

Supplemental Digital Content is available in the text
Keywords: efficacy, elderly, feasibility, non-small cell lung cancer (NSCLC), open thoracotomy, safety
Abstract
This study aimed to compare the feasibility, efficacy and safety among uniport video assisted thoracoscopic surgery (U-VATS), multiport VATS (M-TATS), and open thoracotomy in elderly non-small cell lung cancer (NSCLC) patients at early stage.
One hundred ninety-one elderly NSCLC patients at early stage underwent U-VATS (N = 73), M-VATS (N = 56) or open thoracotomy (N = 62) were included. Perioperative parameters, short-term outcomes, postoperative complications, and overall survival (OS) were assessed.
Three-group analysis disclosed that operational duration, blood loss, drainage duration, hospital stay, pain score on the first day (D1) and D3, patients’ global assessment (PGA), lasing air leak, infection, arrhythmia, and cardio-cerebrovascular events incidences were different among U-VATS, M-VATS, and open thoracotomy groups. Subsequently, 2-group analysis revealed that:
-
1.
Pain score on D1 and D3 and PGA score were decreased in U-VATS group compared with M-VATS group;
-
2.
The operational duration was longer, blood loss, drainage duration, hospital stay, pain score on D1 and D3, PGA score, lasing air leak, infection, arrhythmia, and cardio-cerebrovascular events were decreased in U-VATS group than open thoracotomy group;
-
3.
The operational duration was longer, blood loss, drainage duration, hospital stay, pain score on D1 and D3, lasing air leak, infection, and arrhythmia were reduced in M-VATS group than open thoracotomy group.
In addition, there was no difference of OS among 3 groups, nor between any of the 2 groups.
U-VATS presents with elevated feasibility, non-inferior tolerance, and similar efficacy compared with M-VATS and open thoracotomy in the elderly NSCLC patients at early stage.
1. Introduction
Lung cancer, the dominant cause of cancer deaths worldwide and the most common and fatal cancer in China, has a prevalence of 44.7/100, 000 in developed area and 30.0/100, 000 in less developed areas in the world.[1,2] Non-small cell lung cancer (NSCLC) is the most frequently diagnosed lung cancer, which mainly contains squamous-cell carcinoma, large cell carcinoma and adenocarcinoma.[3] The early stage NSCLC patients account for approximately 35% of all NSCLC cases, and the elderly is the major population of early stage NSCLC patients, for whom thoracotomy is the first choice of treatment if the patient is clinically operable.[4,5]
Performing thoracotomy on the elderly NSCLC patients at early stage is rather complex due to that the surgeons have to consider more factors before operation, such as reduced performance status, inadequate liver or renal function, higher incidence of surgical complications and more comorbidities of the elderlies.[6,7] Open thoracotomy, broadly applied but presents with many complications in NSCLC patients, requires a more complete physical functions, which limited its applications in the elderly patients. Video assisted thoracoscopic surgery (VATS) has been established by mounting clinical trials and cohort studies on its practicability, tolerance and efficacy in early stage NSCLC patients, moreover, uniport VATS (U-VATS) has been reported to be more feasible than multiport VATS (M-VATS), including less blood loss, less postoperative drainage time and so on.[8–10] Nonetheless, despite that there are various advantages of VATS treatments, including U-VATS, and M-VATS, compared with open thoracotomy in early stage NSCLC patients, they have rarely been compared in the elderly NSCLC patients.
Herein, the aim of this study was to compare the feasibility, efficacy, and safety among U-VATS, M-VATS, and open thoracotomy in treating elderly NSCLC patients at early stage.
2. Materials and methods
2.1. Patients
From Jan 2013 to Dec 2015, 191 elderly patients with early stage NSCLC who underwent U-VATS, M-VATS, or open thoracotomy were included in this retrospective cohort study. The inclusion criteria were:
-
1.
postoperative pathological diagnosis of NSCLC;
-
2.
with TNM stage Ia or Ib;
-
3.
age ≥60 years old;
-
4.
underwent U-VATS, M-VATS, or open thoracotomy;
-
5.
clinical data, surgical information, short-term outcomes, and records of adverse events were complete and accessible.
The exclusion criteria included:
-
(1)
patients with TNM stage II-IV;
-
(2)
had a history of malignancies other than NSCLC;
-
(3)
without follow-up data or follow-up duration less than 1 year.
This study was approved by the Ethics Committee of The Second People's Hospital of Liaocheng. All patients or their guardians provided the written informed consents.
2.2. Baseline characteristics collection
Patients’ baseline characteristics were collected from medical records, which included:
-
(1)
demographics: age, gender, and BMI;
-
(2)
smoke status and complications: smoke, hypertension, diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), and cardiac disease;
-
(3)
tumor features: tumor location, histological type, tumor size, and TNM stage;
-
(4)
preoperative evaluation of pulmonary function: forced expiratory volume in 1 second (FEV1) and predicted FEV1.
2.3. Grouping and procedures
Patients were assigned to U-VATS group (N = 73), M-VATS group (N = 56), or open thoracotomy group (N = 62), respectively, according to the surgery they received. As for the U-VATS and M-VATS, all patients underwent intravenous combined general anesthesia in the lateral decubitus position with single lung ventilation using double lumen endotracheal intubation, and the operator and thoracoscopic assistant stood at the anterior side of the patient during all steps of the procedure.
-
1.
U-VATS: A 3 to 5 cm incision was performed in the fifth intercostal space in the anterior axillary line area without rib spreading, and a plastic wound protector was used for the operation port incision to avoid surgical site infection and tumor spread. Then a 30-degree, 10-mm high definition camera thoracoscope was introduced into the pleural cavity and maintained in the posterior part of the incision. The main procedures of lobectomy were as follows: firstly, adhesions were separated, inferior pulmonary ligament was dissociated, and the pleura of pulmonary hilar was opened, then the pulmonary vein, pulmonary artery, and bronchus were ligated and cut with an endoscopic stapler. Subsequently, a complete lymphadenectomy was carried out, which included stations 4L, 5, 6, 7, and 9 for left side cancers and stations 2R, 4R, 7, 8, and 9 for right side cancers. After resection, all specimens were placed in an endoscopic plastic bag under thoracoscopic assistance and removed through the operational incision. Finally, the chest was rinsed using normal saline, and the bleeding was examined. Single lung ventilation was changed to double lung ventilation, and expansion of lung lobe and leakage were checked. A closed thoracic drainage tube was inserted through the posterior border of the incision, which was removed depending on the drainage. The muscular layer and subcutaneous tissue around the drainage tube were carefully stitched.
-
2.
M-VATS: The operative incision consisted of 3 parts: operation port, observation port, and auxiliary operation port. A 4 to 5 cm incision was made in the fourth intercostal space in the anterior axillary line area and used as the utility port, and another two 1 to 2 cm incisions used as observation port and auxiliary operation port were made between the seventh and eighth intercostal space in the midaxillary line and posterior axillary line, respectively. A 10 mm thoracoscope was inserted into the observation port to perform intrathoracic exploration. During the operation, the latissimus dorsi was not cut off, and the serratus anterior was split along the muscle fibers without rib spreading. The procedures of lobectomy and lymphadenectomy were as same as U-VATS. All resected tumor specimens were removed from the chest using a retrieval bag. After operation, the thoracic cavity was cleaned up using normal saline, bleeding and leakage were examined, and a closed thoracic drainage tube was inserted through the observation port, reaching the apex of the thorax. Finally, the muscular layer and subcutaneous tissue were stitched.
-
3.
Open thoracotomy: Double lumen tracheal intubation, intravenous, and respiratory combined general anesthesia, single lung ventilation on the healthy side and routine disinfection were performed before operation. A traditional posterolateral incision about 15 to 30 cm in the chest was made, and the tumor size and invasion were identified. After dissociating the blood vessels (about 1–2 cm), the pulmonary vein, pulmonary artery and bronchus were ligated and cut off with an endoscopic stapler, and the underdeveloped pulmonary fissure was cut by the linear stapler. Lymphadenectomy was performed as same as U-VATS. Normal saline cleaning, bleeding and leakage examination were conducted after operation. A closed thoracic drainage tube was inserted at operated side between the seventh and eighth intercostal space in the midaxillary line, and for the patients who underwent radical resection of upper pulmonary carcinoma, another thoracic drainage tube was inserted at operated side in the second intercostal space in midline of clavicle.
2.4. Postoperative management
The postoperative pain was treated by intravenously administering 150 mL normal saline (0.9%), 50 μg sufentanil, 150 mg dezocine and 8 mg ondansetron hydrochloride for 48 hours according to pain visual analogy scale (VAS) score. Chest X-ray (CXR) was performed on the day of operation, on the first day after operation and after thoracic drainage tube removal before discharge. Thoracic drainage tube removal occurred with normal CXR findings, no air leak and secretions of less than 250 cc in 24 hours.
2.5. Operational and short-term assessments
Assessments of operations included operational duration (from incision to suturing the skin), blood loss, drainage duration (from the day of surgery to the day of drainage tube removal) and hospital stay; the short-term assessments included pain VAS score on the first day and third day after operation and patient global assessment (PGA) score on last day of hospitalization.
2.6. Safety and survival assessments
Postoperative complications were used to assess safeties of the operations, which included air leak, atrial fibrillation, atelectasis, bleeding, infection, arrhythmia, cardiovascular, and cerebrovascular events. After operation, patients were followed up regularly, and median follow-up duration was 33.0 months (range: 1.0–55.0 months). The overall survival (OS) was used to evaluate long-term outcome, which was defined as the duration from the time of operation to the time of patients’ death.
2.7. Statistical analysis
SPSS 22.0 software (IBM, USA) was applied for statistical analysis and graph making. Normal distributed continuous variables were presented as mean ± standard deviation, and comparison among three groups was determined by one-way ANOVA followed by Bonferroni test. Skewed distributed continuous variables were presented as median (25th–75th quantiles), comparison was determined by Kruskal–Wallis H rank sum test (among 3 groups) or Wilcoxon rank sum test (between 2 groups). Categorized variables were presented as count (percentage), and comparison was determined by Chi-square test, Yates corrected Chi-square test or Fisher exact test. Kaplan–Meier curve was used to show the survival profiles, and log-rank test was applied for comparison of OS among 3 groups. P value <.05 was considered as significant.
3. Results
3.1. Study flow
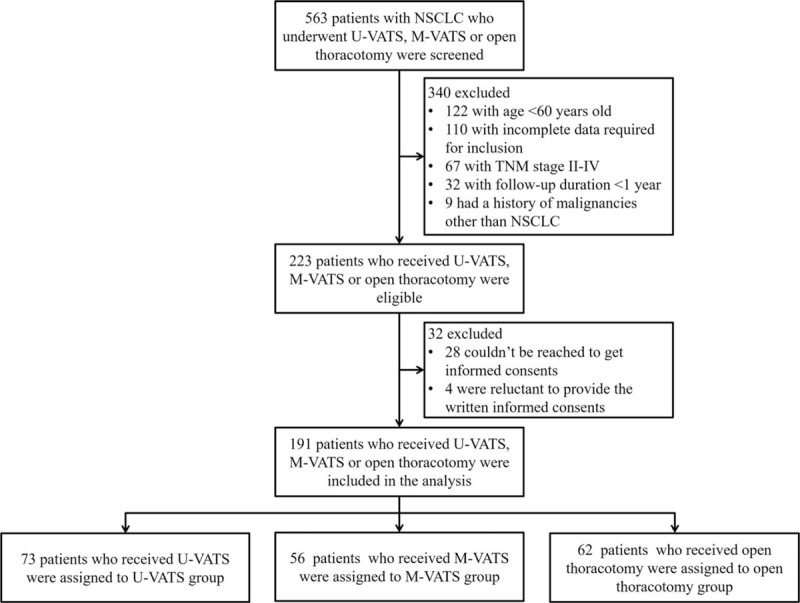
At the beginning of our study, 563 NSCLC patients who underwent U-VATS, M-VATS, or open thoracotomy were screened for eligibility, after which 340 patients were excluded because of the following reasons: age <60 years old (N = 122), incomplete data required for inclusion (N = 110), TNM stage II-IV (N = 67), follow-up duration <1 year (N = 32), history of malignancies other than NSCLC (N = 9) (Fig. 1). Therefore, the remaining 223 patients who received U-VATS, M-VATS, or open thoracotomy were eligible for our study, among whom 32 patients were excluded (28 could not be reached to get informed consents and 4 were reluctant to provide the written informed consents). And then the remaining 191 patients who received U-VATS, M-VATS, or open thoracotomy were included in the analysis, who were divided into U-VATS group (N = 73), M-VATS group (N = 56) and open thoracotomy group (N = 62) accordingly.
Figure 1.
OS comparison among 3 groups. There was no difference of OS in the elderly NSCLC patients at early stage among U-VATS group, M-VATS group, and open thoracotomy group, nor between any of the 2 groups. Kaplan–Meier curve was used to show the survival profiles, and log-rank test was applied for comparison of OS among 3 groups. P < .05 was considered significant. M-VATS = multiport video assisted thoracoscopic surgery, NSCLC = non-small cell lung cancer, OS = overall survival, U-VATS = uniport video assisted thoracoscopic surgery.
3.2. Baseline characteristics
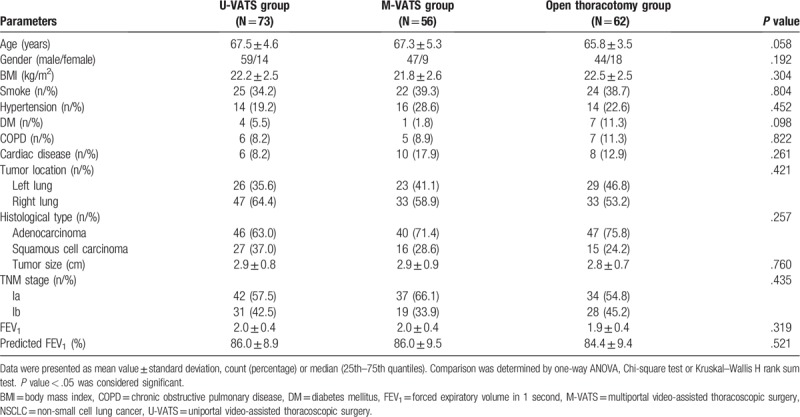
Mean values of age were 67.5 ± 4.6 years, 67.3 ± 5.3 years, and 65.8 ± 3.5 years in U-VATS group, M-VATS group, and open thoracotomy group, respectively (Table 1). And the male/female was 59/14 in U-VATS group, 47/9 in M-VATS group and 44/18 in open thoracotomy group. There was no difference among 3 groups in regard to all the baseline characteristics, including age (P = .058), gender (P = .192), BMI (P = .304), current smoke (P = .804), concomitant diseases (hypertension (P = .452), DM (P = .098), COPD (P = .822), cardiac disease (P = .261)), tumor location (P = .421), histological type (P = .257), tumor size (P = .760), TNM stage (P = .435), FEV1 (P = .319) and predicted FEV1 (P = .521). In addition, we observed that the mean value of age in open thoracotomy group was numerically reduced than those in U-VATS group and M-VATS group. The other clinical characteristics at baseline were displayed in Table 1.
Table 1.
Baseline characteristics of NSCLC patients in U-VATS group, M-VATS group, and open thoracotomy group.
3.3. Comparisons of perioperative parameters and short-term outcomes among 3 groups
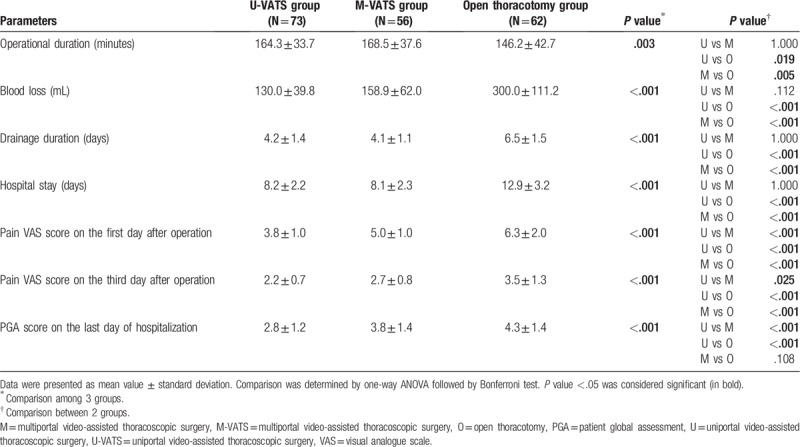
Perioperative parameters and short-term outcomes were compared among three groups, which disclosed that all the perioperative parameters and short-term outcomes were different among the three groups (all P < .05) (Table 2). Subsequently, further 2-group comparisons disclosed that:
Table 2.
Comparison of perioperative parameters and short-term outcomes among 3 groups.
-
1.
the pain VAS score on the first day after operation (P < .001), pain VAS score on the third day after operation (P = .025) and PGA score on the last day of hospitalization (P < .001) were declined in U-VATS group compared with M-VATS group;
-
2.
the operational duration was elevated (P = .019), while blood loss (P < .001), drainage duration (P < .001), hospital stay (P < .001), pain VAS score on the first day after operation (P < .001), pain VAS score on the third day after operation (P < .001) and PGA score on the last day of hospitalization (P < .001) were decreased in U-VATS group compared with open thoracotomy group;
-
3.
the operational duration was more prolonged (P = .005), however, blood loss (P < .001), drainage duration (P < .001), hospital stay (P < .001), pain VAS score on the first day after operation (P < .001) and pain VAS score on the third day after operation (P < .001) were reduced in M-VATS group than those in open thoracotomy group.
These results indicated that U-VATS and M-VATS were both better than open thoracotomy concerning feasibility, and U-VATS was superior to M-VATS in regard to postoperative pain and PGA score in the elderly NSCLC patients at early stage.
3.4. Comparisons of postoperative complications among the three groups
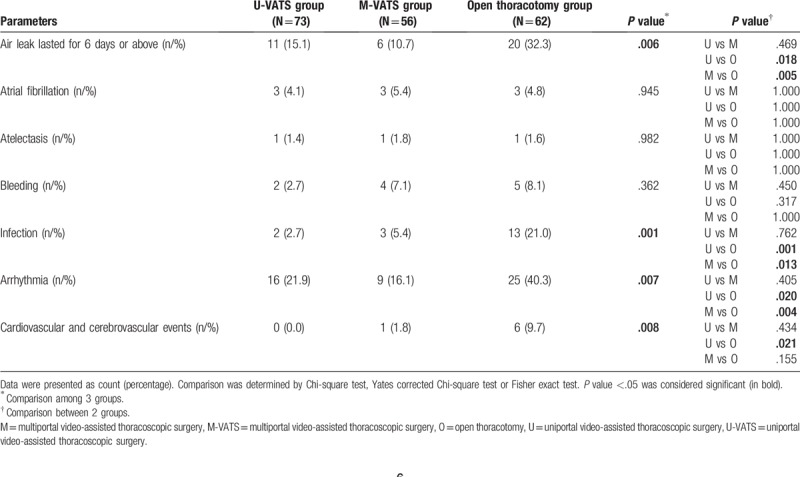
There were no difference in the incidences of atrial fibrillation (P = .945), atelectasis (P = .982) and bleeding (P = .362) among three groups, while the incidences of air leak lasted for 6 days or above (P = .006), infection (P = .001), arrhythmia (P = .007) and cardiovascular and cerebrovascular events (P = .008) were distinct among 3 groups (Table 3). Furthermore, the subsequent 2-group comparisons were performed, which displayed that:
Table 3.
Comparison of postoperative complications among 3 groups.
-
1.
there were no differences of all the postoperative complications incidences between U-VATS group and M-VATS group (all P > .05);
-
2.
the air leak lasted for 6 days or above (P = .018), infection (P = .001), arrhythmia (P = .020) and cardiovascular, and cerebrovascular events (P = .021) were less in U-VATS group than open thoracotomy group;
-
3.
the air leak lasted for 6 days or above (P = .005), infection (P = .013) and arrhythmia (P = .004) were also reduced in M-VATS group compared with open thoracotomy group.
And those results suggested that U-VATS was as tolerable as M-VATS in the elderly NSCLC patients at early stage, while they both caused less postoperative complications compared with open thoracotomy.
3.5. Comparison of OS among three groups
Kaplan–Meier curve and log-rank test were applied for OS comparison, which exhibited that there was no difference of OS among three groups (P = .327) (Fig. 2). Additionally, there was no difference of OS between U-VATS group and open thoracotomy group (P = .150), M-VATS group and open thoracotomy group (P = .525) or U-VATS group and M-VATS group (P = .327), either, which indicated that the survival profile of patients receiving U-VATS and M-VATS were not inferior to that of patients treated by open thoracotomy.
Figure 2.
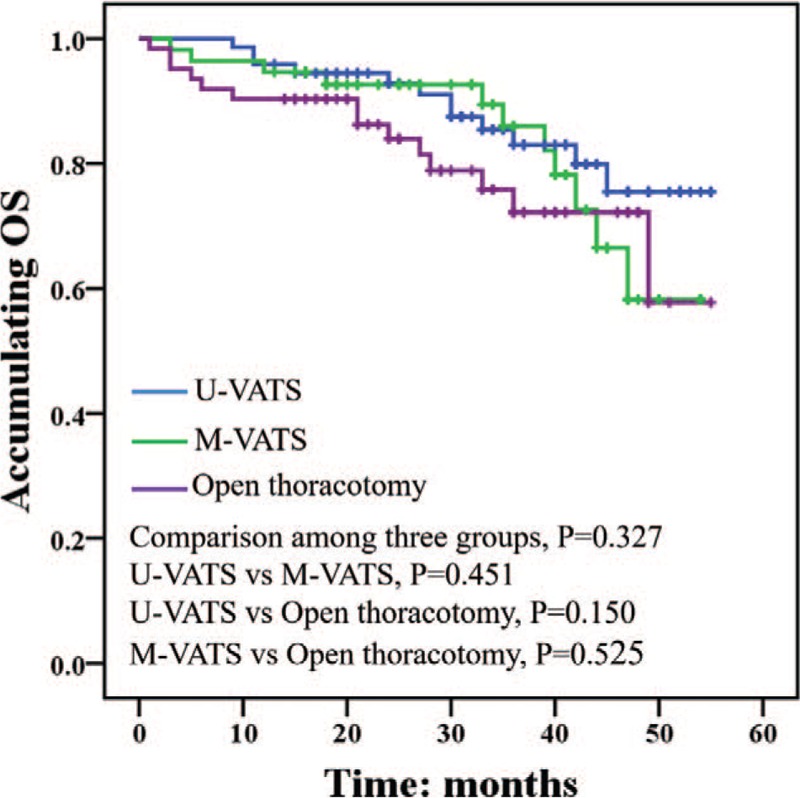
OS in patients receiving U-VATS, M-VATS, and open thoracotomy. No difference was observed among 3 groups or between any of the 2 groups. Kaplan–Meier curve was drawn to present the survival profiles, and log-rank test was utilized for comparison of OS among three groups or between 2 groups. P < .05 was considered significant. M-VATS = multiport-video assisted thoracoscopic surgery, OS = overall survival, U-VATS = uniport-video assisted thoracoscopic surgery.
3.6. Comparison of cause of deaths among 3 groups
There was no difference of number of deaths (P = .666) or the cause of deaths, which included cancer progression (P = .930), infection (P = .320), complications (P = .982), and unknown reason (P = .366), among the U-VATS, M-VATS and open thoracotomy groups (Supplementary Table 1).
4. Discussion
In this study, we discovered that:
-
1.
U-VATS presented with the best feasibility among the three thoracotomies;
-
2.
no difference concerning safety between U-VATS and M-VATS was observed, while both of them were more tolerable than open thoracotomy;
-
3.
there was no difference of efficacy among U-VATS, M-VATS, and open thoracotomy, nor between any of the 2 thoracotomies.
Perioperative parameters and short-term outcomes are crucial for feasibility assessment of thoracotomy in the elderly NSCLC patients, specifically for fragile elderly patients, however, the feasibility of VATS compared with open thoracotomy in the elderly NSCLC patients at early stage is still quite insufficient, and most of the studies are focusing on total NSCLC patients. For instance, a case control study with propensity score weighting-based analysis validates that NSCLC patients who receive VATS show notably shorter duration of hospital stay post operation compared with those receiving open thoracotomy.[11] And another study conducted illuminates that intraoperative blood loss and chest tube duration are less in NSCLC patients treated with VATS than those in patients treated by open thoracotomy.[12] And an earlier retrospective cohort study reports a much less blood loss in NSCLC patients receiving VATS compared with patients treated by open thoracotomy.[13] In our study, we found that except for operational duration, U-VATS and M-VATS were superior to open thoracotomy concerning blood loss, drainage duration, hospital stay, pain VAS score on the first and third day post operation, and the PGA score on the last day of hospitalization was also higher in patients treated by U-VATS than that in patients receiving open thoracotomy. Here are some possible explanations for these results:
-
1.
the operational duration were longer in U-VATS and M-VATS groups compared with that in open thoracotomy group, which may be derived from 2 reasons, firstly, U-VATS and M-VATS required more instruments and more complicated operation technique, which needed more time; secondly, open thoracotomy provided a broader view of the upper thoracic region anatomical structure, and surgeons were usually more skilled in the procedure of open thoracotomy, which largely reduced the operation time;
-
2.
technically, U-VATS and M-VATS were minimally invasive surgical operations, which caused smaller incision and diminished damage to the chest anatomical structure, while open thoracotomy needed a large incision and more damage to thorax, thereby U-VATS and M-VATS caused less blood vessel injury, smaller volume of intrathoracic liquid and gas, less need of post-operative care and less pain compared with open thoracotomy, which subsequently led to less blood loss, drainage duration, hospital stay and lower pain VAS score on the first and third day after operation;
-
3.
because of shorter drainage duration, hospital stay and less pain after operation, the elderly patients may experience less unsatisfactory after U-VATS and M-VATS compared with open thoracotomy, contributing to a higher PGA score on the last day of hospitalization.
VATS is initially designed as a single port thoracotomy, however, is firstly applied in a multiport way in clinical practice, namely the M-VATS. Nonetheless, due to that complications such as chest paresthesia are reported in NSCLC patients post M-VATS, the U-VATS is re-introduced in clinical practice to minimize the complications.[14] Since U-VATS was developed, there are various benefits of this surgery have been reported. A retrospective cohort study reveals that NSCLC patients present with less blood loss, reduced pain, and elevated VAS score of satisfaction after treatment by U-VATS than M-VATS.[15] And another study finds that the Numeric Rating scale (NRS) pain score is decreased in early stage NSCLC patients treated with U-VATS compared with M-VATS.[16] Partially in accordance with the previous studies, we found that the pain VAS score on the first and third day after operation as well as PGA score on the last day of hospitalization were lower in U-VATS group compared with M-VATS group. The probable explanations of these results are:
-
1.
pain post operation was related to the injury of intercostal nerves, which was less in U-VATS compared with M-VATS because of that the incision located at mid-axillary and posterior axillary line in M-VATS but not in U-VATS, furthermore, the pressure in intercostal nerve was also milder in U-VATS compared with M-VATS;
-
2.
comprehensively, U-VATS presented with less drainage duration, hospital stay and pain in the elderly NSCLC patients, moreover, the U-VATS resulted in very limited cosmetic appearance loss compared with M-VATS. Therefore, the elderly NSCLC patients presented with better global satisfaction after U-VATS than M-VATS.
The elderly NSCLC patients, although at early stage, often present with inadequate physical condition, therefore the elderly NSCLC patients more easily to develop complications after operation, thus, surgeons have to be very cautious before decision making and in dealing with the perioperative complications.[5] A study that analyzes patients undergoing lung resection elucidates that after propensity score matching, the major cardiopulmonary complication rate and overall complication rate in patients receiving VATS are reduced compared with patients who receive open thoracotomy.[17] A retrospective cohort study reports that the in-hospital mortality rate is markedly declined in patients with various lung diseases treated by VATS compared with that in patients treated by open thoracotomy.[18] These prior studies suggest that VATS may be more tolerable in patients with lung diseases including lung cancer than open thoracotomy. In our study, we found that incidence of air leak lasted for 6 days or above, infection or arrhythmia was decreased in the elderly NSCLC patients receiving U-VATS and M-VATS compared with patients treated by open thoracotomy, and less cardiovascular and cerebrovascular events were found in patients treated by U-VATS than that in patients receiving open thoracotomy, suggesting that U-VATS and M-VATS were more tolerable than open thoracotomy in the elderly NSCLC patients. The possible explanations might consist of:
(1) air leak and infection were closely related to destruction of thoracic anatomic structure, which was much milder in U-VATS and M-VATS than that in open thoracotomy;
(2) arrhythmia was usually caused by hypovolemia, cardiac damage, decrease in lung compliance and so on.[19] The hypovolemia might be the main reason for arrhythmia in the elderly NSCLC patients receiving thoracotomies in our study, and there was less blood loss of patients in U-VATS and M-VATS groups compared with open thoracotomy group, causing less hypovolemia and subsequently less cases with arrhythmia.
(3) Cardiovascular and cerebrovascular events: blood loss during operation, long time of lay in bed, pain and tension during and post operation may result in myocardial and cerebral ischemia, venous thrombus, increase of blood pressure and heart rate elevation, which were more severe in the open thoracotomy group compared with U-VATS group in our study. Therefore, the patients in the open thoracotomy group presented with more cardiovascular and cerebrovascular events than patients in the U-VATS group.
Studies that assess the survival profile of the elderly NSCLC patients who receive VATS and open thoracotomy are rare, and most of the reported studies are performed in total NSCLC patients, which display rather controversial results.[9,20–22] For example, a retrospective cohort study finds that NSCLC patients have better OS after VATS compared with open thoracotomy, and a similar 3-year survival rate while a higher 5-year survival rate are found in patients receiving VATS than patients treated by open thoracotomy as well.[20] And a study which analyze the data from an institutional registry including the profile between 2002 and 2012 validates that the 5-year survival rate and OS are better in patients with or suspected of lung cancer who are treated with VATS compared with open thoracotomy.[23] Another study that is conducted on stage Ia NSCLC patients reveals that the disease-free survival (DFS) and 5-year OS rate display no difference between patients treated with VATS and patients treated by open thoracotomy, which is in line with our study.[24] We found that there was no difference of OS among U-VATS, M-VATS, and open thoracotomy group, or between any of the 2 groups, suggesting that these different types of thoracotomies may be even in view of the survival in the elderly NSCLC patients at early stage. As for the explanations, it was probably because of the follow up time in our study was not long enough, or the sample size was relatively small.
In addition, there were several limitations in this study. First, the follow up time may be too short to observe the long-term efficacy, with the median follow up duration being only 33.0 months (range: 1.0–55.0 months). Second, VATS is a relatively complicated thoracotomy that demands the surgeon to be more skilled and familiar to the surgery process, thus the surgeons’ skill level might cause bias of our results. Third, the sample size was relatively small, which reduced the statistical power to some extent. Forth, as an observational study, there might be several baseline characteristics that are confounding factors in this study.
In conclusion, U-VATS presents with elevated feasibility, non-inferior tolerance, and similar efficacy compared with M-VATS and open thoracotomy in the elderly NSCLC patients at early stage.
Author contributions
Conceptualization: Siqiang Cheng.
Formal analysis: Ruixing Zhao.
Methodology: Ruixing Zhao.
Supervision: Zhihua Shi.
Validation: Zhihua Shi.
Writing – original draft: Ruixing Zhao.
Writing – review & editing: Siqiang Cheng.
Siqiang Cheng orcid: 0000-0002-5902-2285.
Supplementary Material
Footnotes
Abbreviations: COPD = chronic obstructive pulmonary disease, CXR = chest X-ray, DM = diabetes mellitus, FEV1 = forced expiratory volume in 1 second, M-VATS = more feasible than multiport VATS, NSCLC = non-small cell lung cancer, OS = overall survival, PGA = patient global assessment, U-VATS = uniport VATS, VAS = visual analogy scale, VATS = video assisted thoracoscopic surgery.
The authors have no funding and conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87–108. [DOI] [PubMed] [Google Scholar]
- [2].Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115–32. [DOI] [PubMed] [Google Scholar]
- [3].Travis WD, Brambilla E, Burke AP, et al. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th edition.Geneva: World Health Organization; 2015. [DOI] [PubMed] [Google Scholar]
- [4].Bakirhan K, Sharma J, Perez-Soler R, et al. Medical treatment in elderly patients with non-small cell lung cancer. Curr Treat Options Oncol 2016;17:13. [DOI] [PubMed] [Google Scholar]
- [5].Potosky AL, Saxman S, Wallace RB, et al. Population variations in the initial treatment of non-small-cell lung cancer. J Clin Oncol 2004;22:3261–8. [DOI] [PubMed] [Google Scholar]
- [6].Hoffe S, Balducci L. Cancer and age: general considerations. Clin Geriatr Med 2012;28:1–8. [DOI] [PubMed] [Google Scholar]
- [7].Edwards BK, Noone AM, Mariotto AB, et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2014;120:1290–314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Stephens N, Rice D, Correa A, et al. Thoracoscopic lobectomy is associated with improved short-term and equivalent oncological outcomes compared with open lobectomy for clinical Stage I non-small-cell lung cancer: a propensity-matched analysis of 963 cases. Eur J Cardiothorac Surg 2014;46:607–13. [DOI] [PubMed] [Google Scholar]
- [9].Swanson SJ, Herndon JE, 2nd, D’Amico TA, et al. Video-assisted thoracic surgery lobectomy: report of CALGB 39802–a prospective, multi-institution feasibility study. J Clin Oncol 2007;25:4993–7. [DOI] [PubMed] [Google Scholar]
- [10].Yang X, Li M, Yang X, et al. Uniport versus multiport video-assisted thoracoscopic surgery in the perioperative treatment of patients with T1-3N0M0 non-small cell lung cancer: a systematic review and meta-analysis. J Thorac Dis 2018;10:2186–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Scott WJ, Matteotti RS, Egleston BL, et al. A comparison of perioperative outcomes of video-assisted thoracic surgical (VATS) lobectomy with open thoracotomy and lobectomy: results of an analysis using propensity score based weighting. Ann Surg Innov Res 2010;4:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Muraoka M, Oka T, Akamine S, et al. Video-assisted thoracic surgery lobectomy reduces the morbidity after surgery for stage I non-small cell lung cancer. Jpn J Thorac Cardiovasc Surg 2006;54:49–55. [DOI] [PubMed] [Google Scholar]
- [13].Iwasaki A, Shirakusa T, Shiraishi T, et al. Results of video-assisted thoracic surgery for stage I/II non-small cell lung cancer. Eur J Cardiothorac Surg 2004;26:158–64. [DOI] [PubMed] [Google Scholar]
- [14].Sihoe AD, Au SS, Cheung ML, et al. Incidence of chest wall paresthesia after video-assisted thoracic surgery for primary spontaneous pneumothorax. Eur J Cardiothorac Surg 2004;25:1054–8. [DOI] [PubMed] [Google Scholar]
- [15].Dai F, Meng S, Mei L, et al. Single-port video-assisted thoracic surgery in the treatment of non-small cell lung cancer: a propensity-matched comparative analysis. J Thorac Dis 2016;8:2872–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Hirai K, Takeuchi S, Usuda J. Single-incision thoracoscopic surgery and conventional video-assisted thoracoscopic surgery: a retrospective comparative study of perioperative clinical outcomesdagger. Eur J Cardiothorac Surg 2016;49 Suppl 1:i37–41. [DOI] [PubMed] [Google Scholar]
- [17].Tsukazan MTR, Terra RM, Vigo A, et al. Video-assisted thoracoscopic surgery yields better outcomes than thoracotomy for anatomical lung resection in Brazil: a propensity score-matching analysis using the Brazilian Society of Thoracic Surgery database. Eur J Cardiothorac Surg 2018;53:993–8. [DOI] [PubMed] [Google Scholar]
- [18].Desai H, Natt B, Kim S, et al. Decreased in-hospital mortality after lobectomy using video-assisted thoracoscopic surgery compared with open thoracotomy. Ann Am Thorac Soc 2017;14:262–6. [DOI] [PubMed] [Google Scholar]
- [19].Xue L, Pan T, Xu Z, et al. Multi-factor investigation of early postoperative cardiac arrhythmia for elderly patients with esophageal or cardiac carcinoma. World J Surg 2009;33:2615–9. [DOI] [PubMed] [Google Scholar]
- [20].Dziedzic R, Marjanski T, Binczyk F, et al. Favourable outcomes in patients with early-stage non-small-cell lung cancer operated on by video-assisted thoracoscopic surgery: a propensity score-matched analysis. Eur J Cardiothorac Surg 2018;54:547–53. [DOI] [PubMed] [Google Scholar]
- [21].Whitson BA, Andrade RS, Boettcher A, et al. Video-assisted thoracoscopic surgery is more favorable than thoracotomy for resection of clinical stage I non-small cell lung cancer. Ann Thorac Surg 2007;83:1965–70. [DOI] [PubMed] [Google Scholar]
- [22].Shigemura N, Akashi A, Funaki S, et al. Long-term outcomes after a variety of video-assisted thoracoscopic lobectomy approaches for clinical stage IA lung cancer: a multi-institutional study. J Thorac Cardiovasc Surg 2006;132:507–12. [DOI] [PubMed] [Google Scholar]
- [23].Witte B, Stenz C, Vahl CF, et al. Comparative intention-to-treat analysis of the video-assisted thoracoscopic surgery approach to pulmonary segmentectomy for lung carcinomadouble dagger. Interact Cardiovasc Thorac Surg 2015;21:276–83. [DOI] [PubMed] [Google Scholar]
- [24].Higuchi M, Yaginuma H, Yonechi A, et al. Long-term outcomes after video-assisted thoracic surgery (VATS) lobectomy versus lobectomy via open thoracotomy for clinical stage IA non-small cell lung cancer. J Cardiothorac Surg 2014;9:88. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.