

Polycystic ovary syndrome (PCOS), one of the most common reproductive abnormalities, shares some components of metabolic cardiovascular syndrome. The cited prevalence of PCOS ranges from 7% to almost 20%, depending on the diagnostic criteria.1–5 PCOS is frequently associated with overweight, obesity, metabolic syndrome, glucose intolerance, hyperinsulinemia, dyslipidemia, and hypertension.5–7 Patients with PCOS may also suffer diabetes, cardiovascular (CV) morbidity and possibly also mortality, sleep apnea, stroke, peripheral vascular disease, fibromyalgia, nonalcoholic fatty liver disease, uterine cancer, and breast malignancy.5–7
Metabolic Syndrome and CV Morbidity in PCOS
PCOS patients have persistently higher prevalence rates of metabolic syndrome than control women, regardless of matched age and body mass index (BMI) ranges.8 Although the prevalence of metabolic syndrome in PCOS patients is comparable to that of 30-year older control women,8 the pathogenesis and the connection between PCOS and metabolic syndrome or CV morbidity and mortality are still debated. Recent evidence has been focused on low-grade chronic inflammation as a potential cause of the long-term consequences of PCOS.5–7 Although the epidemiology is not unequivocal, some studies do suggest a possible association between PCOS and CV morbidity and mortality.5–7 Insulin resistance and obesity may be the mediators of early ventricular abnormalities, endothelial dysfunction, arterial stiffness, and both carotid and coronary atherosclerosis.5–7 The suggested mechanisms relate to the consequences of insulin resistance such as dyslipoproteinemia, hypertension, increased oxidative stress, low-grade inflammation, altered hemostasis and dysfibrinolysis, as well as alterations in myocardial energetics and collagen turnover.5–7
C-Reactive Protein and PCOS
Elevated C-reactive protein (CRP) levels, inflammatory cytokines (such as interleukin-6 and interleukin-18), and increased leucocyte count indicate on low-grade chronic inflammation in PCOS.7–11 CRP has been shown to be a good marker of inflammation and one of the most sensitive predictors of CV morbidity.7,9,10 Of 12 measured markers, high sensitive-CRP was the strongest univariate predictor of CV disease.11 In multivariate analysis, the only markers that independently predicted CV risk were CRP and total cholesterol to HDL-cholesterol ratio.11 Furthermore, higher CRP levels were measured in healthy postmenopausal women participating in the Women’s Health Study who have subsequently suffered a CV event compared with those women who did not experience any CV morbidity.11,12
Lipids, Inflammation, and CVD
Uncoupling of nitrous oxide synthase (NOS) activity with decreased production of nitrous oxide (NO) and generation of peroxynitrite may be a pathophysiologic event generating endothelial dysfunction, atherogenesis, and thromboembolic morbidity.7,11–13 However, it is still equivocal whether hyperandrogenemia significantly contributes to the CV morbidity.7 The PCOS patients possess a higher percentage of central abdominal fat despite similar percentage of total fat compared with weight matched controls. Changes in the concentrations of transforming growth factor beta (TGF-β) superfamily members such as inhibins, anti-Müllerian hormone, activin, and the non-TGF-β superfamily follistatin also take place in PCOS and may have a pathophysiologic role.7,9-13 High visceral adiposity may be a causative factor of insulin resistance, dyslipidemias, and hyperglycemia. Visceral fat cells may secrete inflammatory molecules, through endocrine and/or paracrine mechanisms. Such pro-inflammatory mediators may consist of oxidative stress mediators, increased white blood cells, chemokines and cytokines, and several other markers of endothelial inflammation, such as high sensitivity (hs)-CRP, tumour necrosis factor alpha, homocysteine, interleukin-6 and interleukin-18, vaspin, monocyte chemoattractant protein-1, advanced glycation end products, and complement C3, being cytokines generated by the fat, alveolar cells.7,9-13
It has been suggested that all PCOS subjects should be assessed for individual CV risk factors and global CVD risk.14 If screening reveals CVD risk factors including obesity, cigarette smoking, dyslipidemia, hypertension, impaired glucose tolerance, and inadequate physical activity, PCOS patients may be at high risk of CV morbidity and mortality. It has been suggested that a fasting lipid profile (total cholesterol, low density lipoprotein cholesterol, high density lipoprotein cholesterol, and triglyceride level at diagnosis) should be assessed in all overweight and obese PCOS subjects, at any age. Afterwards, repeated measurement should be dictated by the results and the global CV profile risk.14 In addition, all the PCOS patients should have annual blood pressure measurements.14 Although the risk of CV morbidity and mortality of PCOS patients is still equivocal, the prevalence of CVD risk factors is increased, suggesting high awareness and considering screening of risk factors consideration (https://www.monash.edu/medicine/sphpm/mchri/pcos/resources/practice-tools-for-health-practitioners).14
However, PCOS and its related CV morbidity and mortality are determined not only by environmental factors and life style behaviour but also by genetic factors. Recently, genome-wide meta-analysis and linkage disequilibrium score regression, in more than 10 000 PCOS patients, found genetic associations with fasting insulin, type 2 diabetes, obesity, lipids and lipoprotein profile, and coronary artery morbidity, augmenting the common genetic trait between metabolic disorders and PCOS.15 Mendelian randomization analyses indicated that variants associated with fasting insulin, age of menopause, BMI, male-pattern alopecia, and depression may have a pathophysiologic role in the PCOS.15 Furthermore, an increased risk of mortality due to fatal coronary heart disease has been attributed to PCOS in a prospective study.16
The Clinical Application of High CRP in PCOS
We, and others, have found significantly higher CRP levels in PCOS patients versus controls.9,10 The CRP concentrations, in our study, were significantly higher in both the lean PCOS patients (BMI < 25), as well as in the obese PCOS group (BMI > 30) versus the control patients of comparable BMI (P < 0.001).10 Our study, in 201 subjects (117 PCOS patients and almost a hundred controls, Figure1) suggested that CRP might indeed be a marker of possible prospective identification of young PCOS women prone to ultimately suffer CVD when they get older.10
Figure 1.
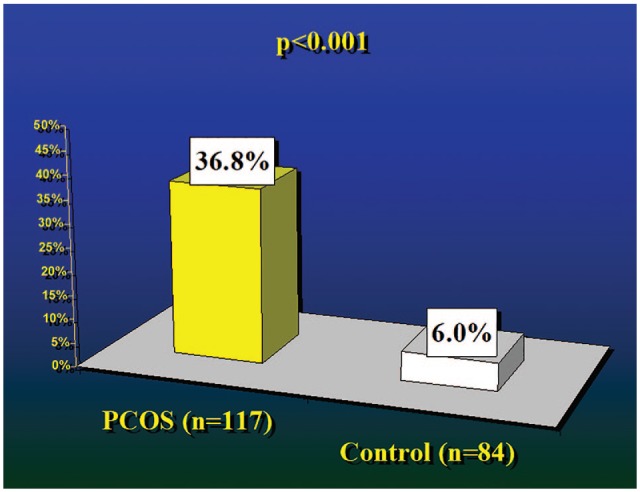
Significantly higher prevalence of high C-reactive protein level (>5 mg/L) in polycystic ovary syndrome (PCOS) patients compared with age- and body mass index–adjusted controls.
Recently, Kalyan et al17 have shown that the ratio of CRP to albumin is a more accurate and stronger correlate of PCOS compared with both free androgens and insulin resistance. These investigators have found that the CRP/albumin ratio had a higher specificity and sensitivity for inflammation associated with metabolic dysfunction than insulin resistance and androgens in matched PCOS patients.17
Although none of our PCOS subjects10 had any sign of inflammation, the higher erythrocyte sedimentation rate in the PCOS patients versus controls supports the study by Kelly et al9 suggesting a chronic subclinical inflammatory process as an underlying mechanism of atherosclerosis in PCOS.10,18
Visceral/abdominal fat distribution is independently associated with low-grade inflammation. Is this a cause or effect for increased CRP levels in women with PCOS? Compared with controls, PCOS patients have increased CRP/albumin ratio irrespective of the BMI.17 This finding supports the view that inflammation may be a central pathophysiologic player in PCOS, independent of BMI and adiposity.
Variability in CRP concentrations may reflect genetic polymorphism in its gene, in addition to environmental parameters.19 It is beyond the scope of this editorial to laboriously discuss the CRP polymorphism. Nevertheless, such polymorphism may be important in establishing the role of CRP as a sensitive and accurate predictor of CVD, in addition to validating the cause and effect relationship between CRP and CV morbidity.19
A busy reproductive endocrinology and infertility clinic may look after thousands or many hundreds of PCOS patients. For such a prevalent syndrome as PCOS (7%-20%), it is practically impossible to closely follow up and tightly control thousands or many hundreds of PCOS patients, for future CV risks, measure their blood pressure and lipid profile, and monitor their lifestyle frequently, as suggested.14 Therefore, a practical compromise may be to concentrate on those PCOS patients with high CRP and other markers of CVD.10 These patients should be more closely and aggressively monitored for their lifestyle (obesity, exercise, smoking, diet), and when not successful, consider the addition of insulin sensitizers such as metformin, aspirin, and/or statins.10 Therefore, treatment regimens directed towards lowering CRP levels (such as diet, smoking cessation, exercise, blood pressure control, low-dose aspirin, metformin, and possibly statins) should probably be more aggressive for those PCOS women with increased CRP levels.10 Whether this attitude may indeed lower the future CV morbidity and mortality in PCOS patients remains to be determined by future prospective randomized trials.
Footnotes
Funding:The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ORCID iD: Zeev Blumenfeld  https://orcid.org/0000-0003-3929-7940
https://orcid.org/0000-0003-3929-7940
References
- 1. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab. 1998;83:3078–3082. doi: 10.1210/jcem.83.9.5090. [DOI] [PubMed] [Google Scholar]
- 2. Copp T, Jansen J, Doust J, Mol BW, Dokras A, McCaffery K. Are expanding disease definitions unnecessarily labelling women with polycystic ovary syndrome? BMJ. 2017;358:j3694. [DOI] [PubMed] [Google Scholar]
- 3. Tehrani FR, Simbar M, Tohidi M, Hosseinpanah F, Azizi F. The prevalence of polycystic ovary syndrome in a community sample of Iranian population: Iranian PCOS prevalence study. Reprod Biol Endocrinol. 2011;9:39. doi: 10.1186/1477-7827-9-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. March WA, Moore VM, Willson KJ, Phillips DI, Norman RJ, Davies MJ. The prevalence of polycystic ovary syndrome in a community sample assessed under contrasting diagnostic criteria. Hum Reprod. 2010;25:544–551. doi: 10.1093/humrep/dep399. [DOI] [PubMed] [Google Scholar]
- 5. Yildiz BO, Bozdag G, Yapici Z, Esinler I, Yarali H. Prevalence, phenotype and cardiometabolic risk of polycystic ovary syndrome under different diagnostic criteria. Hum Reprod. 2012;27:3067–3073. doi: 10.1093/humrep/des232. [DOI] [PubMed] [Google Scholar]
- 6. Bates GW., Jr. Polycystic ovary syndrome: a reproductive and metabolic web of risk, comorbidities, and disease. Fertil Steril. 2019;111:471–472. doi: 10.1016/j.fertnstert.2019.01.028. [DOI] [PubMed] [Google Scholar]
- 7. Legro RS. Evaluation and treatment of polycystic ovary syndrome. In: De Groot LJ, Chrousos G, Dungan K, et al., eds. Endotext. South Dartmouth, MA: MDText.com, Inc; 2017. https://www.endotext.org/chapter/evaluation-and-treatment-of-polycystic-ovary-syndrome/. Accessed February 14, 2019. [Google Scholar]
- 8. Apridonidze T, Essah PA, Iuorno MJ, Nestler JE. Prevalence and characteristics of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2005;90:1929–1935. [DOI] [PubMed] [Google Scholar]
- 9. Kelly CC, Lyall H, Petrie JR, Gould GW, Connell JM, Sattar N. Low grade chronic inflammation in women with polycystic ovarian syndrome. J Clin Endocrinol Metab. 2001;86:2453–2455. [DOI] [PubMed] [Google Scholar]
- 10. Boulman N, Levy Y, Leiba R, et al. Increased C-reactive protein levels in the polycystic ovary syndrome: a marker of cardiovascular disease. J Clin Endocrinol Metab. 2004;89:2160–2165. [DOI] [PubMed] [Google Scholar]
- 11. Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000;342:836–843. [DOI] [PubMed] [Google Scholar]
- 12. Ridker PM, Buring JE, Shih H, Matias M, Hennekens CH. Prospective study of C-reactive protein and the risk of future cardiovascular events among apparently healthy women. Circulation. 1998;98:731–733. [DOI] [PubMed] [Google Scholar]
- 13. Diamanti-Kandarakis E, Paterakis T, Kandarakis HA. Indices of low-grade inflammation in polycystic ovary syndrome. Ann N Y Acad Sci. 2006;1092:175–186. [DOI] [PubMed] [Google Scholar]
- 14. www.monash.edu/medicine/sphpm/mchri/pcos.
- 15. Day F, Karaderi T, Jones MR, et al. Large-scale genome-wide meta-analysis of polycystic ovary syndrome suggests shared genetic architecture for different diagnosis criteria. PLoS Genet. 2018;14:e1007813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Solomon CG, Hu FB, Dunaif A, et al. Menstrual cycle irregularity and risk for future cardiovascular disease. J Clin Endocrinol Metab. 2002;87:2013–2017. [DOI] [PubMed] [Google Scholar]
- 17. Kalyan S, Goshtesabi A, Sarray S, Joannou A, Almawi WY. Assessing C reactive protein/albumin ratio as a new biomarker for polycystic ovary syndrome: a case-control study of women from Bahraini medical clinics. BMJ Open. 2018;8:e021860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Center for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107:499–511. [DOI] [PubMed] [Google Scholar]
- 19. Hage FG, Szalai AJ. The role of C-reactive protein polymorphisms in inflammation and cardiovascular risk. Curr Atheroscler Rep. 2009;11:124–130. [DOI] [PubMed] [Google Scholar]