written consent for each participant was obtained from a parent or legal guardian. Verbal assent from each participant was also obtained. Testing sessions consisted of the following tasks that were randomized in order for each participant: (1) vocabulary assessment, (2) word-reading task, (3) self-report questionnaires (anxiety, sense of mastery, emotional reactivity), and (4) dot-probe paradigm. All questionnaires had audio options for items to be read out loud to the participant. The entire protocol lasted about one hour for each child.
Measures
Vocabulary.
The Picture Vocabulary subtest from the Woodcock Johnson-IV Test of Achievement (WJ-IV ACH; Schrank, Mather, & McGrew, 2014) was administered in order to determine the vocabulary level of each participant. Standard scores from this assessment were used to compare the vocabulary level of the SLD and TD groups to ensure that there were no significant differences.
Word Reading.
Word-reading fluency was assessed by administering the Sight Word Efficiency subtest from the Test of Word Reading Efficiency Second Edition (TOWRE-2; Torgesen, Wagner, & Rashotte, 2012). Standard scores were obtained and used to control for reading ability in our analyses.
Anxiety.
Participants completed the anxiety scale from the Behavior Assessment System for Children Second Edition (BASC-2) adolescent self-report. This scale instructs participants to rate how frequently feelings and thoughts of generalized fear and worry occur. Although BASC-2 reports are not used for clinical diagnoses, T-scores obtained can fall into three categories: within normal limits, at risk, or clinically significant. The BASC-2 is widely used to assess behavioral and emotional issues in children, and the anxiety self-report scale has excellent reliability (coefficient alpha = 0.86) and convergent validity with other anxiety scales (Reynolds & Kamphaus, 2004).
Attentional bias.
Attentional bias was measured using an adapted version of the dot-probe paradigm (MacLeod et al., 1986, see Figure 1). Each participant was seated approximately 1.5 feet away from a CF-54 Panasonic Toughbook laptop with a 14” screen (visual angle < 5°). Participants were told that they would see a fixation cross, followed by a pair of words one on top of the other, and then an arrow pointing either left or right. Participants were instructed to press an arrow key on a keyboard that corresponded to the direction of an arrow on the screen as quickly as possible. The fixation cross appeared for 500 ms, followed by 1250 ms of word pairs. After the word pairs, an arrow remained on the screen until participant response, and a 500 ms inter-trial interval preceded the next fixation cross. These parameters were chosen to be consistent with stimulus durations in previous literature using dot-probe tasks with children (Dudeney et al., 2017; Vasey et al., 1995). Words appeared 1 cm tall with 3 cm of vertical separation in a monospaced font (Courier) previously shown to be appropriate for individuals with SLD (Rello & Baeza-Yates, 2013). Arrows replaced either the top or bottom word and were 1 cm tall. All stimuli appeared in white on a black screen using E-Prime 2.0 software. Response times and accuracy for each arrow keyboard response were recorded.
Figure 1.
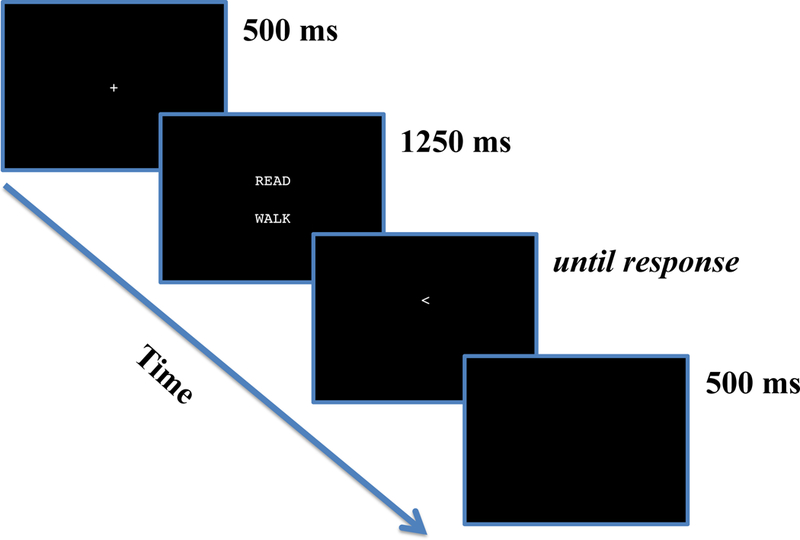
An illustration of the dot probe paradigm.
Participants were given 4 practice trials and needed an accurate response on at least three of these (75% accuracy) to move on to the test trials. If participants did not reach this level of accuracy, further sets of practice with 4 trials were administered up to two more times until 75% accuracy was achieved – all participants in our sample met at least 75% accuracy on one of the sets of practice trials. Test trials consisted of 16 neutral-neutral (NN) word pairs, 16 threat-neutral (TN) word pairs, 16 reading-neutral (RN) word pairs, and 16 stereotype-neutral (SN) word pairs. Word pairs were matched on their number of letters and syllables, as well as their frequency of appearance in the English language. Each word selected had a maximum age of acquisition rating of nine years. Frequency, age of acquisition rating, and emotional valence of words were determined from a database of 13,915 English lemmas (Warriner, Kuperman, & Brysbaert, 2013). Each word pair was presented four times to counterbalance word and arrow location for a total of 256 trials. Participants were given a two-minute break in the middle of the task.
NN word pairs were selected based on their rated valence and appropriate age of acquisition (< 9 years; Warriner et al., 2013). Threat words were selected using valence ratings and terms from previous literature when available (e.g. Hunt et al., 2007; Neshat-Doost et al., 2000; Vasey et al., 1995), then paired with neutral words on the properties described above to create TN pairs.
To generate reading words for RN pairs, the first author used school curriculums and a thesaurus to compile a list of 20 words related to reading. This list of words was then sent to a pilot group of 12 children between the ages of 10 and 14 (n=8 SLD and n=4 TD). The pilot group was asked to rate (a) their understanding of the meaning of the word (0 = do not understand, 1 = sort of understand, 2 = understand), and (b) the valence of the term (negative, neutral, or positive). From these ratings, two words with the lowest understanding were excluded. An additional two words were excluded whose average ratings did not fall into the neutral valence range. The resulting list of words was matched on valence (from Warriner et al., 2013), frequency, and number of letters and syllables to form 16 RN word pairs.
To generate words associated with stereotypes of SLD, a focus group (n=76) of individuals were recruited from an organization for persons with SLD. The focus group was asked to list terms that they believed were associated with stereotypes of SLD. A list of the top 20 most frequently listed words was compiled and sent to the pilot group, who rated the words on understanding and valence. The list was narrowed down to 16 words by excluding three words with low understanding and one word rated as having a positive valence. The resulting list of words was matched with neutral words on frequency (from Warriner et al., 2013) and number of letters and syllables to form 16 SN word pairs.
The final list of words and used in the present study are detailed in Supplementary Table 1.
Data Preparation
Trials with incorrect responses and inordinately fast (< 200 ms) or slow (> 2000 ms) response times (RTs) were excluded per standard practice (e.g. (Bradley, Mogg, White, Groom, & Bono, 1999; Mogg et al., 2004; Pérez-Edgar et al., 2011). These RTs suggest either unintentional responses or lapses in attention. Additionally, individual outliers of trials were excluded, defined as RTs that were 3 standard deviations away from that participant’s mean RT. Participants with removed trials constituting more than 5% of their data were excluded from further analysis – 2 participants from the SLD group were dropped as a result. Following removal of these participants, excluded trials accounted for 4.7% of the final data.
Attentional bias indices were calculated by subtracting the mean RT when the arrow replaced the threat/reading/stereotype word from the mean RT when the arrow replaced the neutral word. The index results in positive values for greater attention towards threat/reading/stereotype stimuli and negative values for attention away from these words.
A Shapiro-Wilk test of normality was performed on all questionnaires, assessments, and dot-probe RT data. Data for each group together and separately (SLD, TD) did not violate the test of normality (all p’s > 0.05). Split-half reliability analysis using intraclass correlation coefficient (ICC) of average probe response time per child in the two parts of the task, separated by condition, indicated excellent reliability (ICC = 0.948, p < 0.001).
Analyses
Differences between the SLD and TD groups on demographic, questionnaire, and assessment data were investigated using t-tests and χ2 tests. A one-sample t-test was used to compare bias indices to 0 to determine if any significant attentional bias was present separately for each group. To analyze group differences in any significant attentional bias, an independent samples t-test was used. To control for potential confounding influences of word-reading level and vocabulary in group differences, an analysis of covariance (ANCOVA) was conducted. Relationships between questionnaire and attentional bias data were examined using correlational analyses. Data were processed using R version 3.3.2 (R Core Team, 2013) and analyzed using SPSS version 23.
RESULTS
Participant Characteristics and Anxiety
Participants consisted of 48 SLD (11.4 ± 1.5 years; 63% male) and 33 TD children (12.1 ± 2.4 years; 48% male). There were no significant differences between gender (χ2(1)=1.565, p=0.211), age (t(79)=-1.579, p=0.121), or vocabulary (t(79)=-1.846, p=0.069) between the two groups. As expected, however, there was a significant group difference in word-reading ability, with higher word reading scores in the TD group (t(79)=-4.806, p<0.001). Children with SLD reported significantly higher anxiety than TD children (t(79)=2.056, p=0.043). Group demographics and comparisons are summarized in Table 1.
Attentional Bias
Attentional bias scores are displayed in Table 2. When compared to zero, the SLD group showed a significant negative bias away from reading stimuli (t(47)=-2.219, p=0.031), but no significant effects of threat (t(47)=-0.513, p=0.610) or stereotype (t(47 =0.019, p=0.985) stimuli on RT biases. The TD group showed no significant bias with threat (t(32) = -1.438, p=0.160), reading (t(32)=1.311, p=0.199), or stereotype (t(32)=0.379, p=0.707) stimuli.
Table 2.
Mean attentional bias indices (standard deviation in parentheses).
| SLD | Control | Effect Size (d) | |
|---|---|---|---|
| Threat bias | −3.07 (41.46) | −8.49 (33.90) | 0.14 |
| Reading bias | −11.78 (36.74) | 5.38 (23.55) | 0.56* |
| Stereotype bias | 0.10 (36.67) | 2.37 (35.94) | 0.06 |
p<.05 in a one-sample t-test compared to 0
Although subsample size was small, we repeated this analysis dividing the SLD group into those with comorbid ADHD (n=26) and without (n=22). Results did not change. A significant negative bias away from reading stimuli was still shown in children with and without comorbid ADHD (all p’s > 0.05), and there were no significant effects of threat or stereotype stimuli on RT biases in both groups (all p’s > 0.05). Because of this, analysis of group differences between the SLD and TD group uses the SLD group as a whole (including those with and without comorbid ADHD).
There was a significant difference between groups in attentional bias scores with reading stimuli (t(79=-2.558, p=0.012 ), with the SLD group having significantly greater attentional bias away from reading words.
To control for the potential confounding impact of vocabulary and word reading, we compared groups on reading attentional bias scores with a one-way ANCOVA. Vocabulary, word-reading scores, and age were mean-centered and entered as covariates. There was still a significant group difference on attentional bias with reading stimuli when controlling for word reading, vocabulary, and age (F(1,77)=4.984, p=0.029). Vocabulary (F(1,77) = 0.775, p=0.381), word reading (F(1,77) = 0.441, p = 0.509), and age (F(1,77) = 3.822, p=0.054) were not significant covariates.
Correlation Analyses
Bivariate correlations were performed between attentional biases and anxiety for children within SLD and TD children separately. There were no significant correlations between any of the attentional bias indices and anxiety scores for either group (all p’s>0.05). There were also no significant correlations between any of the attentional bias indices and word reading or vocabulary scores (all p’s>0.05).
DISCUSSION
The current study investigated differences in anxiety and attentional biases in children with SLD and TD controls. As hypothesized, the SLD group reported significantly higher anxiety compared to the TD group. Children with SLD showed a significantly greater attentional bias away from reading stimuli than TD children. Finally, attentional bias in each stimuli condition was not correlated with anxiety scores.
The finding of significantly higher anxiety in children with SLD compared to controls is in line with previous literature on this topic (Nelson & Harwood, 2011). Children with SLD face a number of academic and social stressors as a result of their disorder, and consequently may experience emotional distress. Results also revealed that there was significant group difference on attentional bias with reading-related words, with children with SLD showing avoidance of reading-related stimuli. Our finding was especially interesting given that the reading words were matched on valence to the neutral words, so these trials could be construed as a neutral-neutral pairing. Why would children with SLD show avoidance of neutral words associated with reading – a pattern otherwise observed with threatening stimuli? One explanation might be that because the task itself presented words, the topic of reading was primed. However, if this were the case, we would expect to see an attentional bias in TD children as well. Therefore, a more likely explanation is that there is greater sensitivity surrounding the reading words for the SLD group, suggesting a perception of threat. Indeed, our SLD group consisted mainly of children with primary impairment in reading –thus, reading is a source of difficulty and emotional struggle for these children. These findings are in line with a recent meta-analysis that showed disorder-congruent stimuli (content specific to a clinical population) evoke greater attentional bias than general threat stimuli for a range of disorders (Pergamin-Hight et al., 2015). In our study, a significant bias away from reading but not general threat content was observed, suggesting reading-related content may be a more salient threat to our SLD sample compared to controls.
The avoidance of reading stimuli observed in the SLD group suggests the engagement of more top-down cognitive mechanisms. This potential use of top-down processing might have been revealed as a result of our longer stimulus duration time (1250ms). This attention avoidance may represent a fear reduction strategy after an initial vigilance to the reading words (Aue et al., 2013) – our current methods do not allow for this initial detection, which represents an area of future research. These results suggest that attentional bias in children with SLD shows avoidance patterns similar to children with fear-related disorders such as specific phobias, rather than vigilance as is observed in children with generalized anxiety. This concurs with finding a content-specific bias with reading, but not general threat words in children with SLD, and has implications for treatment. Current attention bias modification treatments that train anxious individuals to be threat avoidant (Eldar et al., 2012) may not be a suitable treatment for children who already show avoidance to threat, such as our sample.
The lack of attentional bias to threat stimuli in the SLD sample warrants further discussion. Studies on attention to threat have generally shown mixed results in children, with significant biases primarily in children diagnosed with clinical anxiety disorders (Dudeney et al., 2015). Our TD group was screened for anxiety disorders, since we sought to investigate group differences in SLD status, rather than anxiety. Only one participant’s self-reported anxiety from the TD group fell into the clinically significant range. Of our SLD group, only five children had clinical levels of anxiety according to the used self-report measure – this sample is too small for separate analyses comparing those with and without clinically significant anxiety symptoms. A future study might specifically recruit a larger sample of children with SLD and comorbid anxiety disorders to see if results with our paradigm would be different.
We also did not find an attentional bias with stereotype stimuli in either SLD or TD children. Because stereotype stimuli were developed specifically for children with SLD, we expected to find an attentional bias with this content in this group. It is possible that, given their context, the words were not perceived as unique to SLD. For example, terms such as “dumb,” “lazy,” and “stupid” might be perceived as general social threats. If this is true, these stimuli might be more salient for children with general social anxiety than SLD. Of note, our study protocol did not cue an SLD identity – children were not told that they were selected for the study because of their SLD. Future work might therefore consider explicitly priming an SLD identity before administering the task. While our findings do not confirm a bias toward SLD stereotype stimuli, they do not necessarily preclude the existence of a stereotype threat phenomenon in this population either.
There were no significant correlations between attentional bias indices and self-reported anxiety. The lack of correlation between threat biases and anxiety may be due to differences between self-report measures and cognitive paradigms, where self-report measures may be susceptible to bias – more research is warranted in this area. A lack of correlation with the reading and stereotype bias indices was expected because of the content-specific nature of the threat. The BASC anxiety scale measures behaviors and feelings in general situations – we may see different results with a questionnaire asking about anxiety specific to reading or stereotype threat. Unfortunately, there are currently no tools to assess for anxiety specific to reading or stereotypes of SLD.
Several limitations of our study should be acknowledged. First, the finding of a significant attentional bias away from reading stimuli in children with SLD was only significant with an uncorrected threshold. Because our study was exploratory in nature as the first to use this paradigm in children with SLD, and because we found significant group differences in this bias, we still chose to discuss the implications of these results with an alpha level of 0.05. Second, the SLD sample had notably low word-reading ability as a result of their disorder, and a linguistic version of the dot-probe paradigm was used. TD children were not matched on reading ability. However, we controlled for the potential confounding impact of word reading by using an ANCOVA, and results remained the same. We also propose that, were children unable to understand the words, there would be no attentional bias at all in any direction (e.g. they would equally attend to each word). However, results indicate that this is not the case, suggesting children were able to successfully read the words and that this impacted their attention. Finally, questionnaire measures were available in an audio format to assist the comprehension of students with SLD. Future research might consider replicating this study using a picture dot-probe task, though some of our words may be difficult to adapt. Our third limitation is that we did not obtain independent SLD diagnoses for all students – thus, we could not investigate differences based on SLD severity. For our study, we were more interested in the impact of the experience of SLD and its associated label on socioemotional functioning assessed using multiple methods (i.e., self-report and attentional biases), rather than its neuropsychological properties. Because our SLD sample came from schools that only admit students with an SLD diagnosis, we can assume that these children were categorized accurately. A fourth limitation is that our sample of both SLD and TD children came from one geographic area – thus, while our groups were demographically similar to each other, they may not be representative of larger child populations. We should therefore be careful in generalizing these results, and future research should make an effort to include children from a wide range of socio-economic, cultural, and geographic backgrounds.
Relatedly, because our children with SLD came from private SLD schools, we may expect different results from children with SLD immersed in public school settings. Research has confirmed that children with SLD experience greater bullying and peer victimization than their TD peers (Cummings, Pepler, Mishna, & Craig, 2006; Mishna, 2003), and lower peer acceptance (Estell et al., 2008). However, it is currently unclear how the prevalence of these instances – and the social disadvantage and socio-emotional consequences that may result – differs between mainstream and SLD-only schools. One might hypothesize that students in SLD-only schools feel less “different” than their peers, leading to greater feelings of social acceptance and lower anxiety. However, research has also found that children with SLD are more frequently identified as perpetrators of bullying than their TD peers (Mishna, 2003)– this may mean that SLD-only schools have similar or even increased instances of bullying than mainstream settings. Given that perceived peer support can impact socio-emotional and mental health outcomes for children with SLD (e.g. (Al-Yagon, 2016), the school social climate would presumably impact anxiety and attentional bias levels. Unfortunately, research comparing differences in social and emotional outcomes for children with SLD between different educational settings is extremely limited, and represents a needed area of investigation.
A final limitation is that there are criticisms of RT paradigms in children (Brown et al., 2014), and with the psychometric properties of the dot-probe task specifically (Kappenman, Farrens, Luck, & Proudfit, 2014; Schmukle, 2005). These criticisms point to poor internal and test-retest reliability of the dot probe. Given that previous research has still found the dot probe to be a useful tool for elucidating cognitive mechanisms in clinical populations (Bar-Haim et al., 2007), and in particular children (Dudeney et al., 2015), we used it in our study. Additionally, we were careful to note some of the best practices recommendations outlined by Price et al., 2015), such as determining outliers in a data-driven manner. Still, future work might consider an additional use of eye-tracking, neurobiological or electrophysiological measures to supplement investigating these research questions.
Even with these limitations, our study offers a notable contribution to work on the unique challenges facing children with SLD. Notwithstanding the attentional bias results, our findings of differences between children with SLD and TD children in anxiety add to the literature on the nature of psychosocial difficulties in this population. Previous work has confirmed greater prevalence of anxiety and socio-emotional issues in children with SLD, but to the author’s knowledge our study is the first to date to offer insight into cognitive mechanisms underlying this maladjustment. Our results suggest that anxiety in children with SLD may manifest as a specific reaction to reading difficulties. Moreover, this attentional bias manifests as avoidance of, rather than vigilance to threat stimuli, suggesting engagement of more controlled top-down processes which may have been captured by our paradigm design. This line of work can inform how anxiety is treated in this population, and suggests the relevance of therapies that focus on students’ emotional difficulties with reading and academics.
It remains to be seen whether the avoidance of reading stimuli in students with SLD maintains or exacerbates negative attitudes and behaviors regarding reading. Previous studies have suggested a link between attentional bias and particular behaviors, such as ability to inhibit a prepotent response and social withdrawal (Pacheco-Unguetti, Acosta, Lupiáñez, Román, & Derakshan, 2012; Pérez-Edgar et al., 2010; Thai, Taber-Thomas, & Pérez-Edgar, 2016)(Pacheco-Unguetti, Acosta, Lupiáñez, Román, & Derakshan, 2012; Pérez-Edgar et al., 2010; Thai, Taber-Thomas, & Pérez-Edgar, 2016). Applied to the classroom context, this could mean that children with high levels of attentional bias may be more distracted by stimuli evoking certain threats, which would render them less able to focus on the task at hand, and might lead to avoidance of the threat. Given these studies and our results, educators and clinicians might consider investigating ways to attenuate the threatening nature of reading for children with SLD (e.g., by providing choices to children in what and how they read and fostering an accommodating reading environment). This has implications for both the socio-emotional well-being and academic success of children with SLD and represents an important area of future research for this population.
Supplementary Material
Table 3.
Correlations between bias indices, anxiety, and reading measures overall and for each group.
| 1 | 2 | 3 | 4 | 5 | ||
|---|---|---|---|---|---|---|
| 1. Threat Bias | Overall | -- | ||||
| SLD | ||||||
| Control | ||||||
| 2. Reading Bias | Overall | .009 | -- | |||
| SLD | .044 | |||||
| Control | −.014 | |||||
| 3. Stereotype Bias | Overall | −.191 | −.159 | -- | ||
| SLD | −.281 | −.188 | ||||
| Control | −.023 | −.150 | ||||
| 4. Word Reading | Overall | −.160 | .035 | −.074 | -- | |
| SLD | −.228 | −.139 | −.069 | |||
| Control | .000 | −.029 | −.147 | |||
| 5. Vocabulary | Overall | .011 | −.068 | −.094 | .302** | -- |
| SLD | .248 | −.128 | −.055 | .371** | ||
| Control | −.317 | −.141 | −.164 | .076 | ||
| 6. Anxiety | Overall | .004 | −.136 | .112 | −.174 | −.225* |
| SLD | .028 | −.139 | .231 | .002 | −.273 | |
| Control | −.102 | .074 | −.080 | −.223 | −.064 | |
= p<.01,
=p<.05
Acknowledgements:
This work was funded by Oak Foundation ORIO-16–012. Author FH was additionally funded by NICHD R01HD086168, R01HD096261, R01HD078351, P50HD052120 (PI: R. Wagner), National Science Foundation NSF-1540854, University of California Office of the President Multicampus Research Programs and Initiatives Award MRP-17–454925, UCSF Dyslexia Center, Ray & Lori dePole, Dyslexia Training Institute, The Potter Family, and ALTA.
Footnotes
Conflict of Interest: The authors declare that they have no conflict of interest.
REFERENCES
- Al-Yagon M (2016). Perceived close relationships with parents, teachers, and peers: predictors of social, emotional, and behavioral features in adolescents with LD or comorbid LD and ADHD. Journal of Learning Disabilities, 49(6), 597–615. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Pub. [Google Scholar]
- Aue T, Hoeppli M-E, Piguet C, Sterpenich V, & Vuilleumier P (2013). Visual avoidance in phobia: particularities in neural activity, autonomic responding, and cognitive risk evaluations. Frontiers in Human Neuroscience, 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bar-Haim Y, Holoshitz Y, Eldar S, Frenkel TI, Muller D, Charney DS, … Wald I (2010). Life-threatening danger and suppression of attention bias to threat. American Journal of Psychiatry, 167(6), 694–698. [DOI] [PubMed] [Google Scholar]
- Bar-Haim Y, Lamy D, Pergamin L, Bakermans-Kranenburg MJ, & Van Ijzendoorn MH (2007). Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. American Psychological Association. [DOI] [PubMed] [Google Scholar]
- Bertó C, Ferrín M, Barberá M, Livianos L, Rojo L, & García-Blanco A (2017). Abnormal emotional processing in maltreated children diagnosed of complex posttraumatic stress disorder. Child Abuse & Neglect, 73, 42–50. [DOI] [PubMed] [Google Scholar]
- Bradley BP, Mogg K, White J, Groom C, & Bono J (1999). Attentional bias for emotional faces in generalized anxiety disorder. British Journal of Clinical Psychology, 38(3), 267–278. [DOI] [PubMed] [Google Scholar]
- Briggs‐Gowan MJ, Pollak SD, Grasso D, Voss J, Mian ND, Zobel E, … Pine DS (2015). Attention bias and anxiety in young children exposed to family violence. Journal of Child Psychology and Psychiatry, 56(11), 1194–1201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown HM, Eley TC, Broeren S, MacLeod C, Rinck M, Hadwin JA, & Lester KJ (2014). Psychometric properties of reaction time based experimental paradigms measuring anxiety-related information-processing biases in children. Journal of Anxiety Disorders, 28(1), 97–107. [DOI] [PubMed] [Google Scholar]
- Carroll JM, Maughan B, Goodman R, & Meltzer H (2005). Literacy difficulties and psychiatric disorders: Evidence for comorbidity. Journal of Child Psychology and Psychiatry, 46(5), 524–532. [DOI] [PubMed] [Google Scholar]
- Cisler JM, & Koster EH (2010). Mechanisms of attentional biases towards threat in anxiety disorders: An integrative review. Clinical Psychology Review, 30(2), 203–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings JG, Pepler DJ, Mishna F, & Craig WM (2006). Bullying and victimization among students with exceptionalities. Exceptionality Education Canada, 16(2/3), 193. [Google Scholar]
- Dalgleish T, Moradi AR, Taghavi MR, Neshat-Doost HT, & Yule W (2001). An experimental investigation of hypervigilance for threat in children and adolescents with post-traumatic stress disorder. Psychological Medicine, 31(3), 541–547. [DOI] [PubMed] [Google Scholar]
- Dandache S, Wouters J, & Ghesquière P (2014). Development of reading and phonological skills of children at family risk for dyslexia: A longitudinal analysis from kindergarten to sixth grade. Dyslexia, 20(4), 305–329. [DOI] [PubMed] [Google Scholar]
- Dodd HF, & Porter MA (2010). I see happy people: attention bias towards happy but not angry facial expressions in Williams syndrome. Cognitive Neuropsychiatry, 15(6), 549–567. [DOI] [PubMed] [Google Scholar]
- Dudeney J, Sharpe L, & Hunt C (2015). Attentional bias towards threatening stimuli in children with anxiety: A meta-analysis. Clinical Psychology Review, 40, 66–75. [DOI] [PubMed] [Google Scholar]
- Dudeney J, Sharpe L, Sicouri G, Lorimer S, Dear BF, Jaffe A, … Hunt C (2017). Attentional Bias in Children with Asthma with and without Anxiety Disorders. Journal of Abnormal Child Psychology, 1–12. [DOI] [PubMed] [Google Scholar]
- Dyson L (2010). Unanticipated effects of children with learning disabilities on their families. Learning Disability Quarterly, 33(1), 43–55. [Google Scholar]
- Dyson LL (2003). Children with learning disabilities within the family context: A comparison with siblings in global self–concept, academic self–perception, and social competence. Learning Disabilities Research & Practice, 18(1), 1–9. [Google Scholar]
- Eldar S, Apter A, Lotan D, Edgar KP, Naim R, Fox NA, … Bar-Haim Y (2012). Attention bias modification treatment for pediatric anxiety disorders: a randomized controlled trial. American Journal of Psychiatry, 169(2), 213–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Estell DB, Jones MH, Pearl R, Van Acker R, Farmer TW, & Rodkin PC (2008). Peer groups, popularity, and social preference: Trajectories of social functioning among students with and without learning disabilities. Journal of Learning Disabilities, 41(1), 5–14. [DOI] [PubMed] [Google Scholar]
- Ferri J, Schmidt J, Hajcak G, & Canli T (2013). Neural correlates of attentional deployment within unpleasant pictures. NeuroImage, 70, 268–277. [DOI] [PubMed] [Google Scholar]
- Hendren RL, Haft SL, Black JM, White NC, & Hoeft F (2018). Recognizing Psychiatric Comorbidity With Reading Disorders. Frontiers in Psychiatry, 9, 101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins EL, Raskind MH, Goldberg RJ, & Herman KL (2002). Stages of acceptance of a learning disability: The impact of labeling. Learning Disability Quarterly, 25(1), 3–18. [Google Scholar]
- Hollocks MJ, Ozsivadjian A, Matthews CE, Howlin P, & Simonoff E (2013). The relationship between attentional bias and anxiety in children and adolescents with autism spectrum disorders. Autism Research, 6(4), 237–247. [DOI] [PubMed] [Google Scholar]
- Hunt C, Keogh E, & French CC (2007). Anxiety sensitivity, conscious awareness and selective attentional biases in children. Behaviour Research and Therapy, 45(3), 497–509. [DOI] [PubMed] [Google Scholar]
- Joormann J, Talbot L, & Gotlib IH (2007). Biased processing of emotional information in girls at risk for depression. Journal of Abnormal Psychology, 116(1), 135. [DOI] [PubMed] [Google Scholar]
- Kappenman ES, Farrens JL, Luck SJ, & Proudfit GH (2014). Behavioral and ERP measures of attentional bias to threat in the dot-probe task: poor reliability and lack of correlation with anxiety. Frontiers in Psychology, 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karande S, Kumbhare N, Kulkarni M, & Shah N (2009). Anxiety levels in mothers of children with specific learning disability. Journal of Postgraduate Medicine, 55(3), 165. [DOI] [PubMed] [Google Scholar]
- Koster EH, Crombez G, Verschuere B, Van Damme S, & Wiersema JR (2006). Components of attentional bias to threat in high trait anxiety: Facilitated engagement, impaired disengagement, and attentional avoidance. Behaviour Research and Therapy, 44(12), 1757–1771. [DOI] [PubMed] [Google Scholar]
- Lowther H, Newman E, Sharp K, & McMurray A (2016). Attentional bias to respiratory-and anxiety-related threat in children with asthma. Cognition and Emotion, 30(5), 953–967. [DOI] [PubMed] [Google Scholar]
- MacLeod C, Mathews A, & Tata P (1986). Attentional bias in emotional disorders. Journal of Abnormal Psychology, 95(1), 15. [DOI] [PubMed] [Google Scholar]
- May T, Cornish K, & Rinehart NJ (2015). Mechanisms of anxiety related attentional biases in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(10), 3339–3350. [DOI] [PubMed] [Google Scholar]
- McGrath LM, Oates JM, Dai YG, Dodd HF, Waxler J, Clements CC, … MacRae R (2016). Attention bias to emotional faces varies by IQ and anxiety in williams syndrome. Journal of Autism and Developmental Disorders, 46(6), 2174–2185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishna F (2003). Learning disabilities and bullying: Double jeopardy. Journal of Learning Disabilities, 36(4), 336–347. [DOI] [PubMed] [Google Scholar]
- Mogg K, Bradley B, Miles F, & Dixon R (2004). Brief report time course of attentional bias for threat scenes: testing the vigilance‐avoidance hypothesis. Cognition and Emotion, 18(5), 689–700. [Google Scholar]
- Moll K, Göbel SM, Gooch D, Landerl K, & Snowling MJ (2016). Cognitive risk factors for specific learning disorder: Processing speed, temporal processing, and working memory. Journal of Learning Disabilities, 49(3), 272–281. [DOI] [PubMed] [Google Scholar]
- Moore DJ, Heavey L, & Reidy J (2012). Attentional processing of faces in ASD: A dot-probe study. Journal of Autism and Developmental Disorders, 42(10), 2038–2045. [DOI] [PubMed] [Google Scholar]
- Morrison GM, & Cosden MA (1997). Risk, resilience, and adjustment of individuals with learning disabilities. Learning Disability Quarterly, 20(1), 43–60. [Google Scholar]
- Murray C, Goldstein DE, Nourse S, & Edgar E (2000). The postsecondary school attendance and completion rates of high school graduates with learning disabilities. Learning Disabilities Research & Practice, 15(3), 119–127. [Google Scholar]
- Nelson JM, & Harwood H (2011). Learning disabilities and anxiety: A meta-analysis. Journal of Learning Disabilities, 44(1), 3–17. [DOI] [PubMed] [Google Scholar]
- Neshat-Doost HT, Moradi AR, Taghavi MR, Yule W, & Dalgleish T (2000). Lack of attentional bias for emotional information in clinically depressed children and adolescents on the dot probe task. The Journal of Child Psychology and Psychiatry and Allied Disciplines, 41(3), 363–368. [PubMed] [Google Scholar]
- Pachankis JE (2007). The psychological implications of concealing a stigma: a cognitive-affective-behavioral model. Psychological Bulletin, 133(2), 328. [DOI] [PubMed] [Google Scholar]
- Pacheco-Unguetti A, Acosta A, Lupiáñez J, Román N, & Derakshan N (2012). Response inhibition and attentional control in anxiety. Quarterly Journal of Experimental Psychology, 65(4), 646–660. [DOI] [PubMed] [Google Scholar]
- Pérez-Edgar K, Bar-Haim Y, McDermott JM, Chronis-Tuscano A, Pine DS, & Fox NA (2010). Attention biases to threat and behavioral inhibition in early childhood shape adolescent social withdrawal. Emotion, 10(3), 349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez-Edgar K, Reeb-Sutherland BC, McDermott JM, White LK, Henderson HA, Degnan KA, … Fox NA (2011). Attention biases to threat link behavioral inhibition to social withdrawal over time in very young children. Journal of Abnormal Child Psychology, 39(6), 885–895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pergamin-Hight L, Naim R, Bakermans-Kranenburg MJ, van IJzendoorn MH, & Bar-Haim Y (2015). Content specificity of attention bias to threat in anxiety disorders: a meta-analysis. Clinical Psychology Review, 35, 10–18. [DOI] [PubMed] [Google Scholar]
- Pine DS, Mogg K, Bradley BP, Montgomery L, Monk CS, McClure E, … Kaufman J (2005). Attention bias to threat in maltreated children: Implications for vulnerability to stress-related psychopathology. American Journal of Psychiatry, 162(2), 291–296. [DOI] [PubMed] [Google Scholar]
- Price M, Tone EB, & Anderson PL (2011). Vigilant and avoidant attention biases as predictors of response to cognitive behavioral therapy for social phobia. Depression and Anxiety, 28(4), 349–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price RB, Kuckertz JM, Siegle GJ, Ladouceur CD, Silk JS, Ryan ND, … Amir N (2015). Empirical recommendations for improving the stability of the dot-probe task in clinical research. Psychological Assessment, 27(2), 365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rello L, & Baeza-Yates R (2013). Good fonts for dyslexia. In Proceedings of the 15th International ACM SIGACCESS Conference on Computers and Accessibility (p. 14). ACM. [Google Scholar]
- Reynolds CR, & Kamphaus RW (2004). Behavior assessment for children,(BASC-2). Circle Pines, MN: American Guidance Service. [Google Scholar]
- Riddick B (2001). Dyslexia and inclusion: time for a social model of disability perspective? International Studies in Sociology of Education, 11(3), 223–236. [Google Scholar]
- Salum GA, Mogg K, Bradley BP, Gadelha A, Pan P, Tamanaha AC, … Polanczyk G (2013). Threat bias in attention orienting: evidence of specificity in a large community-based study. Psychological Medicine, 43(4), 733–745. [DOI] [PubMed] [Google Scholar]
- Schmukle SC (2005). Unreliability of the dot probe task. European Journal of Personality, 19(7), 595–605. [Google Scholar]
- Schrank FA, Mather N, & McGrew KS (2014). Woodcock-Johnson IV tests of achievement. Rolling Meadows, IL: Riverside. [Google Scholar]
- Shalev RS, Manor O, & Gross-Tsur V (2005). Developmental dyscalculia: a prospective six-year follow-up. Developmental Medicine and Child Neurology, 47(2), 121–125. [DOI] [PubMed] [Google Scholar]
- Shifrer D (2013). Stigma of a label: Educational expectations for high school students labeled with learning disabilities. Journal of Health and Social Behavior, 54(4), 462–480. [DOI] [PubMed] [Google Scholar]
- Spencer SJ, Logel C, & Davies PG (2016). Stereotype threat. Annual Review of Psychology, 67, 415–437. [DOI] [PubMed] [Google Scholar]
- Sylvester CM, Hudziak JJ, Gaffrey MS, Barch DM, & Luby JL (2016). Stimulus-driven attention, threat bias, and sad bias in youth with a history of an anxiety disorder or depression. Journal of Abnormal Child Psychology, 44(2), 219–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taghavi MR, Neshat-Doost HT, Moradi AR, Yule W, & Dalgleish T (1999). Biases in visual attention in children and adolescents with clinical anxiety and mixed anxiety-depression. Journal of Abnormal Child Psychology, 27(3), 215–223. [DOI] [PubMed] [Google Scholar]
- Thai N, Taber-Thomas BC, & Pérez-Edgar KE (2016). Neural correlates of attention biases, behavioral inhibition, and social anxiety in children: An ERP study. Developmental Cognitive Neuroscience, 19, 200–210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torgesen JK, Wagner RK, & Rashotte CA (2012). TOWRE-2: Test of Word Recognition Efficiency–. Austin, TX: Pro-Ed. [Google Scholar]
- Vasey MW, Daleiden EL, Williams LL, & Brown LM (1995). Biased attention in childhood anxiety disorders: A preliminary study. Journal of Abnormal Child Psychology, 23(2), 267–279. [DOI] [PubMed] [Google Scholar]
- Warriner A, Kuperman V, & Brysbaert M (2013). Norms of valence, arousal, and dominance for 13,915 English lemmas. Behavioral Research Methods, 45(4), 1191–1207. 10.3758/s13428-012-0314-x [DOI] [PubMed] [Google Scholar]
- Waters AM, Bradley BP, & Mogg K (2014). Biased attention to threat in paediatric anxiety disorders (generalized anxiety disorder, social phobia, specific phobia, separation anxiety disorder) as a function of “distress” versus “fear”diagnostic categorization. Psychological Medicine, 44(3), 607–616. [DOI] [PubMed] [Google Scholar]
- Waters AM, Henry J, Mogg K, Bradley BP, & Pine DS (2010). Attentional bias towards angry faces in childhood anxiety disorders. Journal of Behavior Therapy and Experimental Psychiatry, 41(2), 158–164. [DOI] [PubMed] [Google Scholar]
- Waters AM, Mogg K, & Bradley BP (2012). Direction of threat attention bias predicts treatment outcome in anxious children receiving cognitive-behavioural therapy. Behaviour Research and Therapy, 50(6), 428–434. [DOI] [PubMed] [Google Scholar]
- Willcutt EG, Petrill SA, Wu S, Boada R, DeFries JC, Olson RK, & Pennington BF (2013). Comorbidity between reading disability and math disability: Concurrent psychopathology, functional impairment, and neuropsychological functioning. Journal of Learning Disabilities, 46(6), 500–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson AM, Deri Armstrong C, Furrie A, & Walcot E (2009). The mental health of Canadians with self-reported learning disabilities. Journal of Learning Disabilities, 42(1), 24–40. [DOI] [PubMed] [Google Scholar]
- Xia Z, Hancock R, & Hoeft F (2017). Neurobiological bases of reading disorder Part I: Etiological investigations. Language and Linguistics Compass, 11(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao X, Zhang P, Fu L, & Maes JH (2016). Attentional biases to faces expressing disgust in children with autism spectrum disorders: an exploratory study. Scientific Reports, 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.