

Abstract
Aims
To explore the relationship between nurse–nurse collaboration and job satisfaction among hospital nurses and to test and refine a model explaining this relationship.
Design
A secondary analysis of a cross‐sectional survey.
Methods
Registered nurses (N = 406, female 88%) in one university hospital in Finland and one in Norway completed a self‐administered questionnaire in 2015. Structural equation modelling analysis was used to analyse the relationships between collaboration and job satisfaction subscales.
Results
The constructed SEM model fit the data well (RMSEA = 0.05, CFI = 0.985, χ2 p‐value > 0.1). The model strongly supported the hypothesized covariance between nurse–nurse collaboration and job satisfaction, while significant and positive relationships were observed between most of the subscales. The results suggest that there is a strong association between nurse–nurse collaboration and job satisfaction such that nurses are more satisfied when there is good collaboration and vice versa.
Keywords: collaboration, job satisfaction, model, nurse-nurse, quantitative research, secondary analysis
1. INTRODUCTION
The healthcare environment is changing, creating challenges in the development of working conditions and environments. This is partly due to societal changes such as the ageing of the population, increased understanding of work‐related issues and increasingly stringent workplace requirements relating to issues such as quality and safety (WHO, 2015).
Professional collaboration within and outside health care is essential for managing the different roles and responsibilities of registered nurses in the face of diverse local, national and global challenges. Good intraprofessional nurse–nurse relationships are important not only for the nurses themselves, but also for patients and healthcare organizations (Weaver Moore, Leahy, Sublett, & Lanig, 2013). According to a work environment study conducted in the USA by the American Association of Critical‐Care Nurses (AACN, 2015), nurses' work environments and perceptions of the quality of care provided in those environments have become worse since the year 2008. The nurses felt that collaboration had declined both in their working units and at the organizational level. Additionally, their overall levels of job satisfaction in terms of nursing in general and their current position in particular had also declined (AACN, 2015). According to the RN4CAST study (2009–2011), more than one in five nurses were dissatisfied with their jobs (Aiken, Sloane, Bruyneel, Heede, & Sermeus, 2013). This is worrying, while nurses and midwives constitute of more than 50% of the health workforce in many countries. Therefore, the WHO has emphasized the need for intra‐ and interprofessional collaborative partnerships to maximize nurses' capacities and potential (WHO, 2016). According to Flinkman and Salanterä (2015), young RNs in Finland have expressed multiple reasons for leaving the profession, one of which is poor nursing environments that provide insufficient support, mentoring and orientation among other things. The most important factor keeping nurses in their current jobs was their colleagues (Wargo‐Sugleris, Robbins, Lane, & Phillips, 2017), salary and benefits (Ulrich, Lavandero, Woods, & Early, 2014). More recently, the AACN identified six standards that make for a healthy work environment: skilled communication, effective decision‐making, true collaboration, proper staffing, authentic leadership and meaningful recognition (AACN, 2015).
Good collaboration in the profession is related to patient satisfaction and job satisfaction (Kvist et al., 2013; Ma, Shang, & Bott, 2015; Uhrenfeldt & Hall, 2015; Weaver Moore et al., 2013), lower intention to leave nursing and better quality of care (Ma et al., 2015). Conversely, poor nurse–nurse relationships may increase nurse turnover (Tuckett, Winters‐Chang, Bogossian, & Wood, 2015). These findings are consistent with those of Galleta, Portoghese, Carta, D'Aloja, and Campagna (2016), whose results suggest that nurses who have higher levels of job satisfaction and experience positive collaboration with physicians are more committed to their teams.
The relationship between nurse–nurse collaboration and nurses' job satisfaction warrants investigation for two reasons: First, it has not been studied extensively before, and second, nurse shortages are a major issue in modern health care (Ulrich et al., 2014), so there is an urgent need to find ways of increasing nurses' job satisfaction to prevent them from leaving the profession.
2. BACKGROUND
Studies have shown that intraprofessional nurse–nurse interactions, and good relationships between nurses have important effects on nurses' job satisfaction (Atefi, Abdullah, Wong, & Mazlom, 2014; Cheung & Ching, 2014; Chenjuan, Jingjing, & Bott, 2015). Moreover, nurses' teamwork and workplace relationships are related to their commitment to their current hospital and intention to leave (Brunetto et al., 2013). Peer support also has important effects on nurses' well‐being and job satisfaction (Averlid & Bihari Axelsson, 2012; Purpora & Bleigen, 2015). According to Utriainen, Ala‐Mursula, and Kyngäs (2015), the well‐being of hospital nurses at work is associated with assistance and support among nurses and with nurses' togetherness and cooperation. Similarly, confidence and appreciation from colleagues have been shown to improve nurses' job satisfaction (Uhrenfeldt & Hall, 2015). Moore, Prentice, and McQuestion (2015) found that social interactions are important to patient care and job satisfaction and enhance collaborative relationships between nurses. In addition, negative peer relationships among nurses are associated with horizontal violence (Purpora & Bleigen, 2015) and workplace incivility has been found to weaken collaborative and safe practice (Lynette, Echevarria, Sun, & Greene Ryan, 2016). Poor nurse relationships may cause some nurses to leave the profession, so it is important for nurse managers to encourage positive relations in nursing units by encouraging nurses, promoting a friendly environment and confronting conflicts as soon as they occur (Weaver Moore et al., 2013).
2.1. Collaboration
Collaboration is a complex process that is central in nursing (Henneman, Lee, & Cohen, 1995). It is based on respect and trust between individuals and requires confidence, competence and commitment from all participants. The word “collaboration” dates back to the mid‐19th century and derives from the Latin word “collaborare,” meaning “to labour together.” It is defined as “the action of working with someone to produce or create something” (Oxford Dictionary, 2017). Intraprofessional collegialism has been described as sharing of knowledge and feedback (Miller & Kontos, 2012), while interdisciplinary collaboration has been defined as sharing and working together using problem‐focused processes (Petri, 2010). Dougherty and Larson (2010) identified five subscales of collaboration: conflict management, communication, shared process, coordination and professionalism. Conversely, Patel, Pettitt, and Wilson (2012) delineated seven main groups of factors involved in collaboration, which they termed context, support, tasks, interaction processes, teams, individuals and overarching factors. Collaboration can be understood in different ways by nurses; Moore and Prentice (2012) found that the terms most commonly used by nurses to describe collaboration were consultation, communication and collegiality. This diversity of interpretations suggests that for nurses to achieve good collaboration, it is important to establish a shared understanding of what collaboration means. Teamwork‐based collaboration has important effects on nurses' work environments (Averlid & Bihari Axelsson, 2012; Uhrenfeldt & Hall, 2015), where good communication is needed for efficient information transfer and to facilitate good decision‐making (Dougherty & Larsen, 2010).
2.2. Job satisfaction
Job satisfaction has been defined in many different ways. Spector (1997, p. 2) defined it as “the degree people like their jobs.” Another well‐known definition is that of Locke (1976, p. 1,304): “a pleasurable or positive emotional state resulting from the appraisal of one's job or job experiences.” A concept analysis conducted by Castaneda and Scanlan (2014) suggested that job satisfaction in nursing is based on three attributes: interpersonal relationships, patient care and autonomy. Autonomy is related to mutual trust, education and support from management and coworkers and teamwork. Kvist et al. (2012) identified seven subscales of job satisfaction: leadership, requiring factors of work, working environment, sense of community, working welfare, motivating factors of work and participation in decision‐making. Their study showed that the highest degree of job satisfaction derived from motivating factors of work such as client feedback, having suitable and challenging work, using one's skills at work, appreciation of one's own work and finding work interesting. According to Atefi et al. (2014), motivating factors of work for nurses include their requiring factors of work, autonomy and professional development. Other studies have highlighted the sensitivity of nurses' job satisfaction to participation in decision‐making (Cheung & Ching, 2014; Kaddourah, Khalidi, Abu‐Shaheen, & Al‐Tannir, 2013; Weaver Moore et al., 2013), control over one's work and the burden of responsibility (Sawatzky, Enns, & Legare, 2015). Similarly, studies have shown that the management plays a vital role in creating and maintaining a healthy work environment (Averlid & Bihari Axelsson, 2012; Ulrich et al., 2014) and enhancing nurses' job satisfaction (Atefi et al., 2014; Sawatzky et al., 2015) and well‐being (Utriainen et al., 2015). This study is based on a theory‐driven hypothesized model of nurse–nurse collaboration and job satisfaction. The aim of this study was to examine the relationship between nurse–nurse collaboration and nurses' job satisfaction based on the hypothesized model presented in Figure 1 using structural equation modelling (SEM). The research question: Is there a relationship between nurse–nurse collaboration and nurses' job satisfaction.
Figure 1.
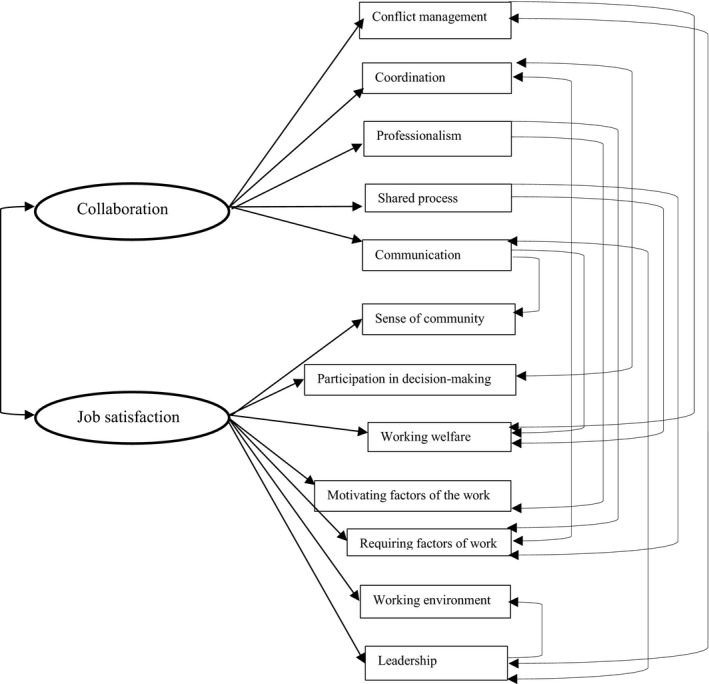
A hypothesized model of pathways relating collaboration to job satisfaction
3. THE STUDY
3.1. Design
The secondary analysis used existing data collected in 2015 during a cross‐sectional study on the relationship between nurse–nurse collaboration and job satisfaction in one university hospital in Finland and one university hospital in Norway. Secondary data analysis is a cost‐effective and efficient way to obtain a broad understanding of a research questions (McCaston, 2005), and in this study, we found it as a good solution to look the relationship between nurse–nurse collaboration and their job satisfaction.
3.2. Participants and data collection
A questionnaire was sent to 1,031 RNs (N = 303) in Finland and 1,039 RNs (N = 103) in Norway. The response rate was 29% in Finland and 10% in Norway. In this study, a Raosoft sample size calculator (Raosoft, 2012) was used to calculate the sample size at a margin error of 95%. The total sample demonstrated sufficient power, with data for 406 RNs in total being available for use in covariance‐based SEM (Hoyle, 2012).
Primary data were collected between April–September 2015 by convenience sampling of registered nurses working at one university hospital in various clinical settings in Finland and Norway. Data were obtained using a self‐report 72‐item survey whose items were divided into three groups: items relating to demographic information (age, gender, main working time, form of employment, work unit, work experience in current unit and total work experience) and items belonging to two scales relating to nurse–nurse collaboration and job satisfaction. Information about the study was given to nursing managers and titled contact persons at the participating hospitals by e‐mail and during site visits to the hospitals. Participants were invited to complete an anonymous web‐based questionnaire voluntary.
3.3. Methods
Collaboration was measured using the Nurse–Nurse Collaboration Scale (NNCS) developed by Dougherty and Larson (2010), which contains 35 items measuring five subscales of collaboration: conflict management (seven items), communication (eight items), shared process (eight items), coordination (five items) and professionalism (seven items). Participants were asked to rate their agreement with each item using a 4‐point Likert scale ranging from 1 = “strongly disagree” to 4 = “strongly agree.”
Job satisfaction was measured using the Kuopio University Hospital Job Satisfaction Scale (KUHJSS) developed by Kvist et al. (2012). This scale has 37 items covering seven subscales: leadership (seven items), requiring factors of work (eight items), motivating factors of work (six items), working environment (four items), working welfare (four items), participating in decision‐making (four items) and sense of community (four items). Participants self‐reported their agreement with a five‐point Likert scale where 1 = “strongly disagree” and 5 = “strongly agree.” In this secondary analysis, data from Finland and Norway were combined and used as a single data set.
3.4. Validity and reliability
Cronbach's alpha coefficient values for the NNCS scale (35 items in total) was 0.92 and those for its five subscales were as follows: conflict management α = 0.81, communication α = 0.82, shared process α = 0.76, coordination α = 0.62 and professionalism α = 0.86. Cronbach's alpha coefficient value for the KUHJSS scale (37 items in total) was 0.93 and those for its seven subscales were as follows: leadership α = 0.92, requiring factors of work α = 0.81, motivating factors of the work α = 0.76, working environment α = 0.80, working welfare α = 0.65, participation in decision‐making α = 0.72 and sense of community α = 0.73. These high values indicate good levels of internal consistency (Polit & Beck, 2008). Cronbach's alpha values for the original job satisfaction scale ranged from 0.72–0.89 (Kvist et al., 2012). Cronbach's alpha value for the Nurse–Nurse Collaboration Scale ranged from 0.66–0.90 (Dougherty & Larson, 2010).
3.5. Data analysis and model testing
In the secondary analysis, structural equation modelling (SEM) (Hoyle, 2012) was used to assess how well the hypothesized model fit the study data. In the first phase of the analysis, the structure of the 7‐factor scale (KUHJSS) and the 5‐factor scale (NNCS) was verified using confirmatory factor analysis (CFA). CFA can be a useful tool for testing the structure of and relationships between theoretical concepts or factors identified in exploratory factor analyses. In particular, it has proven to be a good tool for verifying theories in nursing sciences (Kääriäinen et al., 2011). CFA confirmed the hypothesized factor structure (results not shown here), justifying the subsequent SEM analysis.
The hypothesized model was then evaluated using SEM. During the analysis, the hypothesized model was modified as follows: First, a path was deleted if the associated parameter estimates were not statistically significant (p > 0.05); paths deleted for this reason included those relating to the nurses' demographics (e.g. their working unit and country). Then, the modification indices (MI) for the model were examined to identify statistically and theoretically justified modifications. To this end, all paths were removed from the model one by one and the resulting change in the model fit was analysed using the sample size‐adjusted Bayesian information criterion (BIC). If the BIC value changed appreciably, the path was restored to the model. Several statistical tests were used to evaluate the fit of the final model, namely chi‐squared test with degrees of freedom, the Comparative Fit Index (CFI) and the root mean square error of approximation (RMSEA). The CFI is a measure commonly used to compare a target model to the null model, while the RMSEA represents the square root of the average or mean of the covariance residuals, that is the differences between corresponding elements of the observed and predicted covariance matrices. CFI should be higher than 0.9, and RMSEA should be less than 0.1 for adequate fit. The latter analyses were conducted using lavaan‐package (Rosseel, 2012) of R (R Core Team, 2017).
3.6. Ethical considerations
Consent to perform the study was obtained from either central or local ethical committees, depending on national legislation. Additionally, the study was approved by the relevant authorities at the participating hospitals. All participants were informed of the study's purpose, the voluntary nature of participation and the confidentiality pledge. Completing and returning the survey was regarded as consent to participation.
4. RESULTS
4.1. Demographics of RNs
In total, 406 RNs completed the survey. Most respondents were female (88%). The mean age was 40.9 years (SD 11.3). The mean length of time working in their current unit and mean total work experience in health care were 7.9 years (SD 8.8) and 15.7 years (SD 10.6), respectively. Most (78%) of the RNs had a permanent position and a shift‐based working schedule (77%).
4.2. Relationships between nurse–nurse collaboration and job satisfaction
The constructed SEM model fit the data well (RMSEA = 0.05, CFI = 0.985, χ2 p‐value > 0.1). In addition to latent variables (collaboration, job satisfaction), the model included two effect types: regression effects, for which the causal direction of the two factors could be assumed and covariance parameters, where the two factors covaried but there was no evidence of causality. The main result of the SEM analysis was its clear support for the hypothesized strong covariance between job satisfaction and collaboration. The model confirmed that collaboration has direct effects on the coordination, professionalism, shared process, conflict management and communication subscales. Moreover, job satisfaction has direct effects on leadership, requiring factors of work, work environment, motivating factors of work, working welfare, participation in decision‐making and sense of community.
Some of the subscales were related to each other: requiring factors of work, working welfare, working environment and participation in decision‐making were all significantly related to one‐another. In addition, participation in decision‐making and leadership and shared process and working welfare were positively linked to each other. Participation in decision‐making and working welfare were related to motivating factors of work (the latter being represented by items such as “Client feedback motivates me in my work” and “My work tasks are suitably challenging”). Communication, conflict management, professionalism and shared process were also positively related to each other. The directions of the paths and their standardized magnitudes are shown in Table 1 and Figure 2.
Table 1.
Standardized direct effects (SE) of nurse–nurse collaboration on job satisfaction
| Path | Estimate | SE | p |
|---|---|---|---|
| Latent variables | |||
| Collaboration | |||
| Conflict management | 0.773 | 0.024 | *** |
| Communication | 0.676 | 0.041 | *** |
| Shared process | 0.640 | 0.047 | *** |
| Coordination | 0.671 | 0.037 | *** |
| Professionalism | 0.864 | 0.021 | *** |
| Job satisfaction | |||
| Leadership | 0.715 | 0.032 | *** |
| Requiring factors of work | 0.662 | 0.033 | *** |
| Motivating factors of work | 0.399 | 0.057 | *** |
| Work environment | 0.615 | 0.037 | *** |
| Working welfare | 0.268 | 0.072 | *** |
| Participation in decision‐making | 0.698 | 0.032 | *** |
| Sense of community | 0.842 | 0.021 | *** |
| Covariances | |||
| Job satisfaction ↔ Collaboration | 0.946 | 0.021 | *** |
| Conflict management ↔ Communication | 0.231 | 0.056 | *** |
| Communication ↔ Professionalism | 0.275 | 0.063 | *** |
| Communication ↔ Shared process | 0.125 | 0.055 | ** |
| Requiring factors of work ↔ Working welfare | 0.212 | 0.046 | *** |
| Requiring factors of work ↔ Work environment | 0.360 | 0.050 | *** |
| Requiring factors of work ↔ Participation in decision‐making | 0.175 | 0.048 | *** |
| Participation in decision‐making ↔ Shared process | 0.231 | 0.048 | *** |
| Leadership ↔ Participation in decision‐making | 0.247 | 0.058 | *** |
| Working welfare ↔ Shared process | 0.292 | 0.048 | *** |
| Regressions | |||
| Motivating factors of work ← Working welfare | 0.245 | 0.055 | *** |
| Motivating factors of work ← Participation in decision‐making | 0.259 | 0.054 | *** |
| Working welfare ← Communication | 0.229 | 0.067 | ** |
Asterisks represent different significance levels (* = p < 0.05; ** = p < 0.01; *** = p < 0.001).
Figure 2.
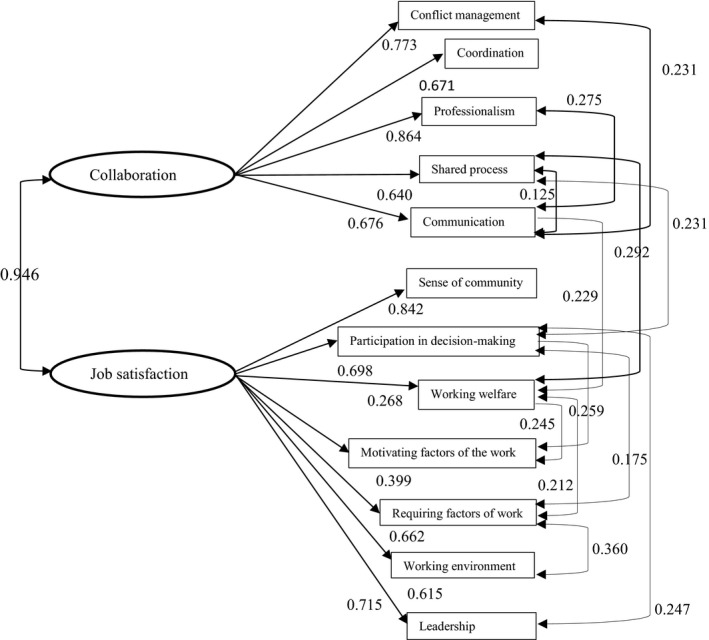
Pathways of factors related to collaboration and job satisfaction
5. DISCUSSION
The aims of this study were to characterize the relationship between nurse–nurse collaboration and nurses' job satisfaction among hospital nurses and to produce a model explaining the effects of nurse–nurse collaboration on job satisfaction. The structural equation modelling results confirmed that collaboration and job satisfaction were significantly and positively related to each other. This is supported by Uhrenfeldt and Hall (2015), which suggests that teamwork builds on both job satisfaction and job dissatisfaction. Relationships with coworkers, clients and relatives increase job satisfaction, while supportive collegial relationships and satisfaction with job status are important factors influencing nurses' intention to stay in the profession (Tourangeau et al., 2014). Additionally, a study conducted in the United States by Chenjuan et al. (2015) indicated that good collaboration among nurses is associated with higher job satisfaction, lower intent to leave and better quality of care. The results of our study suggest that communication has important effects on nurses' working welfare. Communication and verbal encouragement strengthen nurse–nurse relationships and ultimately create healthy working environments (Weaver Moore et al., 2013). Recognition from other nurses is valued as meaningful because it helps nurses recognize the importance of their work (Ulrich et al., 2014). In our study, nurses who experienced autonomy were involved in decision‐making and reported high levels of working welfare. They also reported higher scores on items relating to motivating factors of work. In other words, more satisfied nurses were more motivated and appreciative of their work and found their work interesting. Similar results were obtained by Shwaihet and Nasaif (2015), who reported that participation in decision‐making and autonomy are strong predictors of job satisfaction. However, it should be noted that young RNs have also reported a lack of support, feelings of isolation and excessive responsibility as reasons for leaving the profession (Flinkman & Salanterä, 2015). The results of our study suggest that good communication promotes better conflict management, professionalism (e.g. mutual respect) and shared processes (e.g. agreement on common goals) and vice versa. In keeping with these findings, an earlier study showed that nurses' decision‐making and innovation could be improved by establishing a supportive culture with respectful discourse where conflict and stress are conveyed to positive resources (Moreland & Apker, 2015). Nurses use communication skills such as caring, openness, interest in others and empathy when communicating with each other and were shown to use these skills to a higher degree than other professionals when communicating in their own group (Andre', Nøst, Frigstad, & Sjøvold, 2016).
These results suggest that requiring factors of work such as work load, salary and staffing levels are associated with nurses' working welfare, working environment and decision‐making. Factors relating to nurses' working welfare such as professional development and competence are enhanced by autonomy and decision‐making. Satisfaction with job status (full‐time or part‐time), work‐life balance and access to resources (support staff) are important factors for retaining nurses in the profession (Tourangeau et al., 2014), while shared governance strategies encourage nurses to play more active roles in decision‐making (Shwaihet & Nasaif, 2015).
5.1. Limitations
One limitation of this study is that the data collection was carried out in two university hospitals, which and can therefore limit the transferability of results to other organizations. A convenience sample was used, which can limit the generalization. Therefore, further studies are suggested to support the results. The questionnaire was quite long because it incorporated two surveys, which might have resulted in survey fatigue. Despite persistent recruitment process, data collection was challenging in spite that reminders were sent electronically. The total number of respondents was satisfactory, although the response rate was low. However, the characteristics of the participating RNs did not differ markedly from those of RNs in Scandinavia as a whole. Levels of collaboration and job satisfaction were measured by self‐assessment, meaning that the results could have been affected by subjectivity and response bias. It should also be noted that the good fit achieved in the SEM analysis does not exclude the possibility that an alternative model could yield a better fit to the data or be more accurate.
6. CONCLUSION
This study was conducted to determine whether there is a relationship between nurse–nurse collaboration and nurses' job satisfaction. The findings revealed that nurse–nurse collaboration and job satisfaction are strongly associated to each other. Good collaboration in groups of nurses improves job satisfaction and thereby reduces the likelihood of nurse turnover. Nurses with more positive experiences of collaboration at work are more satisfied, which would be expected to positively affect nurse outcomes, patient safety and nurses' well‐being at work.
The produced model provides insights into several factors associated with nurse–nurse collaboration and job satisfaction. It will facilitate the identification of features that could improve collaboration and job satisfaction, thereby helping to create positive working environments. Collaboration and communication skills should be emphasized during nurse education because intraprofessional collaboration is important not only for individual nurses but also for the entire working environment. Further research is needed to establish if there are differences in RN‐RN collaboration and job satisfaction in diverse healthcare settings or in different countries.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
AUTHOR CONTRIBUTIONS
All authors agreed on the final version and meet at least one of the following criteria [recommended by the ICMJE (http://www.icmje.org/recommendations/)]:
substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; and
drafting the article or revising it critically for important intellectual content.
ACKNOWLEDGEMENTS
This research was supported through the first author's involvement in the European Science Foundation Research Network Program “Reflection”—09‐RNP‐049. The views expressed are those of the first author and not necessarily those of the European Science Foundation.
Ylitörmänen T, Turunen H, Mikkonen S, Kvist T. Good nurse–nurse collaboration implies high job satisfaction: A structural equation modelling approach. Nursing Open. 2019;6:998–1005. 10.1002/nop2.279
Funding information
This research was supported by The Finnish Work Environment Fund, University of Eastern Finland, The Finnish Association of Nursing Research and the Finnish Foundation of Nursing Education.
REFERENCES
- AACN Standards for Establishing and Sustaining Healthy Work Environments: A Journey to Excellence. (2015). (2nd edn). California, CA: American Association of Critical‐Care Nurses. Available from https://www.aacn.org/WD/HWE/Docs/HWEStandards.pdf. [last accessed 2 9 2017]. [PubMed]
- Aiken, L. H. , Sloane, D. M. , Bruyneel, L. , Van den Heede, K. , & Sermeus, W. (2013). RN4CAST Consortium. Nurses' reports of working conditions and hospital quality of care in 12 countries in Europe. International Journal of Nursing Studies. 50(2), 143–153. 10.1016/j.ijnurstu.2012.11.009. [DOI] [PubMed] [Google Scholar]
- André, B. , Nøst, T. H. , Frigstad, S. A. , & Sjøvold, E. (2016). Differences in communication within the nursing group and with members of other professions at a hospital unit. Journal of Clinical Nursing, 26(7–8), 956–963. 10.1111/jocn.13410 [DOI] [PubMed] [Google Scholar]
- Atefi, N. , Abdullah, K. L. , Wong, L. P. , & Mazlom, R. (2014). Factors influencing registered nurses perception of their overall job satisfaction: a qualitative study. International Nursing Review, 61, 352–360. [DOI] [PubMed] [Google Scholar]
- Averlid, G. , & Bihari Axelsson, S. (2012). Health-promoting collaboration in anesthesia nursing: A qualitative study of nurse anesthetists in Norway. American Association of Nurse Anesthetists, 80(4), 74–80. [PubMed] [Google Scholar]
- Brunetto, Y. , Xerri, M. , Shriberg, A. , Farr‐Wharton, R. , Shacklock, K. , Newman, S. , & Dienger, J. (2013). The impact of workplace relationships on engagement, well‐being, commitment and turnover for nurses in Australia and the USA. Journal of Advanced Nursing, 69(12), 2786–2799. 10.1111/jan.12165 [DOI] [PubMed] [Google Scholar]
- Castaneda, G. A. , & Scanlan, J. M. (2014). Job satisfaction in nursing: A concept analysis. Nursing Forum, 49(2), 130–138. 10.1111/nuf.12056 [DOI] [PubMed] [Google Scholar]
- Chenjuan, M. , Jingjing, S. , & Bott, M. J. (2015). Linking unit collaboration and nursing leadership to nurse outcomes and quality of care. The Journal of Nursing Administration, 45(9), 435–442. 10.1097/NNA.0000000000000229 [DOI] [PubMed] [Google Scholar]
- Cheung, K. , & Ching, S. S. Y. (2014). Job satisfaction among nursing personnel in Hong Kong: A questionnaire survey. Journal of Nursing Management, 22(5), 664–675. 10.1111/j.1365-2834.2012.01475.x [DOI] [PubMed] [Google Scholar]
- Core Team, R. (2017). R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; Available from https://www.R-project.org/.[last accessed 2 92017]. [Google Scholar]
- Dougherty, M. B. , & Larson, E. L. (2010). The Nurse‐Nurse Collaboration Scale. Journal of Nursing Administration, 40(1), 17–25. 10.1097/NNA.0b013e3181c47cd6 [DOI] [PubMed] [Google Scholar]
- Flinkman, M. , & Salanterä, S. (2015). Early career experiences and perceptions – a qualitative exploration of the turnover of young registered nurses and intention to leave the nursing profession in Finland. Journal of Nursing Management, 23(8), 1050–1057. 10.1111/jonm.12251 [DOI] [PubMed] [Google Scholar]
- Galleta, M. , Portoghese, I. , Carta, M. G. , D'Aloja, E. , & Campagna, M. (2016). The effect of nurse‐physician collaboration on job satisfaction, team commitment and turnover intention in nurses. Research in Nursing & Health, 39(5), 375–385. 10.1002/nur.21733 [DOI] [PubMed] [Google Scholar]
- Henneman, E. , Lee, J. , & Cohen, J. (1995). Collaboration: A concept analysis. Journal of Advanced Nursing, 21, 103–109. 10.1046/j.1365-2648.1995.21010103.x [DOI] [PubMed] [Google Scholar]
- Hoyle, R. (2012). Handbook of Structural Equation Modeling. New York, NY: The Guildford Press. [Google Scholar]
- Kääriäinen, M. , Kanste, O. , Elo, S. , Pölkki, T. , Miettunen, J. , & Kyngäs, H. (2011). Testing and verifying nursing theory by confirmatory factor analysis. Journal of Advanced Nursing, 67(5), 1163–1172. 10.1111/j.1365-2648.2010.05561.x [DOI] [PubMed] [Google Scholar]
- Kaddourah, B. T. , Khalidi, A. , Abu‐Shaheen, A. K. , & Al‐Tannir, M. A. (2013). Factors impacting job satisfaction among nurses from a tertiary care centre. Journal of Clinical Nursing, 22(21–22), 3153–3159. 10.1111/jocn.12261 [DOI] [PubMed] [Google Scholar]
- Kvist, T. , Mäntynen, R. , Partanen, P. , Turunen, H. , Miettinen, M. , & Vehviläinen‐Julkunen, K. (2012). The job satisfaction of Finnish nursing staff: The development of a job satisfaction scale and survey results. Nursing Research and Practice, 2012, 998–11. 10.1155/2012/210509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kvist, T. , Mäntynen, R. , Turunen, H. , Partanen, P. , Miettinen, M. , Wolf, G. A. , & Vehviläinen‐Julkunen, K. (2013). How magnetic are Finnish hospitals measured by transformational leadership and empirical quality outcomes? Journal of Nursing Management, 21(1), 152–164. [DOI] [PubMed] [Google Scholar]
- Locke, E. (1976). Handbook of industrial and organizational psychology In Dunnette M. D. (Ed.), The nature and causes of job satisfaction. Chicago: Rand McNally. [Google Scholar]
- Lynette, J. , Echevarria, I. , Sun, E. , & Greene Ryan, J. (2016). Incivility across the nursing continuum. Holistic Nursing Practice, 30(5), 263–268. 10.1097/HNP.0000000000000167 [DOI] [PubMed] [Google Scholar]
- Ma, C. , Shang, J. , & Bott, M. J. (2015). Linking unit collaboration and nursing leadership to nurse outcomes and quality of care. The Journal of Nursing Administration, 45(9), 435–442. 10.1097/NNA.0000000000000229 [DOI] [PubMed] [Google Scholar]
- McCaston, M. K. (2005). Tips for collecting, reviewing and analyzing secondary data. Partnership & Household Livelihood Security Unit. Available from https://www.ands.org.au/__data/assets/pdf_file/0003/713235/Tips_for_Collecting_Reviewing_and_Analyz.pdf.
- Miller, K.‐L. , & Kontos, P. C. (2012). The intraprofessional and interprofessional relations of neurorehabilitation nurses: A negotiated order perspective. Journal of Advanced Nursing, 69(8), 1797–1807. 1111/jan.12041 [DOI] [PubMed] [Google Scholar]
- Moore, J. , & Prentice, D. (2012). Collaboration among nurse practitioners and registered nurses in outpatient oncology settings in Canada. Journal of Advanced Nursing, 69(7), 1574–1583. 10.1111/jan.12017 [DOI] [PubMed] [Google Scholar]
- Moore, J. , Prentice, D. , & McQuestion, M. (2015). Social interaction and collaboration among oncology nurses. Nursing Research and Practice, 2015, 248067.https://www.hindawi.com/journals/nrp/2015/248067/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moreland, J. J. , & Apker, J. (2015). Conflict and stress in hospital nursing: Improving communicative responses to enduring professional challenges. Health Communication, 31(7), 815–823. http://dx.doi.org.ezproxy.uef.fi:2048/10.1080/10410236.2015.1007548 [DOI] [PubMed] [Google Scholar]
- Oxford Dictionary (2017). Available from https://en.oxforddictionaries.com/definition/us/collaboration. [last accessed 2 9 2017].
- Patel, H. , Pettitt, M. , & Wilson, J. R. (2012). Factors of collaborative working: A framework for a collaboration model. Applied Ergonomics, 43(1), 998–26. 10.1016/j.apergo.2011.04.009 [DOI] [PubMed] [Google Scholar]
- Petri, L. (2010). Concept analysis of interdisciplinary collaboration. Nursing Forum, 45(2), 73–82. 10.1111/j.1744-6198.2010.00167.x [DOI] [PubMed] [Google Scholar]
- Polit, D. , & Beck, C. (2008). Nursing Research. Generating and Assessing Evidence for Nursing Practice (8th edn). Philadelphia, PA: Lippincott Williams 6 Wilkins. [Google Scholar]
- Purpora, C. , & Bleigen, M. A. (2015). Job satisfaction and horizontal violence in hospital staff registered nurses: The mediating role of peer relationships. Journal of Clinical Nursing, 24(15–16), 2286–2294. 10.1111/jocn.12818 [DOI] [PubMed] [Google Scholar]
- Raosoft.com . (2012). Sample size calculator. [online]. Retrieved from http://www.raosoft.com/samplesize.html. [last accessed 1 1 2019].
- Rosseel, Y. (2012). lavaan: An R Package for Structural Equation. Modeling. Journal of Statistical Software, 48(2), 998–36 http://www.jstatsoft.org/v48/i02/. [Google Scholar]
- Sawatzky, J.‐A. , Enns, C. L. , & Legare, C. (2015). Identifying the key predictors for retention in critical care nurses. Journal of Advanced Nursing, 71(10), 2315–2325. 10.1111/jan.12701 [DOI] [PubMed] [Google Scholar]
- Shwaihet, N. H. , & Nasaif, H. A. (2015). The relationship of participation in shared governance to work satisfaction among cardiovascular nurses working in a tertiary hospital in Saudi Arabia. Clinical Nursing Studies, 3(4), 79–87. 10.5430/cns.v3n4p79 [DOI] [Google Scholar]
- Spector, P. E. (1997). Job Satisfaction: Application, Assessment, Causes and Consequences. Thousand Oaks, CA: SAGE publications. [Google Scholar]
- Tourangeau, A. , Saari, M. , Patterson, E. , Ferron, E. M. , Thomson, H. , Widger, K. , & MacMillan, K. (2014). Work, work environments and other factors influencing nurse faculty intention to remain employed: A cross‐sectional study. Nursing Education Today, 34(2014), 940–947. 10.1016/j.nedt.2013.10.010 [DOI] [PubMed] [Google Scholar]
- Tuckett, A. , Winters‐Chang, P. , Bogossian, F. , & Wood, M. (2015). Why nurses are leaving the profession…lack of support from managers': What nurses from an e‐cohort study said. International Journal of Nursing Practice, 21(4), 359–366. 10.1111/ijn.12245 [DOI] [PubMed] [Google Scholar]
- Uhrenfeldt, L. , & Hall, E. O. C. (2015). Job satisfaction as a matter of time, team and trust: A qualitative study of hospital nurses' experiences. Journal of Nursing Education and Practice, 5(2), 998–1005. [Google Scholar]
- Ulrich, B. , Lavandero, R. , Woods, D. , & Early, S. (2014). Critical Care Nurse Work Environments 2013: A Status Report. Critical Care Nurse, 34(4), 64–79. 10.4037/ccn2014731 [DOI] [PubMed] [Google Scholar]
- Utriainen, K. , Ala‐Mursula, L. , & Kyngäs, H. (2015). Hospital nurses' wellbeing at work: A theoretical model. Journal of Nursing Management, 23(6), 736–743. 10.1111/jonm.12203 [DOI] [PubMed] [Google Scholar]
- Wargo‐Sugleris, M. , Robbins, W. , Lane, C. J. , & Phillips, L. R. (2017). Job satisfaction, work environment and successful aging: Determinants of delaying retirement among acute care nurses. Journal of Advanced Nursing, 74(4):900–913. 10.1111/jan.13504 [DOI] [PubMed] [Google Scholar]
- Weaver Moore, L. , Leahy, C. , Sublett, C. , & Lanig, H. (2013). Understanding nurse‐nurse relationships and their impact on work environments. MEDSURG Nursing, 22(3), 172–179. [PubMed] [Google Scholar]
- World Health Organization . (2015). World report on ageing and health. WHO Library Cataloguing‐in‐Publication Data . ISBN 978 92 4 069479 8 (ePub). Available from http://apps.who.int/iris/bitstream/10665/186463/1/9789240694811_eng.pdf. [last accessed 29 12 2017].
- World Health Organization (2016). Global strategic directions for strengthening nursing and midwifery 2016–2020. Available from http://www.who.int/hrh/nursing_midwifery/global-strategic-midwifery2016-2020.pdf. [last accessed 2 9 2017]. [PubMed]