

INTRODUCTION
India is the second most populous country in the world with a population of 1.236 billion.[1] In this vast population, every fifth person is an adolescent between 10 and 19 years and every third person is aged between 10 and 24 years.[2] There are >434 million children and adolescents in India which is the highest in the world.[1] The country is expected to have 250 million working population by 2030 which can be termed as an enormous demographic dividend.[3] Such a working young population can be an asset for the country, contributing to the nation's growth and development. Such an advancement can be expected and provided the health of children and adolescents – both physical and mental are accorded priority in the policy arena. While the focus on infant and under-five mortalities, immunization, and nutrition have contributed to the overall improvement of physical health, little emphasis is given to the Child and Adolescent Mental Health (CAMH) in India.[4] In this article, we discuss the severity of CAMH disorders, existing measures to address the same and policy recommendations to improve the prevention of protection strategies for CAMH in India.
CURRENT STATUS OF CHILD AND ADOLESCENT MENTAL HEALTH IN INDIA
At any given point of time, nearly 50 million Indian children suffer from mental disorders, and this number will increase if the adolescent population is considered as well.[5] Wide variations in the prevalence of different CAMH disorders are found in the existing literature. A study conducted in Lucknow estimated the prevalence of child and adolescent mental disorders as 12.1%, whereas disease-specific prevalence was 4.16% for nocturnal enuresis, 2.38% for pica, 1.78% for conduct disorders, and 1.26% for developmental disorders.[6] The similar study conducted in Bangalore revealed an overall prevalence of 12.5% while the rate was 12.4% in rural areas, 10.8% in slums, and 13.9% (highest) in urban areas of the city. The prevalence was found to be different in rural and urban areas. Several studies conducted at community level reported the prevalence of child and adolescent mental disorders varying from 1.06% to 5.84% in rural areas, 0.8% to 29.4% in urban areas, and 12.5% to 16.5% in studies that were conducted in both rural and urban population.[7] It also varied from time to time in different studies. Investigations conducted in rural schools of Haryana and West Bengal have shown the prevalence of CAMH disorders as 20.7% and 33.33%, respectively.[7] In contrast, the prevalence found in the urban schoolchildren in Tamil Nadu and Chandigarh was 33.7% and 6.33%, respectively.[7] Apart from such studies, the National Mental Health Survey 2016 reported that the prevalence of mental disorders is 7.3% among children aged 13–17 years and it is similar in both genders.[8] The prevalence among urban children is nearly double (13.5%, 10.4–16.5, 95% CI) compared to the rural children (6.9%, 4.0–9.7, 95% CI). Major illnesses include depressive disorders (2.6%), agoraphobia (2.3 disabilities affecting intellectual status [1.7%]), autism spectrum disorders (1.6%), psychotic disorders (1.3%), and anxiety disorders (1.3%).[8] Moreover, the survey estimated the prevalence of depression as 6.9%, anxiety as 15.5%, tobacco as 7.6%, and alcohol consumption as 7.2% in a study conducted in Himachal state.[8] The survey reported that the real estimation of nationwide CAMH was beyond the scope of the survey. Furthermore, it is estimated that about 9.8 millions of Indian aged 13–17 years suffer from serious mental illness which would be greater in number if the entire age spectrum of childhood and adolescence is considered.[8] Another report published by the WHO showed that the prevalence of suicide is 21.1/100,000 population and nearly 258,075 Indians committed suicide in 2012 among which a large proportion are students aged 0–19 years.[9] Therefore, the impact of mental illness is far beyond the imagination of the society, in which the awareness about the severity of these diseases is the least. The economic burden of neuropsychiatric disorders outweighs other noncommunicable diseases and it can be as high as 4% of the gross national product (GNP) among which nearly 2% was accounted for treating mentally ill people.[10] The indirect cost of mental illness would include the time given by the caregivers, lost economic opportunities of the patients as well as caregivers due to the illness and many other factors- which implies a greater burden than the direct cost of the treatment itself.[10] Such high economic burden due to CAMH disorders cannot be overlooked considering the size of the population at risk and the potential benefits of timely intervention to address mental illness among children and adolescents across India.
EXISTING POLICIES, PROGRAMS, AND SERVICES FOR CHILD AND ADOLESCENT MENTAL HEALTH IN INDIA
Despite such severity and magnitude of CAMH disorders, India has no comprehensive CAMH policy for the huge population of >435 million children and adolescents.[7] Establishment of the first child guidance clinic in 1937 and Indian Council for Mental Hygiene was established in the 1940s and can be described as earlier efforts to address CAMH problems in India.[11] Till the 1980s, there were 120 child guidance clinics in India, which were operated by 400 caregivers.[12] From 1991 to 1995, national authorities of medical sciences increasingly participated in the development of the academic area of CAMH and CMEs as well as fellowships in child and adolescent psychiatry were held.[12] Moreover, India has adopted several national policies for different areas of child development, which include the National Policy for Children (1974), National Policy on Education (1986) and Labor (1987), Mental Health Act (1987), National Nutrition Policy (1993), National Trust for Welfare of Persons with Autism, Cerebral Palsy, Mental Retardation and Multiple Disability Act 1999, Charter for Children (2004), and National Plan of Action for Children (2005), but none of these adopted CAMH as a policy thrust.[5] The National Health Policy (2002, 2016) and the National Mental Health Policy (2014) provided little emphasis on the mental illness among the young population.[13] In the state level, most states lack an explicit policy on CAMH except Kerala which adopted an intent to improve mental health in the young population.[14] However, some programs, such as the National Mental Health Program and District Mental Health Program, are providing basic psychiatric care to the population in general without special emphasis on CAMH.[15] Other initiatives such as school health program, teacher's orientation program, student enrichment program, and school-based campaigns are done by NIMHANS which aims to increase awareness about psychosocial disorders, understand self, and improve interpersonal relationships with peers and teachers. In addition, few other small-to-medium scale initiatives were taken by autonomous and nonprofit agencies in Bangalore, Delhi, Mumbai, and many other cities across India.[16] Such school-based programs are mostly clustered in urban areas and mostly they run for a short duration.[16] Furthermore, the issue of mental health was also recognized as one of the six strategic priorities of national adolescent health strategy named Rashtriya Kishor Swasthya Karyakram (RKSK).[17] This initiative was conceptualized by the Government of India in 2014 and planned to be implemented by the State Government through the National Health Mission. Along with other activities such as improving nutrition and reproductive health, the program introduced peer counseling at school and community levels. This program is a landmark to improve overall adolescent health at the national level, but it has several limitations to address the mental health issues.[17] First, mental health is considered as one of the components within the multipronged program, not perceived as the prime concern. Second, the target population itself aims to reach only the adolescents aged 10–19 years, and the peer educators are selected from 15 to 19 years' age group. Therefore, the children in 0–10 years' age remain beyond the reach of the counseling services. Third, this program aims to raise awareness about mental health and substance abuse without a holistic approach to provide clinical and psychological support to those who need the same. Although this initiative aims to improve overall adolescent health, it seems to be inadequate to address the mental health epidemic in child and adolescent population in India.
PERSISTENT GAP IN MENTAL HEALTH CARE AFFECTS CHILDREN AND ADOLESCENTS
It is noteworthy that people of all ages in India who suffer from mental health do not have access to quality care. The treatment gap in mental health is about 50%–60% for schizophrenia, 88% for depression, 97.2% for substance abuse, and 22%–95% for seizure disorders.[8] The treatment gap for common mental disorders is 95% which is higher than the gap in severe disorders which is 76%.[8] Another critical issue for mental health is the patterns of how health services are being utilized by the population. Several factors such as median duration of mental illness, delay in seeking care from the time of onset, choice of providers, distance from the health center, and the number of visits to the service provider further contribute to this issue. Previous studies have reported a median duration of depressive disorders as 36 months which is about 72 months for diseases such as bipolar disorder.[8] Further, the median number of visits to the service providers was 2, ranging from 1 to 30. In 4%–50% of cases, the preferred provider was based on the government institutions.[8] These data are collected from the general population in all age groups. There was no significant evidence of these patterns estimated in child and adolescent population, which is a limitation of the existing evidence. However, due to underreporting of the cases, these gaps are likely to be wider among children and adolescents in India.[18] It is estimated that <1% of the children and adolescents suffering from mental disorders receive treatment.[5] Moreover, there are several critical disorders including learning, speech, visual, hearing, and personality disorders that require multispecialty care which is not available and accessible even in urban areas. Furthermore, very little attention has been given to the special population such as orphans, street children, juvenile homes, rescue homes, and many other places where children and adolescents are exposed to the higher risk of mental illness.[19]
POLICY DEVELOPMENT FOR IMPROVING CHILD AND ADOLESCENT MENTAL HEALTH IN INDIA
India lacks a robust policy for CAMH to avert the health-care expenditure and realize the demographic dividend; this young population can yield in their adulthood. It is the need of the hour to acknowledge this gap and set CAMH as a priority to ensure the future prospects of the country which has the largest population of children and adolescents in the world. Developing a CAMH policy which would sustain over time and bring desired results following implementation requires strong motivation of key stakeholders and a scientific basis to translate that motivation to policy actions. Based on an extensive review of policy analytical methods and evidence, we recommend a framework given in Figure 1 which can be used to develop CAMH policy in India. The framework and allied components are adopted from the Centers for Disease Control and Prevention Guidelines[20] and WHO's CAMH policy and plan framework.[21]
Figure 1.
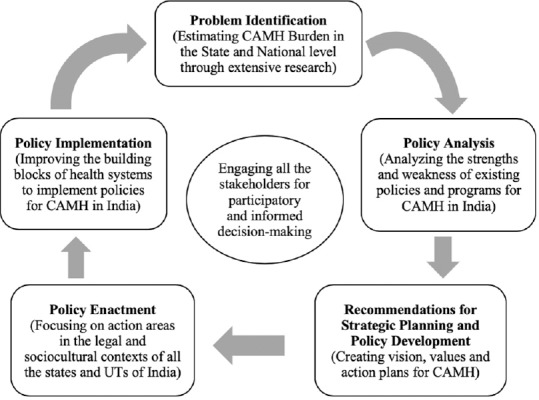
A framework to create, analyze, and implement child and adolescent mental health policy in India
Starting from identifying the mental health burden, the policy-makers should evaluate the current health policies and programs to find the scope of CAMH. These findings can be useful to create a comprehensive CAMH policy adopting the vision and values of the stakeholders. In a country like India, cultural diversity and social connections are very important; therefore, such values can provide valuable directions for policy development.[22] The values for policy development should be identified thoroughly from the perspectives of each player of the policy dynamics. Further, the values must be translated to the principles of the policy. Adopting the guidelines of the WHO, several principles can be included in the CAMH policy in India – (a) development of specific mental health care for children and adolescents, (b) integration of CAMH services in primary health care, (c) ensure availability and accessibility of necessary services and resources in both urban and rural areas for equitable distribution of care, (d) reduction of the risk factors and promotion of the protective factors for CAMH, (e) the environment within and outside the residence/school should be friendly for the optimum development of the children and adolescents, and (f) involve the children and adolescents individually and collectively in making the decisions regarding programs or plans for CAMH.[21] Once the principles are enumerated, the policy-makers must determine the potential areas for action. According to the suggested framework of the WHO, the key areas for CAMH are financing, legislation, policy advocacy, mental health information systems, research on CAMH, quality improvement, the organization of the services, and developing resources for CAMH and intersectoral collaboration.[21] While each of these areas should be strengthened to improve CAMH, it is equally important to understand the barriers of policy development and utilization of services to eliminate them for better progress of CAMH. There is primarily a lack of awareness which also results in social stigma for mental health – one of the biggest barriers in this regard.[23] The families and communities have a greater role in bringing the affected children to the needful treatment, but in every level of the society, mental health is a stigmatized issue to be acknowledged. This phenomenon leads to underreported cases as well as delayed reporting of severe mental disorders, which causes severe impairment of mental health status.[23] Next, the lack of required resources is another obstacle to achieve the optimum mental health.[24,25] These resources include trained professionals, financial provisions for mental health, and sufficient facilities providing mental care to the child and adolescent population. The mental health, in general, suffers from a lack of resources even in the developed countries which becomes worse in developing countries like India. The WHO has identified such scarcity of resources as a significant challenge to develop further resources such as trained human resources within the health system.[24] Further, the distance between the affected individual and health facilities offering mental health services is a barrier in India as the health facilities are not the same in rural and urban areas.[24,26,27] Almost 68.84% population reside in rural areas and their health cannot be underestimated.[2] Availability of health facilities and mental health practitioners in those facilities is critical to delivering mental health services in rural areas. From the systems perspective, one of the most important barriers to develop CAMH policies and programs is the absence of mental health from the mainstream health policy. Although India has a mental health policy, the provisions of mental health care for the children and adolescents are the least discussed in the policy documentation.[8] Moreover, only 0.06% of the total national health budget is allocated to mental health, which is even lower than the average mental health budget in low-income countries.[28] A comparison of mental health budgets in India at the global context is illustrated in Figure 2.[28]
Figure 2.
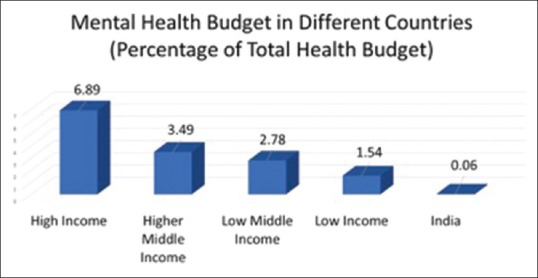
Percentage of the mental health budget within the total health budget in different countries
Further, a smaller portion of that tiny mental health budget is allocated to CAMH-related programs and services. Therefore, a lack of will at policy levels in both state and national stakeholders is affecting the overall development of CAMH in India.[12] Another significant barrier is the organization of mental health services within the health system.[29] In India, the existing mental health services are largely centralized, and the links between community demands and central health services are very poor. This condition was not addressed in several health system reforms over the past 70 years.[12] Moreover, funding and other supports are required to be reallocated to the thrust areas such as CAMH to improve the mental health outcomes. The distribution of mental health services in public and private sectors is not adequately managed, and there is a substantial lack of partnerships among these stakeholders to combat the CAMH catastrophes in India.[5] The next barrier in systems' perspective is the absence of mental health services in primary health-care facilities.[30] The Alma-Ata Declaration was instrumental in enabling the attainment of massive reform of the health system for delivering the essential health services in the community level which have the potential to treat the patients at lower cost and promote CAMH across the nation. Last but not least, the lack of public health leadership in mental health is a barrier to improve the CAMH in India.[31] Although the focus of public health approaches has shifted to noncommunicable diseases due to the epidemiological transitions, mental health remained neglected and it suffers from lack of sufficient efforts to assess and address mental health issues at the population level, particularly of the child and adolescent population from whom maximum benefits of the interventions can be yielded. The absence of the proactive role of the public health community in the development of mental health policies and programs focused on children and adolescents has acted as another major barrier. All these issues contribute to the status of mental health and allied services; therefore, these should be addressed while developing CAMH policy at state and national level ensuring the participation of all the stakeholders including the policy-makers, researchers, practitioners, and the patients as well as their caregivers.
CONCLUSION
Since its independence from England in 1947, India has achieved significant successes in many health indicators, but very fewer efforts are taken to ensure the intellectual and spiritual well-being of the young population who are the future representatives of the nation. The very high magnitude of mental disorders among the children and adolescent in India is alarming for the future. The economic burden of this ignorance includes the cost of treatment and the loss of potential opportunities that could be achieved if the child and adolescent population could grow in a healthier condition. Till now, the magnitude of diseases, socioeconomic significance, and gaps in the health system for CAMH are least discussed in the existing national policies and programs in India. There are well-documented challenges and barriers which can be minimized with a proactive, comprehensive, integrated, and multisectoral approach. A well-structured policy for CAMH can serve as the foundation of the future initiatives to understand critical problems related to CAMH, address the issues with a stewardship approach, and create an enabling environment enforcing positive mental health. Last but not the least, it is essential to recognize the importance of developing strong human capital for a prosperous future of the nation and establish a national vision for the prevention of mental disorders and promotion of mental well-being among the child and adolescent population in India.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We acknowledge our sincere gratitude to Professor Dr. SD Gupta, Chairman, IIHMR University and Adjunct Professor, Johns Hopkins Bloomberg School of Public Health, for his continued support and encouragement to our scholastic pursuits in mental health research in the context of India.
REFERENCES
- 1.United Nations International Children's Emergency Fund. India: Information by Country. United Nations International Children's Emergency Fund; 2013. [Last accessed on 2018 Dec 11]. Available from: https://www.unicef.org/infobycountry/india_statistics.html . [Google Scholar]
- 2.Census of India. 2011. [Last accessed on 2018 Dec 11]. Available from: http://www.censusindia.gov.in/2011-prov-results/paper2/data_files/india/Rural_Urban_2011.pdf .
- 3.Thomson Reuters. India's Demographic Dividend: A Beacon of Economic Hope. 2016. [Last accessed on 2018 Dec 11]. Available from: https://www.blogs.thomsonreuters.com/answerson/indias-demographic-dividend .
- 4.Ministry of Health and Family Welfare, Government of India. Burden of Disease in India. 2005. [Last accessed on 2018 Dec 11]. Available from: http://www.who.int/macrohealth/action/NCMH_Burdenofdisease_(29Sep2005).pdf .
- 5.Shastri PC. Promotion and prevention in child mental health. Indian J Psychiatry. 2009;51:88–95. doi: 10.4103/0019-5545.49447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Srinath S, Girimaji SC, Gururaj G, Seshadri S, Subbakrishna DK, Bhola P, et al. Epidemiological study of child & adolescent psychiatric disorders in urban & rural areas of Bangalore, India. Indian J Med Res. 2005;122:67–79. [PubMed] [Google Scholar]
- 7.Malhotra S, Patra BN. Prevalence of child and adolescent psychiatric disorders in India: A systematic review and meta-analysis. Child Adolesc Psychiatry Ment Health. 2014;8:22. doi: 10.1186/1753-2000-8-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ministry of Health and Family Welfare, Government of India. National Mental Health Survey of India; 2016. [Last accessed on 2018 Dec 11]. Available from: http://www.indianmhs.nimhans.ac.in/Docs/Summary.pdf . [Google Scholar]
- 9.World Health Organization. Preventing Suicide: A global Imperative. 2012. [Last accessed on 2018 Dec 11]. Available from: https://www.who.int/mental_health/suicide-prevention/world_report_2014/en .
- 10.World Health Organization. Investing in Mental Health. 2003. [Last accessed on 2018 Dec 11]. Available from: http://www.who.int/mental_health/media/investing_mnh.pdf .
- 11.Parkar SR, Dawani VS, Apte JS. History of psychiatry in India. J Postgrad Med. 2001;47:73–6. [PubMed] [Google Scholar]
- 12.Malhotra S. Child and adolescent psychiatry in India: Slow beginnings and rapid growth. Ment Health Indian Perspect. 2004. pp. 244–9. Available from: https://mhpolicy.files.wordpress.com/2011/05/mental-health-e-book_published10oct20041.pdf .
- 13.Ministry of Health and Family Welfare, Government of India. New Pathways New Hope: National Mental Health Policy of India. 2014. [Last accessed on 2018 Dec 11]. Available from: https://www.nhp.gov.in/sites/default/files/pdf/national mental health policy of India 2014.pdf .
- 14.Health and Family Welfare Department, Government of Kerala. 2013. [Last accessed on 2018 Dec 11]. Available from: https://www.kerala.gov.in/documents/10180/46696/Health%20Policy%202013 .
- 15.Murthy RS. Mental health programme in the 11th five year plan. Indian J Med Res. 2007;125:707–11. [PubMed] [Google Scholar]
- 16.Kishore Kumar D, Mukesh Y. Clinical Practice Guidelines for School Mental Health Program. 2017. [Last accessed on 2018 Dec 11]. pp. 307–21. Available from: http://www.indianjpsychiatry.org/cpg/cpg2008/CPG-CAP_14.pdf .
- 17.Ministry of Health and Family Welfare, Government of India. Rashtriya Kishor Swasthya Karyakram RKSK Guidelines. 2015. [Last accessed on 2018 Dec 11]. Available from: http://www.nhm.gov.in/nhm/nrhm/guidelines/nrhm-guidelines/arsh.html .
- 18.Saporito JM, Ryan C, Teachman BA. Reducing stigma toward seeking mental health treatment among adolescents. Stigma Res Action. 2011;1:9–21. [PMC free article] [PubMed] [Google Scholar]
- 19.Vostanis P. Mental health services for children in public care and other vulnerable groups: Implications for international collaboration. Clin Child Psychol Psychiatry. 2010;15:555–71. doi: 10.1177/1359104510377715. [DOI] [PubMed] [Google Scholar]
- 20.Center for Disease Control and Prevention. CDC's Policy Analytical Framework. 2015. [Last accessed on 2018 Dec 11]. Available from: https://www.cdc.gov/policy/analysis/process/analysis.html .
- 21.World Health Organization. Child and adolescent mental health policies and plans. [Last accessed on 2018 Dec 11];Ment Health Policy Serv Guide Packag. 2005 1:1–64. Available from: http://www.who.int/mental_health/policy/Childado_mh_module.pdf . [Google Scholar]
- 22.Snoeren F, Hoefnagels C, Evers SM, Lamers-Winkelman F. Design of a prospective study on mental health and quality of life of maltreated children (aged 5-16 years) after a report to an advice and reporting center on child abuse and neglect. BMC Public Health. 2013;13:942. doi: 10.1186/1471-2458-13-942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shidhaye R, Kermode M. Stigma and discrimination as a barrier to mental health service utilization in India. Int Health. 2013;5:6–8. doi: 10.1093/inthealth/ihs011. [DOI] [PubMed] [Google Scholar]
- 24.World Health Organization. Caring for Children and Adolescents with Mental Disorders Setting WHO Directions. World Health Organization; 2003. [Last accessed on 2018 Dec 11]. Available from: http://www.who.int/mental_health/media/en/785.pdf . [Google Scholar]
- 25.United for Sight. Barriers to Mental Health Care. United for Sight. 2015. [Last accessed on 2018 Dec 11]. Available from: http://www.uniteforsight.org/mental-health/module6 .
- 26.Harrison R. Distance as a Barrier to Child and Adolescent Mental Health Service Access in Post-Katrina Orleans Parish. 2008. [Last accessed on 2018 Dec 11]. Available from: http://www.digitalcommons.lsu.edu/gradschool_theses/3113 .
- 27.Reddy SK, Thirthalli J, Channaveerachari NK, Reddy KN, Ramareddy RN, Rawat VS, et al. Factors influencing access to psychiatric treatment in persons with schizophrenia: A qualitative study in a rural community. Indian J Psychiatry. 2014;56:54–60. doi: 10.4103/0019-5545.124714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.World Health Organization. India: Mental Health Atlas. World Health Organization; 2011. [Last accessed on 2018 Dec 11]. pp. 1–4. Available from: http://www.who.int/mental_health/evidence/atlas/profiles/ind_mh_profile.pdf . [Google Scholar]
- 29.Simpson EL, House AO. Involving users in the delivery and evaluation of mental health services: Systematic review. BMJ. 2002;325:1265. doi: 10.1136/bmj.325.7375.1265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.van Ginneken N, Jain S, Patel V, Berridge V. The development of mental health services within primary care in India: Learning from oral history. Int J Ment Health Syst. 2014;8:30. doi: 10.1186/1752-4458-8-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Srivastava K, Chatterjee K, Bhat PS. Mental health awareness: The Indian scenario. Ind Psychiatry J. 2016;25:131–4. doi: 10.4103/ipj.ipj_45_17. [DOI] [PMC free article] [PubMed] [Google Scholar]