

Abstract
Soft tissue injuries around the knee present a challenge for providing a cover when there is loss of tissue. Various flaps comprising of skin and muscles around the joint have been described. Understanding the anatomical basis and the design of these flaps can aid in choosing the right flap for a given situation. A prompt cover of the defects aids in quicker healing and quicker rehabilitation of the patient.
Keywords: soft tissue defect, Knee joint, flap cover
Introduction
Soft tissue defects around the knee joint are caused by varied etiology. They present a challenge to the treating surgeon as the flap used for these has to not only cover the defect but also has to be pliable enough to restore full mobility of the joint after healing. Various flaps including muscle flaps and skin flaps have been described which have their own advantages and limitations ( Table 1 ). 1 A proper flap cover can be provided with a good understanding of the nature of the defect and the requirements for cover.
Table 1. Choice of flaps available for defects around the knee.
| Abbreviations: ALT, anterolateral thigh. | |
| Skin flaps | |
| Local flaps | Fasciocutaneous flap |
| Perforator based flaps | ALT perforator flap, lateral supragenicular artery perforator flap, pedicled vastus medialis perforator flap |
| Other cutaneous flaps | Medial sural artery flap, saphenous flap, lateral sural cutaneous artery flap |
| Muscle flaps | |
| Proximally based flaps | Gastrocnemius flap, peroneus longus flap, vastus medialis flap (V-Y flap) |
| Distally based flaps | Gracilis flap, sartorius flap, vastus medialis flap |
| Musculocutaneous flaps | |
| Proximally based flaps | Gastrocnemius musculocutaneous flap |
| Distally based flaps | Reverse ALT flap, split vastus lateralis musculocutaneous flap |
| Free flaps | |
| Free flaps | ALT flap, latissimus dorsi flap |
Etiology
The defects around the knee joint can be of varied etiology. They are as follows:
Trauma causing injuries in road traffic accidents: This is the most common cause in our country. Apart from addressing the soft tissue loss, the underlying bony fracture too, when present, needs to be addressed. Hence, it needs to be planned to cover the bone and the implant.
Resection of tumors: The extent of resection is planned preoperatively depending on the nature and spread of tumor and based on the final defect the type of flap required is decided.
Skin and soft tissue infections which cause necrosis of skin
Post-burn contractures of knee which after release will leave a defect. The challenge in these defects is that the flap choices may be limited due to the surrounding scar.
Vascular Anatomy
The blood supply around the knee comes mainly from the femoral and the popliteal vessels. The branches and perforators which arise from these vessels form an anastomosis around the knee which forms the basis for distally based flaps. On the medial side, there are perforators from the descending genicular artery and the recurrent artery from anterior tibial artery. On the lateral side, superior and inferior lateral genicular arteries arising from the popliteal artery contribute to the anastomosis. The flaps can be raised based just on the perforators or along with the underlying muscles and their feeding vessels. In the leg, they can be based on the perforators from anterior tibial, posterior tibial, or peroneal arteries or along with the muscle and their feeding vessels ( Fig. 1 ).
Fig. 1.
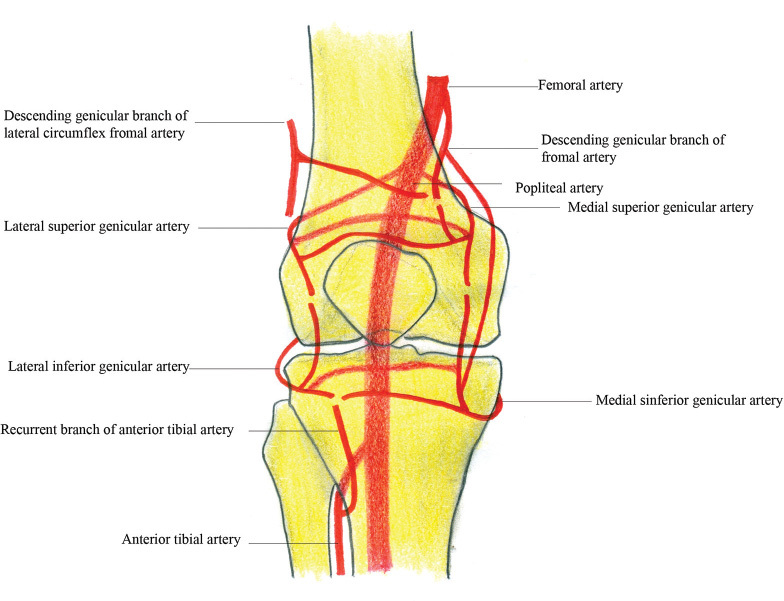
Anastomosis around knee joint.
Considerations for Coverage of Defects around Knee Joint
Knee joint is a hinge type joint with main movements of flexion and extension apart from minimal rotation. The thin pliable skin around the joint permits these movements without problem and any flap must be able to match this.
When a flap is bulky, the extent of the defect can be planned with knee in full flexion so that it will not restrict the flexion of the joint. The stability of the joint depends on the integrity of the ligaments and other structures around the joint. In case of loss of these structures like patellar tendon, they should also be reconstructed along with the flap coverage either separately with a fascia or using the aponeurotic portion of the covering flap. Achieving a primary healing in a shortest possible time reduces the duration of immobilization and helps preventing stiffness of the joint.
Planning a Flap
A proper analysis of the defect around the knee joint will have to be done before choosing the proper flap for cover.
The first consideration is the dimension of the defect. If it is a small-to-moderate defect, it can be covered with a local fasciocutaneous flap or a muscle flap. If it is large, it will require a free flap or a reverse flow skin flap from the thigh. Surface defects can be covered with a skin flap, while the deeper cavity may need a muscle flap to fill the associated dead space.
The next consideration will be the condition of the surrounding tissues. When there is degloving of the skin, a fasciocutaneous flap cannot be planned reliably. In case of injury to the muscles, they cannot be used as a flap. These should be assessed at the time of initial debridement. If flaps from the leg are not possible, the extent of damage in the thigh needs to be for the possibility of designing a reverse flow muscle or skin flap. This may be tricky in case of fractures involving the lower end of the femur where the anastomosis around the knee joint or the perforators in that region will be damaged.
The third consideration will be to look for the condition of the vessels in and around the knee joint which can be used as recipient vessels for free flaps. Unlike the ankle region where the vessels are quite superficial, near the knee they lie at a much deeper plane.
Choice of whether to do a fasciocutaneous flap, musculocutaneous flap, or muscle flap with skin graft depends on the surgeon ( Fig. 2 ). It was believed that muscle flaps are better in case of infection as they can fight it better. But studies have shown that it is not so and the vascularity of both types of flaps is equal. 2 3 Studies also have indicated there is no difference whatsoever in terms of healing or functional outcome between these two types of flaps in trauma. 4
Fig. 2.
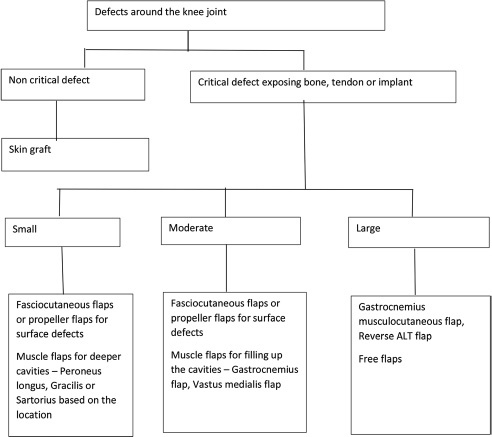
Algorithm for choosing a flap for coverage of knee defects. ALT, anterolateral thigh.
The advantages of the skin flaps are that they are aesthetically better than muscle flaps covered with skin grafts. They also spare the function of a core muscle. When a later surgical intervention like a bone graft or debulking is planned, a skin flap will allow better access and closure of the surgical wound compared with muscle flaps which can have problems in such situations. 5
Fasciocutaneous Flaps
These flaps have been used ever since Ponten described them. The flap is raised at the sub fascial level. If any perforators are seen during dissection, they can be preserved if they do not affect the mobility of the flap. They are reliable if there is no degloving or contusion of the skin.
Usually they are raised as proximally based flaps from the leg but if it is not possible, a distally based flap can be designed from the thigh which may need a prior delay procedure to increase their reliability. If they include the perforators from underlying descending branch of lateral circumflex femoral artery or lateral supragenicular artery or saphenous artery they may be raised more reliably in a single stage. 6
Muscle Flaps
Even though no muscle are present at the knee joint, their presence in the thigh and the leg has made their use possible for cover of the knee defects. Their purported advantages are their ability to fill up the cavity and help to combat infections due to their vascularity. 7 The following muscles have been described for knee defects.
Gastrocnemius
This is the first choice in case of knee and the upper third leg defects. Either the medial or the lateral belly or both can be used for coverage. They get their blood supply from the femoral artery with the branches that originate above the knee joint. As the origin of these vessels is deep inside the popliteal fossa, the pedicles are usually protected in case of trauma and are available for use.
The flap is raised proximally up to its origin. The reach of the flap can be increased by dividing the tendinous fibers at the origin on the superficial surface or scoring the aponeurotic layer in the under surface of the muscle or totally islanding the flap based on its vascular pedicle. 8 9
The lateral belly of gastrocnemius is smaller compared with the medial belly but can be used to cover the defects on the lateral aspect of the knee. One should avoid injury to the common peroneal nerve when raising and tunneling it across to the defect.
The tendinous portion of the muscle can be used for bridging the quadriceps tendon and helps reconstruction of the quadriceps apparatus along with coverage of the wound around the joint thus providing dual function. 10
The modifications like distally based gastrocnemius flap with arterial anastomosis or as local free flap where a vein graft is interposed between the pedicle to lengthen its reach have been described. 11 12 13
Both the bellies can be used as split muscle for coverage of different areas as the pedicle arteries bifurcate within the substance of the muscle. This has been found to happen after 2.3 cm in medial belly and 3.1 cm in lateral belly. Hence, the muscle can be split up to this level without worrying about jeopardizing the blood supply. 14
If the defect is larger or requires volume, it can be combined with the soleus flap to give a larger surface area of flap to cover the defect. The perforators joining the soleus in the distal half of the gastrocnemius provide a retrograde flow to the soleus component. 15
The advantages of this flap are that it is reliable and easy to dissect. It can be used to reconstruct the patellar tendon too. The disadvantage is that the overlying skin graft may give an unaesthetic appearance ( Fig. 3A–D ).
Fig. 3.

( A ) Defect around knee joint. ( B ) Gastrocnemius flap covering the defect. ( C ) Postoperative photo—front view. ( D ) Postoperative photo—medial view.
Peroneus Longus
The peroneus longus muscle flap can be used as a proximally based flap to cover small-to-medium defects over the knee. This is a type IV muscle as per classification of Mathes and has a dense intramuscular web of vessels. As per the cadaveric studies, its average size has been found 4.7 × 15.8 cm with a constant perforator arising from anterior tibial artery ~4.4 cm below the fibular head. Although it may not be the first choice, it can be considered for small defects either alone when other options are not available or in conjunction with other flaps for bigger defects. The dissection starts from distal to proximal direction by an incision overlying the peroneal compartment and identifying the peroneus longus tendon. The flap may have a small perforator to the skin also which can be utilized if required. 16
The advantage of this flap is that it does not cause any functional morbidity but the disadvantage is that it is possible to cover only very small defects with this flap.
Vastus Medialis
This muscle is a part of quadriceps tendon and gets its segmental blood supply from the superficial femoral vessels. It has been used as an advancement flap based on its blood supply either alone or with the skin overlying it in a V-Y fashion to cover the defects over the knee joint. It also helps in reconstruction of the quadriceps tendon if there is loss of the same. Since it is transferred along with nerve supply, no function is lost in quadriceps function. There are very few reports of its use unlike the vastus lateralis. 17
Distally Based Muscle Flaps
When the muscles in the leg are not available due to injury or not sufficient in size to cover the defect, the muscles in the thigh can be used as distally based flaps to cover the knee defects.
Gracilis
When required, gracilis muscle can be used as a distally based flap to cover defects over the knee based on minor pedicles. But since its size is small, it can be used for small defects only. This can be used either alone for small defects or along with gastrocnemius.
A prior delay of the flap by ligating the proximal pedicles will make the flap more reliable. During dissection of the flap, a clamp is applied over the major pedicle and it is assessed for the viability based on the minor pedicles. If it is good, then an immediate transfer may be performed without delay. If not, the major pedicle is ligated and the flap is transferred at a later date. 18
Since it is a staged procedure, it is not commonly used but can be used when other choices are not available.
Vastus Lateralis
This is supplied by the descending branch of the lateral circumflex femoral artery. In the distal part, this gets perforators from superficial femoral and lateral genicular artery. 19 The entire muscle can be turned down as a distally based flap to cover large defects over the knee. This has a good reach and go to even 10 cm below the patella. 20 This is preserved by limiting the dissection about a hand breadth above the superior border of the patella. This flap is used when the other options are exhausted as it has some amount of morbidity in the form of decrease in strength of extension but it is not clinically significant. 21
A prior delay by ligating the proximal end of the feeding artery or supercharging and venous augmentation can ensure good survival of the flap. 22 23
Sartorius Flaps
This muscle has been used to cover small defects in the knee and leg when raised as a distally based flap. The distal part of muscle is supplied by branches from descending genicular and saphenous arteries. 24 A modification with skin island has also been described based on the anastomosis between the terminal saphenous artery, perforators of posterior tibial artery, and medial inferior genicular artery. The skin island is designed in the lower third of thigh and elevates the descending genicular artery along with sartorius with the pivot point at the adductor tubercle. It can be used to cover the defects at the knee and upper third of the leg. 25
Musculocutaneous Flaps
When the reach of the muscle alone is not good or when we need a cutaneous component to provide a better cover which can be opened later for secondary procedures, a musculocutaneous flap is planned. The following are the musculocutaneous flaps which are commonly used.
Gastrocnemius Musculocutaneous Flap
This skin overlying the muscle is elevated along with it as a flap. This can extend distally onto a point 5 cm proximal to the ankle. This skin component of the flap is supplied by a perforator arising from the muscle belly and the fascial network of vessels. This provides a longer flap with more skin when only the gastrocnemius muscle flap will not be sufficient to cover the defect. In the traditional design, both the muscle and the skin flap move together in the same direction. 26
Some modifications are described which can facilitate the differential movement of the muscle and the skin component which can better cover the defects as per the needs ( Fig. 4A–D ). This modification describes the skin component as islanded on the perforator which comes out of the muscle belly and supplies the overlying skin especially the lateral row of perforator. 27 28
Fig. 4.

( A ) Defect over the knee joint. ( B ) Defect with gastrocnemius myocutaneous flap. ( C ) Postoperative photo—front view. ( D ) Postoperative photo—donor site.
Reverse Flow Anterolateral Thigh Flap
Anterolateral thigh (ALT) flap can be used as a distally based pedicled musculocutaneous flap to cover the defects over the knee. The descending branch of lateral circumflex femoral artery has rich communications distally with perforators of lateral genicular artery and anastomosis around knee joint. 29 30 This flap has a large size and can reach up to 14 cm below the knee joint. The fascia lata can be utilized for reconstructing the quadriceps tendon if required. 31 As in case of the distally based flaps, a delay procedure will ensure better survival of the flap. A venous augmentation may be done by repairing the cut end of vein to a local vein to prevent possible venous congestion. 32
To reduce the bulk, an adipofascial flap can be raised which reduces the bulk of the flap and can be covered with a skin graft 33 ( Fig. 5A-B ).
Fig. 5.

( A ) Defect over knee joint. ( B ) Defect covered with reverse anterolateral thigh flap—postoperative photo.
Reverse Flow Split Vastus Lateralis Musculocutaneous Flap
The descending branch of lateral circumflex femoral artery descends up to the knee to anastomose with superior lateral genicular artery and has perforators at 3, 7, and 10 cm above the superior border of patella. The flap is designed based on these perforators. The musculocutaneous perforator along with the descending branch of lateral circumflex femoral artery is harvested along with a cuff of vastus lateralis muscle and the overlying skin and turned over to cover the knee defect. The donor site can be primarily closed or grafted as the case may be. 34
Free Flaps
When the defects are large and when the local flap options are either not available or used up, free flaps are chosen. The commonly used free flaps are the latissimus dorsi muscle flap and the ALT flap.
The recipient vessels have to be chosen according to the availability. The major vessels like superficial femoral vessels and popliteal vessels can be used and the anastomosis to these can performed in end to side fashion. 35 The tibial vessels lie deep and can be exposed by using a posterior incision and splitting the gastrocnemius and soleus muscles in prone position and used as recipient vessels. Descending branch of lateral circumflex femoral artery too has been used.
The other vessels nearby are medial sural artery which supplies the medial belly of gastrocnemius which can be detached and used. Descending genicular branch of the femoral artery which runs in the adductor canal can be used to attach the free flap. 36 These obviate the need for changing the position of the patient during surgery as they can be exposed in the supine position ( Fig. 5A–D ).
In case there is no ideal vessel nearby, procedures like vessel loops and vein grafts have been described but the failure rate is more with them. 1
Miscellaneous Skin Flaps
Medial Sural Artery Flap
This is based on the perforators which arise from the medial belly of the gastrocnemius. These arise between 8 and 12 cm in the line joining the midpoint of popliteal crease and the medial malleolus. The perforator is identified preoperatively by Doppler and later surgically by going through an exploratory incision. The skin island is raised based on the same. The perforator is followed through the muscle carefully by splitting the muscle and dissected proximally which can be traced up to the origin of the vessel. This gives a reliable pedicled flap for coverage of small-to-moderate sized defects. 37 38
Saphenous Flap
This is based on the saphenous artery which arises from the descending genicular vessels. This is flap which has thin pliable tissue on the medial aspect of knee and upper leg. This is more often used as a free flap and can also be used as a pedicled flap for defects around the knee. The saphenous artery is identified by its close proximity to saphenous nerve. But there are variations in anatomy with origin of this artery arising from superficial femoral artery in some patients. 39 Similar to medial sural artery flap this can also be raised as a pedicled flap to cover the knee defects.
Lateral Sural Cutaneous Artery Flap
This flap is based on the lateral sural cutaneous artery which branches directly from the popliteal artery at the level of lateral condyle. This accompanies the lateral sural cutaneous nerve (arising from common peroneal nerve), pierces the fascia, and descends along the posterior border of fibula. The dissection starts distally raising along with the nerve and vein including the fascia going proximally up to the origin. This can cover the defects around the knee and is reliable. 40
Pedicled Perforator Flaps/Propeller Flaps
Skin flaps may be raised based on any perforator which is found around the knee joint. After the initial exploration of the area, a good-sized perforator is found based on which the skin island is turned around to reach the defect in the knee. The following flaps are some constant perforators.
ALT Perforator Flap
When the defect extends proximally from the knee destroying the perforator from the lateral genicular artery and anastomosis around the knee joint, it will not be possible to use the reverse ALT flap cover. In such a situation if the distal perforators from the descending branch of the lateral circumflex femoral artery are intact, a flap can be designed on it and rotated 180 degree like a propeller flap to cover the defect over the knee. Extending the dissection into the muscle will help to avoid the kinking of the pedicle and increasing the reach. 41
Lateral Supragenicular Artery Perforator Flap
One such flap is lateral supragenicular artery perforator flap which has a constant anatomy and is located around 5.3 cm from the superolateral corner of patella. This is marked by Doppler preoperatively and then isolated by surgical dissection. The flap can go up to the mid-thigh level. 42
Pedicled Vastus Medialis Perforator Flap
This is based on cutaneous perforator from the large muscular branch of vastus medialis muscle from superficial femoral artery which traverses through the muscle and called medial vastus medialis artery. The perforator site is relatively constant and located ~9 cm proximal to the adductor tubercle. A line is drawn from mid-inguinal point to medial femoral condyle. From the midpoint of this line, another line is drawn to midpoint of superior border of patella. The perforator is located along this line and marked with Doppler and used for designing the flap. 43 44
Postoperative Rehabilitation
As the defects are over or around the mobile joint, they are immobilized postoperatively for a period of 2 to 3 weeks to allow the flap or the skin graft to heal well. As there is injury to the periarticular structures like the ligaments and the capsule, the chances of stiffness are high. Mobilization is started as soon as healing is achieved. In case repair or reconstruction of deeper structures like ligamentum patellae or quadriceps tendon has been done physiotherapy may be done as per the needs of the repaired structures. The extent of movement gained is dependent on the injury to deeper structures and scarring.
Summary
Defects around the knee require careful assessment of the size of the defect and the condition of the surrounding skin and muscles to decide on the type of flap which is chosen to cover them. The flaps can be raised from the leg or thigh based on the size needed or the pattern of injury. In case both are injured, we need to use distant flaps in form of free flaps depending on the condition of the vessels. Prompt and early coverage of the knee with good pliable flap will go a long way in retaining good mobility of the joint.
Fig. 6.

( A ) Defect over the knee joint. ( B ) Defect with free anterolateral thigh flap. ( C ) Postoperative photo—front view. ( D ) Postoperative photo—medial view.
Footnotes
Conflict of Interest None declared.
References
- 1.Gravvanis A, Kyriakopoulos A, Kateros K, Tsoutsos D. Flap reconstruction of the knee: a review of current concepts and a proposed algorithm. World J Orthop. 2014;5(05):603–613. doi: 10.5312/wjo.v5.i5.603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Salgado C J, Mardini S, Jamali A A, Ortiz J, Gonzales R, Chen H C. Muscle versus nonmuscle flaps in the reconstruction of chronic osteomyelitis defects. Plast Reconstr Surg. 2006;118(06):1401–1411. doi: 10.1097/01.prs.0000239579.37760.92. [DOI] [PubMed] [Google Scholar]
- 3.Buono P, Castus P, Dubois-Ferrière V. Muscular versus non-muscular free flaps for soft tissue coverage of chronic tibial osteomyelitis. World J Plast Surg. 2018;7(03):294–300. doi: 10.29252/wjps.7.3.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cherubino M, Corno M, D'Arpa S.Muscle versus fasciocutaneous flap in lower limb reconstruction: is there a best option? J Reconstr Microsurg 201733(S 01)S27–S33. [DOI] [PubMed] [Google Scholar]
- 5.Cho E H, Shammas R L, Carney M J. Muscle versus fasciocutaneous free flaps in lower extremity traumatic reconstruction: a multicenter outcomes analysis. Plast Reconstr Surg. 2018;141(01):191–199. doi: 10.1097/PRS.0000000000003927. [DOI] [PubMed] [Google Scholar]
- 6.Akhtar M S, Khan A H, Khurram M F, Ahmad I. Inferiorly based thigh flap for reconstruction of defects around the knee joint. Indian J Plast Surg. 2014;47(02):221–226. doi: 10.4103/0970-0358.138954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chang N, Mathes S J. Comparison of the effect of bacterial inoculation in musculocutaneous and random-pattern flaps. Plast Reconstr Surg. 1982;70(01):1–10. doi: 10.1097/00006534-198207000-00001. [DOI] [PubMed] [Google Scholar]
- 8.Le Nen D, Hu W, Liot M, Moineau G, Gerard R. Gastrocnemius medial flaps. Interact Surg. 2007;1:1–10. [Google Scholar]
- 9.Veber M, Vaz G, Braye F. Anatomical study of the medial gastrocnemius muscle flap: a quantitative assessment of the arc of rotation. Plast Reconstr Surg. 2011;128(01):181–187. doi: 10.1097/PRS.0b013e318217423f. [DOI] [PubMed] [Google Scholar]
- 10.Babu N V, Chittaranjan S, Abraham G, Bhattacharjee S, Prem H, Korula R J. Reconstruction of the quadriceps apparatus following open injuries to the knee joint using pedicled gastrocnemius musculotendinous unit as bridge graft. Br J Plast Surg. 1994;47(03):190–193. doi: 10.1016/0007-1226(94)90053-1. [DOI] [PubMed] [Google Scholar]
- 11.Keller A, Allen R, Shaw W. The medial gastrocnemius muscle flap: a local free flap. Plast Reconstr Surg. 1984;73(06):974–976. doi: 10.1097/00006534-198406000-00025. [DOI] [PubMed] [Google Scholar]
- 12.Salibian A H, Rogers F R, Lamb R C. Microvascular gastrocnemius muscle transfer to the distal leg using saphenous vein grafts. Plast Reconstr Surg. 1984;73(02):302–307. doi: 10.1097/00006534-198402000-00030. [DOI] [PubMed] [Google Scholar]
- 13.Bashir A H. Inferiorly-based gastrocnemius muscle flap in the treatment of war wounds of the middle and lower third of the leg. Br J Plast Surg. 1983;36(03):307–309. doi: 10.1016/s0007-1226(83)90049-8. [DOI] [PubMed] [Google Scholar]
- 14.Agarwal P, Dawar R, Yadav P. The segmental gastrocnemius muscles’ flap: a cadaveric study. J Plast Reconstr Aesthet Surg. 2011;64(09):1202–1206. doi: 10.1016/j.bjps.2011.04.011. [DOI] [PubMed] [Google Scholar]
- 15.Hyodo I, Nakayama B, Takahashi M, Toriyama K, Kamei Y, Torii S. The gastrocnemius with soleus bi-muscle flap. Br J Plast Surg. 2004;57(01):77–82. doi: 10.1016/j.bjps.2003.10.008. [DOI] [PubMed] [Google Scholar]
- 16.Wagner T, Hupkens P, Slater N J, Ulrich D JO. The proximally based long peroneal muscle turnover flap: a novel salvage flap for small to medium-sized defects of the knee. J Plast Reconstr Aesthet Surg. 2016;69(04):533–537. doi: 10.1016/j.bjps.2015.11.012. [DOI] [PubMed] [Google Scholar]
- 17.Tobin G R. Vastus medialis myocutaneous and myocutaneoustendinous composite flaps. Plast Reconstr Surg. 1985;75(05):677–685. doi: 10.1097/00006534-198505000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Mitsala G, Varey A H, O'Neill J K, Chapman T W, Khan U. The distally pedicled gracilis flap for salvage of complex knee wounds. Injury. 2014;45(11):1776–1781. doi: 10.1016/j.injury.2014.06.019. [DOI] [PubMed] [Google Scholar]
- 19.Wang Y, Bégué T, Masquelet A C. Anatomic study of the distally based vastus lateralis muscle flap. Plast Reconstr Surg. 1999;103(01):101–103. doi: 10.1097/00006534-199901000-00017. [DOI] [PubMed] [Google Scholar]
- 20.Swartz W M, Ramasastry S S, McGill J R, Noonan J D. Distally based vastus lateralis muscle flap for coverage of wounds about the knee. Plast Reconstr Surg. 1987;80(02):255–265. doi: 10.1097/00006534-198708000-00016. [DOI] [PubMed] [Google Scholar]
- 21.Auregan J C, Bégué T, Tomeno B, Masquelet A C. Distally-based vastus lateralis muscle flap: a salvage alternative to address complex soft tissue defects around the knee. Orthop Traumatol Surg Res. 2010;96(02):180–184. doi: 10.1016/j.rcot.2010.02.013. [DOI] [PubMed] [Google Scholar]
- 22.Rao A J, Kempton S J, Erickson B J, Levine B R, Rao V K. Soft tissue reconstruction and flap coverage for revision total knee arthroplasty. J Arthroplasty. 2016;31(07):1529–1538. doi: 10.1016/j.arth.2015.12.054. [DOI] [PubMed] [Google Scholar]
- 23.Ihara J, Imanishi N, Kishi K. Venous anastomosis for prevention of venous congestion in distally based flaps. Plast Reconstr Surg Glob Open. 2017;5(12):e1585. doi: 10.1097/GOX.0000000000001585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Clavert P, Cognet J M, Baley S. Anatomical basis for distal sartorius muscle flap for reconstructive surgery below the knee. Anatomical study and case report. J Plast Reconstr Aesthet Surg. 2008;61(01):50–54. doi: 10.1016/j.bjps.2006.01.059. [DOI] [PubMed] [Google Scholar]
- 25.Shen Y M, Yu D N, Hu X H, Qin F J, Li M, Ning F G. Repairing proximal and middle lower-leg wounds with retrograde sartorius myocutaneous flap pedicled by perforating branches of medial inferior genicular artery or posterior tibial artery. J Plast Reconstr Aesthet Surg. 2012;65(09):1158–1164. doi: 10.1016/j.bjps.2012.03.041. [DOI] [PubMed] [Google Scholar]
- 26.Feldman J J, Cohen B E, May J W., Jr The medial gastrocnemius myocutaneous flap. Plast Reconstr Surg. 1978;61(04):531–539. doi: 10.1097/00006534-197804000-00006. [DOI] [PubMed] [Google Scholar]
- 27.McCraw J B, Fishman J H, Sharzer L A. The versatile gastrocnemius myocutaneous flap. Plast Reconstr Surg. 1978;62(01):15–23. doi: 10.1097/00006534-197807000-00002. [DOI] [PubMed] [Google Scholar]
- 28.Innocenti M, Cardin-Langlois E, Menichini G, Baldrighi C. Gastrocnaemius-propeller extended miocutanous flap: a new chimaeric flap for soft tissue reconstruction of the knee. J Plast Reconstr Aesthet Surg. 2014;67(02):244–251. doi: 10.1016/j.bjps.2013.10.011. [DOI] [PubMed] [Google Scholar]
- 29.Zhou G, Zhang Q-X, Chen G-Y. The earlier clinic experience of the reverse-flow anterolateral thigh island flap. Br J Plast Surg. 2005;58(02):160–164. doi: 10.1016/j.bjps.2004.10.011. [DOI] [PubMed] [Google Scholar]
- 30.Pan S C, Yu J C, Shieh S J, Lee J W, Huang B M, Chiu H Y. Distally based anterolateral thigh flap: an anatomic and clinical study. Plast Reconstr Surg. 2004;114(07):1768–1775. doi: 10.1097/01.prs.0000142416.91524.4c. [DOI] [PubMed] [Google Scholar]
- 31.Demirseren M E, Efendioglu K, Demiralp C O, Kilicarslan K, Akkaya H. Clinical experience with a reverse-flow anterolateral thigh perforator flap for the reconstruction of soft-tissue defects of the knee and proximal lower leg. J Plast Reconstr Aesthet Surg. 2011;64(12):1613–1620. doi: 10.1016/j.bjps.2011.06.047. [DOI] [PubMed] [Google Scholar]
- 32.Yeh H-K, Hsu C-C, Lin C-H. Reverse-flow anterolateral thigh flap without antegrade venous reconstruction for knee soft-tissue reconstruction. Formosan Journal of Surgery. 2015;48:21–25. [Google Scholar]
- 33.Wang X C, Lu Q, Li X F. Reversed anterolateral thigh adipofascial flap for knee and proximal calf defects. Burns. 2008;34(06):868–872. doi: 10.1016/j.burns.2007.09.015. [DOI] [PubMed] [Google Scholar]
- 34.Sahasrabudhe P, Panse N, Baheti B, Jadhav A, Joshi N, Chandanwale A. Reconstruction of complex soft-tissue defects around the knee joint with distally based split vastus lateralis musculocutaneous flap: a new technique. J Plast Reconstr Aesthet Surg. 2015;68(01):35–39. doi: 10.1016/j.bjps.2014.09.034. [DOI] [PubMed] [Google Scholar]
- 35.Hierner R, Reynders-Frederix P, Bellemans J, Stuyck J, Peeters W. Free myocutaneous latissimus dorsi flap transfer in total knee arthroplasty. J Plast Reconstr Aesthet Surg. 2009;62(12):1692–1700. doi: 10.1016/j.bjps.2008.07.038. [DOI] [PubMed] [Google Scholar]
- 36.Venkatramani H, Sabapathy S R, Nayak S. Free-flap cover of complex defects around the knee using the descending genicular artery as the recipient pedicle. J Plast Reconstr Aesthet Surg. 2014;67(01):93–98. doi: 10.1016/j.bjps.2013.09.011. [DOI] [PubMed] [Google Scholar]
- 37.Cavadas P C, Sanz-Giménez-Rico J R, Gutierrez-de la Cámara A, Navarro-Monzonís A, Soler-Nomdedeu S, Martínez-Soriano F.The medial sural artery perforator free flap Plast Reconstr Surg 2001108061609–1615.discussion 1616–1617 [DOI] [PubMed] [Google Scholar]
- 38.Shim J S, Kim H H.A novel reconstruction technique for the knee and upper one third of lower leg J Plast Reconstr Aesthet Surg 20065909919–926.discussion 927 [DOI] [PubMed] [Google Scholar]
- 39.Sananpanich K, Atthakomol P, Luevitoonvechkij S, Kraisarin J. Anatomical variations of the saphenous and descending genicular artery perforators: cadaveric study and clinical implications for vascular flaps. Plast Reconstr Surg. 2013;131(03):363e–372e. doi: 10.1097/PRS.0b013e31827c7067. [DOI] [PubMed] [Google Scholar]
- 40.Li Z, Liu K, Lin Y, Li L. LI. Lateral sural cutaneous artery island flap in the treatment of soft tissue defects at the knee. Br J Plast Surg. 1990;43(05):546–550. doi: 10.1016/0007-1226(90)90118-j. [DOI] [PubMed] [Google Scholar]
- 41.Chen C Y, Hsieh C H, Kuo Y R, Jeng S F. An anterolateral thigh perforator flap from the ipsilateral thigh for soft-tissue reconstruction around the knee. Plast Reconstr Surg. 2007;120(02):470–473. doi: 10.1097/01.prs.0000267432.03348.97. [DOI] [PubMed] [Google Scholar]
- 42.Nguyen A T, Wong C, Mojallal A, Saint-Cyr M. Lateral supragenicular pedicle perforator flap: clinical results and vascular anatomy. J Plast Reconstr Aesthet Surg. 2011;64(03):381–385. doi: 10.1016/j.bjps.2010.05.029. [DOI] [PubMed] [Google Scholar]
- 43.Zheng H-P, Lin J, Zhuang Y-H, Zhang F-H. Convenient coverage of soft-tissue defects around the knee by the pedicled vastus medialis perforator flap. J Plast Reconstr Aesthet Surg. 2012;65(09):1151–1157. doi: 10.1016/j.bjps.2012.03.027. [DOI] [PubMed] [Google Scholar]
- 44.Clavero J´A . Moscatiello F, Masià J, Carrera A, Larrañaga J R, Pons G. The ‘propeller’ distal anteromedial thigh perforator flap. Anatomic study and clinical applications. J Plast Reconstr Aesthet Surg. 2007;60(12):1323–1330. doi: 10.1016/j.bjps.2007.02.027. [DOI] [PubMed] [Google Scholar]