

 This work is licensed under a
This work is licensed under a Abstract
Objective
To investigate the mutant status of BRAF gene and analyze its relationship to epidemiological risk factors and clinical outcomes among patients with papillary thyroid cancer (PTC) in the largest, single-institution Chinese cohort to date.
Methods
The medical records of 2048 PTC patients were reviewed in this retrospective study. Single-factor and multiple logistic regression analyses were applied to identify risk factors for BRAF V600E mutation. Survival outcomes including distant metastatic and persistent or recurrent PTC were examined, with a mean follow-up time of 23.4 (5–47) months.
Results
The BRAF V600E mutation was present in 83.7% of patients (1715 of 2048). Correlation was found between BRAF V600E mutation and several epidemiological features, including age, concomitant hypertension and Hashimoto thyroiditis (HT). For the clinicopathological features, BRAF V600E was significantly associated with bilateral multifocality (odds ratio (OR) 1.233, 95% confidence interval (CI) 1.063–1.431, P < 0.01) and less lateral lymph node metastases (OR 0.496, 95% CI 0.357–0.689, P < 0.01). Smaller tumor size and advanced disease stage were significant in single-factor analyses but became insignificant after multivariate adjustment. No association was found between BRAF V600E mutation and extrathyroidal invasion, distant metastatic and disease persistence or recurrence.
Conclusion
Part of epidemiological features are independent risk or protective factors for BRAF V600E mutation. The presence of BRAF V600E mutation is not an aggressive prognosis on poor clinical outcomes in PTC. However, the high prevalence of BRAF V600E may provide guidance for surgery strategy and opportunity for targeted treatment in recurrent and advanced stage disease.
Keywords: papillary thyroid cancer, BRAF V600E, epidemiological features, clinicopathological features
Introduction
Thyroid cancer, especially papillary subtype, is the most common malignancy in the endocrine system (1). Papillary thyroid cancer (PTC) can be further classified into conventional variant (CPTC), follicular variant (FVPTC) and other rare variants (2). Despite PTC is usually a well-differentiated thyroid carcinoma with a favorable prognosis, its incidence has been sharply rising in many countries over the last decades (3) (the average incidence in the USA was 2.4% from 1980 to 1997 and 6.6% from 1997 to 2009 (2)). In addition, recurrence and metastases are common for a small proportion of PTCs who reach advanced disease stages (4). In recent years, molecular markers have received extensive attention to improving risk stratification of PTC (5).
BRAF is the main subtype of RAF kinase and plays a key role in tumorigenesis. The mutation of BRAF V600E could trigger tumorigenesis through constitutively activating MAPK pathway (6). As the most common mutation observed in PTC, BRAF V600E has received special attention in various ethnic populations since this protein kinase may contribute to cell proliferation, growth and division. However, due to the limited large cohort evidence, the function of BRAF V600E as a biomarker in driving aggressiveness in PTC continues debatable (7, 8). The majority of researches claimed that BRAF V600E mutation was associated with poor clinicopathologic outcomes in patients with PTC, such as large tumor size, lymph node metastases, advanced clinical stages and recurrence (9, 10). By contrast, several studies suggested that BRAF V600E mutation had no significant association with clinical stage, multicentricity or recurrence (11, 12). These equivocal findings have hindered the fact that whether the mutation had an impact on aggressive behavior of PTC. Furthermore, most researches have focused on the relationship between mutation and clinicopathological characteristics, but the epidemiologic factors related to BRAF V600E mutations were rarely studied in previous researches. Here, we investigated epidemiological characteristics that may be associated with the mutation of BRAF V600E and then studied the role of BRAF V600E mutation in the clinicopathological features of PTC.
Patients and methods
Patient identification and clinicopathologic data collection
This study included 2048 patients (1556 women and 492 men) age 43.14 ± 11.01 years (mean ± s.d.) who were diagnosed with PTC and underwent surgery between January 2015 and July 2018 at the Department of the thyroid, breast and vascular surgery in Xijing Hospital. These patients were clinically observed with mean follow-up time of 23.4 months (range 5–47 months) after the initial treatments. All these patients were regularly followed with physical examinations, thyroid function tests and neck ultrasonography every 6–12 months after the initial surgery. If suspicious or indeterminate thyroid nodules or lymph nodes were found, ultrasound-guided fine-needle aspiration cytology (US-FNAC) was used for evaluation. Between January 2015 and July 2018, 2850 patients were diagnosed with thyroid cancer. Among these, 2805 patients (98.42%) were diagnosed with PTC, and 45 patients (1.58%) were diagnosed with other types of thyroid carcinoma. PTC patients without BRAF V600E status or lost to follow-up were excluded. The flow diagram of patient included was shown in Fig. 1.
Figure 1.

Flow diagram of patient included according to the inclusion and exclusion criteria.
After institutional review board approval and informed patient consenting, we retrospectively collected detailed BRAF V600E and clinicopathologic data from institutional patient records. The epidemiological data and clinicopathological features were summarized in Tables 1 and 2, respectively. Patients with alcohol history was defined as patients who drinking more than twice a month and lasting more than 1 year. Patients with smoking history was defined as patients who had a current or past smoking history of ≥6 months. Tumor node metastasis (TNM) stages were defined based on the seventh edition of the American Joint Committee on Cancer (AJCC) staging system. Persistent or recurrent disease was defined as the presence of a structural abnormality confirmed by cytological or surgical pathology after the initial surgery. The BRAF V600E mutation results had no influence on the treatment decision making.
Table 1.
Association of BRAF V600E with epidemiologic features of all PTC.
| BRAF V600E mutation (−) | BRAF V600E mutation (+) | χ2 | P value | |
|---|---|---|---|---|
| No. (%) | No. (%) | |||
| Total No. of cases | 333 (16.3) | 1715 (83.7) | ||
| Age at diagnosis | ||||
| ≤45 | 224 (20.3) | 881 (79.7) | 28.366 | <0.001 |
| >45 | 109 (11.6) | 834 (88.4) | ||
| Sex | ||||
| Male | 74 (15.0) | 418 (85.0) | 0.707 | 0.400 |
| Female | 259 (16.6) | 1297 (83.4) | ||
| Family history of cancer | ||||
| Had any family member(s) with history of cancer | 27 (11.4) | 209 (88.6) | 4.550 | 0.033 |
| None | 306 (22.5) | 1506 (77.5) | ||
| Presence of history of cancer | ||||
| Had any other cancer | 5 (12.5) | 35 (87.5) | 0.424 | 0.515 |
| None | 328 (16.3) | 1680 (83.7) | ||
| Presence of smoking history | ||||
| Ever | 28 (18.1) | 127 (81.9) | 0.401 | 0.527 |
| Never | 305 (16.1) | 1588 (83.9) | ||
| Presence of alcohol history | ||||
| Ever | 7 (15.2) | 39 (84.8) | 0.038 | 0.846 |
| Never | 326 (16.3) | 1676 (83.7) | ||
| Concomitant diabetes | ||||
| Yes | 8 (8.6) | 85 (91.4) | 4.196 | 0.041 |
| No | 325 (16.6) | 1630 (83.4) | ||
| Concomitant hypertension | ||||
| Yes | 18 (7.0) | 238 (93.0) | 18.300 | <0.001 |
| No | 315 (17.6) | 1477 (82.4) | ||
| Concomitant benign thyroid diseases | ||||
| Hyperthyroid | ||||
| Yes | 7 (24.1) | 22 (75.9) | / | 0.305 |
| No | 326 (16.1) | 1693 (83.9) | ||
| Nodular goiter | ||||
| Yes | 19 (20.4) | 74 (79.6) | 1.244 | 0.265 |
| No | 314 (16.1) | 1641 (83.9) | ||
| HT | ||||
| Yes | 96 (28.9) | 236 (71.1) | 46.611 | <0.001 |
| No | 237 (13.8) | 1479 (86.2) | ||
The chi-square test (χ2 test) or, for small cell sizes, Fisher’s exact test was employed to examine the significance of association between BRAF V600E and epidemiologic features. P value <0.05 was treated as statistically significant. Bold indicates statistical significance.
‘/’ means no χ2 value because cell sizes were small and Fisher’s exact test was employed. ‘%’ is the proportion of patients with or without BRAF V600E mutations in the subgroup of patients.
HT, Hashimoto thyroiditis.
Table 2.
Relationship of BRAF V600E with clinicopathological features of All PTC.
| BRAF V600E mutation (−) | BRAF V600E mutation (+) | χ2 | P value | |
|---|---|---|---|---|
| No. (%) | No. (%) | |||
| Total no. of cases | 333 (16.3) | 1715 (83.7) | ||
| Surgery | ||||
| Lobectomy | 53 (14.8) | 306 (85.2) | 0.716 | 0.397 |
| Total thyroidectomy | 280 (16.6) | 1409 (83.4) | ||
| Histological type | ||||
| CPTC | 321 (15.9) | 1701 (84.1) | / | <0.001 |
| FVPTC | 12 (46.2) | 14 (53.8) | ||
| Tumor size | ||||
| ≤2 cm | 290 (15.6) | 1564 (84.4) | 5.488 | 0.019 |
| >2 cm | 43 (22.2) | 151 (77.8) | ||
| Median (quartile), cm | 1.0 (0.7–1.5) | 0.9 (0.7–1.4) | ||
| Lesions | ||||
| Unilateral | 260 (18.0) | 1184 (82.0) | 10.959 | 0.001 |
| Bilateral | 73 (12.1) | 531 (87.9) | ||
| Extrathyroidal invasion | ||||
| Yes | 45 (15.6) | 244 (84.4) | 0.117 | 0.732 |
| No | 288 (16.4) | 1471 (83.6) | ||
| Vascular invasion | ||||
| Yes | 43 (15.4) | 237 (84.6) | 0.194 | 0.660 |
| No | 290 (16.4) | 1478 (83.6) | ||
| Status of lymph node metastasesa | ||||
| Yes | 190 (18.2) | 855 (81.8) | 3.704 | 0.054 |
| No | 127 (14.9) | 727 (85.1) | ||
| Site of lymph node metastases | ||||
| Only central | 92 (14.0) | 564 (86.0) | 20.648 | <0.001 |
| Only lateral | 13 (23.2) | 43 (76.8) | ||
| Central and lateral | 85 (25.5) | 248 (74.5) | ||
| Disease stage (7th edition)b | ||||
| I + II | 282 (17.8) | 1301 (82.2) | 6.718 | 0.010 |
| III + IV | 48 (12.3) | 341 (87.7) | ||
| Distant metastatic | ||||
| Yes | 1 (20.0) | 4 (80.0) | / | 1.000 |
| No | 332 (16.3) | 1711 (83.7) | ||
| Persistent or recurrent disease | ||||
| Yes | 19 (22.1) | 67 (77.9) | 2.243 | 0.134 |
| No | 314 (16.0) | 1648 (84.0) | ||
The chi-square test (χ2 test) or, for small cell sizes, Fisher’s exact test was employed to examine the significance of association between BRAF V600E and clinicopathological features. P value <0.05 was treated as statistically significant. Bold indicates statistical significance. Tumor size was summarized with medians (quartile).
‘/’means no χ2 value because cell sizes were small and Fisher’s exact test was employed. ‘%’ is the proportion of patients with or without BRAF V600E mutations in the subgroup of patients. ‘a’ means there are missing cases in ‘Status of lymph node metastases’. In patients without BRAF V600E mutations, 16 patients had undetermined lymph node metastasis status. In patients with BRAF V600E mutations, 133 patients had undetermined lymph node metastasis status. ‘b’ means there are missing cases in ‘Disease stage’. In patients without BRAF V600E mutations, the disease stage of three patients cannot be determined. In patients with BRAF V600E mutations, the disease stage of 73 patients cannot be determined.
CPTC, conventional papillary thyroid carcinoma; FVPTC, follicular variant papillary thyroid carcinoma.
Mutational analyses
BRAF V600E mutational analyses were performed by pathologists after surgical treatments of patients. DNA was isolated from formalin-fixed, paraffin-embedded (FFPE) tissue blocks by SDS-proteinase K method and subjected to Amplification Refractory Mutation System (ARMS)- real-time PCR for the detection of BRAF V600E mutations. DNA was extracted from each sample via a commercial kit (FFPE DNA reagent, Cat No. ADx-FF01) according to the manufacturer’s instructions. Typically, 5 μm sections (2–4 pieces) were carefully micro-dissected from FFPE tissue blocks. The sections were initially treated with 1.5 mL xylene/ethanol three times, then digested during an overnight incubation with 20 μL proteinase K solution and 180 μL buffer DTL in a 56°C rotating incubator, and DNA purification was performed through QIAgen columns, according to the manufacturer’s instructions. Then, the most common T1799A transversion (BRAF V600E) mutation was studied. The PCR was used to amplify exon 15 of the BRAF gene, which was detected by BRAF V600 Mutations Detection Kit (Applied by ADx-BR01, AmoyDx Company, China) according to the manufacturer’s instructions. PCR primer sequences were as follows: forward primer, TCTGTAGCAGCCCTCAGTAGCGAAGCAGTGATTTTGGTCTAGCTACAGA; reverse primer, AGCCCTCAGTAGCGAAGCAACTCAGCAGCATCTCAGG. BRAF gene reactions were performed in a final volume of 40 μL using as template 10–15 ng of genomic DNA, with 1× buffer including 14 pmol forward primer, 20 pmol reverse primer, 12.5 pmol dNTPs, 350 pmol MgCl2, mutant probe 20 pmol and 1 unit of Taq polymerase. Each reaction included a positive and a negative control sample, and in negative sample, DNA template was substituted by water. PCR recycling started with initial denaturation step at 95°C for 5 min, followed by 40 cycles of denaturation (95°C, 25 s), annealing (64°C, 20 s) and extension (72°C, 20 s) and a last step of 10 min extension at 72°C. PCR efficiency was determined by measuring the Ct value of FAM signal.
Statistical analyses
Data related to histologic characteristics, patient epidemiological data and clinical outcomes were collected. Categorical data were summarized with frequencies and percentages. Continuous data were summarized with means ± standard deviations (if it is a normal distribution) or medians and quartile (if it is not a normal distribution). The chi-square test (χ2 test) or, for small cell sizes, Fisher’s exact test was employed to examine categorical variables. All P values were two-sided, and a P value <0.05 was treated as statistically significant. Pooled ORs with their corresponding 95% confidence intervals (95% CIs) were calculated to assess the relationship between BRAF V600E mutation and clinicopathological features. All statistical analyses were conducted by the software of SPSS with version 23.0.
Results
BRAF V600E mutation in PTC
There were 2048 patients included in the study with an average age of 43.14 ± 11.01 (range 5–80), and 76.0% of the patients were female (1556 women and 492 men). BRAF V600E mutation was found in 1701 of 2022 (84.1%) CPTCs, and 14 of 26 (53.8%) FVPTCs, with an overall prevalence of 83.7% (1715 of 2048). No significant difference of BRAF V600E mutation was observed in female and male patients (P = 0.400). With regard to ages, significant difference of BRAF V600E incidence was found between patients aged ≤45 and >45 years (79.7 vs 88.4%, P < 0.001). To further investigate the influence of age on mutational incidence, we divided all patients into children/adolescent group (≤25 years) and adults groups of various age ranges (25–35, 35–45, 45–55, >55 years old). As shown in Fig. 2, patients were more prone to be BRAF V600E positive with the growth of age.
Figure 2.
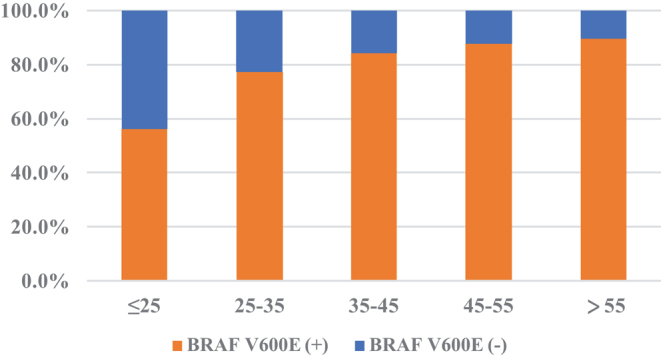
The correlation between the presence of the BRAF V600E mutation and the age of patients at the time of diagnosis.
Association of BRAF V600E and epidemiological features in PTCs
To identify epidemiological factors associated with BRAF V600E mutation, the relationship between epidemiological features and the mutation was investigated. In the univariate analysis of 2048 PTCs (Table 1), the presence of BRAF V600E mutation was found to be significantly associated with several epidemiological features, including age at diagnosis, family history of cancer, concomitant diabetes, hypertension and Hashimoto thyroiditis (HT). The incidence of BRAF V600E mutations in patients with family cancer history was higher than that in patients without family history of cancer (88.6 vs 77.5%, P = 0.033). Interestingly, patients with diabetes or hypertension presented higher mutation rates than those who did not have diabetes or hypertension (91.4 vs 83.4%, P = 0.041; 93.0 vs 82.4%, P < 0.001). Conversely, the patients concomitant of HT displayed less BRAF V600E mutations than patients without HT (71.1 vs 86.2%, P < 0.001). Similarly, patients with hyperthyroid or nodular goiter showed lower mutation frequency than those who did not have hyperthyroid or nodular goiter, but the association was insignificant. Except the factors mentioned above, no significant association was found between the presence of BRAF V600E mutation and other features including gender, presence of history of cancer, presence of smoking and alcohol history.
Relationship of BRAF V600E and clinicopathological features in PTCs
In the univariate analysis of all PTCs (Table 2), the presence of BRAF V600E was found to be significantly associated with small tumor size (P = 0.019), bilateral multifocality (P = 0.001), less central and lateral lymph node metastases simultaneously (P < 0.001) and advanced disease stage (III and IV) (P = 0.010). Although there was no significant association, less BRAF V600E mutation was found in patients with lymph node metastases than patients without lymph node metastases (81.8 vs 85.1%, P = 0.054). Furthermore, it was worth noticing that less BRAF V600E presented in patients with aggressive lymph node metastases (central and lateral metastases at the same time) than patients with only central or only lateral lymph node metastases (74.5 vs 86.0% or 76.8%, P < 0.001). No significant association was found between BRAF V600E mutation and another high-risk clinicopathologic characteristics, such as extrathyroidal invasion (P = 0.732), vascular invasion (P = 0.660), distant metastatic (P = 1.000) and PTC persistence or recurrence (P = 0.134).
Multivariate logistic regression analysis of BRAF V600E mutation in PTCs
To further confirm the relationship between BRAF V600E and epidemiological or clinicopathological features, multivariate logistic regression analysis was performed (Table 3). The results showed that age (P = 0.002, OR = 1.024, 95% CI = 1.009–1.041), concomitant hypertension (P = 0.032, OR = 1.812, 95% CI = 1.052–3.120) and lesions (P = 0.006, OR = 1.233, 95% CI = 1.063–1.431) were positive independent factors for BRAF V600E mutation. In contrast, concomitant HT (P < 0.001, OR = 0.402, 95% CI = 0.300–0.538) and lateral lymph node metastases (P < 0.001, OR = 0.496, 95% CI = 0.357–0.689) were negative independent factors for BRAF V600E mutation. After adjustment for patients’ age and sex, the association between BRAF V600E mutation and disease stage was not statistically significant (P = 0.771, OR = 1.028, 95% CI = 0.856–1.234).
Table 3.
Multivariate logistic regression analysis of BRAF V600E mutation of all PTC.
| BRAF V600E mutation (n, %) | P Value | OR | 95% CI | ||
|---|---|---|---|---|---|
| − | + | ||||
| Age at diagnosis | 39.29 ± 11.44 | 43.88 ± 10.77 | 0.002 | 1.024 | 1.009–1.041 |
| Sex | 0.750 | 1.051 | 0.773–1.431 | ||
| Male | 74 (15.0%) | 418 (85.0%) | |||
| Female | 259 (16.6%) | 1297 (83.4%) | |||
| Family history of cancer | 0.195 | 1.352 | 0.857–2.131 | ||
| Had any family member(s) with history of cancer | 27 (11.4%) | 209 (88.6%) | |||
| None | 306 (22.5%) | 1506 (77.5%) | |||
| Concomitant diabetes | 0.428 | 1.389 | 0.616–3.129 | ||
| Yes | 8 (8.6%) | 85 (91.4%) | |||
| No | 325 (16.6%) | 1630 (83.4%) | |||
| Concomitant hypertension | 0.032 | 1.812 | 1.052–3.120 | ||
| Yes | 18 (7.0%) | 238 (93.0%) | |||
| No | 315 (17.6%) | 1477 (82.4%) | |||
| Concomitant HT | <0.001 | 0.402 | 0.300–0.538 | ||
| Yes | 96 (28.9%) | 236 (71.1%) | |||
| No | 237 (13.8%) | 1479 (86.2%) | |||
| Tumor size | 1.0 (0.7–1.5) | 0.9 (0.7–1.4) | 0.571 | 0.950 | 0.795–1.135 |
| Lesions | 0.006 | 1.233 | 1.063–1.431 | ||
| Unilateral | 260 (18.0%) | 1184 (82.0%) | |||
| Bilateral | 73 (12.1%) | 531 (87.9%) | |||
| Site of lymph node metastasis | |||||
| Central | 177 (17.9%) | 811 (82.1%) | 0.346 | 1.157 | 0.854–1.568 |
| Lateral | 98 (25.2%) | 290 (74.8%) | <0.001 | 0.496 | 0.357–0.689 |
| Disease stage (7th edition)a | 0.771 | 1.028 | 0.856–1.234 | ||
| I + II | 282 (17.8%) | 1301 (82.2%) | |||
| III + IV | 48 (12.3%) | 341 (87.7%) | |||
Age at diagnosis was summarized with means ± standard deviations. Tumor size was summarized with medians (quartile). Multivariate logistic regression analysis was employed to identify risk factors for BRAF V600E mutations. P value <0.05 was treated as statistically significant. Bold indicates statistical significance.
‘%’ is the proportion of patients with or without BRAF V600E mutations in the subgroup of patients. ‘a’ means there are missing cases in ‘Disease stage’. In patients without BRAF V600E mutations, the disease stage of three patients cannot be determined. In patients with BRAF V600E mutations, the disease stage of 73 patients cannot be determined.
HT, Hashimoto thyroiditis; OR, odds ratio; 95% CI, 95% confidence interval.
Discussion
This study sought to find the epidemiological factors associated with BRAF V600E mutation and clarify the relationship between BRAF V600E mutation and clinical outcomes in PTC. Previously, the BRAF V600E mutation has been reported as an aggressive prognosis in PTC, although a large cohort study was inadequate and there have been noteworthy inconsistencies in some studies (13, 14). In our analysis, we found a lack of correlation between BRAF V600E mutation and either aggressive clinicopathological features or persistent or recurrent disease.
The incidence of BRAF V600E mutation increased in recent years, it seems that BRAF V600E mutation gradually become the accompanying phenomenon for PTC patients. Mingzhao Xing et al. reported BRAF V600E rate of 38.3% in patients between 1990 and 2012 (15). In 2007, Electron et al. reported the prevalence of BRAF V600E was 46.4% (16). In 2012, Kurtulmus et al. showed BRAF V600E mutation rate of 39.45% in PTCs (17). The meta-analysis showed BRAF V600E mutations occurred in 60.6% of PTCs (update to August, 2015) (6). In 2016, Kim et al. reported BRAF V600E mutations were presented in 83.7% PTC patients (2789 of 3332) (18), and we found the similar mutation rate in our sample. Compared to previous researches, we update BRAF V600E mutation data from 2015 to 2018. The reason why mutation prevalence in our study is higher than the average may ascribe to population aging in recent years and different research methodology. In this study, the BRAF V600E mutations were tested from the postoperative tissue samples using the ARMS- real-time PCR method, which was more sensitive and robust at detecting BRAF V600E somatic mutations than DNA sequencing on clinical samples (19).
Our study indicated that older age and concomitant hypertension were independent risk factors of BRAF V600E mutation. On the contrary, concomitant HT was an independent protective factor of the mutation. Despite being insignificant after multivariate adjustment, the presence of family history of cancer was associated with higher BRAF V600E mutation incidence in the univariate analysis, which were in agreement with the data reported in previous study (20). In addition, with the large size of this study, negative correlation between HT and BRAF V600E mutation was demonstrated, which was confirmed in a recent smaller study (21). Potential mechanisms and immunological link that might lead to the synchronous appearance of HT and PTC had been investigated (22, 23). If there is more clinical evidence, the correlation between BRAF V600E and family history of cancer, hypertension and HT may help to promote the investigation of BRAF V600E mutation mechanism. As for the factor of age, plenty of researches had found that incidence of BRAF V600E was higher in patients >45 years old (10, 16), but few studies found the positive correlation between BRAF V600E and age (Fig. 2). Compared to adults, PTC in pediatric and adolescents presents more lymph node metastases, distant metastases and recurrence (24, 25). Combining the study mentioned above, the phenomenon that less number of BRAF V600E mutations appears in patients aged under 25 years suggested that aggressive features displayed in these patients may not be caused by BRAF V600E mutation.
The aggressive role of BRAF V600E mutations has been widely investigated in previous studies (6, 8, 10). However, our results did not show that BRAF V600E mutation is a biomarker in driving aggressiveness. Given the high and increased prevalence of BRAF V600E mutation in recent years (60.6%, on average, in the meta-analysis mentioned above (6), and 83.7% in our study), and the oppositely indolent behavior, the rarity recurrence and mortality of PTC (16 and 3%, respectively) (26, 27), an absence of association between BRAF V600E mutation, and these negative events seem logical. In univariate analyses, BRAF V600E mutations were significantly associated with smaller tumor, bilateral multifocality, advanced disease stage and less aggressive lymph node metastases in PTCs. Advanced TNM stage showed insignificant after multivariate adjustment. Therefore, bilateral multifocality seems to be the only risk factor associated with BRAF V600E. Notably, a recent study showed tumor multifocality has no independent risk prognostic value in outcomes of PTC (28). Other classic risk factors (29), such as extrathyroidal extension, distant metastases and disease recurrence, were insignificantly associated with BRAF V600E mutation. Therefore, presence of BRAF V600E is not an aggressive role associated with poor clinicopathologic outcomes in PTC. A recent publication has called into question the relationship of BRAF V600E mutation and prognosis in PTC. In the analysis of 508 patients with BRAF V600E mutation, Henke et al. found the mutation is not predictive of long-term outcome in PTC (7).
Although the presence of BRAF V600E mutation is not an aggressive prognosis on poor clinical outcomes, surgery strategy and treatment guided by the presence of the mutation may be available. Such therapies might include determining surgery extent and the use of BRAF inhibitors. The association between BRAF V600E and bilateral lesions and less lateral lymph node metastases was found in our study. If there is more clinical evidence in the future, the status of BRAF V600E mutation may be considered as one of the factors for determining the surgery extent besides tumor size, extrathyroidal extension, vascular invasion, lymph node size and willingness of patients (30). Furthermore, considerable patients with BRAF V600E mutation will have recurrence since a majority of PTC patients in our cohort (83.7%) had the mutation. We propose that high-risk patients with BRAF V600E mutation use BRAF inhibitors, such as sorafenib, lenvatinib and vemurafenib. Those patients might benefit from the targeted therapy, which (sorafenib and lenvatinib) have been approved for metastatic PTC (31).
The greatest strengths of this study are its consecutive large cohort (2048 PTC patients) and its latest research time (from 2015 to 2018). The limitations of this study were as follows. First, a selection bias could occur in this retrospective unicentral research. The large consecutive cohort of patients may help minimize the bias. Second, follow-up time was short in this study (mean 23.4 months, range, 5–47 months). And research on the mechanism of epidemiological features associated with BRAF V600E mutation in PTCs should be carried out in the future.
In summary, this was a large consecutive retrospective study that investigated the relationship of BRAF V600E mutation with epidemiological and clinicopathological features. Older age and concomitant hypertension were independent risk factors of BRAF V600E mutation. Concomitant HT was an independent protective factor for the BRAF V600E expression. Bilateral multifocality was the only risk factor associated with BRAF V600E but a recent study showed it has no independent risk prognostic value in outcomes of PTC. Other poor clinicopathological features were insignificantly associated with the mutation. Although the presence of BRAF V600E mutation is not an aggressive prognosis on poor clinical outcomes, surgery and treatment guided by the presence of the mutation may be available.
Declaration of interest
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding
The authors would like to acknowledge support from the National Natural Science Foundation of China (No. 81572917).
Ethical approval
Consent has been obtained from each patient after full explanation of the purpose and nature of all procedures used. The study was approved by an independent ethics committee of Xijing Hospital (first affiliated hospital of Fourth Military Medical University).
References
- 1.Pacini F, Castagna MG. Approach to and treatment of differentiated thyroid carcinoma. Medical Clinics of North America 2012. 96 . ( 10.1016/j.mcna.2012.01.002) [DOI] [PubMed] [Google Scholar]
- 2.Pellegriti G, Frasca F, Regalbuto C, Squatrito S, Vigneri R. Worldwide increasing incidence of thyroid cancer: update on epidemiology and risk factors. Journal of Cancer Epidemiology 2013. 2013 965212 ( 10.1155/2013/965212) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jung CK, Little MP, Lubin JH, Brenner AV, Wells SA, Jr, Sigurdson AJ, Nikiforov YE. The increase in thyroid cancer incidence during the last four decades is accompanied by a high frequency of BRAF mutations and a sharp increase in RAS mutations. Journal of Clinical Endocrinology and Metabolism 2014. 99 E276–E285. ( 10.1210/jc.2013-2503) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vuong HG, Altibi AM, Abdelhamid AH, Ngoc PU, Quan VD, Tantawi MY, Elfil M, Vu TL, Elgebaly A, Oishi N, et al The changing characteristics and molecular profiles of papillary thyroid carcinoma over time: a systematic review. Oncotarget 2017. 8 . ( 10.18632/oncotarget.12885) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nikiforov YE, Nikiforova MN. Molecular genetics and diagnosis of thyroid cancer. Nature Reviews: Endocrinology 2011. 7 . ( 10.1038/nrendo.2011.142) [DOI] [PubMed] [Google Scholar]
- 6.Zhang Q, Liu SZ, Zhang Q, Guan YX, Chen QJ, Zhu QY. Meta-analyses of association between BRAF(V600E) mutation and clinicopathological features of papillary thyroid carcinoma. Cellular Physiology and Biochemistry 2016. 38 . ( 10.1159/000443032) [DOI] [PubMed] [Google Scholar]
- 7.Henke LE, Pfeifer JD, Ma C, Perkins SM, DeWees T, El-Mofty S, Moley JF, Nussenbaum B, Haughey BH, Baranski TJ, et al BRAF mutation is not predictive of long-term outcome in papillary thyroid carcinoma. Cancer Medicine 2015. 4 . ( 10.1002/cam4.417) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tufano RP, Teixeira GV, Bishop J, Carson KA, Xing M. BRAF mutation in papillary thyroid cancer and its value in tailoring initial treatment: a systematic review and meta-analysis. Medicine 2012. 91 . ( 10.1097/MD.0b013e31826a9c71) [DOI] [PubMed] [Google Scholar]
- 9.Xing M, Westra WH, Tufano RP, Cohen Y, Rosenbaum E, Rhoden KJ, Carson KA, Vasko V, Larin A, Tallini G, et al BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2005. 90 . ( 10.1210/jc.2005-0987) [DOI] [PubMed] [Google Scholar]
- 10.Kim TH, Park YJ, Lim JA, Ahn HY, Lee EK, Lee YJ, Kim KW, Hahn SK, Youn YK, Kim KH, et al The association of the BRAF(V600E) mutation with prognostic factors and poor clinical outcome in papillary thyroid cancer: a meta-analysis. Cancer 2012. 118 . ( 10.1002/cncr.26500) [DOI] [PubMed] [Google Scholar]
- 11.Walczyk A, Kowalska A, Kowalik A, Sygut J, Wypiorkiewicz E, Chodurska R, Pieciak L, Gozdz S. The BRAF(V600E) mutation in papillary thyroid microcarcinoma: does the mutation have an impact on clinical outcome? Clinical Endocrinology 2014. 80 . ( 10.1111/cen.12386) [DOI] [PubMed] [Google Scholar]
- 12.Nam JK, Jung CK, Song BJ, Lim DJ, Chae BJ, Lee NS, Park WC, Kim JS, Jung SS, Bae JS. Is the BRAF(V600E) mutation useful as a predictor of preoperative risk in papillary thyroid cancer? American Journal of Surgery 2012. 203 . ( 10.1016/j.amjsurg.2011.02.013) [DOI] [PubMed] [Google Scholar]
- 13.Russo M, Malandrino P, Nicolosi ML, Manusia M, Marturano I, Trovato MA, Pellegriti G, Frasca F, Vigneri R. The BRAF(V600E) mutation influences the short- and medium-term outcomes of classic papillary thyroid cancer, but is not an independent predictor of unfavorable outcome. Thyroid 2014. 24 . ( 10.1089/thy.2013.0675) [DOI] [PubMed] [Google Scholar]
- 14.Gandolfi G, Sancisi V, Piana S, Ciarrocchi A. Time to re-consider the meaning of BRAF V600E mutation in papillary thyroid carcinoma. International Journal of Cancer 2015. 137 . ( 10.1002/ijc.28976) [DOI] [PubMed] [Google Scholar]
- 15.Xing M, Liu R, Liu X, Murugan AK, Zhu G, Zeiger MA, Pai S, Bishop J. BRAF V600E and tert promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. Journal of Clinical Oncology 2014. 32 . ( 10.1200/JCO.2014.55.5094) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kebebew E, Weng J, Bauer J, Ranvier G, Clark OH, Duh QY, Shibru D, Bastian B, Griffin A. The prevalence and prognostic value of BRAF mutation in thyroid cancer. Annals of Surgery 2007. 246 ; discussion . ( 10.1097/SLA.0b013e318148563d) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kurtulmus N, Duren M, Ince U, Cengiz Yakicier M, Peker O, Aydin O, Altiok E, Giray S, Azizlerli H. BRAF(V600E) mutation in Turkish patients with papillary thyroid cancer: strong correlation with indicators of tumor aggressiveness. Endocrine 2012. 42 . ( 10.1007/s12020-012-9651-x) [DOI] [PubMed] [Google Scholar]
- 18.Kim SK, Woo JW, Lee JH, Park I, Choe JH, Kim JH, Kim JS. Chronic lymphocytic thyroiditis and BRAF V600E in papillary thyroid carcinoma. Endocrine-Related Cancer 2016. 23 . ( 10.1530/ERC-15-0408) [DOI] [PubMed] [Google Scholar]
- 19.Ellison G, Donald E, McWalter G, Knight L, Fletcher L, Sherwood J, Cantarini M, Orr M, Speake G. A comparison of ARMS and DNA sequencing for mutation analysis in clinical biopsy samples. Journal of Experimental and Clinical Cancer Research 2010. 29 132 ( 10.1186/1756-9966-29-132) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zhang Q, Song F, Zheng H, Zhu X, Song F, Yao X, Zhang L, Chen K. Association between single-nucleotide polymorphisms of BRAF and papillary thyroid carcinoma in a Chinese population. Thyroid 2013. 23 . ( 10.1089/thy.2012.0228) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zeng RC, Jin LP, Chen ED, Dong SY, Cai YF, Huang GL, Li Q, Jin C, Zhang XH, Wang OC. Potential relationship between Hashimoto’s thyroiditis and BRAF(V600E) mutation status in papillary thyroid cancer. Head and Neck 2016. 38 (Supplement 1) E1019–E1025. ( 10.1002/hed.24149) [DOI] [PubMed] [Google Scholar]
- 22.Ehlers M, Schott M. Hashimoto’s thyroiditis and papillary thyroid cancer: are they immunologically linked? Trends in Endocrinology and Metabolism 2014. 25 . ( 10.1016/j.tem.2014.09.001) [DOI] [PubMed] [Google Scholar]
- 23.Boi F, Pani F, Mariotti S. Thyroid autoimmunity and thyroid cancer: review focused on cytological studies. European Thyroid Journal 2017. 6 . ( 10.1159/000468928) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Spinelli C, Rossi L, Piscioneri J, Strambi S, Antonelli A, Ferrari A, Massimino M, Miccoli P. Pediatric differentiated thyroid cancer: when to perform conservative and radical surgery. Current Pediatric Reviews 2016. 12 . ( 10.2174/1573396312666161014092023) [DOI] [PubMed] [Google Scholar]
- 25.Al-Qurayshi Z, Hauch A, Srivastav S, Aslam R, Friedlander P, Kandil E. A national perspective of the risk, presentation, and outcomes of pediatric thyroid cancer. JAMA Otolaryngology: Head and Neck Surgery 2016. 142 . ( 10.1001/jamaoto.2016.0104) [DOI] [PubMed] [Google Scholar]
- 26.Xing M, Alzahrani AS, Carson KA, Shong YK, Kim TY, Viola D, Elisei R, Bendlova B, Yip L, Mian C, et al Association between BRAF V600E mutation and recurrence of papillary thyroid cancer. Journal of Clinical Oncology 2015. 33 . ( 10.1200/JCO.2014.56.8253) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Xing M, Alzahrani AS, Carson KA, Viola D, Elisei R, Bendlova B, Yip L, Mian C, Vianello F, Tuttle RM, et al Association between BRAF V600E mutation and mortality in patients with papillary thyroid cancer. JAMA 2013. 309 . ( 10.1001/jama.2013.3190) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wang F, Yu X, Shen X, Zhu G, Huang Y, Liu R, Viola D, Elisei R, Puxeddu E, Fugazzola L, et al The prognostic value of tumor multifocality in clinical outcomes of papillary thyroid cancer. Journal of Clinical Endocrinology and Metabolism 2017. 102 . ( 10.1210/jc.2017-00277) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM, Schlumberger, et al 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016. 26 . ( 10.1089/thy.2015.0020) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wang TS, Sosa JA. Thyroid surgery for differentiated thyroid cancer – recent advances and future directions. Nature Reviews: Endocrinology 2018. 14 . ( 10.1038/s41574-018-0080-7) [DOI] [PubMed] [Google Scholar]
- 31.Brose MS, Nutting CM, Jarzab B, Elisei R, Siena S, Bastholt L, de la Fouchardiere C, Pacini F, Paschke R, Shong YK, et al Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet 2014. 384 . ( 10.1016/S0140-6736(14)60421-9) [DOI] [PMC free article] [PubMed] [Google Scholar]