

Abstract
Background
There is a growing body of evidence that blood pressure (BP) level is one of the major determinants of cardiovascular morbidity and mortality in individuals, including elderly people. However, to achieve a target BP level in the elderly is more difficult compared with patients aged <65 years. Current guidelines recommend combination drug therapy with different modes of action for the treatment of elderly patients with moderate hypertension (HT). However, the optimal combination regimen is not well established in elderly HT.
Hypothesis
We hypothesized that combination therapy of telmisartan plus amlodipine would exert favorable cardiometabolic actions in elderly HT.
Methods
Seventeen elderly patients with essential HT who failed to achieve a target home BP level with treatment of 5 mg amlodipine plus 80 mg valsartan or 8 mg candesartan for at least 2 months were enrolled. Then the patients were assigned to replace their valsartan or candesartan with 40 mg telmisartan. The subjects were instructed to measure their own BP at home every day during the study periods.
Results
Replacement of valsartan or candesartan by telmisartan in amlodipine‐treated elderly hypertensive patients showed a significant reduction in morning home systolic BP and evening home systolic and diastolic BP at 12 weeks. Switching to telmisartan significantly increased serum adiponectin level.
Conclusions
Our present study suggests that combination therapy with telmisartan plus amlodipine may exert more beneficial cardiometabolic effects in elderly patients with HT compared with valsartan or candesartan plus amlodipine treatment. © 2011 Wiley Periodicals, Inc.
This work was supported in part by Grants of Collaboration with Venture Companies Project from the Ministry of Education, Culture, Sports, Science and Technology, Japan (to S.Y.). The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Introduction
The number of elderly individuals, defined as persons aged ≥65 years, keeps increasing in developed continues.1, 2 Hypertension (HT) is highly prevalent in the elderly population. More than 60% of people aged ≥65 years in the United States and Japan have HT.1, 2 There is a growing body of evidence that blood pressure (BP) level is one of the major determinants of cardiovascular morbidity and mortality in individuals, including elderly people.2, 3, 4, 5, 6 Indeed, a positive association between elevation of BP level and increased risk of future cardiovascular events is observed in elderly individuals, and the absolute risk of cardiovascular disease is higher in the aged population.2, 3, 4, 5, 6 Therefore, aggressive control of BP is also desirable in the elderly with HT.
Elderly HT is characterized by impairment of fluid volume and electrolyte regulation, decrease in the baroreceptor reflex, and coexistence of atherosclerosis, insulin resistance, and glucose intolerance.2, 3 Therefore, to achieve a target BP level in the elderly is more difficult compared with patients aged <65 years. The Japanese Society of Hypertension recommends calcium channel blockers (CCBs), angiotensin‐converting enzyme (ACE) inhibitors, angiotensin II type 1 receptor blockers (ARBs), or low‐dose thiazide diuretics as the first‐line drugs for the management of elderly HT, and if BP control is insufficient with monotherapy, combination therapy with these agents should be conducted.2 Combination therapy with ACE inhibitors/ARBs plus CCBs has an advantage in the lack of metabolic adverse effects, whereas diuretics are associated with hyperglycemia, hyperuricemia, dyslipidemia, and hypokalemia.2, 3 Furthermore, recently, 2 landmark trials, Avoiding Cardiovascular Events in Combination Therapy in Patients Living With Systolic Hypertension (ACCOMPLISH) and Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint (ONTARGET), have revealed that combination therapy with ACE inhibitors/ARBs plus CCBs is also effective and well‐tolerated in elderly HT.7, 8 However, an optimal combination regimen is not well established in elderly HT. Because risk of cough from ACE inhibitors is relatively high in East Asian patients compared with white patients,9 ARBs are more popular than ACE inhibitors in Japan. Therefore, we examined here in elderly patients whose BP level at home was uncontrolled by combination treatment with 5 mg amlodipine plus 80 mg valsartan or 8 mg candesartan for at least 2 months whether additional BP lowering could be achieved by switching to 5 mg amlodipine plus 40 mg telmisartan. We also investigated whether switching from valsartan or candesartan to telmisartan could have favorable metabolic effects in elderly hypertensive patients.
Methods
Subjects
This was a prospective, open‐label, 12‐week study. Patients aged ≥65 years with essential HT not achieving a target home BP level were recruited from multiple centers in Japan.10, 11 All patients were taking 5 mg amlodipine plus 80 mg valsartan (n = 5) or 8 mg candesartan (n = 12) for at least 2 months. A screening period of up to 2 to 4 weeks was used to assess eligibility and to eliminate prior medications. Finally, 17 eligible patients (14 males and 3 females; mean age, 74.5 ± 7.3 y) were assigned to replace their valsartan or candesartan with 40 mg telmisartan. During the study period, subjects were instructed not to change their lifestyles and to continue taking the same dose of any concomitant drugs. We excluded any patients with secondary HT, chronic liver disease, severe chronic heart failure, and those who had recent (<6 mo) acute coronary syndromes, stroke, and any acute infections. Patients who were aged <20 years, whose BP level was ≥180/110 mm Hg, or whose serum creatinine (Cr) level was ≥1.5 mg/dL were also excluded. Anthropometric and metabolic variables and serum chemistries were measured at baseline and at 12 weeks after telmisartan treatment as described previously.12 Informed consent was obtained from all the subjects, and the study protocol was approved by the Institutional Ethics Committee of Kurume University School of Medicine.
Study Design
The medical history was ascertained by a questionnaire. Height and weight were measured, and body mass index (kg/m2) was calculated as an index of the presence or absence of obesity. The subjects were instructed to measure their own BP at home every day by using an automatic device based on the cuff‐oscillometric method (HEM‐7501‐HP; Omron Healthcare, Kyoto, Japan). Blood pressure was measured in a sitting position after at least 5 minutes of rest twice a day: once in the morning within 1 hour of awakening, after micturition, but before taking antihypertensive agents (morning home BP); and once in the evening, just before going to bed (evening home BP). Morning and evening systolic BP (SBP) and diastolic BP (DBP) were averaged in each subject for the final 5 days of the screening period (days −4–0) and for the final 5 days of twelfth week of the treatment period (days 80–84). The mean of these values was used as the BP level at baseline and at 12 weeks after telmisartan treatment, respectively.
Blood was drawn from the antecubital vein in the morning after 12‐hour fasting for determination of lipids (high‐density lipoprotein cholesterol, low‐density lipoprotein cholesterol, and triglycerides), fasting plasma glucose (FPG), insulin, glycated hemoglobin, serum Cr, and adiponectin. Blood chemistries were measured at a commercially available laboratory (SRL Inc., Hachioji, Japan). The homeostasis model assessment of insulin resistance index was calculated from the values of FPG (mg/dL) and insulin (μU/mL) using the following formula: (glucose × insulin) / 405. Estimated glomerular filtration rate was calculated with the modified isotope dilution mass spectrometry‐traceable, 4‐variable Modification of Diet in Renal Disease Study equation for Japanese.13
Statistical Methods
Data were expressed as mean ± SD. To compare the parameter changes between baseline and after the telmisartan treatment, we used the paired t test. Statistical significance was defined as P < 0.05. All statistical analyses were performed with SAS software, version 9.2 (SAS Institute Inc., Cary, NC).
Results
Demographic data of the subjects are presented in the Table 1. As shown in Figure 1, replacement of valsartan or candesartan with telmisartan in amlodipine‐treated elderly hypertensive patients showed a significant reduction in morning home SBP and evening home SBP and DBP at 12 weeks; morning and evening BP level decreased from 153.3/75.1 mm Hg and 141.7/67.8 mm Hg at baseline to 145.9/74.5 mm Hg and 132.6/65.1 mm Hg at 12 weeks after the telmisartan treatment, respectively. As shown in Figure 2, serum adiponectin level was significantly increased after switching to telmisartan therapy. However, the changes in serum adiponectin level were not correlated with those in mean BP levels (MBP; Figure 3). There were no significant differences in values of body mass index, low‐density lipoprotein cholesterol, triglycerides, high‐density lipoprotein cholesterol, FPG, glycated hemoglobin, homeostasis model assessment of insulin resistance index, Cr, and estimated glomerular filtration rate before and after the treatment of telmisartan (Table).
Table 1.
Clinical Variables at Baseline and at 12 Weeks After Telmisartan Treatment
| Clinical Variable | Baseline | At 12 Weeks | P Value |
|---|---|---|---|
| BMI (kg/m2) | 24.8 ± 1.8 | 24.9 ± 1.8 | 0.83 |
| Heart rate (beats/min) | 66.4 ± 16.5 | 61.8 ± 9.1 | 0.22 |
| Morning SBP (mm Hg) | 153.3 ± 14.2 | 145.9 ± 14.0 | <0.05 |
| Morning DBP (mm Hg) | 75.1 ± 8.3 | 74.5 ± 9.3 | 0.55 |
| Evening SBP (mm Hg) | 141.7 ± 14.6 | 132.6 ± 16.4 | <0.01 |
| Evening DBP (mm Hg) | 67.8 ± 7.8 | 65.1 ± 8.7 | <0.05 |
| LDL‐C (mg/dL) | 113.1 ± 28.8 | 113.1 ± 26.6 | 0.99 |
| TG (mg/dL) | 101.2 ± 33.4 | 113.4 ± 53.6 | 0.27 |
| HDL‐C (mg/dL) | 55.5 ± 8.9 | 54.8 ± 9.8 | 0.64 |
| FPG (mg/dL) | 100.1 ± 8.5 | 100.9 ± 10.4 | 0.80 |
| HbA1c (%) | 4.9 ± 0.4 | 4.9 ± 0.4 | 0.09 |
| Fasting insulin (μU/mL) | 5.1 ± 3.2 | 5.3 ± 3.7 | 0.82 |
| HOMA‐IR | 1.3 ± 0.8 | 1.3 ± 0.9 | 0.87 |
| Adiponectin (μg/mL) | 13.2 ± 10.0 | 14.3 ± 11.0 | <0.01 |
| Cr (mg/dL) | 0.7 ± 0.2 | 0.8 ± 0.2 | 0.54 |
| eGFR (mL/min/1.73m2) | 78.7 ± 19.0 | 77.8 ± 19.7 | 0.62 |
| DM, n | 3 | 3 | NA |
| Dyslipidemia, n | 9 | 9 | NA |
Abbreviations: BMI, body mass index; Cr, creatinine; DBP, diastolic blood pressure; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL‐C, high‐density lipoprotein cholesterol; HOMA‐IR, homeostasis model assessment of insulin resistance; LDL‐C, low‐density lipoprotein cholesterol; NA, not applicable; SBP, systolic blood pressure; TG, triglycerides.
Figure 1.

Morning (A) and evening (B) home BP levels at baseline and after telmisartan treatment. Replacement of valsartan or candesartan with telmisartan showed a significant reduction in morning SBP and evening SBP and DBP at 12 weeks. Abbreviations: BP, blood pressure; DBP, diastolic blood pressure; SBP, systolic blood pressure.
a The * indicates P < 0.05 compared with baseline values.
b The ** indicates P < 0.001 compared with baseline values.
Figure 2.
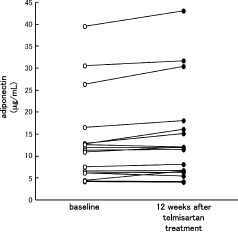
Serum adiponectin levels of each subject at baseline and after telmisartan treatment. Replacement of valsartan or candesartan with telmisartan showed a significant increase in serum adiponectin levels at 12 weeks.
Figure 3.

Correlation of the changes in serum adiponectin (Δadiponectin) obtained by switching from valsartan or candesartan to telmisartan therapy with those in morning (A) and evening (B) MBP (ΔMBP). Δadiponectin was not correlated with morning (A) or evening (B) ΔMBP. Abbreviations: MBP, mean blood pressure; R2, coefficient of determination.
Discussion
Recent analysis by the Blood Pressure Lowering Treatment Trialists' Collaboration (BPLTTC) revealed that any commonly used BP‐lowering regimen reduced the risk of total major cardiovascular events, and larger lowering in BP level produced larger reductions in the risk.4 These observations suggest that most of the differences among treatment regimens in their effects on cardiovascular outcomes could be explained by the differences in achieved BP level. However, it may also be true that a particular treatment regimen may be superior or inferior to others with regard to reduction of risk of cardiovascular events.7, 8, 14, 15, 16 Further, to achieve a target BP level is often difficult in the elderly on single‐drug therapy.2, 3 Therefore, current Japanese guidelines recommend combination drug therapy with different modes of action for the treatment of elderly patients with moderate HT.2
In this study, we demonstrated for the first time that in elderly hypertensive patients uncontrolled by the combination treatment of 5 mg amlodipine plus 80 mg valsartan or 8 mg candesartan, additional morning and evening home BP lowering was achieved by switching to 5 mg amlodipine plus 40 mg telmisartan. Morning home SBP and evening home SBP and DBP levels were significantly decreased at 12 weeks after the telmisartan treatment. Several clinical studies have shown that home BP is superior to office BP in predicting the risk of cardiovascular mortality in hypertensive patients.17, 18, 19 Furthermore, cardiovascular events often occur in the early morning,20, 21 and there is a strong correlation between early‐morning HT and the risk of future cardiovascular events.22, 23 Therefore, our present findings suggest that combination therapy with telmisartan plus amlodipine may exert more cardioprotective effects in elderly patients with HT by reducing home BP, especially morning BP, compared with valsartan or candesartan plus amlodipine treatment. Nishimura et al reported that the antihypertensive effects of telmisartan on morning and evening home BP level were greater than those of candesartan or valsartan in patients with essential HT,24 thus supporting our observations. Telmisartan has the strongest binding affinity to angiotensin II type 1 receptor and the longest elimination half‐life among various ARBs.25, 26 These characteristics of telmisartan may explain the long‐lasting home BP‐lowering effects in our uncontrolled elderly hypertensive patients.
In this study, switching to telmisartan significantly increased serum adiponectin levels (Figure 2). Furthermore, the changes in serum adiponectin (Δadiponectin) obtained by switching from valsartan or candesartan to telmisartan therapy were not correlated with those in morning MBP or evening MBP (ΔMBP) (Figure 3). These findings suggest that telmisartan may increase serum adiponectin level in a BP‐lowering–independent manner. Recently, telmisartan was reported to act as a partial agonist of peroxisome proliferator‐activated receptor‐γ (PPAR‐γ),15, 27 which promotes differentiation of preadipocytes by activating adipose‐specific gene expression.15, 28 Telmisartan treatment was shown to decrease weight of visceral adipose tissue and increase serum adiponectin level in diet‐induced obese mice.29 In addition, Miura et al reported that replacement of valsartan or candesartan with telmisartan in hypertensive patients with type 2 diabetes resulted in a significant increase in serum adiponectin level.30 These findings suggest that telmisartan could increase serum adiponectin level via PPAR‐γ –modulating activity.
Conclusion
Although switching to telmisartan did not affect other anthropometric and metabolic variables in our subjects, given the insulin‐sensitizing and anti‐inflammatory properties of adiponectin,28, 31 telmisartan plus amlodipine therapy may exert favorable cardiometabolic actions in elderly HT. Further longitudinal study is needed to clarify the issue.
References
- 1. US Census Bureau . Estimated world population figures 2020. Available at: http://www.census.gov/ipc/www/idb/tables.html. Accessed April 13, 2009.
- 2. Ogihara T, Kikuchi K, Matsuoka H, et al; Japanese Society of Hypertension Committee. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Chapter 8. Hypertension in the elderly. Hypertension Res. 2009;32:57–62. [Google Scholar]
- 3. Kostis JB. Antihypertensive therapy with CCB/ARB combination in older individuals: focus on amlodipine/valsartan combination. Am J Ther. 2010;17:188–196. [DOI] [PubMed] [Google Scholar]
- 4. Turnbull F. Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood‐pressure‐lowering regimens on major cardiovascular events: results of prospectively‐designed overviews of randomised trials. Lancet. 2003;362: 1527–1535. [DOI] [PubMed] [Google Scholar]
- 5. Arima H, Tanizaki Y, Kiyohara Y, et al. Validity of the JNC VI recommendations for the management of hypertension in a general population of Japanese elderly: the Hisayama study. Arch Intern Med. 2003;163:361–366. [DOI] [PubMed] [Google Scholar]
- 6. Murakami Y, Hozawa A, Okamura T, et al; Evidence for Cardiovascular Prevention From Observational Cohorts in Japan Research Group (EPOCH‐JAPAN). Relation of blood pressure and all‐cause mortality in 180,000 Japanese participants: pooled analysis of 13 cohort studies. Hypertension. 2008;51:1483–1491. [DOI] [PubMed] [Google Scholar]
- 7. Jamerson K, Weber MA, Bakris GL, et al. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high‐risk patients. N Engl J Med. 2008;359:2417–2428. [DOI] [PubMed] [Google Scholar]
- 8. ONTARGET Investigators , Yusuf S, Teo KK, Pogue J, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547–1559. [DOI] [PubMed] [Google Scholar]
- 9. McDowell SE, Coleman JJ, Ferner RE. Systematic review and meta‐analysis of ethnic differences in risks of adverse reactions to drugs used in cardiovascular medicine. BMJ. 2006;332:1177–1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ogihara T, Kikuchi K, Matsuoka H, et al; Japanese Society of Hypertension Committee. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Chapter 2. Measurement and clinical evaluation of blood pressure. Hypertens Res. 2009;32:11–23. [Google Scholar]
- 11. Bekki H, Yamamoto K, Sone M, et al. Efficacy of combination therapy with telmisartan plus amlodipine in patients with poorly controlled hypertension. Oxid Med Cell Longev. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tahara N, Imaizumi T, Takeuchi M, et al. Insulin resistance is an independent correlate of high serum levels of advanced glycation end products (AGEs) and low testosterone in non‐diabetic men. Oxid Med Cell Longev. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Matsuo S, Imai E, Horio M, et al; Collaborators developing the Japanese equation for estimated GFR. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–992. [DOI] [PubMed] [Google Scholar]
- 14. Higaki J, Baba S, Katsuya T, et al. Deletion allele of angiotensin‐converting enzyme gene increases risk of essential hypertension in Japanese men: the Suita Study. Circulation. 2000;101: 2060–2065. [DOI] [PubMed] [Google Scholar]
- 15. Yamagishi S, Nakamura K, Matsui T. Potential utility of telmisartan, an angiotensin II type 1 receptor blocker with peroxisome proliferator‐activated receptor‐γ (PPAR‐γ)‐modulating activity for the treatment of cardiometabolic disorders. Curr Mol Med. 2007;7:463–469. [DOI] [PubMed] [Google Scholar]
- 16. Lewis EJ, Hunsicker LG, Clarke WR, et al; Collaborative Study Group. Renoprotective effect of the angiotensin‐receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345:851–860. [DOI] [PubMed] [Google Scholar]
- 17. Kamoi K, Miyakoshi M, Soda S, et al. Usefulness of home blood pressure measurement in the morning in type 2 diabetic patients. Diabetes Care. 2002;25:2218–2223. [DOI] [PubMed] [Google Scholar]
- 18. Ohkubo T, Imai Y, Tsuji I, et al. Home blood pressure measurement has a stronger predictive power for mortality than does screening blood pressure measurement: a population‐based observation in Ohasama, Japan. J Hypertens. 1998;16:971–975. [DOI] [PubMed] [Google Scholar]
- 19. Tsunoda S, Kawano Y, Horio T, et al. Relationship between home blood pressure and longitudinal changes in target organ damage in treated hypertensive patients. Hypertens Res. 2002;25: 167–173. [DOI] [PubMed] [Google Scholar]
- 20. Kelly‐Hayes M, Wolf PA, Kase CS, et al. Temporal patterns of stroke onset: the Framingham Study. Stroke. 1995;26: 1343–1347. [DOI] [PubMed] [Google Scholar]
- 21. Goldberg RJ, Brady P, Muller JE, et al. Time of onset of symptoms of acute myocardial infarction. Am J Cardiol. 1990;66: 140–144. [DOI] [PubMed] [Google Scholar]
- 22. Weber MA. The 24‐hour blood pressure pattern: does it have implications for morbidity and mortality? Am J Cardiol. 2002;89:27A–33A. [DOI] [PubMed] [Google Scholar]
- 23. Kario K, Pickering TG, Umeda Y, et al. Morning surge in blood pressure as a predictor of silent and clinical cerebrovascular disease in elderly hypertensives: a prospective study. Circulation. 2003;107:1401–1406. [DOI] [PubMed] [Google Scholar]
- 24. Nishimura T, Hashimoto J, Ohkubo T, et al. Efficacy and duration of action of the four selective angiotensin II subtype 1 receptor blockers, losartan, candesartan, valsartan and telmisartan, in patients with essential hypertension determined by home blood pressure measurements. Clin Exp Hypertens. 2005;27: 477–489. [DOI] [PubMed] [Google Scholar]
- 25. Kakuta H, Sudoh K, Sasamata M, et al. Telmisartan has the strongest binding affinity to angiotensin II type 1 receptor: comparison with other angiotensin II type 1 receptor blockers. Int J Clin Pharmacol Res. 2005;25:414–416. [PubMed] [Google Scholar]
- 26. Burnier M, Brunner HR. Angiotensin II receptor antagonists. Lancet. 2000;355:637–645. [DOI] [PubMed] [Google Scholar]
- 27. Benson SC, Pershadsingh HA, Ho CI, et al. Identification of telmisartan as a unique angiotensin II receptor antagonist with selective PPARγ‐modulating activity. Hypertension. 2004;43:993–1002. [DOI] [PubMed] [Google Scholar]
- 28. Gurevich‐Panigrahi T, Panigrahi S, Wiechec E, et al. Obesity: pathophysiology and clinical management. Curr Med Chem. 2009;16:506–521. [DOI] [PubMed] [Google Scholar]
- 29. Araki K, Masaki T, Katsuragi I, et al. Telmisartan prevents obesity and increases the expression of uncoupling protein 1 in diet‐induced obese mice. Hypertension. 2006;48:51–57. [DOI] [PubMed] [Google Scholar]
- 30. Miura Y, Yamamoto N, Tsunekawa S, et al. Replacement of valsartan and candesartan by telmisartan in hypertensive patients with type 2 diabetes: metabolic and antiatherogenic consequences. Diabetes Care. 2005;28:757–758. [DOI] [PubMed] [Google Scholar]
- 31. Gustafson B. Adipose tissue, inflammation and atherosclerosis. J Atheroscler Thromb 2010;17:332–341. [DOI] [PubMed] [Google Scholar]