

Abstract
Background:
Although recent federal mandate provides incentives for physicians to use electronic prescribing (e‐prescribing), clinical end points to support its use are lacking.
Hypothesis:
E‐prescribing should improve low‐density lipoprotein (LDL) goal attainment.
Methods:
In this retrospective cohort study, we queried the electronic medical records (Allscripts Electronic Health Record [EHR]) of a multispecialty outpatient academic medical practice to identify patient encounters during which consecutive lipid panels were drawn in 2007 (n = 2218). The EHR did not include a clinical decision tool for guideline adherence but did include formulary decision support (FDS), which informs physicians about drug costs specific to each patient. Logistic regression was used to examine whether the odds of reaching LDL goal were influenced by e‐prescribing and adjusted for characteristics known to affect prescribing patterns and goal attainment.
Results:
Of 796 patients not at LDL goal at baseline, 49% (n = 393) were at goal at follow‐up. Patients receiving an e‐prescription with FDS were 59% more likely to achieve LDL goal than those with a manual prescription (95% confidence interval [CI]: 1.12–2.25). Superior LDL goal attainment may be from lower cost of medications; patients with an e‐prescription were significantly more likely to receive a generic statin than patients with a manual prescription (38% vs 22.9%; P = 0.0004), and for each $10 increase in prescription price, the likelihood of being at goal decreased by 5% (odds ratio = 0.95; 95% CI: 0.93–0.98).
Conclusions:
Our study is the first to demonstrate that e‐prescribing with FDS is associated with improved LDL goal attainment. Therefore, e‐prescribing can deliver tangible clinical gains to patients, likely from improved adherence to more affordable treatment. © 2011 Wiley Periodicals, Inc.
Presented at American College of Cardiology Meeting, Atlanta, Georgia, March 14, 2010.
This work was supported in part by the W. T. Gill Jr. Fellowship, George Washington University. The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Introduction
Lowering low‐density lipoprotein cholesterol (LDL) reduces the incidence of coronary and cerebrovascular events across a broad spectrum of at‐risk patients.1, 2 Guidelines established by the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) outline specific LDL goals for patients based on their cardiovascular risk and suggest strategies for reaching them.3, 4
Over the past decade, guideline adherence and LDL goal attainment have improved.5 However, according to the Lipid Treatment Assessment Project 2, the success rate for LDL goal achievement is 73% overall and only 30% in patients at the highest risk of developing coronary heart disease (CHD). Furthermore, it is estimated that less than one half of individuals who would benefit from lipid‐lowering therapy actually receive it.3 This treatment gap likely results from failure by physicians to monitor their patients' lipids levels and appropriately adjust therapy as well as poor patient persistence in taking medications as prescribed.6
Recently, the federal government has identified electronic prescribing (e‐prescribing) as a valuable tool in the delivery of effective patient care and provides physicians with financial incentives to encourage its use.7, 8 Although clinical end points to support its utilization are lacking, there is evidence to show that it is associated with increased administration of needed medications and fewer medical errors.9 Additionally, e‐prescribing with formulary decision support (FDS) enables physicians to prescribe “tier 1” medications, those with the lowest copayment, more frequently, with substantial financial savings to the patient.10 This finding is significant, because there is evidence that an increase in cost of medications, specifically those indicated for lowering LDL levels, negatively impacts patient adherence.11, 12
Therefore, there is evidence to suggest that use of e‐prescribing could enhance treatment effectiveness for patients with elevated LDL based on its ability to increase patient adherence by decreasing cost of medications. We investigated whether e‐prescribing with FDS is correlated with improved attainment of patient's NCEPT ATP III guidelines‐based LDL goals. Additionally, we determined whether there is any association between LDL goal attainment and other potentially influential variables, including the patient's risk category, gender of the patient, and physician characteristics.
Methods
Study Cohort
In this retrospective cohort study, we queried the electronic medical records (Allscripts Electronic Health Record [EHR]; Allscripts‐Misys Healthcare Solutions, Inc., Chicago, IL) of the George Washington University Medical Faculty Associates to identify patient encounters in which a lipid panel was drawn between January 1, 2007 and December 31, 2007. All physicians used the EHR and had the option to e‐prescribe. The EHR did not include a clinical decision tool for guideline adherence but did include FDS (Figure 1). The years 2006 and 2008 were excluded due to major changes in prescribing patterns during these years; simvastatin became available in a generic preparation in 2006,13 and in 2008, results of a clinical trial of ezetimibe highlighted its potential negative effects.14 Years prior to 2006 were excluded because the most recent cholesterol guideline update was published in 2004,4 and practice patterns may not have changed sufficiently in 2005. Patients were included in the analysis if they were at least 18 years of age and had a lipid panel drawn on 2 separate encounters. For inclusion in the study, encounters had to be with a primary care physician, cardiologist, or endocrinologist. Encounters were excluded if the LDL level could not be determined (eg, triglyceride [TRIG] >400 mg/dL), or after chart review there was insufficient information to determine the patient's LDL goal. The institutional review board at the George Washington University Medical Center approved the study, and the need for written informed consent was waived.
Figure 1.
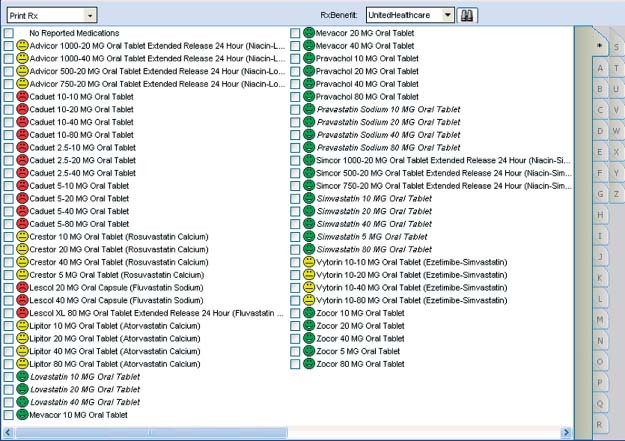
Screen shot example of formulary decision support from the Allscripts Electronic Health Record. Green “happy faces” indicate low co‐pay; red “unhappy faces” indicate high co‐pay; yellow “straight faces” indicate medium co‐pay.
Study Measurements
We determined each patient's LDL goal by the level of cardiovascular risk at the time of the encounter in accordance with the update to the NCEP ATP III guidelines.4 At each encounter, the lipid panel values that were reported included total cholesterol, LDL, high‐density lipoprotein (HDL), and TRIG. In accordance with the NCEP ATP III algorithm, patients were divided into 3 risk categories, and their LDL goals were determined accordingly: (1) established CHD, 10‐year risk of developing CHD according to the Framingham risk assessment tool >20%, and CHD risk equivalents with LDL goal <100 mg/dL; (2) multiple (2+) risk factors or 10‐year Framingham risk of 10% to 20% with LDL goal <130 mg/dL; and (3) 0 to 1 risk factor with LDL goal <160 mg/dL. The presence of CHD, CHD equivalents, or risk factors was ascertained by review of patient records on Allscripts EHR. Some of these patients were further categorized as “very high risk,” with history of acute coronary syndrome, the presence of CHD plus multiple major risk factors (2 or more of the following: cigarette smoking, hypertension, family history of premature CHD, CHD risk equivalent) or CHD plus multiple risk factors of the metabolic syndrome (TRIG ≥200 mg/dL plus non‐HDL ≥130 mg/dL with low HDL).4 These very high risk patients were assigned an LDL goal <70 mg/dL. For each encounter, it was determined whether the patient was at LDL goal, and the dose(s) and type(s) of anti hyperlipidemic medication(s) prescribed before and after the lipid panel was drawn were determined from the relevant physician's notes. It was also noted whether the patient was advised to make therapeutic lifestyle changes. The total cost of medications for each encounter was calculated using approximate retail prices.15 Whether these medications were ordered via e‐prescription was determined from Allscripts EHR. Because physician characteristics have been shown to influence hypertension management, we conducted a similar analysis of variables that may affect guideline adherence: physician age, years since medical school graduation, and years since last American Board of Internal Medicine (ABIM) certification.16
Statistical Analysis
A χ 2 analysis was used to determine if there were significant differences in prescription patterns by e‐prescribing habits. Hierarchical logistic regression analysis was used to examine if the odds of reaching LDL goal were influenced by e‐prescription and retail price while controlling for provider specialty, insurance type, provider age, provider years since ABIM certification, provider years since graduation, patient age, gender, prescription drugs that were prescribed to more than 5% of the study cohort, and targeted NCEP ATP III LDL goal. A multilevel model was chosen to account for the clustering of patients by provider. PROC GLIMMIX in SAS version 9.2 (SAS Institute Inc., Cary, NC) was used to control for the intraclass correlation by provider. A P value <0.05 defined statistical significance.
Results
Patient Characteristics
We identified 2218 patient encounters during which consecutive lipid panels were drawn in 2007. At initial presentation, 796 patients were not at their NCEP ATP III LDL goal; 612 (77%) received an e‐prescription with FDS, and 184 had a manual prescription (Figure 2, Figure 3). The average time between the initial lipid panel and follow‐up was 4.6 ± 2.4 months (mean ± standard deviation) in the e‐prescription group, and 4.7 ± 2.5 months in the manual prescription group. Patient characteristics are shown in Table 1. The greater number of risk factors in the e‐prescription group necessitated a more aggressive LDL goal.
Figure 2.
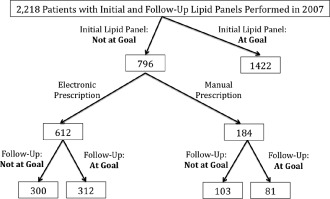
Flow chart of patients included in the study.
Figure 3.
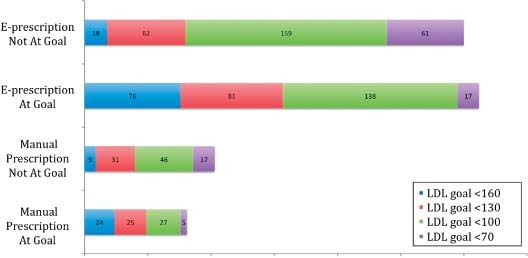
Bar graph of patients at follow‐up by low‐density lipoprotein (LDL) goal.
Table 1.
Patient Characteristics (n = 2218) at Time of Initial Evaluation
| E‐Prescription (n = 1613) | Manual Prescription (n = 605) | |
|---|---|---|
| Age, y, mean ± SD | 62.5 ± 11.8 | 59.3 ± 13.8 |
| Women, % | 54.9 | 59.3 |
| Cholesterol, mg/dL, mean ± SD | ||
| Total | 189.9 ± 48.1 | 198.5 ± 38.98 |
| Low‐density lipoprotein | 110 ± 41.8 | 118 ± 34.7 |
| High‐density lipoprotein | 54.1 ± 15.8 | 56 ± 16.7 |
| Triglycerides | 127.9 ± 66.69 | 123.3 ± 57.61 |
| Smokers, % | 7.3 | 8.7 |
| Hypertension, % | 70.1 | 58.8 |
| Family history of premature, % | 3.5 | 3.0 |
| Peripheral arterial disease, % | 1.7 | 0.4 |
| Abdominal aortic aneurysm, % | 0.4 | 0.1 |
| Coronary heart disease, % | 11.7 | 5.1 |
| Diabetes mellitus, % | 40.2 | 24.8 |
| Acute coronary syndrome, % | 3.6 | 1.5 |
| Multiple major risk factors, % | 4.2 | 1.9 |
| Multiple risk factors of the metabolic syndrome, % | 2.8 | 3.6 |
| NCEP ATP III Goal | ||
| ≤160 mg/dL, % | 27.5 | 48.6 |
| ≤130 mg/dL, % | 23.6 | 22.9 |
| ≤100 mg/dL, % | 41.0 | 24.1 |
| ≤70 mg/dL, % | 7.8 | 4.4 |
| Health insurance, % | ||
| Private | 65.6 | 68.1 |
| Medicare | 31.4 | 26.1 |
| Medicaid | 2.9 | 5.7 |
| Self‐pay | 0.1 | 0.1 |
Abbreviations: NCEP ATP III, National Cholesterol Education Program Adult Treatment Panel III; SD, standard deviation.
Relationship Between Physician Characteristics and LDL Goal Attainment
Of the 2218 patients included in the study, 6.6% were cared for by a cardiologist and 93.4% by a physician in another department (Table 2). The average age of physicians was 51.3 ± 11.7 years. The average time since medical school graduation was 25.1 ± 12 years. The average time since last ABIM board certification was 14.0 ± 11.6 years. Physician age, specialty, the number of years since medical school graduation or last ABIM board certification were not significant predictors of whether patients were at LDL goal at follow‐up (Table 3). There were no major differences in provider characteristic by prescription status (e‐prescription vs manual).
Table 2.
Provider Characteristics for Patient Encounters Included in the Study (n = 2218)
| E‐Prescription n = 1613 | Manual Prescription n = 605 | |
|---|---|---|
| Provider specialty, % | ||
| Cardiology | 7.5 | 4.3 |
| Noncardiology | 92.5 | 95.7 |
| Age, y, mean ± SD | 51.1 ± 11.2 | 51.5 ± 12.8 |
| Years since medical school graduation, n, mean ± SD | 25.0 ± 11.6 | 25.3 ± 13 |
| Years since last board certification, n, mean ± SD | 13.3 ± 11.4 | 15.9 ± 11.7 |
Abbreviations: SD = standard deviation.
Table 3.
Effect of Variables on Low‐Density Lipoprotein Goal Attainment From Initial Presentation to Follow‐Up
| Odds Ratio | 95% CI | P Value | |
|---|---|---|---|
| Specialty | |||
| Cardiology | 1.00 | — | |
| Noncardiology | 0.53 | 0.23–1.20 | 0.13 |
| E‐prescription | |||
| No | 1.00 | — | |
| Yes | 1.59a | 1.12–2.25 | 0.009 |
| Insurance type | |||
| Private | 1.00 | — | |
| Medicaid | 0.65 | 0.30–1.42 | 0.41 |
| Medicare | 0.76 | 0.52–1.12 | 0.98 |
| Provider characteristics | |||
| Age (y) | 1.03 | 0.96–1.10 | 0.46 |
| Years since last board certification | 0.99 | 0.96–1.01 | 0.26 |
| Years since medical school graduation | 0.99 | 0.93–1.06 | 0.78 |
| Patient age | 0.99 | 0.98–1.02 | 0.72 |
| Patient sex | |||
| Female | 1.00 | — | |
| Male | 1.53a | 1.13–2.08 | 0.006 |
| Price of prescriptions ($10 increase) | 0.95a | 0.93–0.98 | 0.0003 |
| Atorvastatin prescription | 2.87a | 2.03–4.05 | <0.0001 |
| Low‐density lipoprotein goal | |||
| <70 mg/dL | 1.00 | — | |
| <100 mg/dL | 3.45a | 1.92–6.21 | <0.0001 |
| <130 mg/dL | 5.16a | 2.76–9.77 | <0.0001 |
| <160 mg/dL | 10.93a | 5.50–21.73 | <0.0001 |
Abbreviations: CI, confidence interval.
Indicates statistical significance (P < 0.05).
Relationship Between E‐Prescription and LDL Goal Attainment
Of the 796 patients not initially at LDL goal, 393 (49%) were at goal at follow‐up, 51% of patients in the e‐prescription group vs 44% in the manual prescription group. Patients with an e‐prescription were 59% more likely to attain their guideline‐based LDL goal (odds ratio [OR] = 1.59; 95% confidence interval [CI]: 1.12–2.25) (Table 3). No significant interaction was found between the e‐prescription and both targeted LDL goal and prescribed medication.
Relationship Between Prescription Price and LDL Goal Attainment
For each $10 increase in prescription price at the initial visit, the likelihood of being at goal decreased by 5% (OR = 0.95; 95% CI: 0.93–0.98). Patients with an e‐prescription were 70% (P = 0.0004) more likely to receive a generic statin (Table 4, Table 5).
Table 4.
Generic vs Branded Statin Prescription Patterns by Method of Prescription
P<0.001.
Table 5.
Use of Each Statin as a Percentage in the E‐Prescription and Manual Prescription Groups
| Statin | E‐Prescription (%) | Manual Prescription (%) |
|---|---|---|
| Atorvastatin | 54.2 | 67.7 |
| Fluvastatin | 0.5 | 0.5 |
| Lovastatin | 7.0 | 2.6 |
| Pravastatin | 6.6 | 2.1 |
| Rosuvastatin | 7.4 | 8.9 |
| Simvastatin | 24.4 | 18.2 |
Other Significant Predictors of LDL Goal Attainment
Male gender was a significant predictor of LDL goal attainment with OR 1.53 (CI: 1.13–2.08, P = 0.006). This gender difference persisted across all levels of risk. Attaining goal was easier with higher target goal, as LDL goal incrementally increased from <70 mg/dL to <160 mg/dL, and the likelihood of goal attainment also demonstrated incremental improvement (Table 3). Of the prescription drugs taken by more than 5% of the study cohort, only atorvastatin was a meaningful covariate, and an atorvastatin prescription demonstrated an OR of 2.87 for goal attainment (CI: 2.03–4.05, P<0.0001).
Discussion
Our study demonstrated that the use of an e‐prescription with FDS has a positive effect on LDL goal attainment. Patients with FDS‐associated e‐prescriptions were more likely to show improvement and be at their NCEP ATP III goal at follow‐up. Although other studies have shown that e‐prescriptions can lead to better patient compliance and fewer medical errors,10, 11, 17 ours is the first to demonstrate that an e‐prescription is associated with more favorable clinical outcomes.
Explanations for the Superiority of an E‐prescription
There are a few possible explanations for this relationship. Physicians who use e‐prescriptions have built‐in access to patient‐specific information about the tier status of prescribed drugs via FDS, and as a result, may be more likely to prescribe affordable medications. Patient adherence as a result is increased,11, 12 and consequently, LDL levels are better managed. Generic statins were more likely to be prescribed with e‐prescribing, and the patient's likelihood of being at goal decreases by 5% with each $10 increase in prescription price in our model. However, it should be noted that patients with more severe hyperlipidemia may require more potent, and consequently, more expensive brand name statins for tighter LDL control. Also, there are more patients with multiple comorbidities in the e‐prescription group, suggesting that patients who require multiple medications and more aggressive lipid‐lowering intervention are more easily managed by e‐prescription.
Other Covariates
Not surprisingly, as the LDL goal increased, patients were more likely to achieve their goal. Patients requiring more aggressive LDL lowering were the least likely to attain their goal, underscoring the importance of finding interventions that best reach this high‐risk population. Confirming the findings of the existence of gender disparity in lipid management, males in our cohort were 53% more likely to attain their LDL goal than women across all levels of CHD risk.18, 19, 20, 21 In contrast to what has been suggested by other studies,16 we did not find that the years since a physician's last board certification had an effect on goal attainment. Additionally, neither physician age nor years since medical school graduation date had any predictive value for changing LDL levels.
Implications of Our Findings
The federal government has identified e‐prescribing as an important tool in the effective delivery of healthcare and has allocated funding to encourage its use among providers, but there have not been any studies that show that it actually leads to better clinical outcomes. Our study provides evidence to support this initiative, provided that e‐prescribing is used with FDS. Moreover, it can be implemented within the broader context of the chronic care model, a guide for effective management of chronic illness that is comprised of 6 components: self‐management support, clinical information systems, delivery system redesign, decision support, health care organization, and community resources.22 Using an e‐prescription with FDS in combination with other components of the chronic care model would likely strengthen its impact on lipid control, because an integrated approach to treating chronically ill patients has already been shown to improve outcome measures and reduce costs.23 An e‐prescription with FDS promotes lipid control through improved patient adherence to lipid‐lowering medications, but other tools such as clinical decision support can improve management of hyperlipidemia through enhanced screening and treatment as well as increased physician adherence to national guidelines.24, 25 Therefore, an e‐prescription with FDS can further benefit a patient whose physician is already employing other interventions for lipid control.
Limitations
This study is restricted to the patients of a single outpatient academic medical center. However, the population that we selected is very comparable to the national norm, with 75% of our population at goal.4 Additionally, we looked only at lipid panels that were performed throughout the course of one year, 2007. However, 2007 was selected because there were no major shifts in prescribing patterns as in neighboring years. The recent worldwide recession that has occurred since the study period may amplify patients' price sensitivity, in which case our results may underestimate e‐prescriptions' effects. Also, because this is a retrospective study, it relied on information documented by providers in the electronic medical record. Finally, our result must be interpreted in association with the FDS built into the EHR. An e‐prescription in the absence of FDS may not have the same results, and this limitation should be considered when e‐prescribing initiatives are promoted.
Conclusion
In conclusion, this retrospective study is the first to show that e‐prescribing with FDS results in improved LDL goal attainment. Therefore, it is an attractive tool for providers not just because of the financial incentives that encourage its use, but more importantly, because it can lead to better patient outcomes.
Acknowledgements
We would like to thank Yousef Bader, MD; Douglas V. Clarke, MD; Lena Furmark, MD; Shireen Khoury, BS; Nina Kukar, MD; Rayan Alhazmi, MD; and Raman Dusaj, MD for their invaluable assistance in chart abstraction. We are very grateful to Vandana Toteja, Tara Aziz, and Marcela Maamari for their generous help and technical expertise in EHR management.
References
- 1. Cannon CP, Steinberg BA, Murphy SA, et al. Meta‐analysis of cardiovascular outcomes trials comparing intensive versus moderate statin therapy. J Am Coll Cardiol. 2006;48:438–445. [DOI] [PubMed] [Google Scholar]
- 2. Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol‐lowering treatment: prospective meta‐analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. [DOI] [PubMed] [Google Scholar]
- 3. Expert Panel on Detection Evaluation and Treatment of High Blood Cholesterol in Adults . Third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106:3143–3421. [PubMed] [Google Scholar]
- 4. Grundy SM, Cleeman JI, Merz CN, et al. Implications of recent clinical trials for the national cholesterol education program adult treatment panel III guidelines. J Am Coll Cardiol. 2004;44:720–732. [DOI] [PubMed] [Google Scholar]
- 5. Waters DD, Brotons C, Chiang C, et al. Lipid treatment assessment project 2: a multinational survey to evaluate the proportion of patients achieving low‐density lipoprotein cholesterol goals. Circulation. 2009;120:28–34. [DOI] [PubMed] [Google Scholar]
- 6. Benner JS, Glynn RJ, Mogun H, et al. Long‐term persistence in use of statin therapy in elderly patients. JAMA. 2002;288:455–461. [DOI] [PubMed] [Google Scholar]
- 7. Medicare Improvements for Patients and Providers Act of 2008, Public Law 110‐275 . HR 6331, 132 (July 15, 2008).
- 8.Health Information Technology Act of 2009. S. 179 (January 8, 2009).
- 9. Teich JM, Merchia PR, Schmiz JL, et al. Effects of computerized physician order entry on prescribing practices. Arch Intern Med. 2000;160:2741–2747. [DOI] [PubMed] [Google Scholar]
- 10. Fischer MA, Vogeli C, Stedman M, et al. Effect of electronic prescribing with formulary decision support on medication use and cost. Arch Intern Med. 2008;168:2433–2439. [DOI] [PubMed] [Google Scholar]
- 11. Doshi JA, Zhu J, Lee BY, Kimmel SE, et al. Impact of a prescription copayment increase on lipid‐lowering medication adherence in veterans. Circulation. 2009;119:390–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Choudhry NK. Copayment levels and medication adherence: less is more. Circulation. 2009;119:365–367. [DOI] [PubMed] [Google Scholar]
- 13. U.S. Food and Drug Administration . FDA approves first generic simvastatin: third new generic approved this week. FDA news release. July 2006. . http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucm108675.htm. Accessed January 4, 2010.
- 14. Kastelein JJP, Akdim F, Stroes ESG, et al. Simvastatin with or without ezetimibe in familial hypercholesterolemia. N Engl J Med. 2008;358:1431–1443. [DOI] [PubMed] [Google Scholar]
- 15. Drugstore.com Web site. Prescription price checker. http://www.drugstore.com/prescriptions/qxc10663. Accessed October 7, 2009.
- 16. Turchin A, Shubina M, Chodos AH, et al. Effect of board certification on antihypertensive treatment intensification in patients with diabetes mellitus. Circulation. 2008;117:623–628. [DOI] [PubMed] [Google Scholar]
- 17. Van Doormaal JE, van den Bemt PM, Zaal RJ, Egberts ACG, Lenderink BW, Kosterink JGW, Haaijer‐Ruskamp FM, Mol PGM. The influence that electronic prescribing has on medication errors and preventable adverse drug events: an interrupted time‐series study. J Am Med Inform Assoc. 2009;16:816–825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Miller M, Byington R, Hunninghake D, et al. Sex bias and underutilization of lipid‐lowering therapy in patients with coronary artery disease at academic medical centers in the United States and Canada. Arch Intern Med. 2000;160:343–347. [DOI] [PubMed] [Google Scholar]
- 19. Ford ES, Mokdad AH, Giles WH, et al. Serum total cholesterol concentrations and awareness, treatment, and control of hypercholesterolemia among US adults: findings from the National Health and Nutrition Examination Survey, 1999 to 2000. Circulation. 2003;107:2185–2189. [DOI] [PubMed] [Google Scholar]
- 20. Arnett DK, Jacobs DR Jr, Luepker RV, et al. Twenty‐year trends in serum cholesterol, hypercholesterolemia, and cholesterol medication use: the Minnesota Heart Survey, 1980–1982 to 2000–2002. Circulation. 2005;112:3884–3891. [DOI] [PubMed] [Google Scholar]
- 21. Mosca L, Merz NB, Blumenthal RS, et al. Opportunity for intervention to achieve American Heart Association guidelines for optimal lipid levels in high‐risk women in a managed care setting. Circulation. 2005;111:488–493. [DOI] [PubMed] [Google Scholar]
- 22. Bodenheimer T, Wagner EH, Grumbach K. Improving Primary Care for Patients with Chronic Illness. JAMA. 2002;288:1775–1779. [DOI] [PubMed] [Google Scholar]
- 23. Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. JAMA. 2002;288:1909–1914. [DOI] [PubMed] [Google Scholar]
- 24. van Wyk JT, van Wijk MAM, Sturkenboom MCJM, et al. Electronic alerts versus on‐demand decision support to improve dyslipidemia treatment: A cluster randomized controlled trial. Circulation. 2008;117:371–378. [DOI] [PubMed] [Google Scholar]
- 25. Bertoni AG, Bonds DE, Chen H, et al. Impact of a multifaceted intervention on cholesterol management in primary care practices. Arch Intern Med. 2009;169:678–686. [DOI] [PMC free article] [PubMed] [Google Scholar]