

Abstract
Hyponatremia is common and is increasingly recognized as an independent prognostic marker that adversely affects morbidity and mortality in various disease states, including heart failure. In acute decompensated heart failure (ADHF), the degree of hyponatremia often parallels the severity of cardiac dysfunction and is further exacerbated by any reduction in glomerular filtration rate and arginine vasopressin dysregulation. A recent study showed that even modest improvement of hyponatremia may have survival benefits. Although management of hyponatremia in ADHF has traditionally focused on improving cardiac function and fluid restriction, the magnitude of improvement of serum sodium is fairly slow and unpredictable. In this article, we discuss the mechanisms of hyponatremia in ADHF, review its evolving prognostic significance, and evaluate the efficacy of various treatments for hyponatremia, including the recently approved vasopressin receptor antagonists for managing hyponatremia among patients hospitalized for ADHF. Copyright © 2008 Wiley Periodicals, Inc.
Dr. Jun Chiong is a member of the Speaker's Bureau of Otsuka Pharmaceutical company. The authors have no additional funding, financial relationships, or conflicts of interest to disclose.
Introduction
Hyponatremia is generally defined as serum sodium (Na) concentration of < 135 mEq/L (1 mEq/L Na = 1 mmol/L Na). Its prevalence in the acute hospital setting ranges from 4% to 45%.1 Nineteen percent to 25% of patients with acute decompensated heart failure (ADHF) have hyponatremia,2, 3, 4 which is independently associated with increasing short‐term and long‐term morbidity and mortality. Even mild hyponatremia among patients with ADHF, regardless of ventricular function, is associated with increased in‐hospital and postdischarge mortality, prolonged hospital length of stay, and frequent rehospitalization. This review will focus on the mechanisms, prognostic significance, and treatment considerations of hyponatremia in ADHF.
Arginine Vasopressin in Sodium and Water Homeostasis
Sodium (Na+) is the major extracellular cation that primarily determines serum osmolality. Under physiologic states, serum osmolality is regulated primarily by arginine vasopressin (AVP), renal responsiveness to AVP, and thirst.5 A 1% to 2% perturbation in serum osmolarity results in accompanying serum AVP changes via a reflex arc designed to maintain fluid and electrolyte homeostasis.6 The baroreceptor‐mediated, nonosmotic release of AVP is the predominant mechanism of hyponatremia in adult hospitalized patients and is more potent than the osmotic path of AVP regulation.7, 8, 9 Thus, a hypo‐osmotic effect to suppress AVP synthesis and release may be overridden by nonosmotic AVP stimulation.
Mechanisms of Hyponatremia in Heart Failure
Ventricular Dysfunction and Neurohormonal Activation
The pathophysiology of the heart failure (HF) syndrome involves the complex interplay between renin‐angiotensin‐aldosterone system (RAAS) activation, sympathetic nervous system stimulation, and nonosmotic AVP release. Though initially triggered to preserve hemodynamic integrity following cardiac injury, these neurohormonal actions, if uncorrected, lead to progressive cardiac dysfunction and retention of salt (sodium chloride; NaCl) and water.
Hyponatremia in HF often parallels the severity of cardiac dysfunction and is further exaggerated by any reduction in glomerular filtration rate and AVP dysregulation.10 Asymptomatic left ventricular dysfunction is associated with preserved Na balance attributed to activation of the cardiac natriuretic peptides. As ventricular dysfunction progresses and clinically evident HF develops, up‐regulation of the maladaptive neurohormonal systems collectively limits distal solute and free water delivery, ensures maximal free water reabsorption, and causes progressive cardiac dysfunction. If uncorrected, this vicious cycle predisposes to hyponatremia.11 RAAS stimulation, primarily through the effect of angiotensin II, increases the resistance of the afferent arterioles, decreases the glomerular filtration rate through reduction of renal perfusion, and increases Na and water reabsorption in the proximal tubule. Sympathetic nervous system activation leads to increased peripheral resistance and heart rate that increase afterload, reduce cardiac output, decrease renal and tissue perfusion, enhance proximal tubular Na reabsorption, and decrease water and Na delivery to the distal diluting segments.12 Circulating levels of AVP are 2× to 3× greater among hyponatremic HF patients compared with normal subjects. The trigger for nonosmotic release of AVP in ADHF remains unclear, but arterial underfilling from reduced cardiac output is the leading hypothesis.13 Both low cardiac output and high angiotensin II levels are also potent thirst stimuli; patients with severe HF may develop hyponatremia with only 1–2 L of water intake per day.11
Diuretic‐Induced Hyponatremia
HF patients are at increased risk for diuretic‐induced hyponatremia because diuretics activate water‐retention pathways similar to those operative in HF. Thiazides are more potent inducers of hyponatremia compared with loop diuretics, because by blocking NaCl cotransport at the distal convoluted duct they increase distal Na delivery and preserve the medullary interstitial gradient, which then effectively prevents the excretion of maximally dilute urine and promotes reabsorption of solute‐free water if AVP is acting at the collecting duct.14 In the largest retrospective review on this subject, thiazide and thiazide‐type diuretics alone or in combination with potassium‐sparing agents were responsible for hyponatremia in 94% of 129 cases. Of note, 97% of the doses were within the limits of pharmacologic recommendations.15 Other proposed mechanisms for diuretic‐induced hyponatremia that both classes of diuretics share are: (1) urinary potassium loss, causing the extracellular Na to shift intracellularly; (2) nonosmotic activation of AVP; and (3) excess thirst, causing increased water intake.
Hypotension From HF Therapeutics vs Progressive Ventricular Dysfunction
Patients with advanced HF who are hyponatremic often have lower systemic blood pressures that limit the adherence to current HF treatment guidelines, because evidence‐based drug therapies for HF that show survival benefits also lower systemic blood pressure. Hypotension is a potent stimulus for the neurohormonal changes seen in HF that cause hyponatremia and cardiac dysfunction.16 Whether hypotension related to progression of cardiac dysfunction and hypotension caused by medical therapy have different consequences is unknown.
Clinical Presentation
The manifestations of hyponatremia are largely related to central nervous system dysfunction secondary to cerebral edema.17 Depending on the rapidity and extent of decline of the serum Na concentration, symptoms may range from nonspecific headache, nausea, vomiting, and disorientation to life‐threatening seizures, coma, respiratory depression, and death.
The brain's compensatory response to hyponatremia‐induced brain swelling is to lose NaCl from the interstitial fluid and potassium and organic osmolytes from the intracellular space. When hyponatremia develops within 48 hours (acute hyponatremia), or when serum Na concentration falls faster than 0.5 mEq/L/hr, irreversible neurologic damage or death may occur if the condition is not emergently addressed.18 In contrast, chronic hyponatremia (>48 h) presents more subtly. But even apparently asymptomatic, mild chronic hyponatremia causes gait disturbances and altered cognition that predispose to increased risk of falls and fractures.19
Hyponatremic ADHF patients tend to have lower systolic blood pressure and worse renal function, and require intravenous inotropes during hospitalization.3 Although the effect of hyponatremia on symptoms specifically for HF patients is uncertain, the Study of Ascending Levels of Tolvaptan in Hyponatremia (SALT) trials have shown significant improved mental component scores of the Short Form‐12 Health Survey if hyponatremia improves.20
Hyponatremia in ADHF: Prognostic Significance
Regardless of the healthcare setting (ie, in‐hospital or ambulatory), ventricular function (depressed or preserved), or the timing of blood draw (on admission, predischarge, or at follow‐up), hyponatremia in HF is associated with adverse short‐term and long‐term morbidity and mortality (Table 1).2, 3, 4, 21, 22, 23, 24, 25, 26 The one exception to this finding is when hyponatremia occurs in the setting of hyperglycemia. Then, serum Na has no prognostic significance.27
Table 1.
Prognostic Studies Evaluating Hyponatremia in ADHF
| Setting | NYHA Class | Study | Findings |
|---|---|---|---|
| Diuretic and digoxin era | |||
| Before and after treatment with ACE inhibitors21 | IV | Prospective cohort (n = 203) | Pretreatment Na <138 meq/L was the strongest predictor of cardiovascular mortality. |
| ACE/ARB, BB, and diuretic era | |||
| Newly diagnosed ADHF patients regardless of systolic function (Canada)22 | NR | Retrospective (n = 4031) | Admission Na <136 meq/L predicts 30‐d and 1‐y mortality |
| Patients with systolic HF who died23 | III‐IV before death | Retrospective (n = 160) | Hyponatremia (mean Na 128 meq/L) was worse in the months preceding death than at the time of death. |
| ADHF with systolic dysfunction (OPTIME‐CHF)24 | III‐IV | Retrospective (n = 949) | Admission Na 132–135 meq/L was associated with increased in‐hospital and 60‐d mortality. |
| ADHF regardless of onset and ventricular function (OPTIMIZE‐HF)2 | III‐IV | Retrospective (n = 47 647) | Admission Na <135 meq/L is independently associated with longer hospital stays and higher in‐hospital and postdischarge 60‐d mortality. |
| ADHF with systolic dysfunction (ESCAPE)3 | IV | Retrospective (n = 433) | Baseline Na <135 meq/L was associated with 6‐mo mortality. Persistent hyponatremia independently predicts mortality, HF hospitalization, and death or rehospitalization despite clinical and hemodynamic improvements similar to normonatremic patients. Patients with corrected Na died more than normonatremic patients but less than persistently hyponatremic patients. The comparison of the latter group is not significant but limited by small number of events. |
| ADHF with systolic dysfunction (ACTIV in HF)4 | III‐IV | Retrospective (n = 301) | Baseline Na <135 meq/L was statistically significant predictor of 60‐d mortality. >2 mEq/L increase among hyponatremic patients was associated with improved survival at 60 d. |
| First hospitalization of patients with HFPEF (EF >50%)25 | II‐IV | Prospective cohort (n = 358) | The risk of 7‐y overall mortality increased by 6% for each 1‐meq/L decrease in baseline serum Na. Patients with normalized Na at discharge had excess 7‐y overall mortality compared with the normonatremic group. Patients with persistent hyponatremia (Na <136 meq/L) had the lowest 7‐y survival. |
| First hospitalization for HF26 | II‐IV | Prospective cohort (n = 735) | Admission Na <136 meq/L is an independent predictor of 7‐y mortality. |
Abbreviations: ACE, angiotensin‐converting enzyme; ACTIV in CHF, Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure; ADHF, acute decompensated heart failure; ARB, angiotensin II receptor blocker; BB, β‐blocker; EF, ejection fraction; ESCAPE, Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness; HF, heart failure; HFPEF, heart failure with preserved ejection fraction; Na, serum sodium concentration; NR, not reported; NYHA, New York Heart Association; OPTIME‐CHF, Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure; OPTIMIZE‐HF, Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With Heart Failure
The first study to establish the prognostic significance of hyponatremia in HF involved 203 New York Heart Association class IV systolic HF patients. In total, 30 clinical, hemodynamic, and biochemical variables were evaluated before and after treatment with vasodilators. Pretreatment hyponatremia was found to be the most powerful predictor of cardiovascular mortality, and this prognostic relationship was modified by use of angiotensin‐converting enzyme inhibitors.21 But despite contemporary, optimal, evidence‐based medical therapy, hyponatremia (when detected) still predicts increased mortality.
The strongest evidence associating hyponatremia in ADHF to long‐term mortality to date is a cohort study that evaluated the relation of serum Na level to 7‐year overall mortality after first hospitalization for HF with preserved ejection fraction.26 Mortality seems to be highest among patents with persistent hyponatremia, lower in those with improved hyponatremia, and lowest in those who maintain normonatremia.
Treatment of Hyponatremia in ADHF
Several factors need to be taken into consideration when choosing the most appropriate treatment for hyponatremia: (1) clinical manifestation, (2) volume status, (3) severity of hyponatremia, (4) rapidity of onset, (5) comorbid illnesses, and (6) rate of correction. The challenge is balancing between the risk of permanent and lethal complications if hyponatremia is treated incorrectly vs the risk of iatrogenic brain injury from overly rapid correction of hyponatremia (>12 mEq/L/d or > 18 mEq/L/48 h). Acute, symptomatic, severe hyponatremia is a medical emergency that demands prompt intervention with hypertonic saline solution (HSS). In this setting, the risk of persistent marked hyponatremia far exceeds any risk from correction of serum Na.28 Conversely, overly rapid correction of chronic hyponatremia causes pontine and extrapontine myelinolysis, the osmotic demyelination syndrome (ODS).29
Hyponatremia among patients with ADHF is usually chronic, rarely overtly symptomatic, or present with serum Na < 120 mEq/L. Administering HSS to this patient subgroup with congestive symptoms and expanded extracellular fluid volume is, therefore, often unnecessary. In the rare event that treatment for acute symptomatic hyponatremia in HF patients is needed, a small, randomized, single‐blind study involving 107 refractory HF patients did show that low‐dose HSS plus a high‐dose loop diuretic (vs high‐dose loop diuretics alone) was safely tolerated, improved hyponatremia, overcame diuretic resistance, and relieved congestive signs and symptoms. Although all patients clinically improved, those on high‐dose diuretics alone had worsening hyponatremia and renal function.30 This study should be interpreted cautiously, because only 10 patients in each arm were hyponatremic.
The management of hyponatremia in ADHF has traditionally focused on improving cardiac function while at the same time restricting fluid intake. Water restriction alone, however, will increase serum Na by only approximately 1–2 mEq/L/day and is poorly tolerated.28 Correction of hypokalemia can improve hyponatremia. Use of lithium and demeclocycline in HF patients is limited by serious renal and/or cardiovascular side effects.11 Vasopressin receptor antagonists (VRAs) are new pharmacologic agents that have been shown to safely and effectively increase serum Na concentration. We shall focus our discussion on tolvaptan and conivaptan, the only VRAs that are approved by the US Food and Drug Administration to treat both euvolemic and hypervolemic hyponatremia.
Vasopressin Receptor Antagonists
AVP release is almost always either increased or inadequately suppressed in persistent hypotonic hyponatremia (once psychogenic polydipsia and pseudohyponatremia are excluded).28 To correct euvolemic and hypervolemic hyponatremia, therefore, AVP synthesis can either be switched off or the site of its action can be blocked. There are 2 major subtypes of vasopressin receptors: V1A and V2. The V1A receptors are found on vascular smooth muscles and cardiomyocytes, affecting vascular tone and myocardial function. V2 receptors are principally located on the basolateral membrane of the cortical and medullary collecting duct, the blockade of which leads to aquaresis, the excretion of electrolyte‐free water.
Tolvapatan
Tolvaptan is the first FDA‐approved oral selective V2 receptor blocker to treat hyponatremia associated with ADHF, liver cirrhosis with ascites, and the syndrome of inappropriate antidiuretic hormone hypersecretion. It was shown in randomized, double‐blind, placebo‐controlled studies to safely and effectively raise serum Na concentration in the short term among patients with euvolemic and hypervolemic hyponatremia.21 A prespecified post hoc analysis of the SALT trials also showed significantly improved mental component scores on the Short Form‐12 Health Survey.
The effects of tolvaptan on ADHF were investigated much earlier by well‐designed clinical trials that showed that tolvaptan was safely tolerated and superior to placebo in reducing body weight and edema and normalizing Na.31 A post hoc analysis of the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Congestive Heart Failure (ACTIV in CHF) trial, which analyzed the effects of changes in serum Na with treatment on the 60‐day mortality among ADHF patients, showed that even modest improvement of hyponatremia may have survival benefits.4 Of the 68 hyponatremic patients, 45 patients whose serum Na improved by ≥ 2 mEq/L were more likely to be alive at 60 days compared with placebo. These findings suggested that treatment of hyponatremia might alter the natural history of HF and provided the rationale for a larger, more definitive investigation.
The Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) trials consisted of 2 multicenter, randomized, double‐blind, placebo‐controlled studies that investigated the effects of tolvaptan on clinical signs and symptoms of HF and an outcome study that combined all patients from the clinical status trials.32 Overall, 4133 patients were randomized to receive tolvaptan 30 mg/day or placebo, plus standard HF treatment, for a minimum of 60 days.33 The mean follow‐up time was 9.9 months. There was an equivalent dropout rate in both arms (20%), attributed to patient request to withdraw from the study and adverse events (mostly dry mouth and thirst) that were similar in both groups. Tolvaptan plus standard HF treatment quickly improved many HF signs and symptoms without serious adverse events. However, there was no difference in the primary endpoints of all‐cause mortality, the composite of cardiovascular death and HF hospitalization, or overall quality of life scores between the groups. It is noteworthy that only 8% of the ADHF patients in this study were hyponatremic, possibly reflecting exclusion of refractory end‐stage HF patients. The findings from EVEREST therefore cannot be generalized to include this subgroup that should theoretically gain the most benefit from treatment with VRAs.
A prespecified post hoc analysis of the EVEREST trials suggested that addition of tolvaptan to standard HF treatment modestly improves dyspnea, whether given early or relatively late after hospitalization.34 Its effects are greatest within 12 hours of the first dose, and although patients continue to report dyspnea improvement up to 60 hours after admission, the magnitude of benefit diminishes with time. Although dyspnea improved regardless of the severity of the patient's baseline dyspnea, the greatest treatment differences were seen in patients with continuous dyspnea at baseline. This study also found a linear correlation between improvement in patient‐assessed dyspnea and reductions in body weight (Figure 1). Whereas weight gain after hospitalization for ADHF strongly predicts HF rehospitalizations, a reduction in body weight as a result of a specific intervention may not necessarily prevent readmissions.35
Figure 1.
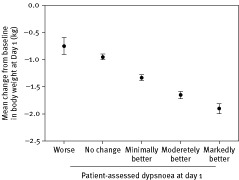
Relationship of patient‐assessed dyspnea to body weight
The hemodynamic effects of tolvaptan in ADHF patients provide a potential mechanistic explanation for the short‐term favorable effects of tolvaptan on dyspnea and sustained body weight reduction. Tolvaptan resulted in modest changes in filling pressures, a dose‐dependent increase in urine output, and increase in free water clearance with no short‐term changes in potassium or renal function. Its ability to achieve these changes while maintaining blood pressure and heart rate (without activating the RAAS) suggests that significant aquaresis may occur primarily by removing excess extravascular volume with minimal reduction in intravascular volume.36
Conivaptan
Conivaptan is the first intravenous nonpeptide VRA that blocks both V1A and V2 receptors and is FDA‐approved for short‐term treatment of euvolemic and hypervolemic hyponatremia. In a randomized, placebo‐controlled trial involving 84 hospitalized patients, conivaptan 40 mg/day was superior to placebo in improving euvolemic or hypervolemic hyponatremia and increased serum Na by ≥ 4 mEq/L in 24 hours; a 6‐ mEq/L increase with normalization of serum Na was achieved in 69% of patients after 4 days.37
In the first randomized, placebo‐controlled study investigating the utility of conivaptan exclusively among New York Heart Association class III or IV HF patients, 142 patients were randomized to receive a single intravenous dose of conivaptan (10, 20, or 40 mg) or placebo.38 Conivaptan in the 20‐mg and 40‐mg groups led to dose‐dependent decrease in pulmonary capillary wedge and right atrial pressures, along with a dose‐dependent increase in urine output compared to placebo. Changes in cardiac index, systemic/pulmonary vascular resistance, blood pressure, or heart rate were similar to placebo.
In another randomized, double‐blind, placebo‐controlled trial, 170 patients with ADHF received conivaptan (a 20‐mg loading dose followed by continuous infusion of 40, 80, or 120 mg/d for 2 d) or placebo, plus standard therapy.39 Conivaptan significantly increased urine output (1–1.5 L/d), was hemodynamically well tolerated, and had minimal side effects, but it did not improve respiratory symptoms.
Clinical Application of VRAs
VRAs were proven safe and effective in correcting euvolemic and hypervolemic hyponatremia in properly selected patients who were closely followed up. The rate of change in serum Na concentration seems to be greatest during the first 24 hours after drug administration; therefore, fluid restriction should be avoided during this time. After all, thirst, dry mouth, and polyuria are among the most commonly encountered adverse effects of VRAs. Because they can cause brisk and prolonged diuresis, VRAs are contraindicated in hypovolemic hyponatremia and should be initiated or reinitiated only in the hospital setting, where serum Na can be closely monitored. The risk of overly rapid correction of chronic hyponatremia causing ODS is a concern, but no cases of ODS have been reported to date.
There is no evidence to date that supports the use of VRAs in patients with acutely symptomatic severe hyponatremia, serum creatinine > 3.5 mg/dL, end‐stage renal disease, and refractory end‐stage HF. The SALT trials did show that serum Na may drop within a week after tolvaptan is discontinued; therefore, optimal treatment of the underlying cause(s) of hyponatremia is recommended prior to discontinuing this drug. The serum Na should be closely followed thereafter.
Conclusion
Hyponatremia in ADHF is a marker of advanced disease severity and predicts increased morbidity and mortality. The currently available VRAs safely and effectively improve hyponatremia, increase urine output, modestly improve dyspnea, and sustain weight loss while preserving hemodynamic status, electrolyte homeostasis, and renal function among patients with ADHF. Although current evidence shows that addition of VRAs to a standard HF regimen does not confer additional survival benefits, further prospective studies are needed to determine whether this holds true for the hyponatremic HF population. Meanwhile, careful adherence to evidence‐based dosing and close follow‐up is needed when administering VRAs to prevent the theoretical but potentially catastrophic risk of ODS.
Acknowledgements
The authors thank Karen Klein, MA, ELS, for her editorial comments.
References
- 1. Upadhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia. Am J Med 2006; 119(7 suppl 1): S30–S35. [DOI] [PubMed] [Google Scholar]
- 2. Gheorghiade M, Abraham WT, et al.; for OPTIMIZE‐HF Investigators and Coordinators. Relationship between admission serum sodium concentration and clinical outcome in patients hospitalized for heart failure: an analysis from the OPTIMIZE‐HF registry. Eur Heart J 2007; 28: 980–988. [DOI] [PubMed] [Google Scholar]
- 3. Gheorghiade M, Rossi J, et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE trial. Arch Intern Med 2007; 167: 1998–2005. [DOI] [PubMed] [Google Scholar]
- 4. Rossi J, Bayram M, Udelson JE, et al. Improvement in hyponatremia during hospitalization for worsening heart failure is associated with improved outcomes: insights from the Acute and Chronic Therapeutic Impact of Vasopressin Antagonist in Chronic Heart Failure (ACTIV in CHF) trial. Acute Card Care 2007; 9: 82–86. [DOI] [PubMed] [Google Scholar]
- 5. Robertson GL. Antidiuretic hormone: normal and disordered function. Endocrinol Metab Clin North Am 2001; 30: 671–694. [DOI] [PubMed] [Google Scholar]
- 6. Wong LL, Verbalis JG. Systemic diseases associated with diseases of water homeostasis. Endocrinol Metab Clin North Am 2002; 31: 121–140. [DOI] [PubMed] [Google Scholar]
- 7. Anderson RJ, Chang HM, Kluge R, et al. Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Ann Intern Med 1985; 102: 164–168. [DOI] [PubMed] [Google Scholar]
- 8. Schrier RW, Berl T. Nonosmolar factors affecting renal water excretion (first of 2 parts). N Engl J Med 1975; 292: 81–88. [DOI] [PubMed] [Google Scholar]
- 9. Schrier RW, Berl T. Nonosmolar factors affecting renal water excretion (second of 2 parts). N Engl J Med 1975; 292: 141–145. [DOI] [PubMed] [Google Scholar]
- 10. Sica DA. Sodium and water retention in heart failure and diuretic therapy: basic mechanisms. Cleve Clin J Med 2006; 73(suppl 2): S2–S7. [DOI] [PubMed] [Google Scholar]
- 11. Sica DA. Hyponatremia and heart failure—treatment considerations. Congest Heart Fail 2006; 12: 55–60. [DOI] [PubMed] [Google Scholar]
- 12. Oren RM. Hyponatremia in congestive heart failure. Am J Cardiol 2005; 95: 2B–7B. [DOI] [PubMed] [Google Scholar]
- 13. Schrier RW, Ecder T. Unifying hypothesis of body fluid volume regulation: implications for cardiac failure and cirrhosis. Mt Sinai J Med 2001; 68: 350–361. [PubMed] [Google Scholar]
- 14. Abramow M, Cogan E. Clinical aspects and pathophysiology of diuretic‐induced hyponatremia. Adv Nephrol Necker Hosp 1984; 13: 1–28. [PubMed] [Google Scholar]
- 15. Sonnenblick M, Friedlander Y, Rosin AJ. Diuretic‐induced severe hyponatremia review and analysis of 129 reported patients. Chest 1993; 103: 601–606. [DOI] [PubMed] [Google Scholar]
- 16. Miller WL, Skouri HN. Chronic systolic heart failure, guideline‐directed medical therapy, and systemic hypotension—less pressure but maybe more risk (does this clinical scenario need more discussion?). J Card Fail 2009; 15: 101–107. [DOI] [PubMed] [Google Scholar]
- 17. Androgué HJ, Madias NE. Hyponatremia. N Engl J Med 2000; 342: 1581–1589. [DOI] [PubMed] [Google Scholar]
- 18. Soupart A, Decaux G. Therapeutic recommendations for management of severe hyponatremia: current concepts on pathogenesis and prevention of neurologic complications. Clin Nephrol 1996; 46: 149–169. [PubMed] [Google Scholar]
- 19. Renneboog B, Musch W, Vandemergel X, et al. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med 2006; 119: 71.e1–71.e8. [DOI] [PubMed] [Google Scholar]
- 20. Schrier RW, Gross P, Gheorghiade M, et al. Tolvaptan, a selective oral vasopressin V2‐receptor antagonist, for hyponatremia. N Engl J Med 2006; 355: 2099–2112. [DOI] [PubMed] [Google Scholar]
- 21. Lee WH, Packer M. Prognostic importance of serum sodium concentration and its modification by converting‐enzyme inhibition in patients with severe chronic heart failure. Circulation 1986; 73: 257–267. [DOI] [PubMed] [Google Scholar]
- 22. Lee D, Austin PC, Rouleau JL, et al. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA 2003; 290: 2581–2587. [DOI] [PubMed] [Google Scholar]
- 23. Teuteberg JJ, Lewis EF, Nohria A, et al. Characteristics of patients who die with heart failure and a low ejection fraction in the new millennium. J Card Fail 2006; 12: 47–53. [DOI] [PubMed] [Google Scholar]
- 24. Klein L, O'Connor CM, Leimberger JD, et al; for OPTIME‐CHF Investigators. Lower serum sodium is associated with increased short‐term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME‐CHF) study. Circulation 2005; 111: 2454–2460. [DOI] [PubMed] [Google Scholar]
- 25. Rusinaru D, Buiciuc O, Leborgne L, et al. Relation of serum sodium level to long‐term outcome after a first hospitalization for heart failure with preserved ejection fraction. Am J Cardiol 2009; 103: 405–410. [DOI] [PubMed] [Google Scholar]
- 26. Tribouilloy C, Buiciuc O, Rusinaru D, et al. Long‐term outcome after a first episode of heart failure: a prospective 7‐year study. Int J Cardiol 2010; 140: 309–314. [DOI] [PubMed] [Google Scholar]
- 27. Milo‐Cotter O, Cotter G, Weatherley BD, et al. Hyponatraemia in acute heart failure is a marker of increased mortality but not when associated with hyperglycaemia. Eur J Heart Fail 2008; 10: 196–200. [DOI] [PubMed] [Google Scholar]
- 28. Sterns RH, Nigwekar SU, Hix JK. The treatment of hyponatremia. Semin Nephrol 2009; 29: 282–299. [DOI] [PubMed] [Google Scholar]
- 29. Sterns RH, Cappuccio JD, Silver SM, et al. Neurologic sequelae after treatment of severe hyponatremia: a multicenter perspective. J Am Soc Nephrol 1994; 1552–1530. [DOI] [PubMed] [Google Scholar]
- 30. Licata G, Di Pasquale P, Parrinello G, et al. Effects of high‐dose furosemide and small‐volume hypertonic saline solution infusion in comparison with a high dose of furosemide as bolus in refractory congestive heart failure: long‐term effects. Am Heart J 2003; 145: 459–466. [DOI] [PubMed] [Google Scholar]
- 31. Gheorghiade M, Niazi I, Ouyang J, et al. Vasopressin V2‐receptor blockade with tolvaptan in patients with chronic heart failure: results from a double‐blind, randomized trial. Circulation 2003; 107: 2690–2696. [DOI] [PubMed] [Google Scholar]
- 32. Gheorghiade M, Konstam MA, Burnett JC Jr, et al; for Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Short‐term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA 2007; 297: 1332–1343. [DOI] [PubMed] [Google Scholar]
- 33. Konstam MA, Gheorghiade M, Burnett JC Jr, et al; for Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA 2007; 297: 1319–1331. [DOI] [PubMed] [Google Scholar]
- 34. Pang PS, Konstam MA, Krasa HB, et al; for Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Effects of tolvaptan on dyspnea relief from the EVEREST trials. Eur Heart J 2009; 30: 2233–2240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Blair JE, Khan S, Konstam MA, et al; for EVEREST Investigators. Weight changes after hospitalization for worsening heart failure and subsequent re‐hospitalization and mortality in the EVEREST trial. Eur Heart J 2009; 30: 1666–1673. [DOI] [PubMed] [Google Scholar]
- 36. Udelson JE, Orlandi C, Ouyang J, et al. Acute hemodynamic effects of tolvaptan, a vasopressin V2 receptor blocker, in patients with symptomatic heart failure and systolic heart failure: an international, multicenter, randomized, placebo‐controlled trial. J Am Coll Cardiol 2008; 52: 1540–1545. [DOI] [PubMed] [Google Scholar]
- 37. Zeltser D, Rosansky S, van Rensburg H, et al; Conivaptan Study Group. Assessment of the efficacy and safety of intravenous conivaptan in euvolemic and hypervolemic hyponatremia. Am J Nephrol 2007; 27: 447–457. [DOI] [PubMed] [Google Scholar]
- 38. Udelson JE, Smith WB, Hendrix GH, et al. Acute hemodynamic effects of conivaptan, a dual V(1A) and V(2) vasopressin receptor antagonist, in patients with advanced heart failure. Circulation 2001; 104: 2417–2423. [DOI] [PubMed] [Google Scholar]
- 39. Goldsmith SR, Elkayam U, Haught WH, et al. Efficacy and safety of the vasopressin V1A/V2‐receptor antagonist conivaptan in acute decompensated heart failure: a dose‐ranging pilot study. J Card Fail 2008; :14: 641–647. [DOI] [PubMed] [Google Scholar]