

A 76-year-old woman with a history of intrahepatic cholangiocarcinoma (ICC) presented to the clinic for persistent epigastric abdominal pain. Her treatment for ICC consisted of systemic chemotherapy and liver-directed therapy with transcatheter arterial chemoembolization and yttrium-90 (Y-90) delivery. She had no history of Helicobacter pylori infection, nonsteroidal anti-inflammatory drug (NSAID) use, melena, hematemesis, or bright red blood per rectum. She was initially treated with oral proton pump inhibitor therapy with esomeprazole 40 mg daily and did not respond. Esophagogastroduodenoscopy revealed erythematous mucosa in the prepyloric region, 2 nonbleeding superficial ulcers with clean bases in the duodenal bulb, and diffuse mildly erythematous mucosa without active bleeding in the second part of the duodenum (Figure 1). Biopsies of the duodenal ulcers demonstrated chronic duodenitis with reactive changes and presence of a foreign material in the lamina propria of the duodenal bulb and second part of the duodenum (Figures 2 and 3).
Figure 1.
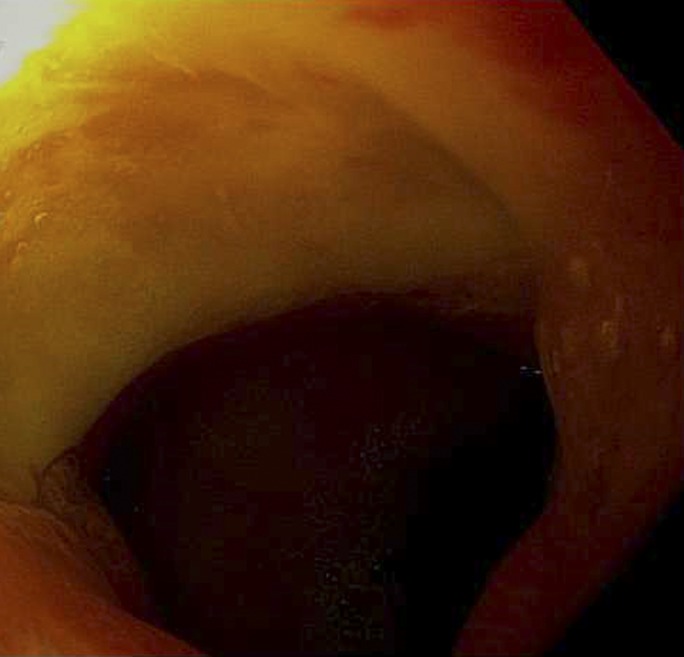
Esophagogastroduodenoscopy showing a nonbleeding superficial duodenal ulcer (10 mm) with no stigmata of bleeding in the duodenal bulb.
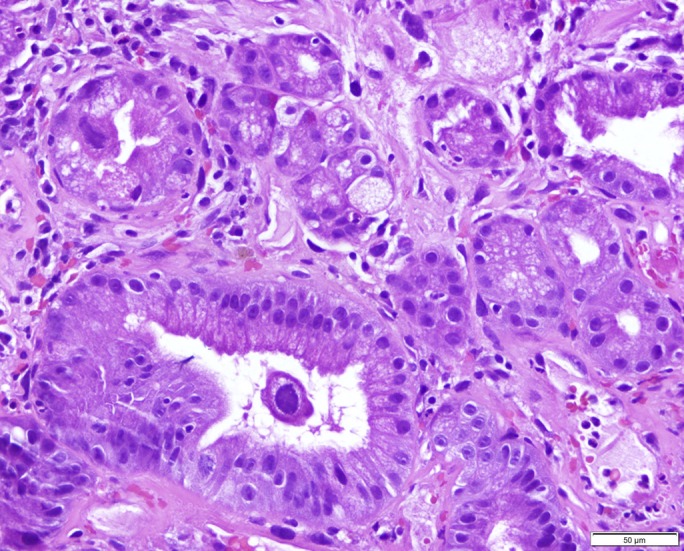
Figure 2.

Biopsies of the duodenal bulb ulcers showing (A) active chronic duodenitis with ulceration, marked reactive atypia, and few Y-90 beads in the lamina propria (arrow) with frank necrosis in the adjacent fragment, and (B) active chronic duodenitis with ulceration, marked reactive atypia, and few Y-90 beads (arrow) in the lamina propria.
Figure 3.
Biopsy of the duodenal erythema showing chronic duodenitis with reactive changes and absence of Y-90 beads but marked cytopathic changes in the epithelium.
The patient was diagnosed with duodenal ulceration as a complication of Y-90 microsphere radioembolization (RE). Two months before her onset of abdominal pain, she had received Y-90 targeted to the left lobe, with the intent to shrink the tumor before resection. The radiology team densely packed the gastroduodenal artery with coils with repeat angiogram of the gastroduodenal artery demonstrating complete stasis of blood flow. The left hepatic artery was then subselectively accessed with a microcatheter to deploy the Y-90 microspheres. These radioactive substances are delivered transarterially to hypervascular tumor-bearing areas where they emit low-penetration, high-energy radiation to tumors. The liver parenchyma is primarily supplied by the portal system; however, most hepatic tumors are supplied by the hepatic artery. The microspheres are selectively injected into the hepatic arterial circulation directed at the tumor's microvasculature.1 The foreign material seen and labeled in Figures 2 and 3 are the Y-90 beads embedded in the mucosa. The differential for contributors to endoscopically confirmed duodenal ulcers is broad, including H. pylori, NSAIDs, and viral infections. The patient was diagnosed with duodenal ulceration as a complication of Y-90 microsphere RE because the Y-90 beads were found embedded in the mucosa of the ulcer, she was not using NSAIDs, and pathology did not identify H. pylori in the gastric mucosa or viral cytopathologic changes such as macrophage aggregates, prominent mononuclear infiltrate, or viral inclusions. This case is unique because of its delayed presentation of the duodenal ulceration.
Y-90 microsphere RE can be an effective regional treatment for primary hepatobiliary malignancies and has been described as safe for patients with ICC2; however, side effects are not widely established, and gastrointestinal ulceration is a rarely reported complication of Y-90 microsphere RE.1 This is likely as a result of undesired flow of the microspheres through an aberrant hepatic arterial vasculature supplying the stomach and duodenum with resultant radiation damage to the mucosa.1 Most complications are caused by radiation injury from nontargeted embolization, such as ischemia from the embolization itself.3 Other vascular injuries that can occur include dissection and hematoma.4 The patient was treated with a trial of proton pump inhibitor by mouth twice a day, achieving a favorable response without the need for further endoscopies.
Author contributions: DJ Estes and GA Wideroff acquired the data and wrote the manuscript. MA Sendzischew Shane and DA Sussman wrote and revised the manuscript. D. Sussman is the article guarantor. Each author has approved the final draft submitted.
Acknowledgments: The authors give special thanks to Dr. Shree Venkat for her involvement and support in this case.
Financial disclosure: None to report.
Previous Presentation: This case report was presented as a poster at the ACG Annual Scientific Meeting; Orlando, Florida; October 16–18, 2017.
Informed consent was obtained for this case report.
REFERENCES
- 1.South CD, Meyer MM, Meis G, et al. Yttrium-90 microsphere induced gastrointestinal tract ulceration. World J Surg Oncol. 2008;6:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mouli S, Memon K, Baker T, et al. Yttrium-90 radioembolization for intrahepatic cholangiocarcinoma: Safety, response, and survival analysis. J Vasc Interv Radiol. 2013;24(8):1227–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jia Z, Wang W. Yttrium-90 radioembolization for unresectable metastatic neuroendocrine liver tumor: A systematic review. Eur J Radiol . 2018;100:23–9. [DOI] [PubMed] [Google Scholar]
- 4.Riaz A, Awais R, Salem R. Side effects of yttrium-90 radioembolization. Front Oncol . 2014;4:198. [DOI] [PMC free article] [PubMed] [Google Scholar]