

A non-smoking 60-year-old Caucasian woman presented with acute onset of dyspnoea and chest tightness. She was haemodynamically stable but tachypneic. Arterial blood gas analysis in room air showed pH values of 7.29, oxygen partial pressure of 50 mmHg and carbon dioxide partial pressure of 65 mmHg. Clinical examination revealed subcutaneous emphysema around the neck. She also showed the shawl sign, the neckline V sign and Gottron’s papules located on the metacarpophalangeal and proximal interphalangeal joints. She complained of arthralgias over the previous 6 months without muscle weakness. Late inspiratory crackles could be heard over the lungs. She had normal serum creatine kinase, liver enzymes and lactate dehydrogenase values. Chest CT showed pneumomediastinum, pneumopericardium, bilateral interstitial thickening and ground glass opacities (Fig. 1). The skin biopsy confirmed the diagnosis of DM. Anti-MDA5 antibodies were identified in line-blot assay. The electromyography was normal. The patient was diagnosed with anti-MDA5-positive clinically amyopathic DM. Spontaneous pneumomediastinum is rarely a presenting symptom of DM [1]. It tends to occur with rapid progressive intestinal lung disease, anti-MDA5 antibody and clinically amyopathic DM, constituting a devastating complication [2]. The patient died shortly thereafter.
Fig. 1.
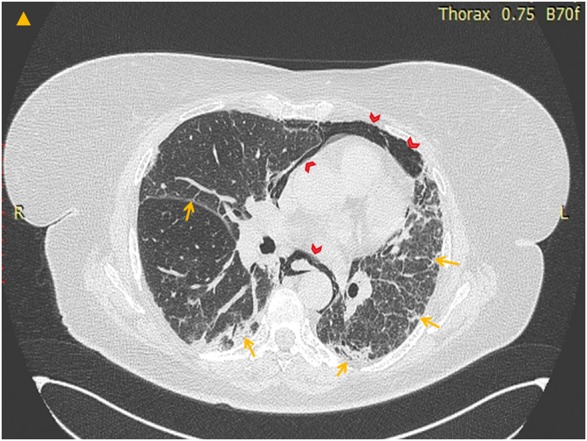
Chest CT shows pneumomediastinum, pneumopericardium (arrowheads), bilateral interstitial thickening and ground glass opacities (arrows)
References
- 1. Ye S, Chen XX, Lu XY. et al. Adult clinically amyopathic dermatomyositis with rapid progressive interstitial lung disease: a retrospective cohort study. Clin Rheumatol 2007;26:1647–54. [DOI] [PubMed] [Google Scholar]
- 2. Ma X, Chen Z, Hu W. et al. Clinical and serological features of patients with dermatomyositis complicated by spontaneous pneumomediastinum. Clin Rheumatol 2016;35:489–93. [DOI] [PubMed] [Google Scholar]