

Abstract
Introduction Laryngeal granulomas are benign, recurrent lesions of many causes (reflux, voice abuse, intubation, and idiopathic), which renders its treatment difficult.
Objective To describe our experience in the treatment of laryngeal granulomas.
Methods From 16 medical records of the patients with laryngeal granulomas seen between 2010 and 2017 in a university hospital, the following data were analyzed: age, gender, vocal and gastroesophageal symptoms, vocal overuse, intubation, treatments, videolaryngoscopy before and after the treatment.
Results Gender: female, 10; male, 6. Age: between 20 and 60 years old (11). Etiology of the granulomas: intubation (9), reflux (4), idiopathic (3). The initial treatments adopted in all cases were: inhaled beclomethasone dipropionate 100 µg 12/12 hours (1 month), proton pump inhibitor, omeprazole 40 mg/day (2 months), and dietary and voice education. After this period, 10 patients (7 postintubation, 3 idiopathic) were submitted to surgery, since no improvements in the symptoms or in the lesions were seen. Of these, two recurred, requiring a second surgery, one of which recurred six times and received botulinum toxin A. Only one patient with granulomas due to laryngopharyngeal reflux presented no improvement in the symptoms nor in the lesion after the pharmacological treatment and had been submitted to microsurgery. All of the other patients with reflux granulomas were successfully treated with the drug treatment, and the longest treatment time for complete remission of the symptoms and of the lesions was 9 months.
Conclusions In laryngeal granulomas caused by reflux, treatment with inhaled steroids and proton pump inhibitors proved to be effective, although prolonged. In postintubation and idiopathic granulomas, surgery was the best treatment.
Keywords: granuloma, larynx, intubation, treatment
Introduction
Laryngeal granulomas are rounded, benign lesions positioned in the posterior glottis 1 ( Fig. 1 ). Vocal granulomas affect both genders and have many etiologies. 2 3 Among the most common causes are acid laryngitis secondary to laryngopharyngeal reflux disease, vocal overuse, and traumatic or prolonged intubation. 3
Fig. 1.
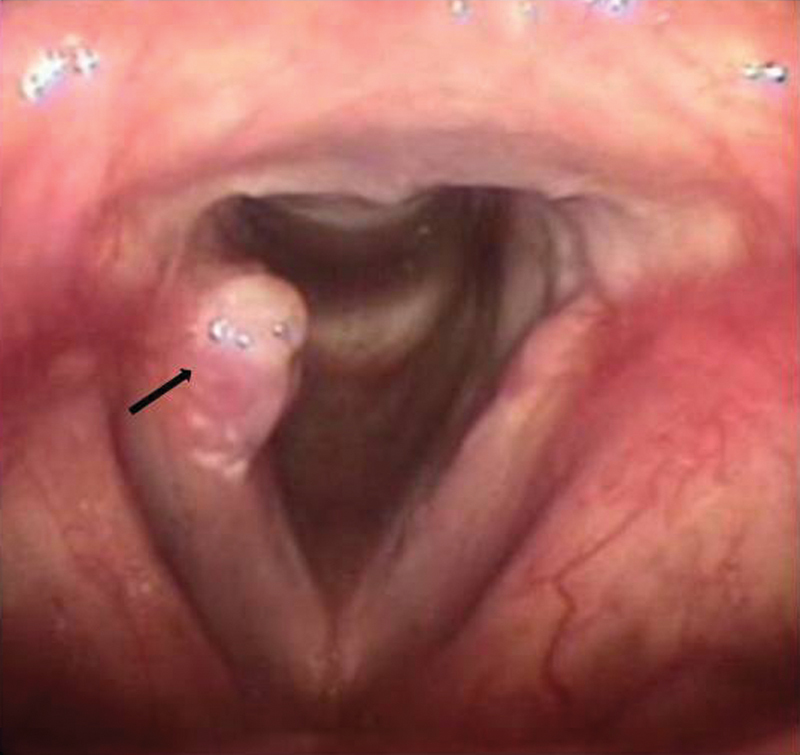
Laryngeal granuloma in the right vocal fold (arrow).
Patients with laryngeal granulomas may be asymptomatic or present with dysphonia of varying degrees, discomfort at the level of the throat, and dyspnea, in the presence of bulky lesions. Many laryngeal granulomas are considered idiopathic, making the treatment difficult. There is no consensus for the treatment of granulomas; however, most often it begins with pharmacological treatment, which includes proton pump inhibitors 4 and possible association with systemic or inhaled corticosteroids. 5 In all cases, antireflux diet education should be provided. Surgery is indicated after failure of the pharmacological treatment and relapse. 6 7 8 9
Voice education is also important in patients with laryngeal granulomas, since voice abuse may make reabsorption dificult. In contact granulomas due to voice abuse, some authors have demonstrated up to 77% of success using botulinum toxin associated with voice therapy. 10
Intubation granulomas are an inflammatory response to endotracheal tube contact. In most cases, they develop in patients with prolonged intubation, but can be diagnosed in patients who underwent short intubation periods, even of a few hours. In intubation granulomas, surgical indication is also reserved for cases of failure of the pharmacological treatment.
The lack of consensus for intubation granulomas reinforces the importance of further studies. In the present study, we describe our experience in the treatment of laryngeal granulomas in order to share it with other specialists.
Methods
The present study was approved by the Internal Review Board of our University. The medical records of the Outpatients Clinic of Voice Disorders of our Hospital were examined to select patients with the diagnosis of laryngeal granuloma seen between 2010 and 2017. The following data were extracted from the records: age, gender, vocal symptoms, gastroesophageal symptoms, vocal overuse, intubation, treatments, and videolaryngoscopy findings before and after treatment. Incomplete records or those of patients who did not undergo a follow-up videolaryngoscopy were excluded from the study.
All of the selected patients had been examined by the same medical team, using a 8 mm in diameter, 70°C rigid laryngeal telescope (Asap - Germany) or a 3.6 mm flexible nasofibroscope (Olympus, Tokyo, Japan), coupled to a ILO ELECTRONIC XE-50 - Eco V 50W X-TFT/USB multifunctional videolaryngoscopy image capture system (Carl Zeiss AG, Oberkochen, Germany) and to a professional lapel microphone (Leson, Osasco, SP, Brazil).
We have classified the granulomas according to their etiology into four types: postintubation, secondary to laryngopharyngeal reflux, secondary to phonotrauma, and idiopathic.
Results
During the study period, 21 patients with the diagnosis of laryngeal granuloma were identified; however, only 16 had complete data (10 females and 6 males). The highest concentration of patients was between 21 and 40 years old ( Fig. 2 ) The youngest and oldest patients were 8 and 61 years old, respectively. The etiological diagnoses were: postintubation (n = 9), laryngopharyngeal reflux (n = 4), and idiopathic (n = 3). Among the patients diagnosed with intubation granulomas, 7 had been intubated for > 10 days, and 2 for only a few hours.
Fig. 2.
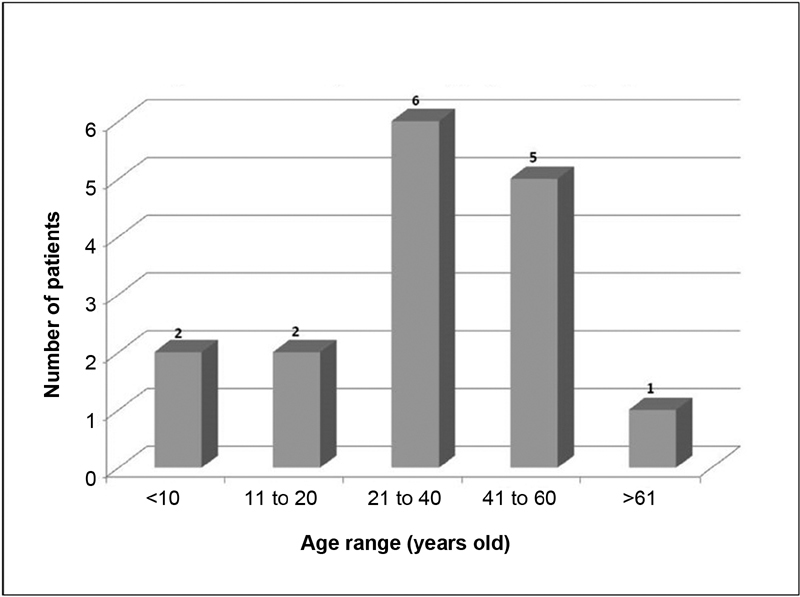
Distribution of the patients with laryngeal granulomas in age range.
Regardless of the etiology, the initial treatment recommended in all of the cases was pharmacological, with inhaled steroids (beclomethasone dipropionate 100 µg every 12 hours, for 1 month) and proton pump inhibitor (omeprazole 40 mg/day for 2 to 3 months). After the pharmacological treatment, patients with intubation or idiopathic granulomas who did not present any improvement in the symptoms and/or in the dimensions of the initial lesion underwent surgical removal ( Table 1 ). In these cases, the proton pump inhibitor was maintained postoperatively until the lesion disappeared. Of these, two patients with idiopathic granulomas presented recurrences, one of which recurred six times, receiving complementary treatment with intraoperative botulinum toxin A. There were no recurrences after this adjuvant treatment.
Table 1. Effectiveness of the pharmacological treatment according to the etiology of the granuloma.
| Etiology of the granuloma | Effectiveness of the pharmacological treatment according to the etiology of the granuloma. N % |
|
|---|---|---|
| Postintubation | 2/9 | 22.2 |
| Pharyngolaryngeal reflux | 3/4 | 75.0 |
| Idiopathic | 0/3 | 0.0 |
| Total | 5/16 | 31.2 |
All of the patients diagnosed with laryngeal granulomas consequent to laryngopharyngeal reflux and who presented some improvement in the vocal symptoms or partial remission of the laryngeal lesions at the 2-month follow-up were instructed to maintain the diet and the proton pump inhibitor for a few more months. Only one of these patients underwent microsurgery. The longest treatment recorded for the remission of the symptoms and for the disappearance of the granuloma was 9 months.
Discussion
There is no consensus in the literature regarding the best treatment for laryngeal granulomas due to the diversity of etiologies. Among the several treatments, there are proton pump inhibitors, inhaled or oral corticosteroids, nonhormonal anti-inflammatory drugs, and botulinum toxin. 7 8 9 10 Pharmacological treatment is usually slow and requires dietary discipline and changing habits. Surgical treatment is fast, but requires general anesthesia, as well as hospitalization, and is not free of complications.
In the present study, intubation granulomas were the most prevalent (56%), confirming the data in the literature. 1 3 11 The pharmacological treatment was ineffective for most of these cases, with 77% requiring surgery. No patient with intubation granuloma submitted to surgery had postoperative recurrence, and the importance of maintaining the antireflux treatment after the surgical procedure should be emphasized. In a study that included 168 patients with vocal fold granulomas, Ma et al 12 found improvement in 41.3% (n = 71) with conservative treatment (pump inhibitors, vocal arrest, and voice therapy); however, higher resolution rates were seen after microsurgery alone (78.4%) or associated with botulinum toxin (95.2%).
Granulomas secondary to reflux corresponded to 25% of the cases and, in these, the pharmacological treatment presented a better success rate (75%). In two cases, remission was seen only after 9 months of treatment, confirming the importance of insisting on antireflux treatment for an extended period in such cases. Surgery was indicated in only one patient with granuloma consequent to reflux, and proved to be effective.
Idiopathic granulomas were the least frequent in our series and also the most refractory to treatment. In one case, complementary treatment with botulinum toxin was required, which has been advocated in recurring granulomas. 10 11 12 13
Conclusion
We presented our results for the treatment of laryngeal granulomas. Pharmacological treatment with inhaled corticosteroids and proton pump inhibitors was quite effective in granulomas secondary to laryngopharyngeal reflux; however, for postintubation granulomas, which were the most frequent, microsurgery was the best treatment.
Footnotes
Conflicts of Interests The authors have no conflicts of interests to declare.
References
- 1.Shoffel-Havakuk H, Halperin D, Yosef L, Feldberg E, Lahav Y. Lesions of the posterior glottis: clinical and pathologic considerations and treatment outcome. J Voice. 2014;28(02):2630–2.63E10. doi: 10.1016/j.jvoice.2013.08.013. [DOI] [PubMed] [Google Scholar]
- 2.Martins R H, Dias N H, Santos D C, Fabro A T, Braz J R. Clinical, histological and electron microscopic aspects of vocal fold granulomas. Rev Bras Otorrinolaringol (Engl Ed) 2009;75(01):116–122. doi: 10.1016/S1808-8694(15)30842-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jin Y J, Lee S J, Lee W Y, Jeong W J, Ahn S H. Prognostic factors for prediction of follow-up outcome of contact granuloma. Eur Arch Otorhinolaryngol. 2014;271(07):1981–1985. doi: 10.1007/s00405-014-2915-8. [DOI] [PubMed] [Google Scholar]
- 4.Lesser H, Rutt A, Sataloff R T. Vocal fold granulomas. Ear Nose Throat J. 2016;95(08):314. [PubMed] [Google Scholar]
- 5.Storck C, Brockmann M, Zimmermann E, Nekahm-Heis D, Zorowka P G. [Laryngeal granuloma. Aetiology, clinical signs, diagnostic procedures, and treatment] HNO. 2009;57(10):1075–1080. doi: 10.1007/s00106-008-1778-y. [DOI] [PubMed] [Google Scholar]
- 6.Lee S W, Hong H J, Choi S H et al. Comparison of treatment modalities for contact granuloma: a nationwide multicenter study. Laryngoscope. 2014;124(05):1187–1191. doi: 10.1002/lary.24470. [DOI] [PubMed] [Google Scholar]
- 7.Mesick M L, Weissbrod P A.Resolution of laryngeal granuloma with high-dose prednisone Ear Nose Throat J 201493(4-5):E60–E61. [PubMed] [Google Scholar]
- 8.Hong-Gang D, He-Juan J, Chun-Quan Z, Guo-Kang F. Surgery and proton pump inhibitors for treatment of vocal process granulomas. Eur Arch Otorhinolaryngol. 2013;270(11):2921–2926. doi: 10.1007/s00405-013-2527-8. [DOI] [PubMed] [Google Scholar]
- 9.Karkos P D, George M, Van Der Veen J et al. Vocal process granulomas: a systematic review of treatment. Ann Otol Rhinol Laryngol. 2014;123(05):314–320. doi: 10.1177/0003489414525921. [DOI] [PubMed] [Google Scholar]
- 10.Yılmaz T, Kayahan B, Günaydın RÖ, Kuşçu O, Sözen T. Botulinum Toxin A for Treatment of Contact Granuloma. J Voice. 2016;30(06):741–743. doi: 10.1016/j.jvoice.2015.07.015. [DOI] [PubMed] [Google Scholar]
- 11.Wang C P, Ko J Y, Wang Y H, Hu Y L, Hsiao T Y. Vocal process granuloma - A result of long-term observation in 53 patients. Oral Oncol. 2009;45(09):821–825. doi: 10.1016/j.oraloncology.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 12.Ma L, Xiao Y, Ye J, Yang Q, Wang J. Analysis of therapeutic methods for treating vocal process granulomas. Acta Otolaryngol. 2015;135(03):277–282. doi: 10.3109/00016489.2014.986756. [DOI] [PubMed] [Google Scholar]
- 13.Yilmaz T, Süslü N, Atay G, Özer S, Günaydin RÖ, Bajin M D. Recurrent contact granuloma: experience with excision and botulinum toxin injection. JAMA Otolaryngol Head Neck Surg. 2013;139(06):579–583. doi: 10.1001/jamaoto.2013.3186. [DOI] [PubMed] [Google Scholar]