

Abstract
Coronary artery disease and myocardial infarctions are believed to be rare in patients with Down's syndrome. Congenital heart malformations are frequently seen in children born with the syndrome and may represent a substrate for coronary artery embolism in later life. We report a case of myocardial infarction in a patient with Down's syndrome and present a review of the literature. Copyright © 2011 Wiley Periodicals, Inc.
The authors have no conflicts of interest to disclose.
Introduction
Down syndrome is the most common inherited form of intellectual disability, with an incidence of 1 in every 600 to 1000 live births. Trisomy of the 21st chromosome is present in the vast majority of cases, although translocation abnormalities and mosaic karyotypes have also been reported.1 Advancing maternal and possibly paternal age is believed to increase the incidence of the disorder.
Coronary artery disease and myocardial infarction (MI) are believed to be rare in patients with Down syndrome. Congenital heart malformations are frequently seen in children born with the syndrome and may represent a substrate for coronary artery embolism in later life.
Improvements in the care of individuals with learning disabilities have resulted in a significant increase in survival of patients with Down syndrome, with a recent Australian study reporting a median life expectancy of 60 years.2 As this group of patients increasingly survives into late adulthood, aging‐related diseases including coronary atherosclerosis may emerge as an important cause for mortality.
We report a case of MI in a patient with Down syndrome and present a review of the literature.
Case Report
A 44‐year‐old male with Down syndrome presented to our center following an out‐of‐hospital cardiac arrest. His past medical history included a ventricular septal defect (VSD) with Eisenmenger syndrome, secondary polycythemia, mild renal insufficiency, and gout.
Physical examination revealed the facies of Down syndrome. He was cyanosed, with cold peripheries. The pulse was 40 beats/minute and the blood pressure was 80/40 mm Hg. The heart sounds were normal with a pansystolic murmur at the left sternal edge. Examination of the chest was unremarkable. A 12‐lead electrocardiogram showed an inferior ST‐segment elevation MI complicated by complete heart block (Figure 1).
Figure 1.
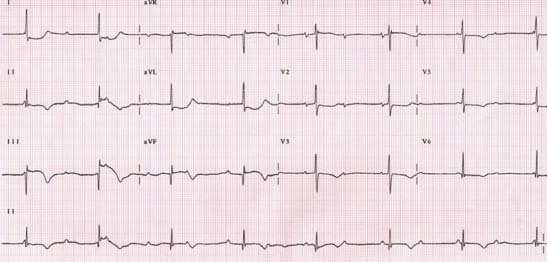
The 12‐lead electrocardiogram.
A transthoracic echocardiogram performed previously had revealed marked dilation of the right ventricle with good biventricular function and a perimembranous VSD with right‐to‐left shunting.
Cardiac catheterization was performed via the radial route, under conscious sedation using intravenous midazolam. Selective coronary angiography demonstrated an atheroma‐free left coronary artery, but a thrombotic occlusion of a proximal dominant right coronary artery (Figure 2A).
Figure 2.
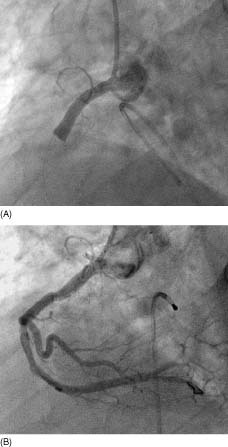
(A) Thrombotic occlusion of right coronary artery. (B) Angiographic result following percutaneous coronary intervention.
A temporary transvenous pacemaker was placed in the right ventricular apex. This was followed by percutaneous intervention of the right coronary artery using a 6‐Fr JR4 guide catheter. The procedure was performed with adjunctive abciximab and a distal protection device (FilterWire EZ; Boston Scientific Corporation, Natick, MA). The lesion was predilated with a 3.0 × 12 Quantum Maverick Monorail balloon (Boston Scientific) followed by the deployment of a 4.0 × 16 Coroflex Blue stent (B. Braun Melsungen, Germany). There was poor downstream distal flow, but the artery appeared free of atheroma (Figure 2B). Examination of the distal protection device after removal failed to reveal any thrombotic debris. Despite the successful coronary intervention, the patient developed progressive multiple organ failure and died 48 hours later.
Discussion
This case represents an unusual presentation of a MI complicated by cardiogenic shock and atrioventricular block in a patient with Down syndrome. A review of the literature revealed 2 previously reported cases of MI in patients with Down syndrome.3., 4.
In the absence of predisposing atherosclerosis, paradoxical embolism to the right coronary artery through the VSD may have been responsible for the MI in our patient.
Congenital anomalies of the heart are common in Down syndrome, with atrial and ventricular septal defects accounting for the majority of malformations. These intracardiac defects may be responsible for embolism of venous thromboses into the systemic circulation through a right‐to‐left shunt.
The prevalence of coronary artery disease is known to be low in this group of individuals, with previous postmortem studies reporting remarkable freedom from atherosclerosis. Murdoch et al in 1977 suggested that Down syndrome may even represent an “atheroma free model.”5 The reasons for the lack of atherosclerosis and low incidence of its sequelae remain unclear, although previous studies have implicated low levels of plasminogen activator inhibitor type 1 as a cause for this vasculoprotective effect.6
References
- 1. Frid C, Drott P, Lundell B, et al. Mortality in Down's syndrome in relation to congenital malformations. J Intellect Disabil Res. 1999;43(part 3):234–241. [DOI] [PubMed] [Google Scholar]
- 2. Glasson EJ, Sullivan SG, Hussain R, et al. The changing survival profile of people with Down syndrome: implications for genetic counselling. Clin Genet. 2002;62:390–393. [DOI] [PubMed] [Google Scholar]
- 3. Ho PC, Nguyen M. Acute two‐vessel coronary closure in a patient with Down syndrome. Int J Cardiovasc Intervent. 2003;5:95–97. [DOI] [PubMed] [Google Scholar]
- 4. Stahl J, Santos LD, Byard RW. Coronary artery thromboembolism and unexpected death in childhood and adolescence. J Forensic Sci. 1995;40:599–601. [PubMed] [Google Scholar]
- 5. Murdoch JC, Rodger JC, Rao SS, et al. Down syndrome: an atheroma‐free model? Br Med J. 1977;2:226–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hopkins WE, Fukagawa NK, Sobel BE, et al. Plasminogen activator inhibitor type 1 in adults with Down syndrome and protection against macrovascular disease. Am J Cardiol. 2000;85: 784–786. [DOI] [PubMed] [Google Scholar]