

Abstract
Background
Myocardial infarction with nonobstructive coronary arteries (MINOCA) is a heterogeneous disease entity. Its prognosis and predictor of mortality remain unclear. This study aimed to compare the prognosis between MINOCA and myocardial infarction with obstructive coronary artery disease and identify factors related to all‐cause death in MINOCA using a nation‐wide, multicenter, and prospective registry.
Methods and Results
Among 13 104 consecutive patients enrolled, patients without previous history of significant coronary artery disease who underwent coronary angiography were selected. The primary outcome was 2‐year all‐cause death. Secondary outcomes were cardiac death, noncardiac death, reinfarction, and repeat revascularization. Patients with MINOCA (n=396) and myocardial infarction with obstructive coronary artery disease (n=10 871) showed similar incidence of all‐cause death (9.1% versus 8.8%; hazard ratio [HR], 1.04; 95% CI, 0.74–1.45; P=0.83). Risks of cardiac death, noncardiac death, and reinfarction were not significantly different between the 2 groups (HR, 0.82; 95% CI, 0.53–1.28; P=0.38; HR, 1.55; 95% CI, 0.93–2.56; P=0.09; HR, 1.23; 95% CI, 0.65–2.31; P=0.38, respectively). MINOCA patients had lower incidence of repeat revascularization (1.3% versus 7.2%; HR, 0.17; 95% CI, 0.07–0.41; P<0.001). Results were consistent after multivariable regression and propensity‐score matching. In a multivariate model, several significant predictors of all‐cause death of MINOCA were found, including the nonuse of renin‐angiotensin system blockers (HR, 2.63; 95% CI, 1.08–6.25; P=0.033) and statins (HR, 2.17; 95% CI, 1.04–4.54; P=0.039).
Conclusions
Patients with MINOCA and those with myocardial infarction with obstructive coronary artery disease had comparable clinical outcomes. Use of renin‐angiotensin system blockers and statins was associated with lower mortality in patients with MINOCA.
Keywords: coronary vasospasm, myocardial infarction, prognosis, renin angiotensin system, statin
Subject Categories: Myocardial Infarction, Prognosis
Short abstract
See Editorial Mukherjee
Clinical Perspective
What Is New?
Patients with Myocardial infarction with nonobstructive coronary arteries (MINOCA) had similar risks of all‐cause death and myocardial infarction compared with those with myocardial infarction with obstructive coronary artery disease.
Risk of all‐cause death of MINOCA with vasospasm did not differ from that of MINOCA without vasospasm.
Use of renin‐angiotensin system blockers and statins was independently associated with decreased risk of all‐cause mortality in patients with MINOCA.
What Are the Clinical Implications?
MINOCA is not a benign disease, but a disease which might require clinical attention and intensive medical treatment with renin‐angiotensin system blockers and statins to reduce mortality.
Introduction
Myocardial infarction with nonobstructive coronary arteries (MINOCA) is characterized by a positive cardiac biomarker and appropriate clinical scenario consistent with acute myocardial infarction (AMI). MINOCA is an infrequent (5–10% of AMI) syndrome with heterogeneous etiologies, including plaque disruption, coronary spasm, and coronary thromboembolism. Sometimes it is difficult to differentiate it from stress‐induced cardiomyopathy, myocarditis, and type 2 myocardial infarction (MI).1
Accordingly, data regarding the long‐term prognosis and its predictors of MINOCA are limited and controversial. Previous studies have demonstrated that MINOCA has a low risk of adverse clinical outcomes.2, 3, 4 Other studies have reported a considerable rate of mortality in MINOCA compared with MI with obstructive coronary artery disease (MI‐CAD).5, 6, 7 This uncertainty has led to variations in its treatment. Calcium‐channel blockers and vasodilators can be used for patients with a positive coronary spasm test.8 Conventional guideline‐recommended therapies, such as dual antiplatelet therapy, renin‐angiotensin system blockers, beta‐blockers, and statins, can also be prescribed for patients with MINOCA.9, 10
Therefore, the objective of this study was to evaluate the long‐term risk of clinical outcomes in patients with MINOCA compared with MI‐CAD. Independent predictors of mortality, including medications after discharge, were also determined using a large‐scale, nation‐wide, multicenter, dedicated registry for AMI.
Methods
Anonymized patient‐level data will be made available by the corresponding author upon reasonable request.
Study Protocols and Population Selection
Patients were derived from the nation‐wide, multicenter, prospective KAMIR‐NIH (Korean Acute Myocardial Infarction‐National Institutes of Health) registry. The KAMIR‐NIH was a dedicated prospective registry that consecutively enrolled AMI‐diagnosed patients at 20 tertiary university hospitals who were eligible for primary percutaneous coronary intervention from November 2011 to December 2015 without any exclusion criteria. The detailed study protocols have been previously published.11 The protocol of the KAMIR‐NIH registry was approved by the ethics committee at each participating center. This study was conducted according to the principles of the Declaration of Helsinki. All patients provided written informed consent upon enrollment.
To include the incident AMI patients only, we excluded patients who did not undergo coronary angiography (n=201) and those who had a previous history of MI, coronary intervention, or bypass surgery (n=1636) from 13 104 patients. We enrolled 396 patients with MINOCA (<50% stenosis in all vessels) and 10 871 patients with MI‐CAD (≥50% stenosis in any of their coronary arteries). If MINOCA was suspected, a vasospasm test was recommended as a standard of care. Of patients with MINOCA, 95 (24% of MINOCA) demonstrated vasospasm defined by spontaneous coronary spasm with ST‐segment elevation (≥0.1 mV) on the coronary angiogram and/or documented coronary spasm during an ergonovine provocation test (Figure 1). The test was considered positive for epicardial coronary spasm in the presence of focal or diffuse epicardial coronary diameter reduction ≥90% in comparison with the relaxed state following intracoronary nitroglycerine administration, associated with the reproduction of the patient's symptoms and ischemic electrocardiographic shifts.12 Data from coronary intravascular imaging or magnetic resonance imaging were limited; we did not include them in this analysis.
Figure 1.
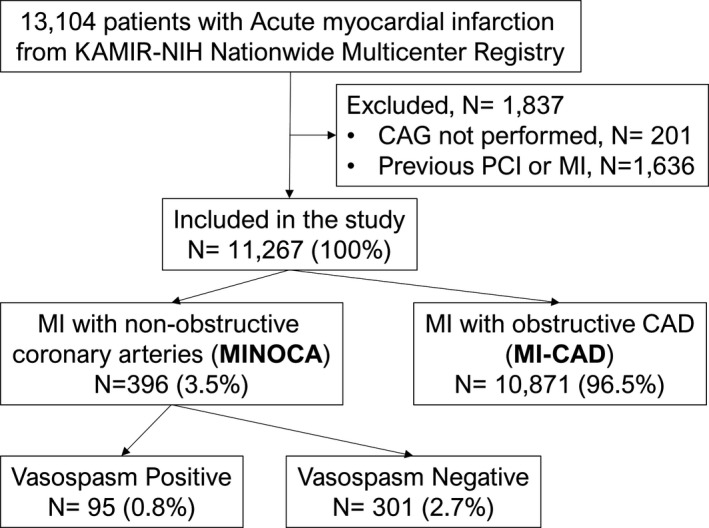
Study flow. The study population was derived from a nation‐wide, multicenter, prospective KAMIR‐NIH (Korea Acute Myocardial Infarction Registry‐National Institute of Health) registry. CAG indicates coronary angiography; MI, myocardial infarction; MI‐CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with nonobstructive coronary arteries; PCI, percutaneous coronary intervention.
Patient Management, Data Collection, and Follow‐up
Patient management was performed according to current standard guidelines. Patients with MI‐CAD underwent percutaneous coronary intervention by a standard technique if the patient was clinically indicated. Patients were also recommended to take aspirin indefinitely plus P2Y12 inhibitors, renin‐angiotensin system blockers, beta‐blockers, and statins that were prescribed according to the practice guidelines. Patients with MINOCA were treated with medications under the physician's discretion.
Demographic features and cardiovascular risk factors were collected by detailed patient interview. Patient chest pain was categorized according to the presence of substernal chest pain or discomfort that was provoked by exertion or emotional stress and was relieved by rest and/or nitroglycerin. Chest pain was classified as “typical” angina if all 3 descriptors were present and as “atypical” if <3 descriptors were present. During hospitalization, the findings of coronary angiography and detailed procedural characteristics of percutaneous coronary intervention as well as information on the discharge medications were collected. A successful percutaneous coronary intervention was defined as a decrease in minimum stenosis diameter to <30% with Thrombolysis in Myocardial Infarction flow grade ≥2 on coronary angiogram. Recurrent ischemia was defined as presence of angina and changes in hemodynamics or ECG. After discharge, patients were followed at 6, 12, and 24 months by the attending physician. If patients did not visit on the day of the scheduled follow‐up, the outcome data were assessed by a telephone interview. All data were collected by independent clinical research coordinators using a web‐based case report form in the Internet‐based Clinical Research and Trial management system (iCReaT), which is a data management system established by the Centers for Disease Control and Prevention, Ministry of Health and Welfare, Republic of Korea (iCReaT Study No. C110016). Clinical events that occurred within 2 years of follow‐up were analyzed.
Primary and Secondary End Points
The primary end point was all‐cause death. Secondary end points were cardiac death, noncardiac death, recurrent MI, and repeat revascularization. All deaths were considered cardiac unless an undisputed noncardiac cause was present. Recurrent MI was defined as recurrence of symptoms or presence of electrocardiographic changes in association with a rise in cardiac biomarker level above the upper limit of normal. Periprocedural MI was not included as a clinical outcome. Clinically driven revascularization that occurred after discharge from the index hospitalization was coded as a repeat revascularization event according to the Academic Research Consortium definitions.
Statistical Analysis
Categorical variables were presented as numbers and relative frequencies (percentages). They were compared using the chi‐squared test. Continuous variables are expressed as mean±SD. They were compared using an independent‐sample t test. Cumulative event rates were calculated based on Kaplan–Meier censoring estimates. Comparison of clinical outcomes between patients with MINOCA and patients with MI‐CAD was performed with a log‐rank test. Given that differences in baseline characteristics could significantly affect outcomes, a multivariable Cox regression model was performed, adjusting for confounders as much as possible. Covariates in the multivariable model were selected if they were significantly different between the 2 groups, including the following: age, sex, Killip class at initial presentation, diabetes mellitus, current smoking, ST changes in the initial ECG, lipid profile, and left ventricular ejection fraction. A propensity score analysis was also performed to adjust for potential confounders with a logistic regression model. The variables listed above were used. Prediction accuracy of the logistic model was assessed with an area under the receiver‐operating characteristic curve (C statistic), which was 0.802 (95% CI, 0.780–0.825). According to the propensity score, patients were selected by 1:1 matching without replacement using the nearest neighbor method. A caliper width of 0.2 standardized differences (SD) was used for matching. This value has been shown to eliminate almost 99% of the bias in observed confounders.13 Furthermore, to identify independent predictors of all‐cause death in patients with MINOCA, we used a multivariable Cox proportional hazard model. The C‐statistics with 95% CI were calculated to validate the discriminant function of the model. Echocardiogram data of 486 patients (4.3%) was missing: 25 in MINOCA (6.3%) and 461 in MI‐CAD (4.2%). We performed the multiple imputation for missing data of the echocardiogram. As a sensitivity analysis, we analyzed data of patients without missing data of echocardiogram (Tables S1 through S3). In all analyses, participating centers were included as the stratification factor. All probability values were 2‐sided, and P<0.05 was considered statistically significant. Statistical packages of SPSS software (version 22.0; SPSS, Inc., Chicago, IL) were used for all statistical analyses.
Results
Baseline Characteristics Between the Groups
Baseline characteristics of the patient groups are listed in Table 1. Compared with patients with MI‐CAD, those with MINOCA were more likely to be women, but less likely to be diabetic. They had a lower Killip class, lower creatine kinase‐myocardial band level, lower low‐density lipoprotein cholesterol, higher high‐density lipoprotein cholesterol, higher ejection fraction, and lower regional wall motion score in the echocardiogram. However, rates of previous angina and previous heart failure were higher in MINOCA than in MI‐CAD.
Table 1.
Baseline Demographic, Laboratory, and Angiographic Characteristics
| Overall Population (N=13 104) | MINOCA (N=396) | MI‐CAD (N=10 871) | P Value | |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age, y | 64.0±12.6 | 62.3±12.6 | 63.4±12.7 | 0.097 |
| Male | 9686 (73.9%) | 227 (57.3%) | 8144 (74.9%) | <0.001 |
| BMI, kg/m2 | 24.0±3.4 | 23.8±3.4 | 24.0±3.3 | 0.149 |
| Symptom at presentation | ||||
| Typical chest pain | 11 294 (86.2%) | 315 (79.5%) | 9475 (87.2%) | <0.001 |
| Dyspnea | 3105 (23.7%) | 85 (21.5%) | 2482 (22.8%) | 0.540 |
| Killip | 0.008 | |||
| 1 | 10 220 (78.0%) | 325 (82.1%) | 8602 (79.1%) | |
| 2 | 1133 (8.6%) | 42 (10.6%) | 893 (8.2%) | |
| 3 | 977 (7.5%) | 14 (3.5%) | 741 (6.8%) | |
| 4 | 773 (5.9%) | 15 (3.8%) | 634 (5.8%) | |
| Cardiac arrest on arrival | 96 (0.7%) | 2 (0.5%) | 77 (0.7%) | 1.0 |
| Previous history of angina | 1279 (9.8%) | 48 (12.1%) | 394 (3.6%) | <0.001 |
| Previous history of heart failure | 213 (1.6%) | 12 (3.0%) | 92 (0.8%) | <0.001 |
| Hypertension | 6690 (51.1%) | 201 (50.8%) | 5320 (48.9%) | 0.506 |
| Diabetes mellitus | 3752 (28.6%) | 87 (22.0%) | 2882 (26.5%) | 0.050 |
| Dyslipidemia | 1388 (10.6%) | 35 (8.8%) | 1116 (10.3%) | 0.397 |
| Family history of CAD | 830 (6.3%) | 19 (4.8%) | 715 (6.6%) | 0.182 |
| Current smoking | 5113 (39.0%) | 126 (31.8%) | 4492 (41.3%) | <0.001 |
| Previous CVA | 888 (6.8%) | 23 (5.8%) | 671 (6.2%) | 0.904 |
| Initial vital sign | ||||
| Systolic BP | 130.1±30.0 | 132.8±30.7 | 130.5±29.9 | 0.136 |
| Diastolic BP | 78.6±18.3 | 78.9±17.9 | 79.0±18.3 | 0.920 |
| Heart rate | 78.7±19.6 | 80.2±18.6 | 78.3±19.3 | 0.046 |
| Initial ECG | ||||
| ST elevation | 6194 (46.9%) | 59 (14.9%) | 5684 (52.3%) | <0.001 |
| ST depression | 1567 (12.0%) | 36 (9.1%) | 1285 (11.8%) | 0.115 |
| Wide QRS tachycardia | 112 (0.8%) | 6 (1.5%) | 83 (0.8%) | 0.134 |
| Atrial fibrillation | 712 (5.4%) | 30 (7.6%) | 610 (5.6%) | 0.093 |
| Complete atrioventricular block | 62 (0.5%) | 0 (0.0%) | 58 (0.5%) | 0.271 |
| Laboratory characteristics | ||||
| Creatinine, mg/dL | 1.1±1.2 | 1.0±1.0 | 1.1±1.1 | 0.085 |
| Peak CK‐MB, ng/mL | 110.6±164.4 | 31.1±67.3 | 118.5±170.1 | <0.001 |
| Troponin, ng/mL | ||||
| Troponin I | 46.8±105.6 (n=11 182) | 9.6±26.7 (n=368) | 50.2±111.7 (n=9197) | <0.001 |
| Troponin T | 14.2±459.6 (n=1922) | 0.6±0.9 (n=28) | 15.9±492.4 (n=1674) | <0.001 |
| Total cholesterol | 177.9±46.3 | 169.1±55.3 | 182.4±45.2 | <0.001 |
| Triglyceride, mg/dL | 134.5±120.1 | 128.5±207.9 | 136.8±120.1 | 0.231 |
| HDL‐C, mg/dL | 42.8±12.5 | 47.2±14.2 | 42.8±12.0 | <0.001 |
| LDL‐C, mg/dL | 112.0±39.6 | 100.6±36.0 | 116.0±39.1 | <0.001 |
| LVEF, % | 51.9±11.2 | 58.5±11.0 | 52.2±10.6 | <0.001 |
| Regional wall motion index | 1.42±0.39 | 1.19±0.33 | 1.41±0.37 | <0.001 |
| Angiographic characteristics | ||||
| Multivessel disease | 5761 (44.0%) | 5024 (46.2%) | ||
| Left main disease | 658 (5.0%) | 526 (4.8%) | ||
| Culprit lesion | ||||
| Left main | 274 (2.1%) | 217 (2.0%) | ||
| LAD | 5476 (41.8%) | 4910 (45.2%) | ||
| LCX | 2053 (15.7%) | 1790 (16.5%) | ||
| RCA | 3951 (30.2%) | 3462 (31.8%) | ||
| Pre‐TIMI flow of culprit | ||||
| 0 | 5518 (42.1%) | 4956 (47.8%) | ||
| 1 | 1286 (9.8%) | 1113 (10.7%) | ||
| 2 | 1813 (13.8%) | 1566 (15.1%) | ||
| 3 | 3137 (23.9%) | 2744 (26.4%) | ||
| Culprit treatment | ||||
| Plain balloon angioplasty | 802 (6.1%) | 458 (4.4%) | ||
| Bare‐metal stent | 325 (2.5%) | 312 (3.0%) | ||
| First‐generation DES | 170 (1.3%) | 148 (1.4%) | ||
| Second‐generation DES | 10 381 (79.2%) | 9400 (91.1%) | ||
| Successful PCI | 11 580 (88.4%) | 10 236 (94.2%) | ||
| Total revascularization | 8063 (61.5%) | 7442 (68.5%) | ||
| Total number of stent | 1.3±0.9 | 1.4±0.8 | ||
| CABG | 258 (2.0%) | 199 (1.8%) | ||
Values are n (%) or mean±SD. P value is from a comparison of MINOCA and MI‐CAD. BMI indicates body mass index; BP, blood pressure; CABG, coronary artery bypass surgery; CAD, coronary artery disease; CK‐MB, creatine kinase‐myocardial band; CVA, cerebrovascular accident; DES, drug‐eluting stent; HDL‐C, high‐density lipoprotein cholesterol; LAD, left anterior descending artery; LCX, left circumflex artery; LDL‐C, low‐density lipoprotein cholesterol; LVEF, left ventricular ejection fraction; MI‐CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with nonobstructive coronary arteries; PCI, percutaneous coronary intervention; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction.
In‐Hospital Events and Medications After Discharge
In‐hospital clinical events in patients and medications at discharge and 1 year are summarized in Table 2. Frequencies of cardiogenic shock and ventricular arrhythmias were lower in patients with MINOCA than in those with MI‐CAD during hospitalization. Rate of in‐hospital death, recurrent MI, stroke, acute kidney injury, sepsis, or multiorgan failure did not significantly differ between the 2 groups of patients. However, the discharge therapies, including dual antiplatelet therapy, renin‐angiotensin system blockers, beta‐blockers, and statin, were less frequently used in patients with MINOCA. Use of calcium‐channel blockers was higher in patients with MINOCA than that in those with significant stenosis. This trend of the medications was maintained at 12 months after the index hospitalization.
Table 2.
In‐Hospital Events and Medications After Discharge
| MINOCA (N=396) | MI‐CAD (N=10 871) | P Value | |
|---|---|---|---|
| In‐hospital events | |||
| Cardiogenic shock | 20 (5.1%) | 971 (8.9%) | 0.008 |
| New‐onset heart failure | 14 (3.5%) | 452 (4.2%) | 0.689 |
| Recurrent ischemia | 0 (0.0%) | 96 (0.9%) | 0.051 |
| Recurrent MI | 0 (0.0%) | 43 (0.4%) | 0.406 |
| Cerebral infarction | 4 (1.0%) | 69 (0.6%) | 0.327 |
| Cerebral hemorrhage | 1 (0.3%) | 14 (0.1%) | 0.416 |
| Hemoglobin decrease >5 g/dL | 3 (0.8%) | 128 (1.2%) | 0.632 |
| Ventricular arrhythmia | 8 (2.0%) | 514 (4.7%) | 0.014 |
| Acute kidney injury | 4 (1.0%) | 99 (0.9%) | 0.785 |
| Sepsis | 4 (1.0%) | 60 (0.6%) | 0.288 |
| Multiorgan failure | 2 (0.5%) | 69 (0.6%) | 1.000 |
| Temporary pacemaker | 0 (0.0%) | 347 (3.2%) | <0.001 |
| ICD | 0 (0.0%) | 6 (0.1%) | 1.000 |
| In‐hospital death | 11 (2.8%) | 382 (3.5%) | 0.575 |
| Cardiac death | 7 (1.8%) | 323 (3.0%) | 0.182 |
| Noncardiac death | 4 (1.0%) | 59 (0.5%) | |
| Medication at discharge | |||
| Aspirin | 378 (95.5%) | 10 840 (99.7%) | <0.001 |
| P2Y12 inhibitor | 146 (36.9%) | 10 493 (96.5%) | <0.001 |
| Calcium‐channel blocker | 208 (52.5%) | 596 (5.5%) | <0.001 |
| Beta‐blocker | 133 (33.6%) | 9080 (83.5%) | <0.001 |
| RAS blocker | 192 (48.5%) | 8517 (78.3%) | <0.001 |
| Statin | 289 (73.0%) | 9988 (91.9%) | <0.001 |
| Medication at 1 year | |||
| Aspirin | 293 (84.9%) | 8783 (91.2%) | <0.001 |
| P2Y12 inhibitor | 57 (16.5%) | 5306 (55.1%) | <0.001 |
| Calcium‐channel blocker | 179 (51.9%) | 647 (6.7%) | <0.001 |
| Beta‐blocker | 90 (26.1%) | 7176 (74.5%) | <0.001 |
| RAS blocker | 137 (39.7%) | 6567 (68.2%) | <0.001 |
| Statin | 223 (64.6%) | 8591 (89.2%) | <0.001 |
Values are n (%). ICD indicates implantable cardioverter‐defibrillator; MI, myocardial infarction; MI‐CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with nonobstructive coronary arteries; RAS, renin‐angiotensin system.
Mid‐Term Clinical Outcomes
Results of the comparison of clinical outcomes at 2 years between MINOCA and MI‐CAD are shown in Table 3 and Figure 2. The median follow‐up duration of patients with MINOCA was similar to that of those with MI‐CAD (median [interquartile range]; 733 [697–759] versus 732 days [694–760]; P=0.68). The unadjusted rate of all‐cause death at 2 years (ie, the primary outcome) did not significantly differ between patients with MINOCA and those with MI‐CAD. For the secondary outcomes, the rate of cardiac death, noncardiac death, and recurrent MI was not significantly different between the 2 groups either. However, the rate of repeat revascularization was higher in patients with MI‐CAD.
Table 3.
Comparison of 2‐Year Clinical Outcomes
| MINOCA (N=396) | MI‐CAD (N=10 871) | Unadjusted | Multivariable‐Adjusted | Propensity‐Score Matched | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | P Value | HR (95% CI) | P Value | HR (95% CI) | P Value | |||
| All‐cause deatha | 9.1 (36) | 8.8 (954) | 1.04 (0.74–1.45) | 0.832 | 1.18 (0.74–1.87) | 0.493 | 1.25 (0.77–2.05) | 0.364 |
| Noncardiac death | 4.0 (16) | 2.6 (285) | 1.55 (0.93–2.56) | 0.09 | 1.21 (0.59–2.48) | 0.596 | 1.81 (0.80–4.10) | 0.154 |
| Cardiac death | 5.1 (20) | 6.2 (669) | 0.82 (0.53–1.28) | 0.384 | 1.13 (0.62–2.08) | 0.689 | 1.01 (0.54–1.87) | 0.986 |
| Recurrent MI | 2.8 (11) | 2.2 (241) | 1.23 (0.65–2.31) | 0.528 | 1.12 (0.52–2.42) | 0.764 | 0.92 (0.39–2.18) | 0.856 |
| Any repeat revascularization | 1.3 (5) | 7.2 (783) | 0.17 (0.07–0.41) | <0.001 | 0.22 (0.09–0.53) | 0.001 | 0.15 (0.06–0.38) | <0.001 |
| Death or MI | 11.6 (46) | 10.7 (1158) | 1.08 (0.81–1.46) | 0.594 | 1.17 (0.78–1.75) | 0.451 | 1.14 (0.74–1.74) | 0.554 |
Values are % (n), unless otherwise indicated. Cumulative incidences of clinical outcomes at 2 years are presented. The number of patients with specific events is presented in parentheses. Multivariable Cox proportional hazard regression model and propensity‐score–matched cohort were used to adjust for baseline differences between the comparative groups. HR indicates hazard ratio; MI, myocardial infarction; MI‐CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with nonobstructive coronary arteries.
The primary outcome of the study.
Figure 2.

Cumulative incidence of primary and secondary outcomes. Kaplan–Meier curves with cumulative hazards of (A) all‐cause death, (B) MI, (C) death or MI, and (D) any repeat revascularization. MI indicates myocardial infarction; MI‐CAD, myocardial infarction with obstructive coronary artery disease; MINOCA, myocardial infarction with nonobstructive coronary arteries. *The primary outcome of the study.
Risk of all‐cause death in patients with MINOCA did not significantly differ from that of those with MI‐CAD after multivariate adjustment (hazard ratio [HR], 1.18; 95% CI, 0.74–1.87; P=0.49) and propensity matching (HR, 1.25; 95% CI, 0.77–2.05; P=0.36; Tables S4 and S5). Risk of cardiac death, noncardiac death, or recurrent MI was not significantly different either between the 2 groups. However, risk of repeat revascularization was higher in patients with MI‐CAD after multivariate adjustment and propensity matching.
Characteristics and Clinical Results According to Coronary Spasm Test in Patients With MINOCA
Patients with positive vasospasm were younger, more male, and more likely to have typical symptoms, ST elevation on the ECG, low serum creatinine, high ejection fraction, and low regional wall motion index compared with those with MINOCA and negative vasospasm (Table S6). The rate of in‐hospital events was not different between the 2 groups. Most of the patients with positive vasospasm were prescribed calcium‐channel blockers whereas dual antiplatelet therapy, renin‐angiotensin system blockers, and beta‐blockers were used less frequently in patients with positive vasospasm. This trend was also maintained at 12 months after the index hospitalization (Table S7). Incidence of all‐cause death was lower in patients with positive vasospasm than in those with negative vasospasm (3.2% versus 11.0%; P=0.023). There is no difference in occurrence of recurrent MI (4.2% versus 2.3%; P=0.304) and repeat revascularization (3.2% versus 0.7%; P=0.092) between the 2 groups.
Independent Predictors of Mortality in Patients With MINOCA
Multivariable Cox proportional hazard models were used to identify the independent predictors of all‐cause death at 2 years in patients with MINOCA (Table 4). At the patients’ initial presentation, an old age, atypical symptoms, ST elevation on the ECG, Killip Class IV, and diabetes mellitus were independent predictors of all‐cause death at 2 years. MI by vasospasm was not associated with risk of all‐cause death at 2 years (HR, 0.54; 95% CI, 0.16–1.84; P=0.323). Patients with ST elevation had lower ejection fraction (54.1±12.1% versus 59.7±10.9%; P=0.003), but higher regional wall motion index (1.41±0.43 versus 1.16±0.31; P<0.001). Regarding medical treatment, the nonuse of renin‐angiotensin system blockers (HR, 2.63; 95% CI, 1.08–6.25; P=0.033) and statins (HR, 2.17; 95% CI, 1.04–4.54; P=0.039) were independently associated with an increased risk of all‐cause death at 2 years.
Table 4.
Independent Predictors of All‐Cause Death in Patients With MINOCA
| Hazard Ratio | 95% CI | P Value | |
|---|---|---|---|
| Age | 1.04 | 1.01 to 1.08 | 0.02 |
| Atypical symptom | 5.98 | 2.68 to 13.37 | <0.001 |
| ST elevation at presentation | 3.57 | 1.61 to 7.90 | 0.002 |
| Killip Class I | Reference | ||
| Class II | 0.81 | 0.27 to 2.40 | 0.705 |
| Class III | 1.81 | 0.64 to 5.17 | 0.265 |
| Class IV | 6.05 | 2.13 to 17.20 | 0.001 |
| Diabetes mellitus | 3.12 | 1.47 to 6.64 | 0.003 |
| Nonuse of RAS blocker | 2.63 | 1.08 to 6.25 | 0.033 |
| Nonuse of statin | 2.17 | 1.04 to 4.54 | 0.039 |
Multivariate Cox model analysis for all‐cause death. MINOCA indicates myocardial infarction with nonobstructive coronary arteries; RAS, renin‐angiotensin system.
Discussion
In the present study, 2‐year clinical outcomes were compared between MINOCA and MI‐CAD using data from a nation‐wide, multicenter, prospective MI registry. Although patients with MINOCA had lower risk profiles compared with those with MI‐CAD, their frequencies of in‐hospital events, such as MI, stroke, acute kidney injury, sepsis, and multiorgan failure and rates of mortality and recurrent MI at 2 years, were similar. For patients with MINOCA, use of renin‐angiotensin system blockers and statins showed a significantly lower risk of all‐cause death.
Previous meta‐analyses have demonstrated that patients with MINOCA have a lower likelihood of death or cardiovascular events than those with MI‐CAD.14, 15 Baseline characteristics were comparable with previous studies. MINOCA patients of our study also were less likely to be male, diabetic, current smoker, and to be treated with antiplatelet agents, beta‐blockers, renin‐angiotensin system blockers, and statins. Age and frequency of hypertension in MINOCA patients were higher compared with the previous studies. The results of each of the studies enrolled in the meta‐analysis are heterogeneous. Several studies have reported that patients with MINOCA and those with MI‐CAD show a similar long‐term mortality.6, 7, 16, 17, 18 The reason for such discrepancies among the studies is likely attributed to the different inclusion criteria because patients with MINOCA have heterogenous mechanistic profiles. In particular, Takostubo syndrome is 1 of the primary mechanisms of MINOCA.1 Other medical conditions and neurological disorders are critical triggering factors and contribute to the mortality increase in Takostubo syndrome.19 In the present study, frequency of those conditions in the index hospitalization did not significantly differ between the MINOCA group and the MI‐CAD group. A previous study16 reported that causes of death of MINOCA patients were significantly less often cardiovascular. Though the rate of noncardiac death was numerically higher in patients with MINOCA of previous studies those with MINOCA in this study, it was not statistically significant in every analysis. This suggests that MINOCA patients in this study were more homogenous than those of the other studies.
Elucidating the pathophysiological cause of MINOCA is challenging, but crucial to establish an appropriate management strategy. Coronary spasm and spontaneous coronary dissection (type 2 MI) as well as atherosclerotic plaque disruption and coronary thrombosis (type 1 MI) may be the cause of MINOCA.20 A provocation test with intracoronary acetylcholine or ergonovine to rule out the vasospasm in MINOCA can be performed safely to identify high‐risk patients.8 In this study, 24% of patients with MINOCA had vasospasm. That rate was comparable with the rate reported in previous studies.15 The prognosis of patients with MINOCA by vasospasm remains controversial.8 However, the presence of vasospasm did not influence the risk of all‐cause death in the present study.
The long‐term medical treatment strategy in patients with MINOCA is also a challenging issue. Previous studies have suggested that use of renin‐angiotensin system blockers9, 10 and statins9 is associated with a lower risk of all‐cause death. Our study was in line with those studies. Although one‐quarter of the patients had vasospasm, use of calcium‐channel blockers was not related to mortality. Use of dual antiplatelet therapy or use of beta‐blockers was not an independent predictor of all‐cause death either. Because nonobstructive coronary artery lesions cause most MIs,21 use of renin‐angiotensin system blockers and statins might be able to suppress the progression of nonobstructive plaques and the occurrence of major cardiac events. Nevertheless, in patients with CAD and absence of heart failure or depressed left ventricular function, renin‐angiotensin system blockers has shown beneficial effects on mortality and morbidity.9 Properly designed and powered randomized clinical trials are needed to confirm this hypothesis.
Consistent with a previous study,22 the present study revealed that nonobstructive coronary artery disease was more common in patients with non‐ST elevation MI than that in patients with ST‐elevation MI. The present study also showed that ST elevation in MINOCA was associated with an increased risk of all‐cause death. This can be explained by more extensive myocardial damage on echocardiography. Female sex also was not the predictor of mortality of MINOCA. Excess risk of post‐MI death in women is restricted to those with MI‐CAD in previous studies.14, 23 Furthermore, atypical symptoms was also an independent predictor of all‐cause death in MINOCA. Compared with typical symptoms, atypical symptoms in MI are related to higher risk profiles of patients and delayed initial management known to be associated with increased mortality.24
This study had an inherent limitation regarding its observational nature with registry data. However, the KAMIR‐NIH registry used standardized definitions for all collected variables regulated and monitored by the National Institutes of Health. In addition, this study did not include information from coronary intravascular imaging or magnetic resonance imaging to reveal all specific causes of AMIs. Stratification by the cause through an in‐depth investigation might provide the prognosis and appropriate management strategy according to causes of MINOCA.
Conclusion
Patients with MINOCA have similar risk of all‐cause death and MI at 2 years compared with those with MI‐CAD. Treatment with renin‐angiotensin system blockers and statins might improve the prognosis of these high‐risk patients.
Disclosures
None.
Supporting information
Appendix S1. Investigators of KAMIR‐NIH.
Table S1. Baseline Demographic, Laboratory, and Angiographic Characteristics in Patients Without Missing Data of Echocardiogram
Table S2. In‐Hospital Events and Medications After Discharge in Patients Without Missing Data of Echocardiogram
Table S3. Comparison of 2‐Year Clinical Outcomes in Patients Without Missing Data of Echocardiogram
Table S4. Baseline Demographic, Laboratory, and Angiographic Characteristics in a Propensity‐Score–Matched Population
Table S5. In‐Hospital Events and Medications After Discharge in a Propensity‐Score–Matched Population
Table S6. Baseline Demographic, Laboratory, and Angiographic Characteristics According to the Presence of Vasospasm
Table S7. In‐Hospital Events and Medication After Discharge According to the Presence of Vasospasm
(J Am Heart Assoc. 2019;8:e011990 DOI: 10.1161/JAHA.119.011990.)
References
- 1. Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, De Caterina R, Zimarino M, Roffi M, Kjeldsen K, Atar D, Kaski JC, Sechtem U, Tornvall P. ESC working group position paper on myocardial infarction with non‐obstructive coronary arteries. Eur Heart J. 2017;38:143–153. [DOI] [PubMed] [Google Scholar]
- 2. Roe MT, Harrington RA, Prosper DM, Pieper KS, Bhatt DL, Lincoff AM, Simoons ML, Akkerhuis M, Ohman EM, Kitt MM, Vahanian A, Ruzyllo W, Karsch K, Califf RM, Topol EJ. Clinical and therapeutic profile of patients presenting with acute coronary syndromes who do not have significant coronary artery disease. The Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy (PURSUIT) Trial Investigators. Circulation. 2000;102:1101–1106. [DOI] [PubMed] [Google Scholar]
- 3. Diver DJ, Bier JD, Ferreira PE, Sharaf BL, McCabe C, Thompson B, Chaitman B, Williams DO, Braunwald E. Clinical and arteriographic characterization of patients with unstable angina without critical coronary arterial narrowing (from the TIMI‐IIIA Trial). Am J Cardiol. 1994;74:531–537. [DOI] [PubMed] [Google Scholar]
- 4. Patel MR, Chen AY, Peterson ED, Newby LK, Pollack CV Jr, Brindis RG, Gibson CM, Kleiman NS, Saucedo JF, Bhatt DL, Gibler WB, Ohman EM, Harrington RA, Roe MT. Prevalence, predictors, and outcomes of patients with non‐ST‐segment elevation myocardial infarction and insignificant coronary artery disease: results from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) initiative. Am Heart J. 2006;152:641–647. [DOI] [PubMed] [Google Scholar]
- 5. Dokainish H, Pillai M, Murphy SA, DiBattiste PM, Schweiger MJ, Lotfi A, Morrow DA, Cannon CP, Braunwald E, Lakkis N. Prognostic implications of elevated troponin in patients with suspected acute coronary syndrome but no critical epicardial coronary disease: a TACTICS‐TIMI‐18 substudy. J Am Coll Cardiol. 2005;45:19–24. [DOI] [PubMed] [Google Scholar]
- 6. Andersson HB, Pedersen F, Engstrom T, Helqvist S, Jensen MK, Jorgensen E, Kelbaek H, Rader S, Saunamaki K, Bates E, Grande P, Holmvang L, Clemmensen P. Long‐term survival and causes of death in patients with ST‐elevation acute coronary syndrome without obstructive coronary artery disease. Eur Heart J. 2018;39:102–110. [DOI] [PubMed] [Google Scholar]
- 7. Planer D, Mehran R, Ohman EM, White HD, Newman JD, Xu K, Stone GW. Prognosis of patients with non‐ST‐segment‐elevation myocardial infarction and nonobstructive coronary artery disease: propensity‐matched analysis from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circ Cardiovasc Interv. 2014;7:285–293. [DOI] [PubMed] [Google Scholar]
- 8. Montone RA, Niccoli G, Fracassi F, Russo M, Gurgoglione F, Camma G, Lanza GA, Crea F. Patients with acute myocardial infarction and non‐obstructive coronary arteries: safety and prognostic relevance of invasive coronary provocative tests. Eur Heart J. 2018;39:91–98. [DOI] [PubMed] [Google Scholar]
- 9. Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjold A, Gard A, Jernberg T. Medical therapy for secondary prevention and long‐term outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation. 2017;135:1481–1489. [DOI] [PubMed] [Google Scholar]
- 10. Manfrini O, Morrell C, Das R, Barth JH, Hall AS, Gale CP, Cenko E, Bugiardini R. Effects of angiotensin‐converting enzyme inhibitors and beta blockers on clinical outcomes in patients with and without coronary artery obstructions at angiography (from a Register‐Based Cohort Study on Acute Coronary Syndromes). Am J Cardiol. 2014;113:1628–1633. [DOI] [PubMed] [Google Scholar]
- 11. Kim JH, Chae SC, Oh DJ, Kim HS, Kim YJ, Ahn Y, Cho MC, Kim CJ, Yoon JH, Park HY, Jeong MH. Multicenter cohort study of acute myocardial infarction in Korea—interim analysis of the Korea Acute Myocardial Infarction Registry‐National Institutes of Health Registry. Circ J. 2016;80:1427–1436. [DOI] [PubMed] [Google Scholar]
- 12. Shin DI, Baek SH, Her SH, Han SH, Ahn Y, Park KH, Kim DS, Yang TH, Choi DJ, Suh JW, Kwon HM, Lee BK, Gwon HC, Rha SW, Jo SH. The 24‐month prognosis of patients with positive or intermediate results in the intracoronary ergonovine provocation test. JACC Cardiovasc Interv. 2015;8:914–923. [DOI] [PubMed] [Google Scholar]
- 13. Austin PC. Optimal caliper widths for propensity‐score matching when estimating differences in means and differences in proportions in observational studies. Pharm Stat. 2011;10:150–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Pizzi C, Xhyheri B, Costa GM, Faustino M, Flacco ME, Gualano MR, Fragassi G, Grigioni F, Manzoli L. Nonobstructive versus obstructive coronary artery disease in acute coronary syndrome: a meta‐analysis. J Am Heart Assoc. 2016;5:e004185 DOI: 10.1161/JAHA.116.004185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131:861–870. [DOI] [PubMed] [Google Scholar]
- 16. Redondo‐Dieguez A, Gonzalez‐Ferreiro R, Abu‐Assi E, Raposeiras‐Roubin S, Aidhodjayeva O, Lopez‐Lopez A, Castineira‐Busto M, Pena‐Gil C, Garcia‐Acuna JM, Gonzalez‐Juanatey JR. Long‐term prognosis of patients with non‐ST‐segment elevation acute myocardial infarction and coronary arteries without significant stenosis. Rev Esp Cardiol (Engl Ed). 2015;68:777–784. [DOI] [PubMed] [Google Scholar]
- 17. Safdar B, Spatz ES, Dreyer RP, Beltrame JF, Lichtman JH, Spertus JA, Reynolds HR, Geda M, Bueno H, Dziura JD, Krumholz HM, D'Onofrio G. Presentation clinical profile, and prognosis of young patients with myocardial infarction with nonobstructive coronary arteries (MINOCA): results from the VIRGO study. J Am Heart Assoc. 2018;7:e009174 DOI: 10.1161/JAHA.118.009174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Da Costa A, Isaaz K, Faure E, Mourot S, Cerisier A, Lamaud M. Clinical characteristics, aetiological factors and long‐term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3‐year follow‐up study of 91 patients. Eur Heart J. 2001;22:1459–1465. [DOI] [PubMed] [Google Scholar]
- 19. Ghadri JR, Kato K, Cammann VL, Gili S, Jurisic S, Di Vece D, Candreva A, Ding KJ, Micek J, Szawan KA, Bacchi B, Bianchi R, Levinson RA, Wischnewsky M, Seifert B, Schlossbauer SA, Citro R, Bossone E, Munzel T, Knorr M, Heiner S, D'Ascenzo F, Franke J, Sarcon A, Napp LC, Jaguszewski M, Noutsias M, Katus HA, Burgdorf C, Schunkert H, Thiele H, Bauersachs J, Tschope C, Pieske BM, Rajan L, Michels G, Pfister R, Cuneo A, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun‐Dullaeus RC, Banning A, Cuculi F, Kobza R, Fischer TA, Vasankari T, Airaksinen KEJ, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Empen K, Felix SB, Delmas C, Lairez O, El‐Battrawy I, Akin I, Borggrefe M, Horowitz J, Kozel M, Tousek P, Widimsky P, Gilyarova E, Shilova A, Gilyarov M, Winchester DE, Ukena C, Bax JJ, Prasad A, Bohm M, Luscher TF, Ruschitzka F, Templin C. Long‐term prognosis of patients with Takotsubo syndrome. J Am Coll Cardiol. 2018;72:874–882. [DOI] [PubMed] [Google Scholar]
- 20. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40:237–269. [DOI] [PubMed] [Google Scholar]
- 21. Chang HJ, Lin FY, Lee SE, Andreini D, Bax J, Cademartiri F, Chinnaiyan K, Chow BJW, Conte E, Cury RC, Feuchtner G, Hadamitzky M, Kim YJ, Leipsic J, Maffei E, Marques H, Plank F, Pontone G, Raff GL, van Rosendael AR, Villines TC, Weirich HG, Al'Aref SJ, Baskaran L, Cho I, Danad I, Han D, Heo R, Lee JH, Rivzi A, Stuijfzand WJ, Gransar H, Lu Y, Sung JM, Park HB, Berman DS, Budoff MJ, Samady H, Shaw LJ, Stone PH, Virmani R, Narula J, Min JK. Coronary atherosclerotic precursors of acute coronary syndromes. J Am Coll Cardiol. 2018;71:2511–2522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Johnston N, Jonelid B, Christersson C, Kero T, Renlund H, Schenck‐Gustafsson K, Lagerqvist B. Effect of gender on patients with ST‐elevation and non‐ST‐elevation myocardial infarction without obstructive coronary artery disease. Am J Cardiol. 2015;115:1661–1666. [DOI] [PubMed] [Google Scholar]
- 23. Smilowitz NR, Mahajan AM, Roe MT, Hellkamp AS, Chiswell K, Gulati M, Reynolds HR. Mortality of myocardial infarction by sex, age, and obstructive coronary artery disease status in the ACTION Registry‐GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry‐Get With the Guidelines). Circ Cardiovasc Qual Outcomes. 2017;10:e003443. [DOI] [PubMed] [Google Scholar]
- 24. Fujino M, Ishihara M, Ogawa H, Nakao K, Yasuda S, Noguchi T, Ozaki Y, Kimura K, Suwa S, Fujimoto K, Nakama Y, Morita T, Shimizu W, Saito Y, Hirohata A, Morita Y, Inoue T, Okamura A, Uematsu M, Ako J, Nakai M, Nishimura K, Miyamoto Y. Impact of symptom presentation on in‐hospital outcomes in patients with acute myocardial infarction. J Cardiol. 2017;70:29–34. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Investigators of KAMIR‐NIH.
Table S1. Baseline Demographic, Laboratory, and Angiographic Characteristics in Patients Without Missing Data of Echocardiogram
Table S2. In‐Hospital Events and Medications After Discharge in Patients Without Missing Data of Echocardiogram
Table S3. Comparison of 2‐Year Clinical Outcomes in Patients Without Missing Data of Echocardiogram
Table S4. Baseline Demographic, Laboratory, and Angiographic Characteristics in a Propensity‐Score–Matched Population
Table S5. In‐Hospital Events and Medications After Discharge in a Propensity‐Score–Matched Population
Table S6. Baseline Demographic, Laboratory, and Angiographic Characteristics According to the Presence of Vasospasm
Table S7. In‐Hospital Events and Medication After Discharge According to the Presence of Vasospasm