

Abstract
Background:
Anorectal disorders are progressively increasing in the society. Out of many of the causes, some important are sedentary lifestyle, irregular and inappropriate diet, prolonged sitting or standing, and certain psychological disturbances. The prime cause of anorectal disorders is the instability of Jatharagni (digestive system), which further leads to constipation.
Aim and Objective:
To compare the efficacy of Apamarga Kshara application (AKA) and sclerotherapy (SCL) in the management of Arsha (1st and 2nd degree piles).
Materials and Methods:
In this study, 50 patients of Arsha (1st and 2nd degree piles) were selected and randomly allocated into two groups. In group AKA (n = 25), Apamarga Tikshna Kshara (alkaline of Achyranthes aspera linn.) application was done and in group SCL (n = 25), SCL was done in 1st and 2nd degree piles. The study was open prospective interventional clinical trial. Patients were assessed for relief in signs and symptoms at weekly interval for a month and another 1 month as follow-up period.
Results:
Patients of group SCL took more time than the patients of group AKA to get reduction in size of pile mass. In group SCL, maximum relief in bleeding as well as discharge per rectum was reported. AKA provided better results in ceasing the bleeding per rectum as well as reducing prolapse piles, than SCL.
Conclusion:
The study concluded that AKA is a effective procedure of choice for the management of 1st and 2nd degree internal piles as compared to SCL.
Keywords: Apamarga Kshara, Ayurveda, hemorrhoid, piles, sclerotherapy
Introduction
Arsha is one of the anorectal disorder mentioned in Ayurveda with four-fold treatment modality as per severity, and it is similar to piles as modern medicine. In regard to its management, Sushruta states four modalities, i.e., (i) Bhaishajya Chikitsa (palliative treatment), (ii) Kshara Karma (potential cauterization agent therapy), (iii) Agni Karma (direct cauterization agent therapy) and (iv) Shastra Karma (operation by sharp instrument).[1] Kshara is alkaline in nature derived from a combination of various herbs that is applied to the pile mass with the help of a special slit proctoscope.[2] Piles are dilated veins within the anal canal in the subepithelial province formed by radicals of the superior, middle, and inferior rectal veins and this condition is progressively increasing in the society day by day.[3] The etiological factors are usually linked with the prevalence of the ailment directly. Its incidence increases with advancing age, at least 50% of people over the age of 50 years have some degree of symptoms of hemorrhoid.[4] Sclerotherapy (SCL) is a medical procedure whereby a chemical, the sclerosant, is injected into a vein to entirely obliterate it. The sclerosant damages the innermost lining of the vessel, resulting in a clot that blocks the blood circulation in the vein beyond.[5]
This research was planned with the objective to find the individual and comparative effect of two therapies, i.e. Apamarga Kshara application (AKA) and SCL. This type of comparative study was not done before to establish the efficacy of Apamarga Kshara with modern standard procedure of SCL.
Materials and Methods
Selection of patients
The patients of piles were selected from outpatient department and inpatient department of Shalya Tantra of IPGT and RA Hospital, irrespective of their age, sex, religion, occupation etc. The selected patients were divided randomly into two groups by computerized randomization method (www.randomization.com). The study was initiated after approval of Institutional Ethics Committee, vide letter no. PGT/7/-A/Ethics/2016-17/2668 (dated November 16, 2016). This clinical trial was also registered, under Clinical Trials Registry, India (CTRI): CTRI Reg. No. CTRI/2017/04/008325, dated: October 4, 2017.
Diagnostic criteria
Patients having complaints of bleeding per rectum, discomfort/painful defecation, discharge per rectum and prolapse of pile mass per rectum were diagnosed as case of piles. Per rectal examination to assess the position and complication of piles as well as proctoscopy examination to assess the position, number and degree of piles was done thereafter.
Inclusion criteria
Patients belonging to age group of 18 years to 65 years were included in this study. Patients who were suffering from 1st and 2nd degree internal piles having with Mridu, Prastruta, Avagadha and Uchritani (soft, deep seated and elevated piles) type of piles were included.
Exclusion criteria
Patient of age <18 and >65 years, having 3rd and 4th degree piles were excluded; rectal prolapse, hemorrhoid associated with fissure, and fistula-in-ano were also excluded. Patient having uncontrolled hypertension, diabetes mellitus, cardiac disorders, malignancy of any organ, pregnant women, hepatitis B, tuberculosis, human immune-virus (HIV) and venereal disease research laboratory (VDRL)-positive cases were excluded.
Laboratory investigation
The routine hematological, biochemical, and microbiological investigation were carried out to assess the patient for physical fitness and exclude any other pathology which was not suitable from the management point of view before the treatment such as hematological tests: total white blood cell, neutrophils, lymphocytes, eosinophils, monocytes, basophils, hemoglobin, packed cell volume, erythrocyte sedimentation rate, red blood cell count, platelet count, bleeding time and clotting time; biochemistry: random blood sugar, blood urea, serum creatinine, serum bilirubin, serum glutamic pyruvic transaminase and serum glutamic oxaloacetic transaminase; and microbiology: HIV, hepatitis B surface antigen, and VDRL.
Materials
After confirming the diagnosis, selected 50 patients were randomly categorized by computer generated randomization into 2 groups. Group A–AKA Group (n = 25): in which patients were subjected for AKA procedure for one to three sitting (as per requirement) at minimum 7 days’ interval. Group B–SCL Group (n = 25): in which patients were subjected for SCL procedure one to three sitting (as per requirement) at minimum 15 days’ interval.
Methodology
Preoperative procedure for both groups
Informed written consent of all patients was taken before procedure and perianal part was prepared.
Half an hour before the procedure, proctolysis enema was given. Injection tetanus toxoid (0.5 ml) was given intramuscularly.
Procedure of Apamarga Kshara application
In lithotomy position, after painting and draping, pile masses were visualized and reassessed for their number, position and size. With proctoscope, one pile mass at a time was selected for Kshara application. First, the pile mass was cleaned with normal saline and dried with dry gauze piece. Kshara was applied on the pile mass with the help of spatula. As soon as Kshara was applied, the opening of proctoscope was covered by cotton swab to prevent direct air contact so that Kshara can work faster and was kept till Pakva Jambu Phala color (violet) was observed, Kshara was washed out with lime juice, and the anal canal was cleaned. 10 ml of Jatyadi oil (Matra Basti) was pushed inside the anal canal for lubrication as well as to prevent burning sensation. Thereafter bandage was done.
Procedure of Sclerotherapy
In lithotomy position after painting and draping, pile masses were visualized, and after that, number and position of pile masses were reassessed by proctoscopic examination. The slit proctoscope was inserted and piles were inspected and confirmed. Injection polidocanol (ASKLEROL 3%) solution was injected through a very fine needle (20 G) directly into the mucosa of vein. The number of pile mass injected in one session depended on the size and location of the pile mass.
Postoperative procedure for both groups
After 2 h of procedure patients were allowed to start with sips of water and liquid diet. Evening onward, patients were advised for sitz bath with Panchavalkala decoction up to 5 min at one sitting. Patient was also advised to take Eranda Bhrishta Haritaki 5 g powder at bed time with warm water. Triphala Guggulu tablet, two tablets of 500 mg each thrice a day after meal with warm water for 15 days was also given.
Do’s and don’t
Patients were advised to consume fiber-rich diet, green vegetables, plenty of water and butter milk. Patients were advised to avoid spicy, non-vegetarian diet, oily, junk and packed foods. A daily morning/evening walk for half an hour was also advised.
Assessment criteria
Effect was assessed weekly up to 4 week for reduction in intensity of bleeding per rectum, painful defecation, prolapse of piles and mucous discharge per rectum based on gradations as shown in Table 1.
Table 1.
Assessment of effect of therapy in group-AKA (Apamarga Kshara application): (n=25)
| Symptom | Time period | Mean | Mean diff. | % Relief | Z | W | SD | SE | P | Significance | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| BT | AT | ||||||||||
| Bleeding per rectum | 7th day | 2 | 0.44 | 1.56 | 78 | -4.51 | -325 | 0.50 | 0.10 | <0.001 | HS |
| 14th day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| 21st day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| 28th day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| Painful defecation | 7th day | 1 | 0.16 | 0.84 | 84 | -4.58 | -231 | 0.37 | 0.07 | <0.001 | HS |
| 14th day | 1 | 0.08 | 0.92 | 92 | -4.79 | -276 | 0.27 | 0.05 | <0.001 | HS | |
| 21st day | 1 | 0.04 | 0.96 | 96 | -4.89 | -300 | 0.20 | 0.04 | <0.001 | HS | |
| 28th day | 1 | 0.04 | 0.96 | 96 | -4.89 | -300 | 0.20 | 0.04 | <0.001 | HS | |
| Prolapse of piles | 7th day | 2 | 0.68 | 1.32 | 66 | -4.56 | -325 | 0.47 | 0.09 | <0.001 | HS |
| 14th day | 2 | 0.08 | 1.92 | 96 | -4.83 | -325 | 0.27 | 0.05 | <0.001 | HS | |
| 21st day | 2 | 0.04 | 1.96 | 98 | -4.91 | -325 | 0.20 | 0.04 | <0.001 | HS | |
| 28th day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| Discharge per rectum | 7th day | 0.12 | 0.04 | 0.08 | 66.67 | -1.41 | -3.00 | 0.20 | 0.04 | 0.500 | NS |
| 14th day | 0.12 | 0.00 | 012 | 100 | -1.73 | -6.00 | 0.00 | 0.00 | 0.250 | NS | |
| 21st day | 0.12 | 0.00 | 0.12 | 100 | -1.73 | -6.00 | 0.00 | 0.00 | 0.250 | NS | |
| 28th day | 0.12 | 0.00 | 0.12 | 100 | -1.73 | -6.00 | 0.00 | 0.00 | 0.250 | NS | |
| Size of piles | 7th day | 2 | 1.16 | 0.84 | 42 | -4.58 | -231 | 0.37 | 0.07 | <0.001 | HS |
| 14th day | 2 | 0.56 | 1.44 | 72 | -4.51 | -325 | 0.50 | 0.10 | <0.001 | HS | |
| 21st day | 2 | 0.08 | 1.92 | 96 | -4.83 | -325 | 0.27 | 0.05 | <0.001 | HS | |
| 28th day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
BT: Before Treatment, AT: After Treatment , Z: Z-test W: Wilcoxon signed rank test, SD: Standard Deviation, SE: Standard Error, P: Probability, HS: Highly Significant, NS: Non Significant
Follow-up period
After completion of the treatment, patients were asked for followup to observe reoccurrence or any other complications due to treatment.
Statistical analysis
Statistical tests such as the Wilcoxon signed-rank test was applied to the nonparametric statistical data for evaluating the difference in the before treatment and after treatment as well as weekly treatment follow-up. The Kruskal–Wallis sum test was applied to nonparametric statistical data for evaluation of difference between two groups.
Observations
Among 50 patients, maximum 58% patients belonged to the age group of 18–35 years. About 96% patients were male whereas maximum 38% patients were having job of prolong sitting or standing in nature while 64% patients were living in rural area. 80% of the patients were not having previous history of piles. Forty-two percent of patients were having habit of tobacco chewing which leads to improper digestion, Agnimandya (poor digestive power) and constipation which are the main causes of Arsha.[6] Sixty-four percent patients were noted with regular bowel habit with semisolid consistency of stool (60%).
On local examination, maximum 72% patients were having bleeding per rectum in which severe bleeding in 75%, syringing manner of bleeding in 80.55%, bleeding before defecation in 50%, and after defecation in 44.44% of patients was found. 80% patients were having prolapse of piles but 90% patients were having spontaneous reduction of prolapse of piles. Among 50 patients, a total of 103 piles mass were noted with equal distribution at 7, 3 and 11 o’clock, respectively, in which maximum 82% patients were suffering with 2nd degree piles. Seventy percent patients reported painful defecation, whereas 30% patients were having painless defecation. Maximum 40% patients had burning type of pain and 66.66% had moderate degree of pain. Discharge per rectum was found in negligible patients.
Results and Discussion
Arsha Roga and its management has been a challenge for physicians of all the system of medicines. Sushruta and Charaka contributed separate chapter on Arsha and included in the list of grave disease.[7,8]
After AKA, bleeding per rectum stopped completely in second week while after SCL, bleeding per rectum completely stopped in 3rd week [Table 2], which was highly significant (P < 0.001) [Table 3]. Early cessation of bleeding might had happened due to the properties of Kshara such as Stambhana (astringent/styptic), Pachana (digestion), and Dahana (cauterizing) resulting in hemostasis.[3] After Kshara application, the mucosa burns and strips to the wall; so, bleeding stops. In SCL, direct intravascular coagulation takes time; hence, it takes some time to stop the bleeding. This happens due to sclerosing agent that locally damages the endothelium of blood vessels which achieve hemostasis.[9] Bleeding is the cardinal sign of internal piles. In classic, bleeding is one of the leading symptoms in 1st and 2nd degree piles.[10] 80.55% of patients had bleeding in syringing manner. Syringing type of bleeding is due to laceration of the mucosa of engorged hemorrhoidal plexus.[11]
Table 2.
Assessment of effect of therapy in group-SCL (sclerotherapy): (n=25)
| Symptom | Time period | Mean | Mean diff. | % Relief | Z | W | SD | SE | P | Significance | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| BT | AT | ||||||||||
| Bleeding per rectum | 7th day | 2 | 0.68 | 1.32 | 66 | -4.14 | -231 | 0.74 | 0.14 | <0.001 | HS |
| 14th day | 2 | 0.52 | 1.48 | 74 | -4-50 | -325 | 0.50 | 0.10 | <0.001 | HS | |
| 21st day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| 28th day | 2 | 0.00 | 2.00 | 100 | -5.00 | -325 | 0.00 | 0.00 | <0.001 | HS | |
| Painful defecation | 7th day | 1 | 0.68 | 0.32 | 32 | -2.00 | -68 | 0.74 | 0.14 | <0.008 | S |
| 14th day | 1 | 0.52 | 0.48 | 48 | -3.46 | -78 | 0.50 | 0.10 | <0.001 | HS | |
| 21st day | 1 | 0.16 | 0.84 | 84 | -4.58 | -231 | 0.37 | 0.07 | <0.001 | HS | |
| 28th day | 1 | 0.08 | 0.92 | 92 | -4.79 | -276 | 0.27 | 0.05 | <0.001 | HS | |
| Prolapse of piles | 7th day | 2 | 1.36 | 0.64 | 32 | -4.00 | -136 | 0.48 | 0.09 | <0.001 | HS |
| 14th day | 2 | 0.84 | 1.16 | 58 | -4.71 | -325 | 0.37 | 0.07 | <0.001 | HS | |
| 21st day | 2 | 0.68 | 1.32 | 66 | -4.56 | -325 | 0.47 | 0.09 | <0.001 | HS | |
| 28th day | 2 | 0.16 | 1.84 | 92 | -4.71 | -325 | 0.37 | 0.07 | <0.001 | HS | |
| Discharge per rectum | 7th day | 0.8 | 0.16 | 0.64 | 80 | -3.17 | -78 | 0.37 | 0.07 | <0.001 | HS |
| 14th day | 0.8 | 0.00 | 0.8 | 100 | -3.17 | -78 | 0.00 | 0.00 | <0.001 | HS | |
| 21st day | 0.8 | 0.00 | 0.8 | 100 | -3.17 | -78 | 0.00 | 0.00 | <0.001 | HS | |
| 28th day | 0.8 | 0.00 | 0.8 | 100 | -3.17 | -78 | 0.00 | 0.00 | <0.001 | HS | |
| Size of piles | 7th day | 2 | 1.64 | 0.36 | 18 | -3.00 | -45 | 0.48 | 0.09 | <0.004 | S |
| 14th day | 2 | 1.16 | 0.84 | 42 | -4.58 | -231 | 0.37 | 0.07 | <0.001 | HS | |
| 21st day | 2 | 0.68 | 1.32 | 66 | -4.56 | -325 | 0.47 | 0.09 | <0.001 | HS | |
| 28th day | 2 | 0.12 | 1.88 | 94 | -4.77 | -325 | 0.33 | 0.06 | <0.001 | HS | |
BT: Before Treatment, AT: After Treatment, Z: Z-test W: Wilcoxon signed rank test, SD: Standard Deviation, SE: Standard Error, P: Probability, HS: Highly Significant, S: Significant
Table 3.
Comparison of results of Apamarga Kshara application (AKA) and group-SCL (sclerotherapy): (n=50)
| Symptom | Time period | Mean | Mean Diff. | % Relief | W | P | Significance | ||
|---|---|---|---|---|---|---|---|---|---|
| AKA | SCL | AKA | SCL | ||||||
| Bleeding per rectum | 7th day | 1.56 | 1.32 | 0.24 | 78 | 66 | 265.5 | 0.312 | NS |
| 14th day | 2 | 1.48 | 0.52 | 100 | 74 | 150 | <0.001 | HS | |
| 21st day | 2 | 2 | 00 | 100 | 100 | 312 | <0.001 | HS | |
| 28th day | 2 | 2 | 00 | 100 | 100 | 312 | <0.001 | HS | |
| Painful defecation | 7th day | 0.84 | 0.32 | 0.52 | 84 | 32 | 192 | 0.005 | HS |
| 14th day | 0.92 | 0.48 | 0.44 | 92 | 48 | 175 | <0.001 | HS | |
| 21st day | 0.96 | 0.84 | 0.12 | 96 | 84 | 275 | 0.167 | NS | |
| 28th day | 0.96 | 0.92 | 0.04 | 96 | 92 | 300 | 0.571 | NS | |
| Prolapse of piles | 7th day | 1.32 | 0.64 | 0.68 | 66 | 32 | 136 | <0.001 | HS |
| 14th day | 1.92 | 1.16 | 0.76 | 96 | 58 | 75 | <0.001 | HS | |
| 21st day | 1.96 | 1.32 | 0.64 | 98 | 66 | 112.5 | <0.001 | HS | |
| 28th day | 2 | 1.84 | 0.16 | 100 | 92 | 262.5 | 0.041 | HS | |
| Discharge per rectum | 7th day | 0.08 | 0.64 | 0.56 | 66.67 | 80 | 441.5 | 0.002 | HS |
| 14th day | 0.12 | 0.8 | 0.68 | 100 | 100 | 437 | 0.003 | HS | |
| 21st day | 0.12 | 0.8 | 0.68 | 100 | 100 | 437 | 0.003 | HS | |
| 28th day | 0.12 | 0.8 | 0.68 | 100 | 100 | 437 | 0.003 | HS | |
| Size of piles | 7th day | 0.84 | 0.36 | 0.48 | 42 | 18 | 162.5 | <0.001 | HS |
| 14th day | 1.44 | 0.84 | 0.6 | 72 | 42 | 147 | <0.001 | HS | |
| 21st day | 1.92 | 1.32 | 0.6 | 96 | 66 | 125 | <0.001 | HS | |
| 28th day | 2 | 1.88 | 0.12 | 100 | 94 | 275 | 0.081 | NS | |
AKA: Apamarga Kshara application, SCL: Sclerotherrapy, W: Wilcoxon signed rank test, P: Probability, HS: Highly Significant, NS: Non Significant
It was observed that in Group AKA, relief in pain was noted on the 7th day onwards to 84%, followed by 92% relief on 14th day and 96% on 21st day as well as 28th day. Pain was relieved due to reduction in congestion and due to Ksharana (alkaline), Pachana (digestion), Amahara (anti-infammatory) and Tridoshahara (pacification of Tridosha) properties of Apamarga Kshara. In group SCL, it was observed that the relief in pain of 32% was noted on the 7th day, 48% on 14th day, 84% on 21st day and 92% on 28th day. This might be due to the fact that it first induces endothelial damage, which causes platelets to aggregate at the site of damage and attach to the venous wall. Then, a dense network of platelets, cellular debris, and fibrin occludes the vessel. This process of change in the tissue takes more time than local Kshara application. Statistically highly significant, relief in painful deafecation during all time period in group AKA and group SCL (P < 0.001) except significant on 7th day in group SCL (P < 0.008) was reported.
In patients of group AKA, 66%, 96%, 98%, and 100% improvement was observed on 7th, 14th, 21st and 28th days, respectively in prolapse of pile mass. It might have reduced due to Vilayana (liquefaction), Shodhana (purification), Shoshana (absorption), and Lekhana (curetting) properties of Kshara.[12] In group SCL, reduction in prolapse was 32% on the 7th day, 58% on 14th day, 66% on 21st day, and 92% on 28th day [Table 2]. This might be due to injection of the sclerosnt solution in engorged veins that cause immediate shrink; hence do not bulge out much into the anal canal. Highly significant effect was found on prolapse of piles during all time period in group AKA and group SCL (P < 0.001). In 1st degree of piles only mild dilatation of hemorrhoidal veins is noted while in 2nd degree, prolapse of piles is found which is self-reducible.[11]
It is observed that in Group AKA, discharge per rectum was reduced on the 7th day onwards by 66.6%, followed by 100% maintaining the condition on 14th day, 21st day and 28th day. Discharge per rectum may have been tackled due to Shoshana (absorption), Tikshana (curetting), Stambhana (styptic), and Dahana (cauterizing) properties of Apamarga Kshara. In group SCL, it was observed that in reducing discharge per rectum, 80% result was noted on the 7th day, 100% improvement on 14th day, on 21st day as well as 28th day [Table 2]. It might be due to the fact that sclerosant solution causes the target vein to immediately shrink and then dissolve over a period of weeks as the body naturally absorbs the treated vein; hence, discharge may have subsided after procedure. Statistically, in significant reduction in discharge per rectum during all time period in group AKA (P < 0.250) and highly significant in group SCL (P < 0.001) was found.
In group AKA, 42% reduction of size of pile was noted on the 7th day, 72% on 14th day, 96% on 21st day and 100% reduction of size of piles on 28th day. Size of pile mass might have reduced due to Vilayana, Shodhana, Shoshana and Lekhana properties of Kshara [Figure 1]. In group SCL, the reduction of size of piles was 18%, 44%, 66% and 94% on 7th, 14th, 21st and 28th days, respectively. This might be due to injection of the sclerosing solution which produce sclerosant damage of endothelial (endosclerosis) that causes endofibrosis which results in the reduction in size of pile mass. Statistically, highly significant reduction on pile size mass was found during all time period in group AKA and group SCL (P < 0.001) but only significant in 7th day in group SCL (P < 0.004).
Figure 1.

(a) Photograph of piles before and after treatment. (b) Apamarga Kshara applied on the piles. (c) Pakva Jambu Phala changes obtained. (d) 2nd day of Kshara Karma. (e) 5th day of Kshara Karma. (f) 7th day of Kshara Karma. (g) After 15th day of Kshara Karma (AT). (h) Trolley for Kshara Karma
In 50 patients, a total of 103 piles were noted during P/S examination; among them, almost equal percentage was observed at 3, 7 and 11 o’clock position. This arrangement attributes to the termination of superior rectal artery which divides into right and left main branches. The left branch continues as a single vessel and terminates at 3 o’clock, whereas the right branch further divides into two branches – one terminates at 11 o’clock (anterior branch) and the other terminates at 7 o’clock (posterior branch). Hence, the chances of development of primary pile masses at 3, 7 and 11 o’clock positions are more. These findings support the classical description of position of piles.[13] It was found that maximum, i.e. 82% patients had of 2nd degree piles. It suggests that patients generally visit hospital when they feel that something protruding out of anus during defecation. Overall effect of AKA was better as compared to the SCL in the management of Abhyantara Arsha (1st and 2nd degree internal piles) [Figure 2].
Figure 2.
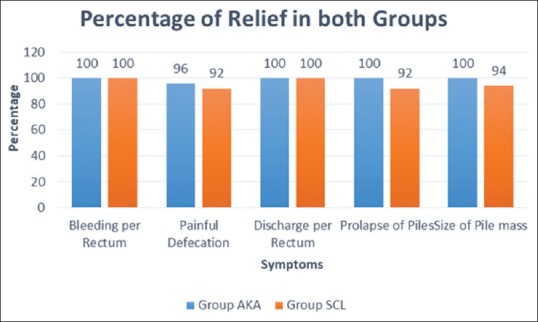
Overall effect of Apamarga Kshara application (AKA) and sclerotherapy (SCL) groups
Overall effect of the therapies showed that out of 50 patients in group AKA, 96% of patients were cured, while in 04% of patient, marked improvement was noted. In group SCL, it was noted that 76% of patients were cured, 12% of them were noted to have marked improvement and 12% of patients achieved moderate improvement [Tables 3 and 4]. After completion of the treatment of 1–3 setting and observation for 4 weeks, the follow-up was done for 1 month in both group, and during that period, a total of three patients (06%) had recurrence (in group AKA – 1 patient and in group SCL – 2 patients) of symptoms and two patients (02%) had complication; among them, one patient had per rectum bleeding in group AKA and one patient (02%) had pain in ano in group SCL.
Table 4.
Overall effect in Apamarga Kshara application (AKA) and group-SCL (sclerotherapy): (n=50)
| Overall Result | Group-AKA (n=25) | Group-SCL (n=25) | Total (n=50) | Total % | ||
|---|---|---|---|---|---|---|
| No. of patient | % | No. of patient | % | |||
| Complete remission | 24 | 96% | 19 | 76% | 43 | 86% |
| Marked improvement | 01 | 4% | 03 | 12% | 04 | 08% |
| Moderate improvement | 00 | 0% | 03 | 12% | 03 | 06% |
| Mild improvement | 00 | 0% | 00 | 00% | 00 | 00% |
| Unchanged | 00 | 0% | 00 | 0% | 00 | 00% |
| Total | 25 | 100 | 25 | 100 | 50 | 100% |
AKA: Apamarga Kshara Application, SCL: Sclerotherapy
Probable mode of action of Apamarga Kshara application
Apamarga Kshara exerts many actions such as incision, excision debridement, scrapping and dissolution simultaneously to cure the disease.[14,15]
Apamarga Kshara generally contain sodium, potassium, carbonate, calcium oxide, magnesium and silica. In Kshara preparation with process, when so many substances come in contact with each other, some of them get decomposed and few new substances are formed. For Ksharana (alkalinity), strength is more dependent on the formation of hydroxides than that of the carbonates. It means Kshara having more hydroxides are having more ability to produce alkaline condition. Proportion of hydroxides can be increased in Kshara by the addition of lime stone, conch shell, etc. These are added by heating and dissolving in the water, by which chemical reaction is set up in Kshara, the outcome of which is the transformation of some of them into carbonates.[16]
The mode of action starts immediately after application of Kshara on the tissue of piles. Kshara penetrates into the mucosal layer of lesion and destroys the tissue due to chemical cauterization property of Kshara. Kshara coagulates the protein of tissue which in fact causes the local necrosis of pile mass, and ultimately, the necrosed tissue leads to fibrosis and thus controls engorgement by fixing the mucosa. The chance of infection does not occur due to antibacterial action of Kshara.[17]
Probable mode of action of Sclerotherapy
The sclerosing agent induces a controlled inflammatory response. The inflammatory response is a result of cell damage with fibroblast proliferation that leads to sclerosis. In addition to fibrosis, agents may produce other effects such as thrombosis, extraction of proteins from lipids, denaturation of proteins, cell dehydration by osmosis, and physical obstruction by polymerization. The result of these processes is controlled disruption of the targeted tissues’ biologic function. Literature shows that the endothelium can be affected within seconds and irreversible damage in minutes.[18]
Conclusion
It was concluded from the clinical trial that Apamarga Kshara application (AKA) is a better choice for the management of 1st and 2nd degree internal piles as compared to sclerotherapy (SCL). Study on large sample size should be performed to generate more data regarding the efficacy of AKA. Kshara injection may be innovated with collaboration of modern pharmaceutical laboratory and compared with SCL.
Declaration of patient consent
The authors certify that they have obtained patient consent for images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Johanson JF, Rimm A. Optimal nonsurgical treatment of hemorrhoids: A comparative analysis of infrared coagulation, rubber band ligation, and injection sclerotherapy. Am J Gastroenterol. 1992;87:1600–6. [PubMed] [Google Scholar]
- 2.Acharya YT, Acharya NR. Sushruta Samhita of Sushruta, Sthana Chikitsa. Ch. 6, Ver. 4. Reprint edition. Varanasi: Chokhambha Sanskrita Sansthan; 2013. p. 430. [Google Scholar]
- 3.Shah B, Dudhamal TS, Prasad S. Efficacy of Kshara application in the management of internal haemorrhoids –A pilot study. J US China Med Sci. 2016;13:169–73. [Google Scholar]
- 4.Goligher J. Surgery of the Anus, Rectum and Colon Vol. 1. Ch. 4. 5th edition. New Delhi: A.I.T.B.S. Publishers &Distributers; 2002. p. 98. [Google Scholar]
- 5.Shah B, Dudhamal TS. Integrated approach in diagnosis of Ano-rectal (guda) diseases: A review. Int J Res Ayurveda Pharm. 2017;8(Suppl 3):72–6. [Google Scholar]
- 6.McGrath DS, Meitner A, Sears CR. The specificity of attentional biases by type of gambling: An eye-tracking study. PLoS One. 2018;13:e0190614. doi: 10.1371/journal.pone.0190614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ambikadutta S, editor. Sushruta Samhita of Sushruta, Sutra Sthana Sharira Sthana. Ch. 4, Ver. 26. Reprint Edition. Varanasi: Chaukhambha Sanskrit Santhan; 2014. p. 41. [Google Scholar]
- 8.Brahmanand T, editor. Charak Samhita of Agnivesha, Sharira Sthana Vol. 1. Ch. 7, Ver. 9. Reprint Edition. Varansi: Chaukhamba Surbharati Prakashan; 2012. p. 924. [Google Scholar]
- 9.Nijhawan S, Udawat H, Gupta G, Sharma A, Mathur A, Sapra B, et al. Flexible video-endsocopic injection sclerotherapy for second and third degree internal hemorrhoids. J Dig Endosc. 2011;2:1. [Google Scholar]
- 10.Kumar PH. Recent Trends in the Management of Arsha/Haemorrhoids. 2nd edition. Ch. 1. New Delhi: Chokhambha Sanskrita Pratishthan; 2011. p. 39. [Google Scholar]
- 11.Goligher J, Duthie H, Nixon H. Surgery of the Anus, Rectum and Colon. 5th Edition. Vol. 1. New Delhi: A.I.T.B.S. Publishers and Distributors; 2004. pp. 98–105. [Google Scholar]
- 12.Prasad L, Prakash S, Prakash A. Colorectal Diseases and Kshara Sutra Surgery. Ch. 5. 1st edition. New Delhi: Global Medika Health Science Publisher; 2013. p. 75. [Google Scholar]
- 13.Keighley MR, Williams NS. Surgery of the Anus, Rectum &Colon. 3rd edition. Vol. 1. China: Elsevier Limited; 2008. p. 454. [Google Scholar]
- 14.Sudarmi K, Dudhamal TS. Comparative clinical study of Apamarga kshara application, infrared coagulation and Arshohara vati in the management of Arsha (1st and 2nd degree hemorrhoids) Ayu. 2017;38:122–6. doi: 10.4103/ayu.AYU_94_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Acharya YT, Acharya NR, editors. Sushruta Samhita, Chikitsa Sthana. Ch. 6, Ver. 4. Reprint Edition. Varanasi: Chokhambha Sanskrita Sansthan; 2008. p. 430. [Google Scholar]
- 16.Ravishankar AG, Prashanth BK. Pratisaraneeya Kshara- a potent weapon against Dushtavrana. Int Ayu Med J. 2013;1:1–7. [Google Scholar]
- 17.Shah B, Harisha CR, Dudhamal TS. Pharmacognostical studies of Apamarga (Achyranthes aspera linn.) and its Tikshnakshara. Int J Curr Med Pharm Res. 2018;4:3152–6. [Google Scholar]
- 18.Nijhawan S, Udawat H, Gupta G, Sharma A, Mathur A, Sapra B, et al. Flexible video-endsocopic injection sclerotherapy for second and third degree internal hemorrhoids. J Dig Endosc. 2011;2:1. [Google Scholar]