

Abstract
Background
World Health Organization (WHO) has created an essential list of in-vitro diagnostics. Supply chain management (SCM) is said to be the vehicle that ensures that developed point-of-care (POC) tests reach their targeted settings for use. We therefore, mapped evidence on SCM of and accessibility to POC testing (availability and use of POC tests) in low- and middle-income countries (LMICs).
Methods
We conducted a systematic scoping review using Arksey and O’Malley’s framework as a guide. We searched PubMed; CINAHL; MEDLINE; WEB of Science; Science Direct; and Google Scholar databases for studies that focused on POC diagnostic tests and SCM. The review included studies that were undertaken in 140 countries defined by the World Bank as LMICs published up to August 2017. Two reviewers independently screened the abstracts and full articles against the eligibility criteria. The study used the mixed methods appraisal tool version 2011 to assess the risk of bias for the included studies. NVivo version 11 was employed to extract themes from all included studies and results presented using a narrative approach.
Results
Of 292 studies identified in this review, only 15 published between 2009 and 2017 included evidence on POC diagnostics and SCM. Of the 15 studies, three were conducted in Zambia, one each in Mozambique, Uganda, Guatemala; South Africa, one in Burkina Faso, Zimbabwe, and one multi-country study (Tanzania, Uganda, China, Peru and Zambia and Brazil). Six studies were not country specific since they were not primary studies. Majority of the studies reported stock-outs of HIV, syphilis, and malaria POC tests. There was a moderate to substantial level of agreement between the reviewers’ responses at full article screening stage (Kappa statistic = 0.80, p < 0.01). Nine studies underwent methodological quality appraisal and all, scored between 90 and 100%.
Conclusions
The results demonstrated limited published research on SCM of and accessibility to POC testing in LMICs. Further studies aimed at investigating SCM of POC tests in resource-limited settings to identify the barriers/challenges and provide a context-specific evidence-based solutions for policy/decision makers, implementers, and POC developers, funders, and development partners would be essential.
PROSPERO registration number
CRD42016043711.
Electronic supplementary material
The online version of this article (10.1186/s12913-019-4351-3) contains supplementary material, which is available to authorized users.
Keywords: Point of care diagnostics; supply chain management; accessibility, Availability, Use, Low-and-middle-income countries
Background
Access to accurate, safe and appropriate point-of-care (POC) testing is vital for routine care, early diseases, and monitoring of diseases [1]. A POC diagnostic tests refer to medical device used for detection, diagnosis, and monitoring of diseases at the POC or near where healthcare service is provided [2–6]. POC testing deliver prompt results for clinical decisions as well as early referrals [4]. Access to POC testing services reduces test result turnaround times and facilitates prompt disease diagnosis and treatment initiation [6]. World Health Organization (WHO) encourages countries to establish their own essential diagnostic list based on the country’s disease burden and epidemiology to improve access to healthcare services [7]. Access to POC testing services can improve health outcomes particularly, in resource-limited settings.
Accessibility to POC diagnostic services is dependent on many factors, including an efficiently managed SCM, which is agile, flexible and responsive [8, 9]. Efficiently managed SCM ensures that appropriate POC diagnostics are available for use by health care professionals to perform test for patients who need it [1, 10]. This study defined SCM according to Pinna et.al. (2015) and Management Science for Health (2012) [10, 11]. SCM of POC diagnostic tests is therefore, defined to include POC test development, selection, forecasting and quantification, procurement, quality assurance, distribution, inventory management, redistribution, usage, and safe disposal of used test kits at the POC [10, 11]. A poor supply chain system may pose a threat to the availability and POC tests usage in rural primary health care facilities [9, 12, 13]. Poor SCM of POC diagnostics could also affect the implementation and sustainability of POC diagnostic services for vulnerable populations such as pregnant women in hard-to-reach communities [14–16] and may result in poor accessibility to POC diagnostic services for essential care [17–19]. Thus, health care SCM is more complex when compared to other industries because of its impact on people’s health [20].
Considering the potential challenges SCM could pose to accessibility of POC diagnostic services particularly in rural communities in LMICs, POC test availability and use, there is an urgent need to explore the role of SCM to help address supply chain barriers of POC diagnostic services in resource-limited settings and rural primary health care clinics. Therefore, this study aimed to map evidence on SCM of and accessibility to POC testing focusing on availability and use of POC tests in LMICs.
Methods
Purpose of the scoping study
We explored SCM and accessibility to POC testing using a scoping review methodology and adduced evidence on availability and use of POC tests in LMICs. A scoping study is useful and enables the identification of research gaps by mapping literature on a research question of interest as prescribed by the enhanced 2005 Arksey and O’Malley’s framework [21, 23]. A scoping review study prior to the conceptualization of a primary research question or a systematic review and meta-analysis may also be useful. We adopted the Preferred Reporting Items for Systematic Reviews and Meta-Analyses [22], and the enhanced Arksey and O’Malley’s framework [21, 23] to guide this study. Prior to the conduct of this study, we registered the review protocol in international prospective register of systematic reviews (CRD42016043711) [24].
Identifying the research question
The main review question was: What is the evidence on supply chain management and accessibility to POC testing services (availability and use) in LMICs?
The sub review questions were as follows:
What is the evidence on availability of POC tests in LMICs?
What is the evidence on use of POC tests in LMICs?
Population, Intervention, Comparison, and Outcome (PICO) framework was used to determine the eligibility of the primary research question as shown in Table 1.
Table 1.
PICO framework for defining the eligibility of the studies for the primary research question
| P-Population | All types of point of care diagnostics |
|---|---|
| I-Interventions | Supply chain management (production, selection, quantification, procurement, storage, distribution, redistribution, quality assurance, inventory management, negotiation with suppliers, and safe disposal of use POC diagnostics) |
| C-Comparison | Absent supply chain management measures |
| O-Outcomes | Availability of POC diagnostic tests Use of POC diagnostic tests |
Literature search
We conducted a systematic literature search from the following databases: PubMed; EBSCOhost (CINAHL and MEDLINE); WEB of Science; Science Direct; and Google scholar. The database search occurred in June up to August 2017 using the following keywords: “diagnostics” “supply chain” “POC diagnostics” “supply chain management” (Additional file 1). Boolean terms (AND/ OR) were used to separate the keywords. Date, language, and study design restrictions were removed to broaden the search and capture the full range of literature on POC diagnostics and supply chain management.
Study selection
Guided by the eligibility criteria, DK conducted the database search and screened the titles. DK and NG then independently screened the abstracts and full articles in parallel. At the abstract screening stage, differences in reviewers’ responses were discussed by the review team until consensus was reached. However, a third reviewer (BV) addressed all discrepancies at the full article screening stage.
Eligibility criteria
Inclusion criteria
Included studies that met the following criteria:
Evidence of POC diagnostics
Evidence of the study been conducted in a LMIC
Evidence of POC diagnostics production
Evidence of POC diagnostics selection
Evidence of POC diagnostics quantification
Evidence of POC diagnostics procurement
Evidence of POC diagnostics storage
Evidence of POC diagnostics distribution
Evidence of POC diagnostics redistribution
Evidence of POC diagnostics quality assurance
Evidence of POC diagnostics inventory management
Evidence of negotiation with suppliers for POC diagnostics supply
Evidence of safe disposal of used POC diagnostics products
Evidence of POC diagnostics accessibility
Evidence of POC diagnostics availability
Evidence POC diagnostics use
Exclusion criterias
A study was excluded if it did not meet the inclusion criteria. The exclusion criteria included the following:
Lack of evidence of POC diagnostics
Studies conducted in high income countries
Laboratory based POC diagnostics
Studies that do not report on the primary outcomes of the study
Charting the data
The selected studies were thoroughly read for data extraction of bibliographic details, aim/objective, study design, targeted population, intervention(s), relevant outcome(s), study setting, type(s) of POC diagnostics used, SCM interventions, and relevant outcomes of interest were extracted. Other information such as geographical location (rural or urban), country of the study, as well as, funding sources were also extracted. Data on country levels of income were obtained from The World Bank Group July, 2017 open data [25].
Quality of the evidence
We used the 2011 version of the mixed methods appraisal tool (MMAT) [26] to appraised all included primary studies. We appraised the included primary studies under the appropriate study designs as prescribed by the MMAT. DK and BV appraised the studies and areas of disagreement in ratings were resolved through discussion. A quality percentage score of ≤50%, 51–75%, 76–100%, was interpreted as low quality, average quality, and high-quality respectively.
Results
Two hundred and ninety-two (292) articles met the eligibility criteria following deletion of 22 duplicates from the total 314 articles identified at the title screening stage (Fig. 1). Subsequently, 262 and 16 articles were also excluded following abstract and full screening respectively. Reasons for the exclusion after full article screening were: one study was not conducted in a LMIC [27], two studies reported no evidence of both supply chain management or the primary outcomes of this study [28–30]; four studies reported no information for POC diagnostics [31–34]; three studies had undefined study setting [35–37] and; five studies reported laboratory-based POC testing [38–42]. In all, 15 studies met the study eligibility criteria for data extraction including one study identified following an updated searched. There was a moderate to substantial level of agreement between the reviewers’ responses at full article screening stage (Kappa statistic = 0.80, p < 0.01) (Additional file 2). Thematic content analysis was conducted using the following themes: POC diagnostics accessibility; availability and; usage. NVivo version 11 was employed to extract themes from all included studies and results presented using a narrative approach. Emerging themes were also reported.
Fig. 1.

PRISMA 2009 Flow Diagram
Characteristics of included studies
Tables 2 and 3 summarises the characteristics of the 15 included studies and findings. The 15 studies comprised of: one cluster randomized controlled trial [43], three cross-sectional studies [44–46], one quasi-experimental study [47], two mixed methods studies [48, 49], one cohort study [50], one qualitative study [51], and six expert reviews [52–57]. All included studies were published in English language between 2009 and 2017. All included studies reported on different POC diagnostic algorithms. Of the 15 studies, five studies were on HIV POC testing [46, 50, 52, 53, 56], three on rapid syphilis testing (RSTs) [47, 49, 51], three on malaria RDTs [43, 45, 48], two reported generally on POC diagnostics [54, 57], one on diabetes, blood pressure and dyslipidaemia assays [55], and one on HIV, RST, and hepatitis b virus RDTS [44]. Seven studies were conducted in rural settings [43–46, 50, 51, 56], and eight studies in both rural and urban [47–49, 52–55] (Fig. 2). Of the 15 studies, three were conducted in Zambia [43, 47, 51]; one in Mozambique [48], one in Uganda [45], one in Guatemala [44], one in Tanzania, Uganda, China, Peru and Zambia and Brazil [49], one in South Africa [46], and one in Burkina Faso and Zimbabwe [50], and six studies were not country specific since they were not primary studies [52, 54–57] (Fig. 3).
Table 2.
Characteristics and finding of studies included in this scoping review
| Author and year | Target Population | Type of POC diagnostic | Supply chain management measures reported | Desirable outcome |
|---|---|---|---|---|
| Alemnji et al., 2011 [56] | General population | HIV | Challenges in procurement, reagent inventory and stock maintenance; timely and quality testing; and challenges with who manages the supply chain systems | Affected confidence in test results and patient care; huge challenges with accessing testing services when services are available at the national level. |
| Ansbro et al., 2015 [51] | Pregnant women | Syphilis RSTs | Quality assurance activities and supervision | Reduced clinic waiting time, travel time and increased case detection and treatment, Acceptability and usability of RST kits and quality assurance activities, supply of RST kits less reliable, and stock-out |
| Bonawitz et al., 2015 [47] | Pregnant women | Syphilis RSTs | None reported | High levels to complete stock-outs at baseline, midline and end line periods over several weeks |
| Hamer et al., 2012 [43] | children < 5 years | Malaria RDTs | Transparent record keeping, adequate supplies, stock management, daily registers and periodic reconciliation of stocks, and ensuring that none had passed their expiration dates | Availability and use of malaria RDTs with over 98% accountability of the RDTs |
| Hasselback et al., 2014 [48] | General population | Malaria RDTs | Analysis of distribution system characteristics | High levels of stock-out |
| Kyabayinze et al., 2012 [45] | General population | Malaria Microscopy and RDTs | None reported | limited availability of RDTs, limited use of RDTs, lack storage space, and lack of glucometers |
| Mabey et al., 2012 [49] | Pregnant women and Sexually active populations | Syphilis RDTs | Training in stock management, record keeping, and quality control, monitoring supply chain problems and provision of sustainable solutions in case of stock-outs | improve access, increase antenatal clinic attendance, availability and use of RSTs |
| McGuire et al., 2014 [55] | General population | Diabetes, Blood Pressure, and Dyslipidemia assays | Reported frequent challenges with distribution of devices | Stock-outs and limited use of devices |
| Peeling, 2015 | General population | Not specified | Called for redistribution when necessary | Prevent diagnostics from expiring |
| Peeling and Ronald, 2009 [54] | General population | Not specified | Reported supply chain failure | Test stock-outs |
| Shott et al., 2012 [53] | General population | HIV | Challenges with quality management (QM)systems | Good QM ensures accuracy of devices; transform the availability of tests in real time; and inform proper patient care. |
| Smith et al., 2015 [44] | Pregnant women | HIV, Syphilis, and HBV RDTs | No supply chain management measures | Increased coverage increase uptake, test stock-outs, limited uptake, and low testing |
| Stevens et al., 2014 [52] | General population | HIV viral load | Raises challenges with reimbursement, quality monitoring, lack guideline and regulations | Where VL testing is available, frequency of CD4 monitoring is reduces or stopped altogether |
| Thairu et al., 2011 [50] | General population | HIV (CD4 testing with Guava EasyCD4 | Guava offered to provide a robust supply chain for reagents and maintenance | Increase access to CD4 testing, low repeated testing, poor stock management, tardy response from Guava resulting in lost operating time |
| Jaya et al., 2017 [46] | Clinics | HIV rapid testing kits | Compliance to guidelines for purchasing and inventory. | HIV rapid test kits shortage in 4 clinics |
Table 3.
Characteristics of included studies and findings
| Author and date | Country | Geographical area | Study setting | Study design |
|---|---|---|---|---|
| Alemnji et al., 2011 [56] | Developing countries | Rural | Resource limited settings | Expert review |
| Ansbro et al., 2015 [51] | Zambia | Rural | Antenatal clinic | Mix method |
| Bonawitz et al., 2015 [47] | Zambia | Urban and Rural | Antenatal clinic | Quasi-experimental evaluation |
| Hamer et al., 2012 [43] | Zambia | Rural | Children clinic | Cluster-randomised controlled trial |
| Hasselback et al., 2014 [48] | Mozambique | Urban and Rural | General clinics | Mix method |
| Kyabayinze et al., 2012 [45] | Uganda | Rural | General clinic | Cross-sectional survey |
| Mabey et al., 2012 [49] | Tanzania, Uganda, China, Peru and Zambia and Brazil | Urban and Rural | Antenatal clinics and Community-based | Mix Method |
| McGuire et al., 2014 [55] | Developing Countries | Urban and Rural | Primary and secondary health facilities | Narrative review |
| Peeling, 2015 | Developing Countries | Urban and Rural | Resource limited settings | Expert review |
| Peeling and Ronald, 2009 [54] | Developing Countries | Urban and Rural | Resource limited settings | Narrative Review |
| Shott et al., 2012 [53] | Sub-Sahara Africa | Urban and rural | Resource limited settings | Expert review |
| Smith et al., 2015 [53] | Guatemala | Rural | Antenatal clinics and Community-based | Cross-sectional survey |
| Stevens et al., 2014 [52] | Developing countries | Urban and rural | Resource limited settings | Expert review |
| Thairu et al., 2011 [50] | Burkina Faso and Zimbabwe | Rural | Hospital and community-based clinic | Cohort study |
| Jaya et al., 2017 [46] | South Africa | Rural | Primary Healthcare Clinics | Cross-sectional (Audit) |
Fig. 2.
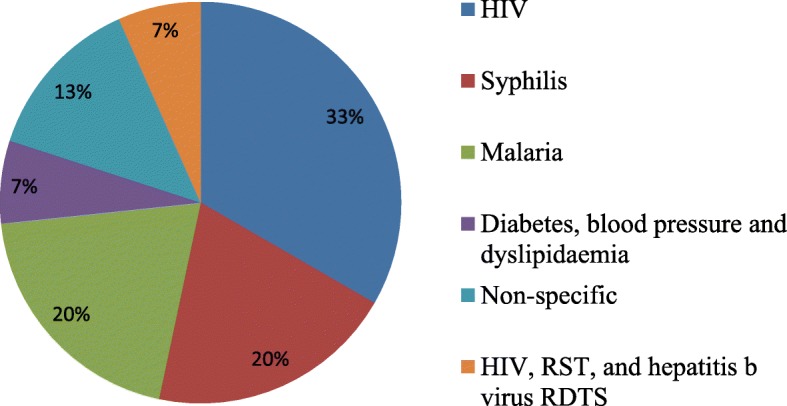
Population of POC test
Fig. 3.
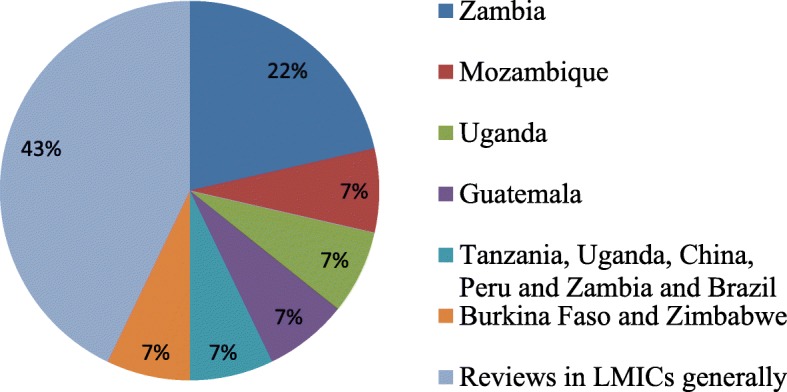
Distribution of countries where included studies were conducted
Quality of evidence
Of the 15 studies, nine underwent methodological quality assessment [43–45, 47–51] using the MMAT – Version 2011 [26]. The remaining six were excluded because they were not primary studies [52–57]. The nine studies which underwent methodological quality appraisal scored between 90 and 100%. Of these, six studies scored the highest quality score of 100% [43–48]. Two studies scored an average of 91.7% [50, 51], and the remaining one study scored 90% [49].
Study findings
Availability of POC diagnostics
A total of 13 studies reported on availability of POC diagnostics in LMICs [43–48, 50, 52–56]. Of the 13 studies, 11 reported stock-out of various POC diagnostics including: RSTs, malaria RDTs, HIV, hepatitis b virus, blood pressure, diabetes, and dyslipidaemia POC assays [43–48, 50, 51, 53–55].
Availability of rapid syphilis tests
A study aimed at comparing healthcare workers experiences and challenges in scaling up from a highly supported non-Government Organization-led pilot to a large-scale ministry of health-led national programme in Zambia has shown that half of the piloted sites reported a stock-out on one occasion [51]. It was also shown that almost a third of rollout sites reported a complete stock-out of RSTs during the month preceding interviews [51]. Another study in Zambia that evaluated the impact of RST and treatment in pregnant women also reported stock-out of RSTs at various stages [47]. A total of 33.3% (2/6) of the facilities documented stock-outs during the baseline ranging from 8 to 20 weeks, 33% (5/15) during the midline period ranging from 4 to 12 weeks with a median stock-out period of 6 weeks; and 60% (9/15) during the end line period ranging from 1 to 16 weeks, with a median stock-out period of 5.5 weeks [47]. Peeling and Ronald (2009) further reported that RSTs stock-out was one of the causes of poor levels of syphilis testing among pregnant women in LMICs [54]. The findings showed weaknesses in the supply chain system such as procurement, inventory and stock management, and human resource capacity for SCM during implementation hence, resulted in significant RST stock-outs.
Availability of malaria RDTs
A substantial high levels of malaria RDTs stock-out was reported in Capo Delgado province in Mozambique [48]. This high levels of stock out was associated with poor test usage [48]. Estimated loss of consumption percentage for malaria RDTs were significantly high with a weighted average of 78% [48]. Increased rates of stock-outs were observed with increasing levels of consumption [48]. In a study aimed at assessing health system’s capacity to absorb Parasite based Malaria Diagnosis in Uganda has shown that, malaria RDTs were available only in 24% (30) out of the 125 lower level health facilities [45]. The study also reported limited availability of malaria RDTs, as well as lack of glucometers [45]. A survey aimed at assessing the quality and safety of having community health workers (CHWs) use RDTs and provide integrated management of malaria and pneumonia revealed 72.2% of CHWs did not receive malaria RDTs kits for 6 months [43].These findings demonstrate limited availability of malaria RDTs, stock out of malaria RDTs, and lack of glucometers in the study settings. The findings also demonstrate that further research is needed to determine the impact of malaria RDTs stock outs on patients’ outcomes in these settings.
Availability of HIV test, HBV test, and other assays
A study conducted in rural antenatal clinic and community- based settings in Guatemala showed that nearly half of the women who turned up for HIV, syphilis, and hepatitis b virus testing services did not get tested partly due to stock-outs [44]. Another study has also demonstrated the prevalence of blood pressure monitoring devices, diabetes, and dyslipidaemia POC assays stock-outs in LMICs [55]. It was reported that manufacturers of new assays entering the market are most often unable to meet the demand of rapid recommendations [52]. A delayed response by Guava trained technicians resulted in Guava EasyCD4 downtimes of 8 out of 45 months, nearly 18% of the total available operating time was reported [50]. In addition, poor stock management resulted in expiration of Guava EasyCD4 since the shelf life was limited to 12 months from the time of production [50]. Shott et al. (2012) noted that, quality management systems of POC diagnostics can really transform the availability of tests in real time to inform proper patient care [53]. Jaya et al. (2017) study findings in primary healthcare clinics in rural KwaZulu-Natal in South Africa showed 4 out of eleven clinics reported past experiences of HIV rapid test kits shortage [46]. Three of the 4 clinics, informed patients when there was a shortage and asked them to return at a later date, whilst the fourth clinic referred the patients to neighbouring healthcare facilities [46]. A study aimed to highlight challenges faced in decentralizing POC testing showed that access to HIV testing can be challenging when the service is only available at the national level [56]. It also demonstrated that long turn-around time for release of test results accounted for a significant proportion of people failing to return for test results in LMICs [56]. These findings reveal stock-outs of HIV and HBV test kits, CD4 test, blood pressure monitoring devices, diabetes, and dyslipidaemia POC assays that requires further investigations to ascertain the supply chain management challenges for these diagnostics in LMICs.
Reasons for POC diagnostic stock-out
This review revealed that POC test stock-outs mostly was due to poor quantification and forecasting, inventory management of POC diagnostic tests, and inadequate/lack of supervision during implementation [44, 51, 54]; inaccurate documentations and distribution systems [48, 57]; lack of storage space [45]; and poor commodity management [47]. The rest included: high cost and poor quality management systems [52, 53]; poor regulatory controls and limited guideline [52]; and inability of production line to meet global uptake [52]. Therefore, future studies are recommended in LMICs aiming at determining the impact of diagnostic test stock-outs and health outcomes especially for HIV, syphilis, and malaria test.
Use of POC diagnostics
Use of POC diagnostics by healthcare workers most often is facilitated by availability of the test ensured through adequate SCM and training. Use of POC diagnostics in this review was reported by 7 out of the 15 studies [43–45, 47–50]. Of the 7 studies, 3 reported malaria RDTs and RST use [43, 49, 51]. The remaining 4 studies reported as follows: limited used of malaria RDTs [45], limited used of blood pressure, diabetes, and dyslipidaemia assays [55], low testing of HBV [44], and low repeated CD4 testing [50].
In a study aimed to assess the quality and safety of having community health workers use rapid diagnostic tests found 96.3% (939/973) of malaria RDTs use for testing children during follow-up visit [43]. Hasselback et al. (2014) found significantly high levels of lost consumption for malaria RDTs ranging from 0 to 149% with an average of 78% weighted by consumption [48]. In addition, malaria RDTs use increased approximately by 300% during rainy seasons [48]. It further reported that consumption was limited up to the point of stock-out [48]. Kyabayinze et al. (2013) found only 20% malaria RDTs use [45]. This outcome demonstrates increased use of malaria RDTs during rainy seasons though usage can also be limited by stock outs, hence needs to be addressed to ensure increased availability of RDTs during rainy season.
Use of syphilis, HIV and HBV diagnostics
A research study conducted in Zambia showed increased syphilis testing during the early stages of RSTs introduction but subsequently dropped at the midline and end line [47]. It demonstrated increased syphilis testing from (140/1365, 10.6%) at the baseline to (976/1446, 67.5%) midline, and dropped to (752/1337, 56.3%) at the end line (P < 0.001) for both midline and end line compared with the baseline [47]. Mabey et al. (2012) study in Tanzania, Uganda, China, Peru and Zambia and Brazil has shown that more than 100,000 pregnant women were tested for syphilis in all the study site [49]. It also showed that in Brazil, healthcare workers exceeded the original set target (30–40%) in remote communities and succeeded in testing 55% of the sexually active population for syphilis [49]. Smith et al. (2015) indicated that, HIV and syphilis testing uptake by pregnant women was 50.3% HIV and 42.2% for HBV following the introduction of these tests in the antenatal clinic [44]. The study also reports corresponding increases for HIV and syphilis testing uptake as 143.9% (P < 0.001) and of 1.3% (P = 0.87) respectively [44]. In all, 51.3% (462/901) pregnant women were tested either at the health posts or by outreach teams and 48.7% (439/901) at the district healthcare center [44]. This finding indicates increased use and uptake of syphilis RSTs, HIV and HBV test though use of RSTs declined at some stages. This also demonstrates a gap in literature on the role of SCM for POC diagnostics use which requires further investigations to determine its effect on clients.
Use of CD4 diagnostics
Thairu et al. (2011) focused on describing lessons learned in providing CD4 diagnostics in Burkina Faso and Zimbabwe [50]. The study reported that, a total of 3287 CD4 tests were performed for 1558 patients enrolled in the programme in Burkina Faso with an average of two tests per patient (range: 1~10) [50]. In all, 60% of the patients had only one test at the initial stage of the programme but the frequency of repeated tests within 12 months as recommended by national guidelines varied from 59% at the baseline to 16% [50]. A total of 8990 tests were done on 6024 patients in Zimbabwe with an average of one test per patient (range: 1~4) [50]. This outcome demonstrates declined repeated CD4 testing due to poor test stock out.
Discussion
We conducted a systematic scoping review of studies to explore evidence on supply chain management of and accessibility to POC testing, focusing on availability and use of POC tests in LMICs. The results demonstrated limited published research on SCM of and accessibility to POC testing in LMICs. It also revealed stock-outs of HIV, syphilis, and malaria POC tests. This study findings further demonstrated limited use of malaria RDTs, blood pressure, diabetes, and dyslipidaemia assays, low testing of HBV, and low repeated CD4 testing due to test stock-outs.
Our study findings suggested quantification and forecasting, procurement, inventory management, distribution systems, quality management systems, and human resource capacity played a key role on the availability and use of POC test. Availability of adequate quality POC diagnostic tests essentially increases access to POC testing and improved healthcare. Despite this, evidence from this study showed weak procurement, inventory and stock management, and human resource capacity for SCM resulted in test stock-outs as well as, declined use of RST [47, 51, 54]. The study findings also showed significant stock-outs of malaria RDTs [43, 45, 48], HIV, CD4, HBV POC diagnostics kits [44, 46, 50, 55] at different study settings. This study findings additionally suggested limited use of various POC tests owing to test stock-outs at implementation sites. It is worthwhile to strengthen quantification and forecasting, procurement, inventory management, distribution systems, quality management systems, and human resource capacity to prevent test stock-outs, sustain POC testing services, and maximize the benefits of implementing POC testing programmes in LMICs.
The first WHO model list of essential in-vitro diagnostics (EDL) has been created [7]. The WHO further encourages countries to create national EDLs based on each country’s disease burden and epidemiology [7] to improve access to health care for all patients [44, 49, 51, 52, 56]. Adopting the WHO quality-ASSURED (Affordability, Sensitivity, Specificity, User friendly, Rapid and robust, Equipment free and Delivered) criteria for selection of POC diagnostics for rural and remote settings clinics [58–60] can potentially contribute to addressing SCM challenges to prevent POC test stock-outs and limited usage as evidenced in this study [43–48, 50, 51, 53–55]. All POC testing related services are introduced with the aim of improving health outcomes. For instance, syphilis among pregnant women is highly associated with increased still births [49, 51]. Hence, ensuring availability of syphilis POC tests through efficient SCM during antenatal care potentially could enable syphilis same-day testing and treatment for pregnant women and their partners [44, 49, 51]. Also, efficient SCM will enable availability and increase use of malaria POC tests hence, reduce syndromic management by clinician and prevent wrong treatment or overtreatment of patients related to syndromic management [13, 58, 61]. HIV testing also serves as a gateway to HIV/AIDS prevention, care, and treatment as well as other needed supportive health care interventions [44, 56, 62, 63]. In view of this, decentralizing HIV access to lower health facilities will help improve access to HIV testing and early initiation of management [52, 56]. Unlike, syphilis, malaria, HIV, and other POC diagnostic tests, CD4 count testing is aimed at improving the health outcomes of people living with HIV/AIDs by enabling the determination of clinical staging for the appropriate antiretroviral treatment [64–67]. Therefore, ensuring availability, use, and sustainability of HIV and CD4 testing diagnostic services in LMICs as evidenced in this study is a necessity [50].
Implications for practice
Majority of the studies reviewed were conducted in a rural setting where access to healthcare and laboratory infrastructure is either not available or poorly developed coupled with lack/inadequate skilled healthcare professional [43–45, 47–51]. This study finding indicates majority of the reviewed studies reported poor availability or stock out of test at the district and primary healthcare settings [43–48, 50–52, 54, 55]. This implies that rural populations including pregnant women and children will have to travel long distances to access diagnostic services. Long distances from rural communities to access laboratory services results in delays, long turnaround time, and failure of people to return for their results [56, 68]. Therefore, sustainability of POC diagnostic services in resource-limited settings and rural health facilities is crucial to improve health outcomes in rural communities [16]. Supply chain management measures such as increase production of POC tests to meet global demand, appropriate quantification and forecasting, strengthening procurement, adequate quality assurance/control, equitable distribution, inventory management; training, among others are highly essential to ensure sustainability of a POC diagnostic service.
Implications for research
Our study shows that there is limited published research specific to SCM for POC diagnostics in LMICs, indicating a gap in literature. Our study findings also have international implications since the included studies were from diverse different countries. We hope this study will prompt further studies to provide a contextual insight on SCM for POC diagnostics bearing in mind the need to improve access for POC diagnostics services in LMICs. We further recommend a study to determine the impact of POC test stock-outs on patient outcome.
Strengths and limitations
This scoping review possibly is the first comprehensive study to map evidence on SCM and accessibility to diagnostic services at POC in LMICs. This study demonstrated a substantial gap in literature on POC tests SCM to guide future research in LMICs. This study’s methodology also allowed the inclusion of different study designs and identification of relevant articles methodically, charting, and analysing the outcomes [21, 69]. The removal of date, language, and study design limitations as well as the comprehensive search for literature is an important strength of this study Despite this, it is possible research on POC tests SCM probably existed under different terminologies which were not captured in this review. Nonetheless, we included Medical Subject Heading terms to address this. Further analysis of included quantitative studies using meta-analysis could provide more information. However, the exploratory nature of scoping reviews does not involve meta-analysis for quantitative studies. Future studies could focus on meta-analysis. Although many other factors such as financial constraints, geographical barriers, and human resource capacity for POC testing also play a crucial role regarding access to POC testing [9, 12, 13], this study was limited to only SCM. We therefore recommend similar studies to investigate the role of other essential potential barriers in LMICs in future.
Conclusion
In conclusion, this study demonstrated limited published research on SCM of and accessibility to POC testing in LMICs. SCM play an essential role on the availability and use of POC tests as well as improved access to healthcare in resource-limited settings. Hence, it is worthwhile to consider SCM as a key component of POC diagnostic service implementation at the planning stages to ensure sustainability. We therefore, recommend primary studies aimed at investigating SCM of POC diagnostic tests in resource-limited settings to identify the barriers/challenges, and provide a context-specific evidence-based solutions for policy/decision makers, implementers, and POC developers, funders, and development partners.
Additional files
Electronic databases search results for title screening. (DOCX 14 kb)
Full articles screening results and output of degree of agreement in Stata Version 13. (DOCX 16 kb)
Acknowledgements
We would like to thank the following institutions: College of Health Sciences and Library services at the University of KwaZulu-Natal for their support in providing us with resources to help with setting up and conducting this study. The authors would also like to thank John Kutsukutsa for assisting with resolving discrepancies in reviewers’ responses at full article screening stage. We are also most grateful to Julius Nyerere for assisting with English editing. Last but not the least; we would like to thank staff of the Department of Public Health Medicine for their support in diverse ways.
Abbreviations
- AIDS
Acquired immuno-deficiency syndrome
- ASSURED
Affordability, Sensitivity, Specificity, User friendly, Rapid and robust, Equipment free, and Delivered
- CD4
T lymphocytes
- CHW
Community health workers
- EDL
List of essential in-vitro diagnostics
- HBV
Hepatitis b virus
- HIV
Human immune-deficiency virus
- LMICs
Low- and middle-income countries
- MMAT
Mixed method appraisal tool
- PICO
Population, intervention, comparison, and outcome
- POC
Point-of-care
- PRISMA
Preferred reporting items for systematic reviews and meta-Analyses
- PROSPERO
International prospective register of systematic reviews
- RDTs
Rapid diagnostic tests
- RSTs
Rapid syphilis tests
- SCM
Supply chain management
- VL
Viral load
- WHO
World Health Organization
Authors’ contributions
DK conceptualized and designed the study together with BV and TPM-T. DK, NG, TPM-T and BV contributed in the abstract, full article screening and the quality assessment of the included studies. TPM-T contributed in the synthesis of data and the design of the sifting and data extraction processes. DK prepared the first draft of the study and TPM-T, PD and BV critical reviewed the draft. DK prepared the final draft and all authors approved it. All authors read and approved the final manuscript.
Funding
This study was funded by the University of KwaZulu-Natal, College of Health Sciences Research Scholarship. The funder played no role in the data collection, analysis, interpretation, and the preparation of the manuscript.
Availability of data and materials
The data supporting the conclusions of this paper are available through the detailed reference list. No original datasets are presented, since this is a review of already existing literature.
Ethics approval and consent to participate
This paper is a systematic scoping study that relied strictly on the review of existing literature, no human participants were involved. Therefore, ethical approval and consent to participate by human participants was not applicable.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Desmond Kuupiel, Email: desmondkuupiel98@hotmail.com.
Vitalis Bawontuo, Email: bawontuovitalis@yahoo.com.
Paul K. Drain, Email: pkdrain@uw.edu
Nonjabulo Gwala, Email: nonjabulojoy@gmail.com.
Tivani P. Mashamba-Thompson, Email: Mashamba-Thompson@ukzn.ac.za
References
- 1.World Health Organization. Manual for procurement of diagnostics and related laboratory items and equipment: diagnostics and laboratory technology. Geneva; 2013.
- 2.Drain PK, et al. Evaluating diagnostic point-of-care tests in resource-limited settings. Lancet Infect Dis. 2015;14(3):239–249. doi: 10.1016/S1473-3099(13)70250-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Peeling RW. Diagnostics in a digital age: an opportunity to strengthen health systems and improve health outcomes. Int Health. 2015;7(6):384–389. doi: 10.1093/inthealth/ihv062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mashamba-Thompson, T.P., B. Sartorius, and P.K. Drain, Point-of-Care Diagnostics for Improving Maternal Health in South Africa. 2016. 3(sdg 3). [DOI] [PMC free article] [PubMed]
- 5.Peeling Rosanna W, McNerney Ruth. Emerging technologies in point-of-care molecular diagnostics for resource-limited settings. Expert Review of Molecular Diagnostics. 2014;14(5):525–534. doi: 10.1586/14737159.2014.915748. [DOI] [PubMed] [Google Scholar]
- 6.Kafkova J. Rapid diagnostic point of care tests in resource limited settings. Int J Infect Dis. 2016;45:56–57. doi: 10.1016/j.ijid.2016.02.169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization, World Health Organization Model List of Essential In Vitro Diagnostics First edition (2018). 2018, World Health Oraganization: Geneva.
- 8.Chandra C, Grabis J. Supply chain configuration: concepts, solutions, and applications: Springer Science & Business Media; 2007.
- 9.Kuupiel D, Bawontuo V, Mashamba-Thompson TP. Improving the accessibility and efficiency of point-of-care diagnostics Services in low-and Middle-Income Countries: lean and agile supply chain management. Diagnostics. 2017;7(4):58. doi: 10.3390/diagnostics7040058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Embrey MA, Health MSf. MDS-3: managing access to medicines and Health technologies: Kumarian Press; 2012.
- 11.Pinna Roberta, Carrus Pier Paolo, Marras Fabiana. Applications of Contemporary Management Approaches in Supply Chains. 2015. Emerging Trends in Healthcare Supply Chain Management — An Italian Experience. [Google Scholar]
- 12.Engel Nora, Wachter Keri, Pai Madhukar, Gallarda Jim, Boehme Catharina, Celentano Isabelle, Weintraub Rebecca. Addressing the challenges of diagnostics demand and supply: insights from an online global health discussion platform. BMJ Global Health. 2016;1(4):e000132. doi: 10.1136/bmjgh-2016-000132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fonjungo PN, et al. Access and quality of HIV-related point-of-care diagnostic testing in Global Health programs. Clin Infect Dis. 2016;62(3):369–374. doi: 10.1093/cid/civ866. [DOI] [PubMed] [Google Scholar]
- 14.Biza A, et al. Challenges and opportunities for implementing evidence-based antenatal care in Mozambique: a qualitative study. BMC Pregnancy Childbirth. 2015;15:200. doi: 10.1186/s12884-015-0625-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kuupiel, D., et al., Poor supply chain management and stock-outs of point-of-care diagnostic tests in Upper East Region’s primary healthcare clinics, Ghana. 2019. 14(2): e0211498. [DOI] [PMC free article] [PubMed]
- 16.Kuupiel D, et al. Empirical framework for point-of-care diagnostics supply chain Management for Accessibility and Sustainability of diagnostic Services in Ghana's primary Health care clinics. Point of Care. 2019;18(2):72–75. [Google Scholar]
- 17.Mashamba-Thompson TP, Sartorius B, Drain PK. Operational assessment of point-of-care diagnostics in rural primary healthcare clinics of KwaZulu-Natal, South Africa: a cross-sectional survey. BMC Health Serv Res. 2018;18(1):380. doi: 10.1186/s12913-018-3207-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kuupiel Desmond, Tlou Boikhutso, Bawontuo Vitalis, Mashamba-Thompson Tivani P. Accessibility of pregnancy-related point-of-care diagnostic tests for maternal healthcare in rural primary healthcare facilities in Northern Ghana: A cross-sectional survey. Heliyon. 2019;5(2):e01236. doi: 10.1016/j.heliyon.2019.e01236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kuupiel D, Adu KM, Bawontuo V, Mashamba-Thompson TP. Geographical Accessibility to District Hospitals/Medical Laboratories for Comprehensive Antenatal Point-of-Care Diagnostic Services in the Upper East Region, Ghana. EClinicalMedicine. 2019. [DOI] [PMC free article] [PubMed]
- 20.Roark DC. Managing the healthcare supply chain. Nurs Manag. 2005. [DOI] [PubMed]
- 21.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. [Google Scholar]
- 22.Moher, D., et al., PRISMA 2009 Flow Diagram. 2009. 6(2009): 1000097.
- 23.Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69. doi: 10.1186/1748-5908-5-69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kuupiel D, Drain P, Mashamba-Thompson TP. Supply chain management and efficiency of point-of-care diagnostics services in resource-limited settings: International Prospective Register of Systematic Reviews (PROSPERO); 2017.
- 25.The World Bank Group . World bank country and lending groups: country classification. 2017. [Google Scholar]
- 26.Pluye P, et al. Mixed methods appraisal tool (MMAT) version 2011, in Proposal: a mixed methods appraisal tool for systematic mixed studies reviews: McGill University, Department of Family Medicine; 2011.
- 27.Albert, H., et al., Development, roll-out and impact of Xpert MTB/RIF for tuberculosis: what lessons have we learnt and how can we do better? Eur Respir J, 2016: p. ERJ-00543-2016. [DOI] [PMC free article] [PubMed]
- 28.Bristow CC, et al. A review of recent advances in rapid point-of-care tests for syphilis. Sex Health. 2015;12(2):119–125. doi: 10.1071/SH14166. [DOI] [PubMed] [Google Scholar]
- 29.Fu E, et al. Perspective on diagnostics for Global Health. IEEE Pulse IEEE Pulse. 2011;2(6):40–50. doi: 10.1109/MPUL.2011.942766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Raja S, Bates J. Strengthening health systems: the role of supply chains in addressing the HIV epidemic. The Changing HIV/AIDS Landscape. 2009:411.
- 31.Annan J. Assessment of logistics management in Ghana health service. Int J Business Soc Res. 2013;3(8):75–87. [Google Scholar]
- 32.Atun R, et al. Health-system strengthening and tuberculosis control. Lancet. 2010;375(9732):2169–2178. doi: 10.1016/S0140-6736(10)60493-X. [DOI] [PubMed] [Google Scholar]
- 33.Baltacioglu T, et al. A new framework for service supply chains. Serv Ind J. 2007;27(2):105–124. doi: 10.1080/02642060601122629. [DOI] [Google Scholar]
- 34.Chege EN. Green supply chain management practices and supply chain performance of private hospitals in Nairobi, Kenya: University of Nairobi; 2012.
- 35.Jamieson David, Kellerman Scott E. The 90 90 90 strategy to end the HIV Pandemic by 2030: Can the supply chain handle it? Journal of the International AIDS Society. 2016;19(1):20917. doi: 10.7448/IAS.19.1.20917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Maltha J, Gillet P, Jacobs J. Malaria rapid diagnostic tests in endemic settings. CLM Clin Microbiol Infect. 2013;19(5):399–407. doi: 10.1111/1469-0691.12151. [DOI] [PubMed] [Google Scholar]
- 37.Piatek AS, et al. GeneXpert for TB diagnosis: planned and purposeful implementation. Global Health: Sci Prac. 2013;1(1):18–23. doi: 10.9745/GHSP-D-12-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Alemnji G, et al. The centrality of laboratory services in the HIV treatment and prevention cascade: the need for effective linkages and referrals in resource-limited settings. AIDS Patient Care STDs. 2014;28(5):268–273. doi: 10.1089/apc.2013.0356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Park PH, et al. Increasing access to the MDR-TB surveillance programme through a collaborative model in western Kenya. Trop Med Int Health: TM & IH. 2012;17(3):374–379. doi: 10.1111/j.1365-3156.2011.02933.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Peter TF, et al. The need for standardization in laboratory networks. Am J Clin Pathol. 2009;131(6):867–874. doi: 10.1309/AJCPCBMOHM7SM3PJ. [DOI] [PubMed] [Google Scholar]
- 41.Sinishaw MA, Gebregergs GB, Shiferaw MB. Distribution and availability of essential tuberculosis diagnostic items in Amhara region, Ethiopia. PLoS One. 2015;10(12):e0141032. doi: 10.1371/journal.pone.0141032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Williams J, et al. Progress in harmonizing tiered HIV laboratory systems: challenges and opportunities in 8 African countries. Global Health, Science And Practice. 2016;4(3):467–480. doi: 10.9745/GHSP-D-16-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Hamer DH, et al. Quality and safety of integrated community case management of malaria using rapid diagnostic tests and pneumonia by community health workers. Pathogens and Global Health. 2012;106(1):32–39. doi: 10.1179/1364859411Y.0000000042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Smith A, et al. Lessons learned from integrating simultaneous triple point-of-care screening for syphilis, hepatitis B, and HIV in prenatal services through rural outreach teams in Guatemala. Int J Gynecol Obstet. 2015;130(Supplement 1):S70–S72. doi: 10.1016/j.ijgo.2015.04.009. [DOI] [PubMed] [Google Scholar]
- 45.Kyabayinze DJ, et al. Parasite-based malaria diagnosis: are Health Systems in Uganda equipped enough to implement the policy? BMC Public Health. 2012;12(1):695. doi: 10.1186/1471-2458-12-695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Jaya Z, Drain PK, Mashamba-Thompson TP. Evaluating quality management systems for HIV rapid testing services in primary healthcare clinics in rural KwaZulu-Natal, South Africa. PLoS One. 2017;12(8):e0183044. doi: 10.1371/journal.pone.0183044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Bonawitz RE, et al. Assessment of the impact of rapid syphilis tests on syphilis screening and treatment of pregnant women in Zambia. Int J Gynaecol Obstet. 2015;130 Suppl 1:S58–S62. doi: 10.1016/j.ijgo.2015.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Hasselback L, et al. Rapid diagnostic test supply chain and consumption study in Cabo Delgado, Mozambique: estimating stock shortages and identifying drivers of stock-outs. Malar J. 2014;13(1):295. doi: 10.1186/1475-2875-13-295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Mabey DC, et al. Point-of-care tests to strengthen health systems and save newborn lives: the case of syphilis. PLoS Med. 2012;9(6):e1001233. doi: 10.1371/journal.pmed.1001233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Thairu L, Katzenstein D, Israelski D. Operational challenges in delivering CD4 diagnostics in sub-Saharan Africa. AIDS Care. 2011;23(7):814–821. doi: 10.1080/09540121.2010.541416. [DOI] [PubMed] [Google Scholar]
- 51.Ansbro ÉM, et al. Introduction of syphilis point-of-care tests, from pilot study to national programme implementation in Zambia: a qualitative study of healthcare workers’ perspectives on testing, training and quality assurance. PLoS One. 2015;10(6):e0127728. doi: 10.1371/journal.pone.0127728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Stevens W, et al. Feasibility of HIV point-of-care tests for resource-limited settings: challenges and solutions. BMC Med. 2014;12(1):173. doi: 10.1186/s12916-014-0173-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Shott JP, Galiwango RM, Reynolds SJ. A quality management approach to implementing point-of-care technologies for HIV diagnosis and monitoring in sub-Saharan Africa. J Trop Med. 2012;2012. [DOI] [PMC free article] [PubMed]
- 54.Peeling RW, Ronald A. Diagnostic challenges of sexually transmitted infections in resource-limited settings. Future Microbiol. 2009;4(10):1271–1282. doi: 10.2217/fmb.09.100. [DOI] [PubMed] [Google Scholar]
- 55.McGuire H, Weigl BH. Medical devices and diagnostics for cardiovascular diseases in low-resource settings. J Cardiovasc Transl Res. 2014;7(8):737–748. doi: 10.1007/s12265-014-9591-3. [DOI] [PubMed] [Google Scholar]
- 56.Alemnji G, Nkengasong JN, Parekh BS. HIV testing in developing countries: what is required? Indian J Med Res. 2011;134(6):779. doi: 10.4103/0971-5916.92625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Peeling R. Bringing diagnostics to developing countries: an interview with Rosanna Peeling. Expert Rev Mol Diagn. 2015;15(9):1107–1110. doi: 10.1586/14737159.2015.1081802. [DOI] [PubMed] [Google Scholar]
- 58.Peeling RW, et al. Rapid tests for sexually transmitted infections (STIs): the way forward. Sex Transm Infect. 2006;82(Suppl 5):v1–v6. doi: 10.1136/sti.2006.024265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Peeling RW, et al. Why do we need quality-assured diagnostic tests for sexually transmitted infections? Nat Rev Microbiol. 2006;4(12):S7. doi: 10.1038/nrmicro1569. [DOI] [PubMed] [Google Scholar]
- 60.Pai NP, et al. Point-of-care testing for infectious diseases: diversity, complexity, and barriers in low- and middle-income countries. PLoS Med. 2012;9(9):e1001306. doi: 10.1371/journal.pmed.1001306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.D'Acremont V, et al. Time to move from presumptive malaria treatment to laboratory-confirmed diagnosis and treatment in African children with fever. PLoS Med. 2009;6(1):e252. doi: 10.1371/journal.pmed.0050252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Kellerman SE, et al. HIV testing within at-risk populations in the United States and the reasons for seeking or avoiding HIV testing. J Acquir Immune Defic Syndr. 2002;31(2):202–210. doi: 10.1097/00126334-200210010-00011. [DOI] [PubMed] [Google Scholar]
- 63.Branson BM, et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR CDC Surveill Summ. 2006;55(14):1–CE-4. [PubMed] [Google Scholar]
- 64.Jani IV, et al. Effect of point-of-care CD4 cell count tests on retention of patients and rates of antiretroviral therapy initiation in primary health clinics: an observational cohort study. Lancet. 2011;378(9802):1572–1579. doi: 10.1016/S0140-6736(11)61052-0. [DOI] [PubMed] [Google Scholar]
- 65.Caldwell MB, et al. Revised classification system for human immunodeficiency virus infection in children less than 13 years of age. MMWR CDC Surveill Summ. 1994;1994:iii–i10. [Google Scholar]
- 66.Faal M, et al. Providing immediate CD4 count results at HIV testing improves ART initiation. J Acquir Immune Defic Syndr. 2011;58(3):e54–e59. doi: 10.1097/QAI.0b013e3182303921. [DOI] [PubMed] [Google Scholar]
- 67.Staszewski S, et al. Determinants of sustainable CD4 lymphocyte count increases in response to antiretroviral therapy. Aids. 1999;13(8):951–956. doi: 10.1097/00002030-199905280-00011. [DOI] [PubMed] [Google Scholar]
- 68.Kuupiel D, et al. Geographic accessibility to public health facilities providing tuberculosis testing services at point-of-care in the upper east region, Ghana. BMC Public Health. 2019;19(1):718. doi: 10.1186/s12889-019-7052-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Pham MT, et al. A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods. 2014;5(4):371–385. doi: 10.1002/jrsm.1123. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Electronic databases search results for title screening. (DOCX 14 kb)
Full articles screening results and output of degree of agreement in Stata Version 13. (DOCX 16 kb)
Data Availability Statement
The data supporting the conclusions of this paper are available through the detailed reference list. No original datasets are presented, since this is a review of already existing literature.