

Abstract
HIV‐exposed and HIV‐uninfected (HEU) infants may be at increased risk of poor health and growth outcomes. We characterized infant growth trajectories in a cohort of HEU infants to identify factors associated with healthy growth. HIV‐positive women participating in prevention of mother‐to‐child HIV transmission programmes in Kigali, Rwanda, were followed until their infants were 2 years old. Infant anthropometrics were regularly collected. Latent class analysis was used to categorize infant growth trajectories. Multiple logistic regression was used to estimate the odds of infants belonging to each growth trajectory class. On average, this population of HEU infants had moderate linear growth faltering, but only modest faltering in weight, resulting in mean weight‐for‐length z‐score (WLZ) above the World Health Organization (WHO) median. Mean WLZ was 0.53, and mean length‐for‐age z‐score (LAZ) was −1.14 over the first 2 years of life. We identified four unique WLZ trajectories and seven trajectories in LAZ. Low neonatal weight‐for‐age and a high rate of illness increased the likelihood that infants were in the lightest WLZ class. Shorter mothers were more likely to have infants with linear growth faltering. Female infants who were older at the end of exclusive breastfeeding were more likely to be in the second tallest LAZ class. In conclusion, the current WHO recommendations of Option B+ and extended breastfeeding may induce higher WLZ and lower LAZ early in infancy. However, there is considerable heterogeneity in growth patterns that is obscured by simply analysing average growth trends, necessitating the analysis of growth in subpopulations.
Keywords: growth, HIV, LAZ, Option B+, WLZ
Key messages.
Mean growth trajectories of these HIV‐exposed and HIV‐uninfected infants show that they continue to experience meaningfully lower LAZ and elevated WLZ than the WHO standard. This pattern is not seen among other infants in low‐resource settings.
There is considerable heterogeneity in the growth trajectories of HIV‐exposed and HIV‐uninfected infants in Kigali, Rwanda.
Characteristics present at birth, such as infant sex, neonatal weight, and maternal height, are predictive of the growth trajectories of these infants.
1. INTRODUCTION
The number of HIV‐exposed and HIV‐uninfected (HEU) infants born in Africa is increasing as the wider use of antiretroviral drugs limits mother‐to‐child HIV transmission (Evans, Jones, & Prendergast, 2016; Filteau, 2009; Joint United Nations Programme on HIV/AIDS, 2013). There is already considerable evidence that HIV‐positive women on antiretroviral therapy (ART) have higher risk of experiencing adverse pregnancy outcomes than HIV‐negative women due to biological effects of the virus or drugs (Alemu, Yalew, Fantahun, & Ashu, 2015; Makasa et al., 2007; Ndirangu, Newell, Bland, & Thorne, 2012; Neri et al., 2013; Sofeu et al., 2014). Their infants may also be at additional risk of slow growth and increased morbidity and mortality due to the biological impact of HIV and ART exposure and covarying socio‐economic risk factors (Brennan et al., 2016; Filteau, Baisley, Chisenga, Kasonka, & Gibson, 2011; Pierre et al., 2016; Slogrove, 2016). Less exposure to breast milk, increased rates of maternal illness and death leading to reduced care, and lower socio‐economic status may partly explain elevated rates of morbidity and mortality among HEU infants (Arikawa, Rollins, Newell, & Becquet, 2016; Conserve et al., 2015; Evans et al., 2016; Filteau, 2009; Filteau et al., 2011; Kuhn et al., 2005; Le Roux, Abrams, Nguen, & Myer, 2016; Nicholson, Chisenga, Siame, Kasonka, & Filteau, 2015; Sugandhi et al., 2013). However, further research is necessary to fully understand growth patterns in this at risk population.
In 2012, the World Health Organization (WHO) recommended Option B+: universal, lifelong ART for all HIV‐positive pregnant and breastfeeding women. Option B+ was quickly adopted in Rwanda, where it was implemented in 2013. Before Option B+ and the WHO recommendation for continued breastfeeding of HEU infants, HEU infants were at higher risk of impaired growth than their unexposed counterparts (Evans et al., 2016; Lartey et al., 2014; Omoni et al., 2017). The prevalence of risk factors for poor growth associated with HIV is expected to decrease with the adoption of Option B+ and the WHO recommendation for continued breastfeeding among HIV‐positive mothers in low‐resource settings (Evans et al., 2016; WHO, 2016). Improved maternal health, increased ART use, and breastfeeding have decreased mortality, morbidity, and undernutrition in HEU infants (Le Roux et al., 2016). The difference in mortality rates between HEU infants and unexposed infants decreased as ART became more available (Brennan et al., 2016). Therefore, the differences in growth outcomes between HEU infants and unexposed infants could further decrease with Option B+ and the recommendation for extended breastfeeding. However, there is, as yet, little understanding of the growth patterns or the factors driving the variability in growth patterns of these infants under the current recommendations.
The objective of our study was to characterize the patterns of change in weight‐for‐length z‐score (WLZ) and length‐for‐age z‐score (LAZ) of HEU infants in Kigali, Rwanda, under current WHO recommendations. We developed growth trajectories in WLZ and LAZ to reflect the variation in growth patterns in this population of HEU infants and attempt to identify maternal and infant characteristics that predict which trajectory infants will follow. We hypothesized that HEU infant growth outcomes are approaching expected values relative to the WHO growth standards (WHO, 2011). Furthermore, we hypothesized that infant sex; neonatal weight‐for‐age z‐score (WAZ); water source; frequency of illnesses; age at the end of exclusive breastfeeding; and maternal height, parity, and education are associated with growth trajectories in these infants.
2. METHODS
2.1. Recruitment and study sample
The Kabeho Study (Kigali Antiretroviral and Breastfeeding Assessment for the Elimination of HIV) enrolled 608 HIV‐positive, pregnant/post‐partum women participating in prevention of mother‐to‐child HIV transmission programmes in selected high‐volume health facilities in Kigali, Rwanda. Women were required to have documented HIV infection, plan on remaining in the Kigali area after delivery, and provide informed consent. All women were enrolled in standard prevention of mother‐to‐child transmission (PMTCT) programmes under Option B+, which provides lifelong ART to all HIV‐positive pregnant or breastfeeding women. PMTCT programmes have active tracking of patients in the community to decrease loss to follow‐up and use performance‐based financing to encourage health teams to support adherence and provide suitable care. Prophylactic cotrimoxazole was started at 6 weeks.
2.2. Study visits and data collection
Study visits were conducted during regularly scheduled follow‐up visits for PMTCT at health facilities within 2 weeks of birth; at 6, 10, and 14 weeks; monthly from 4 to 18 months; and at 21 and 24 months. Immunizations, growth monitoring, infant feeding counselling, maternal ART dispensing, and family planning were all standard parts of these visits. Birthweight was measured by birth attendants in the clinical settings where births took place. If recorded birthweight was not available, we used measurements taken at first study visit as a measure of neonatal weight. At each visit, trained nurses took duplicate measures of infant length to the nearest centimetre using Shorr boards and weight to the nearest 10 g using UNICEF scales. HIV testing of the infants was conducted according to standard national procedures for early infant diagnosis by HIV polymerase chain reaction (PCR) or rapid HIV testing at 6 weeks, 9 months, 18 months, and 24 months by the National Reference Laboratory using Roche COBAS AmpliPrep/TaqMan (V2.0). Dried blood spots were also used to determine the infants HIV status at birth and 24 months. Mothers were asked to report whether the infant currently or since the last visit had cough, fever, diarrhoea, or oral thrush and to provide details on infant feeding including breastfeeding and feeding of all other foods and liquids.
2.3. Power calculation
The minimum sample size necessary to estimate the proportion of stunted infants was determined to be 608 mother–infant pairs under an assumption of 23.5% stunting with a precision of 4.5% (nQuery Advisor v 4.0; National Institute of Statistics, Ministry of Health, & ICF International, 2015). Ethical approvals were obtained from the Rwandan National Ethics Committee, the Rwanda National Health Research Committee, and the George Washington University Institutional Review Board. The protocol is registered with the U.S. National Institutes of Health at http://clinicaltrials.gov (NCT02295800).
2.4. Data analysis
The repeat measurements for infant length and weight were averaged at each time point and converted to z‐scores using the WHO growth standards (WHO, 2011). The WHO standard and z‐scores were used instead of raw weight and length to account for age differences at each study visit and for easy comparison with other studies that also use this standard. These standards were specifically designed to monitor trends in child growth and allow for international comparison (de Onis & Blossner, 2003). They are meant to represent expected growth of infants living under conditions that allow them to reach their full genetic potential, including with mothers who breastfeed and do not smoke (WHO, 2006). The use of this standard means that we are comparing the growth of infants in this cohort with a worldwide ideal for healthy growth rather than to other infants in the region. Stunting, wasting, and underweight were defined using the −2 standard deviation cut points.
Data analysis was conducted in R (R Core Team, 2013). Latent class models used the lcmm package to identify characteristic infant growth trajectories for WLZ and LAZ (Prost‐Lima, Phillips, Diakite, & Liquet, 2017). Latent class growth mixture models allow for the examination of heterogeneity in patterns of longitudinal outcomes within a population. They do not assume that all individuals within the sample come from the same underlying population, so they can be used to identify subpopulations that experience different patterns in longitudinal outcomes. Therefore, this method is appropriate for our research goal of identifying the variation in growth patterns that occurs within this cohort. Other studies have used latent class growth mixture modelling to identify subpopulations that grew similarly and then used class membership as a predictor of disease risk (Hoekstra, Barbosa‐Leiker, Koppes, & Twisk, 2011; Landa, Gross, Stuart, & Bauman, 2012; Rzehak et al., 2013). It is less common to use baseline characteristics to predict latent class membership (Li, Goran, Kaur, Nollen, & Ahluwalia, 2007; Mebrahtu, Feltbower, Petherick, & Parslow, 2015). Nonetheless, the same theoretical framework applies. An additional advantage of latent class analysis is that it does not require that all infants have measurements at the same ages. Although study measurements were collected at regularly scheduled follow‐up visits, mothers were not always able to attend visits at the specified ages. Our method allows for infants to be classified into trajectories even if some measurements occurred at different ages or were missing.
The LAZ models used age and age2 terms for growth; however, the WLZ models used age, age2, and age3 terms. The number of latent classes was chosen to maximize the number of possible trajectories while maintaining sufficient sample size within each class. A post hoc analysis of variance was used to examine correlations between class membership. Multinomial logistic regression was conducted in the mlogit package to identify maternal and infant characteristics associated with class membership (Crossant, 2013).
Two models were used to identify infant and maternal factors associated with WLZ and LAZ class membership. The first model included baseline (non‐time‐varying) characteristics: infant sex, maternal education, maternal height, water source, and neonatal WAZ. Water source was defined as a binary variable reflecting where the infant's household got water (a tap or an open water source). Neonatal WAZ was used instead of birthweight because birth measures took place up to a week after delivery. The second model included infant sex, maternal education, percent of observation periods during which the infant experienced an illness (percent of illness periods), and age at the end of exclusive breastfeeding. The percent of illness periods was calculated by dividing the number of times the mother reported at least one illness since the last visit by the total number of observations. Age at the end of exclusive breastfeeding was estimated as the midpoint of the time period between the visit when the mother first reported giving the infant food or water and the previous visit. Before the introduction of foods or liquids, infants are considered to be exclusively breastfed. These factors were chosen because they are known to be associated with infant growth endpoints in unexposed populations. Because HEU infants experience somewhat different risk factors than unexposed infants, known risk factors for poor growth may not have the same effect in this population. We sought to show that these variables were related, not only to endpoints but also to the path or trajectory by which infants reach their growth endpoints among HEU infants. These models were not combined so that factors determined before the period over which growth trajectories are characterized are separated from those known only after. Therefore, the first model can be interpreted as factors likely to influence growth trajectories, whereas the second reflects factors that may covary with, influence, or be influenced by growth. Each variable was tested for sex differences, and when appropriate, sex interactions were included in multivariate analysis.
3. RESULTS
3.1. Study population
Recruitment took place from April 2013 to January 2014, and 608 women were initially recruited into the study; however, 34 mothers left the study before the 6‐week visit. In addition, there were seven sets of twins, resulting in a total of 581 mother–infant pairs enrolled in the study at 6 weeks (Gill et al., 2017). Growth trajectories could be made for 578 infants included in final analysis; however, only 453 infants were retained through the entire 2 years of the study. During the course of the study, 15 infants died and the remainder were lost to follow‐up. Female infants represented 49% of the study population. The majority of women had not completed primary school (56%). Within 1 month of enrolment, all women were receiving ART. Adherence to the ART regimen was high with less than 10% of women reporting having missed one dose in the last 3 days at any of the study visits. Mothers were generally in good health, with a mean body mass index (BMI) of 25.5 at the end of the study. No women were underweight. Only 6% of women had CD4 counts less than 200. The average age at the end of exclusive breastfeeding was 4.6 months, with 80% of infants being exclusively breastfed from 3 to 4 months but only 22% being exclusively breastfed through 6 months. Only 15% of the population relied on an open water source. On average, 36% of mothers reported that their infant had been ill since the last visit.
Average LAZ was −0.48 at 6 weeks and declined steadily over most of the study period, reaching −1.55 by 24 months (Figure 1). Average WAZ decreased less rapidly than LAZ. At 6 weeks, mean WAZ was −0.05 and declined slowly in a nearly linear trend to −0.51 at 24 months. As a result, average WLZ for the first observation was 0.67 and only declined to 0.41 by 24 months. At 24 months, four (0.7%) infants were wasted, 24 (4.1%) were underweight, and 78 (13.4%) infants were stunted.
Figure 1.
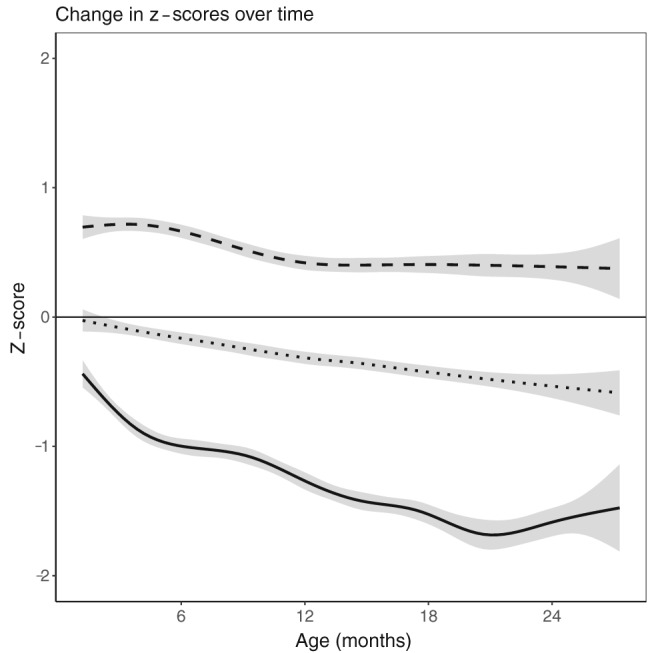
Average anthropometric values for weight‐for‐length z‐score (dotted), weight‐for‐age z‐score (dashed), and length‐for‐age z‐score (solid). Grey shaded area represents 95% confidence interval
3.2. Latent class analysis
Figure 2 shows mean growth trajectories of each class for WLZ and LAZ. Three of the four WLZ classes have z‐scores near 1 at 6 weeks but quickly diverge. The outlying class, Class 4, has a lower initial WLZ, which declines until about 9 months. This pattern is markedly different from that of Class 1, which gains weight rapidly and maintains an average z‐score above 2 from 9 to 24 months.
Figure 2.
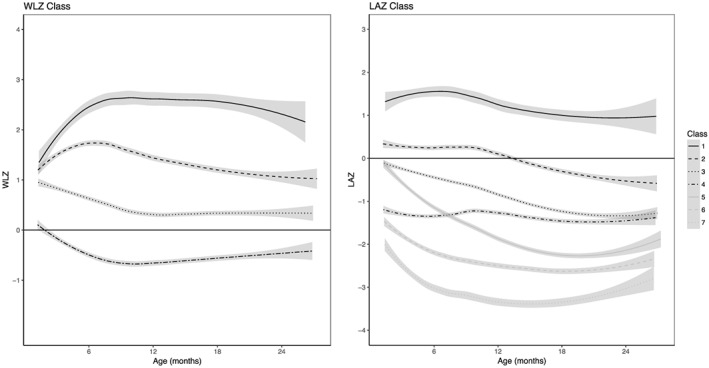
Growth trajectories of infants from 6 to 24 months according to latent class analysis. Classes are numbered such that the class with the largest number of infants at birth is Class 1. Grey shaded area represents 95% confidence interval. WLZ: weight‐for‐length z‐score; LAZ: length‐for‐age z‐score
Growth trajectories in LAZ are more variable than WLZ, resulting in more classes. LAZ Classes 1 and 4 show little change in z‐score over time. Classes 6 and 7 have z‐scores below −1 at 6 weeks and experience parallel declines before slight recoveries. Class 5 has an early, average LAZ near 0, but z‐score rapidly declines, dropping below Class 4 and falling to −2.21 by 18 months. In contrast, Class 1 has a LAZ of 1.83 at 6 weeks and experiences only a slight decline to 0.98 by 24 months.
Class membership for WLZ and LAZ is correlated (P value: 0.04). Infants in heavier WLZ classes also tend to be in taller LAZ classes; infants that are large in terms of weight also tend to be large in terms of height. However, there are 14 infants in the heaviest WLZ class and an LAZ class (Class 5, 6, or 7) that became stunted.
3.3. Predictors of class membership
Male infants have an increased likelihood of being in the class that develops the highest WLZ (Table 1). Infants with high neonatal WAZ and firstborn infants are more likely to be in the second highest WLZ class. Infants with low neonatal WAZ have an increased likelihood of being in the lowest WLZ class and the two lowest LAZ classes. Shorter mothers are more likely to have infants that experience linear growth faltering; however, females have taller mothers than males in this class (Table 2).
Table 1.
Odds of weight‐for‐length z‐score class membership by infant characteristics and life events
| Class 1 | Class 2 | Class 3 | Class 4 | |
|---|---|---|---|---|
| Odds of class membership by infant characteristics | ||||
| Sex | −1.11 (−2.05, −0.18) | −0.23 (−0.71, 0.24) | Ref | 0.1 (−0.38, 0.58) |
| Firstborn | 0.89 (0.02, 1.75) | 0.57 (0.06, 1.07) | Ref | −0.006 (−0.34, 0.70) |
| Maternal education | 0.06 (−0.14, 0.25) | 0.06 (−0.05, 0.16) | Ref | −0.006 (−0.12, 0.11) |
| Neonatal WAZ | 0.22 (−0.12, 0.55) | 0.35 (0.15, 0.55) | Ref | −0.21 (−0.40, −0.03) |
| Water source | 0.04 (−1.27, 1.34) | 0.48 (−0.16, 1.12) | Ref | −1.13 (−2.06, −0.20) |
| Maternal height | 0.04 (−0.03, 0.11) | 0.002 (−0.04, 0.04) | Ref | 0.009 (−0.03, 0.05) |
| Odds of class membership by infant life events | ||||
| Sex | −0.82 (−1.68, 0.04) | −0.13 (−0.59, 0.33) | Ref | 0.18 (−0.10,0.12) |
| Maternal education | 0.03 (−0.16, 0.21) | 0.02 (−0.08, 0.44) | Ref | 0.01 (0.28, 2.70) |
| Proportion of visits ill | −1.89 (−4.21, 0.44) | −0.5 (−1.74, 0.74) | Ref | 1.49 (0.28, 2.70) |
| Intro. to compl. feeding | 0.04 (−0.27, 0.35) | 0.09 (−0.08, 0.26) | Ref | 0.05 (−0.12, 0.23) |
Note. WAZ: weight‐for‐age z‐score.
Numbers in bold are P < 0.05.
Table 2.
Odds of length‐for‐age z‐score class membership by infant characteristics and life events
| Class 1 | Class 2 | Class 3 | Class 4 | Class 5 | Class 6 | Class 7 | |
|---|---|---|---|---|---|---|---|
| Odds of class membership by infant characteristics | |||||||
| Sex | −23.79 (−60.17, 15.60) | −0.4 (−18.54, 17.74) | Ref | −5.47 (−22.56, 11.61) | −20.52 (−38.45, −2.61) | 0.09 (−18.30, 18.12) | −12.65 (−44.46, 19.14) |
| Firstborn | −2.58 (−1.47, 0.95) | −0.09 (−0.73, 0.55) | Ref | −0.14 (−0.78, 0.49) | −0.51 (−1.22, 0.19) | −0.05 (−0.72, 0.62) | −0.05 (−1.05, 0.95) |
| Maternal education | −0.08 (−0.39, 0.24) | 0.02 (−0.12, 0.17) | Ref | 0.08 (−0.05, 0.21) | 0.03 (−0.19, 0.10) | −0.5 (−0.48, 0.02) |
−0.02 −0.13 |
| Neonatal WAZ | 0.23 (−0.27, 0.73) | −0.1 (0.35, 0.16) | Ref | −0.41 (−0.65, −0.16) | −0.1 (−0.36, 0.16) | −0.69 (−0.95, −0.43) | −1.06 (−1.47, −0.66) |
| Water source | −0.15 (−331.65, 3285.75) | 0.19 (−1.05, 0.94) | Ref | 0.31 (−0.71, 1.08) | 0.72 (−0.15, 1.59) | 0.31 (−0.61, 1.23) | −1.47 (−3.65, 0.72) |
| Maternal height | 0.19 (−0.00009, 0.38) | 0.07 (−0.02, 0.16) | Ref | −0.06 (−0.15, 0.02) | −0.11 (−0.19, −0.03) | −0.11 (−0.19, −0.03) | −0.19 (−3.00, 0.09) |
| Maternal Height × Sex | 0.15 (−0.09, 0.39) | 0.002 (−0.11,0.12) | Ref | 0.03 (−0.07, 0.14) | 0.12 (0.01, 0.24) | −0.007 (−0.12, 0.11) | 0.07 (−0.14, 0.27) |
| Odds of class membership by infant life events | |||||||
| Sex | 1.72 (−3.56, 6.00) | −2.14 (−4.63, −0.15) | Ref | 1.3 (−3.49, 0.90) | −2.28 (−4.73, −0.27) | −1.31 (−3.52, 1.06) | 1.82 (−6.11, 0.74) |
| Maternal education | −0.07 (−0.33, 0.25) | 0.02 (−0.11, 0.17) | Ref | 0.07 (−0.04, 0.22) | 0.07 (−0.07, 0.22) | 0.03 (−0.11, 0.17) | −0.16 (−0.50, 0.003) |
| Proportion of visits ill | −0.77 (−3.78, 2.57) | 0.88 (−2.15, 1.06) | Ref | 0.38 (−1.99, 1.11) | 0.76 (−0.71, 2.43) | 0.63 (−0.86, 2.31) | 0.22 (−1.48, 2.72) |
| Intro. to compl. feeding | 0.29 (−0.43, 0.98) | −0.31 (−0.70, 0.04) | Ref | −0.24 (−0.58, 0.14) | −0.33 (−0.68, 0.006) | 0.14 (−0.45, 0.23) | −0.16 (−0.52, 0.30) |
| Intro. to Compl. Feeding × Sex | −0.4 (−1.25, 0.59) | 0.42 (0.003, 0.92) | Ref | 0.24 (−0.21, 0.68) | 0.3 (−0.13, 0.79) | 0.08 (−0.40, 0.53) | 0.08 (−0.48, 0.90) |
Note. WAZ: weight‐for‐age z‐score.
Numbers in bold are P < 0.05.
Regardless of breastfeeding status, infants with a higher percent of illness periods are more likely to be in the lowest WLZ class (Table 1). Among female infants, delaying the end of exclusive breastfeeding was related to increased odds of being in the second tallest LAZ class (Table 2).
4. DISCUSSION
4.1. Mean growth trends
In the context of Option B+ and extended breastfeeding, these HEU infants develop elevated weight‐for‐length, but linear growth remained well below the WHO standard. In contrast, infants in low‐ and middle‐income countries worldwide tend to have roughly equivalent decreases in weight and length for the first year of life relative to the WHO standard (Victora, de Onis, Hallal, Blossner, & Shrimpton, 2010). This results in the average weight‐for‐length of infants in these low‐resource environments being slightly below 0. After 1 year, in low‐ and middle‐income contexts, linear growth decreases more than ponderal growth and weight‐for‐length increases slightly. However, study infants exhibited greater length than weight deficits from birth, resulting in WLZ averaging about 0.5 standard deviations above the WHO median. As such, we conclude that these HEU infants have unique growth trajectories that are not observed in other infants in resource‐restricted settings.
Compared with the Rwandan population, as represented in the 2015 Rwanda Demographic and Health Survey (DHS), these HEU infants have lower early LAZ and elevated early WLZ; however, their growth patterns converge towards the national means over time (National Institute of Statistics, Ministry of Health, & ICF International, 2015). The DHS mean LAZ was −0.7 at 6–8 months and −1.8 by 18–23 months. In the Kabeho sample, mean LAZ was −1.02 at 6–8 months but only declined to −1.66 by 18–23 months. The DHS mean WLZ was 0.3 at 6–8 months and remained the same at 18–23 months. Mean WLZ in Kabeho infants was 0.63 at 6–8 months and declined to 0.38 at 18–23 months. These data show that HEU infants do not follow the average growth trajectory of other infants in their geographic area.
Differences in growth between infants in the Kabeho Study and the broader Rwandan population could, in theory, be related to continued lower rates of breastfeeding among HIV‐positive women despite current recommendations. Rwandan mothers and women in this study both engage in intensive and prolonged breastfeeding (National Institute of Statistics, Ministry of Health, & ICF International, 2015). However, in Rwanda, exclusive breastfeeding occurs for 5.4 months on average, but in Kabeho, exclusive breastfeeding ends almost a month earlier on average. Among the broader Rwandan population, any breastfeeding continues for more than 28 months on average. In contrast, in the Kabeho Study, only 5% of infants were still breastfed at 24 months. Nonetheless, studies in Malawi failed to find an association between breastfeeding and infant WLZ (Kamudoni, Maleta, Shi, & Holmboe‐Ottesen, 2015; Kuchenbecker et al., 2015). In addition, in a randomized controlled trial in Kenya, there was no difference in the risk of stunting, underweight, or wasting between HEU infants who were breastfed or formula fed. These results indicate that our findings may not be driven by differences in breastfeeding (McGarth et al., 2012). However, in Bhutan, breastfeeding proved to be protective against infant overweight status (Campbell, Kang, & West, 2017). Therefore, if breastfeeding were to have an effect, it would likely be in the opposite direction from what we observed.
The pattern of low early LAZ and elevated early WLZ relative to unexposed infants in the same setting was not seen in studies that occurred before the widespread availability of ART. In Ghana, infants born to HIV‐positive women and treated with nevirapine had consistently lower LAZ from birth to 12 months than infants born to HIV‐negative women; however, there was no difference in WLZ by HIV exposure status (Lartey et al., 2014). These infants did not have the elevated WLZ observed in our population. In Zimbabwe before the availability of ART, HEU infants had higher risk of stunting and wasting, but growth trajectories in LAZ and WLZ were not meaningfully different from unexposed infants over the first 2 years of life (Omoni et al., 2017). HEU infant WLZ was lower than unexposed infants WLZ in this setting, whereas we find that HEU infant WLZ is higher than the average WLZ of Rwanda as a whole. In Zimbabwe case, both unexposed and HEU infants had slightly elevated WLZ at 3 months, but this rapidly declined to approximately 0. In the absence of ART, mean LAZ, WAZ, and WLZ were all close to −1 by 24 months in Kenya (McGarth et al., 2012). Under these conditions, formula feeding was protective against slow growth. In Tanzania before the widespread availability of ART but with nearly universal breastfeeding, 24‐month LAZ was nearly −2 and WLZ was below −1 (Webb, Manji, Fawzi, & Villamor, 2009). As such, we conclude that this pattern of low LAZ combined with elevated WLZ is unique to HEU infants in the modern era of PMTCT practices.
The mean growth patterns observed in these HEU infants are consistent with previous work in HEU infants exposed to ART. A similar study in Malawi found high average BMI z‐score and declining LAZ from 24 to 48 weeks (Flax et al., 2013). These infants were part of an intervention study that counselled women to exclusively breastfeed for 6 months, and in the majority of cases, either the mother or the infant received ART. In a Zambian study in which mothers received single dose nevirapine, average LAZ was below −2.2 and WAZ was about −1.2, resulting in a higher average WLZ of −0.1 by 21 months (Arpadi et al., 2009). WLZ and WAZ were significantly higher in breastfed infants compared with infants that had stopped breastfeeding from 4 to 15 months. In both of these studies, the combination of ART and breastfeeding resulted in a higher WAZ relative to LAZ and, therefore, much higher weight relative to height. One study in Botswana among breastfed infants whose mothers received either highly active ART or zidovudine found a different pattern, with WAZ lower than LAZ and WLZ of approximately 0 (Powis et al., 2011). However, this study was restricted to 0 to 6 months. Together, these results show that breastfeeding and ART may increase WLZ in HEU infants. Nonetheless, ART and breastfeeding are not sufficient to promote a healthy LAZ among HEU infants.
4.2. Variation in growth trends
The considerable heterogeneity in growth patterns demonstrated in our population through the latent class analysis highlights the importance of our approach. Mean growth trends do not adequately describe the actual variation in growth that occurs within this population. Classes exhibit a variety of patterns with some LAZ classes barely decreasing in z‐score, whereas others fall considerably. One WLZ class has a large decrease in z‐score, whereas the others remain above 0 throughout the entire study period. In addition, the 14 infants in both the highest WLZ class and the growth faltering LAZ classes show that these growth trajectories can have unusual combinations and different determinants may influence growth in both LAZ and WLZ.
To our knowledge, only one other paper has attempted to classify and predict growth trajectories within infants in low‐income settings (Gough et al., 2016). This paper examined growth in non‐HEU infants in Zimbabwe using cluster analysis. Similar to our findings, authors report that infants with greater birthweight, birth length, and taller mothers were more likely to be in LAZ growth classes with healthier trajectories. In addition, among these Zimbabwean infants, males were more likely than females to be in the most growth‐restricted groups. In our population, males were at increased odds of being in the class that had normal weight near birth then experienced growth faltering. No studies have examined patterns in WLZ trajectories.
The likelihood of growth trajectory membership varied by infant sex, neonatal WAZ, maternal height, percent illness periods, and age at the end of exclusive breastfeeding. Males, infants with taller mothers, or those with higher neonatal WAZ were more likely to grow quickly in terms of relative weight. Similarly, one study of HEU infants in Malawi found that BMI z‐score was positively associated with maternal height, but not with infant sex (Flax et al., 2013). However, another study, also in HIV‐exposed infants in Malawi, found that males had higher WLZ than females, after adjusting for HIV status (Taha et al., 2010). Maternal height was low in classes that became stunted. This is consistent with previous work that found maternal height to be associated with stunting in HEU infants (Flax et al., 2013; McGarth et al., 2012).
Study infants with a higher percent of illness periods had increased odds of being in the lowest WLZ class. Among HIV‐exposed infants in Tanzania, an illness episode since the last measurement was also associated with a decline in WLZ but not LAZ, independent of the infant's HIV status (Webb et al., 2009). Among HEU infants in Kenya, incidence of diarrhoea was associated with increased hazard of wasting (McGarth et al., 2012). Additionally, among females, ending exclusive breastfeeding at an older age was associated with an increased likelihood of the second tallest LAZ class. Among study infants, 81% of infants were exclusively breastfed between 3 and 4 months, and this may have been an important contributor to their modest weight deficits at (WAZ = −0.16) at 4 months. Similarly, among HIV‐exposed infants in Malawi, breastfeeding was associated with higher LAZ and WLZ after controlling for infant HIV status (Taha et al., 2010). However, in Zambia, the early cessation of breastfeeding among HEU infants had little impact on LAZ but was associated with a decrease in WLZ (Arpadi et al., 2009).
4.3. Limitations
There are several limitations to this study. Our sample size may be too small to detect effects for certain classes with smaller numbers, and many infants do not have data at all‐time points, making some analyses less powerful. There was some loss to follow‐up, which could result in biases estimates of growth values later in life. However, infants who were subsequently lost had no difference in growth outcomes from those who remained in the study. In addition, because these are observational data, there can be no proof of causality from this study. We do not have detailed dietary data on the amounts of breast milk or complementary foods consumed. Nonetheless, this research is a descriptive first step in understanding growth trajectories in an HEU population. Future research should attempt to replicate these findings in larger cohorts and may include longer follow‐up periods. Also of interest are the infants in the highest WLZ class and LAZ classes that experience stunting. This discordance between WLZ and LAZ status is a rare opportunity to study factors that cause high WLZ without a similar effect on LAZ. The long‐term health consequences of this growth pattern could be of public health interest as the elevated WLZ may serve to counteract some of the negative impacts of low LAZ on health outcomes in this population.
4.4. Future directions
The vast majority of the literature on the relationship between early growth and later health considers growth endpoints such as z‐scores or stunting and wasting status at specific ages. Infant growth endpoints are related to a variety of future outcomes including school attainment, productivity, cognitive development, wages, obesity, insulin resistance, and blood pressure (Adair, 2014; Denneman et al., 2018; Ribe, Svensen, Lyngmo, Mduma, & Hinderaker, 2018). However, there has been little study of the effect of the path by which infants reach their growth endpoints on future health. Our work shows that considering growth endpoints alone may not be sufficient due to the variety of paths by which infants may reach their endpoints. For example, LAZ Classes 4 and 5 have essentially the same mean z‐scores at 6 months but show very different growth patterns thereafter. LAZ Classes 3 and 4 have similar z‐scores by 24 months, but Class 3 experienced a decrease in mean z‐score of almost 1 SD whereas Class 4 had nearly no change in z‐score. The path by which infants reach their endpoints is likely to impact future health outcomes. In Europe, infants in growth classes with rapid BMI increases in the first 2 years of life have higher risk of developing asthma before age six (Rzehak et al., 2013). We start the effort to relate growth trajectories to health outcomes by characterizing heterogeneity in infant growth outcomes and identifying some predictors of poor growth patterns. Future work should consider heterogeneity in infant growth patterns and attempt to link these patterns to health outcomes later in life.
5. CONCLUSION
From a public health standpoint, understanding the variability of growth trajectories in a population allows for an understanding of the variability in the health and well‐being of that population. Growth can be viewed as either a determinant of future health or as a marker of an underlying process that also determines adult outcomes (Dewey & Begum, 2011). Regardless of whether growth is a determinant of these outcomes or a metric of some other determinant, early development is essential for adult achievement (Grantham‐McGregor et al., 2007). Therefore, an understanding of the various trajectories by which these infants grow allows us to understand the variability in the health of these infants. We show that mean values do not adequately describe the meaningful variations in growth patterns of this population. We also show that many of the factors related to poor growth endpoints in other populations put infants on developmental tracks that affect health and well‐being throughout infancy and likely into later life.
As the population of HEU infants increases in sub‐Saharan Africa, it is becoming more important to take steps to ensure that these infants achieve optimal growth so they can maximally contribute to the economic and social development of their countries. Efforts should be taken to support the health and well‐being of these infants who experience increased risk of morbidity and mortality. The widespread adoption of Option B+ and continued breastfeeding may be able to improve growth outcomes for these infants. In our population of HEU infants exposed to Option B+ and continued breastfeeding, infants have higher WLZ for the first 2 years of life and lower LAZ for the first 6 months than infants in other low‐resource settings, including Rwanda, but their growth converges towards that seen in comparable populations. When compared with the Rwandan population, these HEU infants had lower early LAZ and higher early WLZ. However, these patterns are very heterogeneous. Future research should investigate both potential causal pathways leading to this unusual growth, slow linear growth and elevated weight, and the long‐term health consequences of these early growth patterns.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
CEL carried out analyses and drafted the manuscript. EAB was one of the study principal investigators and thus conceptualized the study and reviewed and approved the final manuscript. DN was the data manager for the study, led data compilation and cleaning, and reviewed and approved the final manuscript. GFN led all data collection for the study and reviewed and approved the final manuscript. LSA designed the study, advised on analysis, contributed insights into the implications of results, and reviewed and approved the final manuscript.
ACKNOWLEDGMENTS
This work was done in collaboration with the Elizabeth Glaser Pediatric AIDS Foundation, with support from United States Agency for International Development through USAID Cooperative Agreement AID‐OAA‐A‐12‐00024.
Lane CE, Bobrow EA, Ndatimana D, Ndayisaba GF, Adair LS. Determinants of growth in HIV‐exposed and HIV‐uninfected infants in the Kabeho Study. Matern Child Nutr. 2019;15:e12776 10.1111/mcn.12776
REFERENCES
- Adair, L. S. (2014). Long‐term consequences of nutrition and growth in early childhood and possible preventive interventions. Nestle Nutrition Institute Workshop Series, 78, 111–120. 10.1159/000354949 [DOI] [PubMed] [Google Scholar]
- Alemu, F. , Yalew, A. , Fantahun, M. , & Ashu, E. (2015). Antiretroviral therapy and pregnancy outcomes in developing countries: A systematic review. International Journal of MCH and AIDS, 3(1), 31–43. [PMC free article] [PubMed] [Google Scholar]
- Arikawa, S. , Rollins, N. , Newell, M. , & Becquet, R. (2016). Mortality risk and associated factors in HIV‐exposed, uninfected children. Tropical Medicine and International Health, 21(6), 720–734. 10.1111/tmi.12695 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arpadi, S. , Fawzy, A. , Aldrovandi, G. M. , Kankasa, C. , Sinkala, M. , Mwiya, M. , & Thea, D. M. (2009). Growth faltering due to breastfeeding cessation in uninfected children born to HIV‐infected mothers in Zambia. The American Journal of Clinical Nutrition, 90(2), 344–353. 10.3945/ajcn.2009.27745.344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brennan, A. T. , Bonawitz, R. , Gill, C. J. , Thea, D. M. , Kleinman, M. , Useem, J. , … Fox, M. P. (2016). A meta‐analysis assessing all‐cause mortality in HIV‐exposed uninfected compared with HIV‐unexposed uninfected infants and children. AIDS, 30(15), 2351–2360. 10.1097/QAD.0000000000001211 [DOI] [PubMed] [Google Scholar]
- Campbell, R. , Kang, Y. , & West, P. (2017). Infant and young child feeding (IYCF) practices and nutritional status under 2 years of age in Bhutan. FASEB Journal, 31(1), 639–638. [Google Scholar]
- Conserve, D. , Eustache, E. , Oswald, C. , Louis, E. , Scanlan, F. , & Mukherjee, J. (2015). Maternal illness and its impact on children well‐being and development in Hatie. Jounal of Child and Family Studies, 24(9), 2779–2785. 10.1007/s10826-014-0081-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crossant, Y. (2013). mlogit: Multiple logit model.
- Denneman, L. , Cohen, S. , Godfried, M. , van Leeuwen, E. , Nellen, J. , Kuijpers, T. , … Bunders, M. (2018). Exposure to improved nutrition from conception to age 2 years and adult cardiometabolic disease risk. The Lancet Global Health, in press, 6(8), e875–e884. 10.1016/S2214-109X(18)30231-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dewey, K. G. , & Begum, K. (2011). Long‐term consequences of stunting in early life. Maternal & Child Nutrition, 7(Suppl. 3), 5–18. 10.1111/j.1740-8709.2011.00349.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans, C. , Jones, C. E. , & Prendergast, A. J. (2016). HIV‐exposed uninfected infants: New global challenges in the era of paediatric HIV elimination. The Lancet Infectios Diseases, 16(6), e92–e107. 10.1016/S1473-3099(16)00055-4 [DOI] [PubMed] [Google Scholar]
- Filteau, S. (2009). The HIV exposed, uninfected African child. Tropical Medicine and International Health, 14(3), 276–287. 10.1111/j.1365-3156.2009.02220.x [DOI] [PubMed] [Google Scholar]
- Filteau, S. , Baisley, K. , Chisenga, M. , Kasonka, L. , & Gibson, R. S. (2011). Provision of micronutrient‐fortified food from 6 months of age does not permit HIV‐exposed uninfected Zambian children to catch up in growth to HIV‐unexposed children: A randomized controlled trial. Journal of Acquired Immune Deficiency Syndromes, 56(2), 166–175. 10.1097/QAI.0b013e318201f6c9 [DOI] [PubMed] [Google Scholar]
- Flax, V. L. , Bentley, M. E. , Chasela, C. S. , Kayira, D. , Hudgens, M. G. , Kacheche, K. Z. , … Adair, L. S. (2013). Lipid‐based nutrient supplements are feasible as a breastmilk replacement for HIV‐exposed infants from 24 to 48 weeks of age. Journal of Nutrition, 143(5), 701–707. 10.3945/jn.112.168245.701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gill, M. , Hoffman, H. , Ndatimana, D. , Mugwaneza, P. , Guay, L. , Ndayisaba, G. , … Mofenson, L. (2017). 24‐month HIV‐free survival among infants born to HIV‐positive women enrolled in Option B+ Program in Kigali, Rwanda: The Kabeho Study. Medicine, 96(51), e9445 10.1097/MD.0000000000009445 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gough, E. K. , Moodie, E. E. M. , Prendergast, A. J. , Ntozini, R. , Moulton, L. H. , Humphrey, J. H. , & Manges, A. R. (2016). Linear growth trajectories in Zimbabwean infants. American Journal of Clinical Nutrition, 104, 1616–1627. 10.3945/ajcn.116.133538.Am [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grantham‐McGregor, S. , Cheung, Y. B. , Cueto, S. , Glewwe, P. , Richter, L. , & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. Lancet, 369(9555), 60–70. 10.1016/S0140-6736(07)60032-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoekstra, T. , Barbosa‐Leiker, C. , Koppes, L. L. J. , & Twisk, J. W. R. (2011). Developmetal trajctories of body mass index throughout the life course: An application of latent class growth (mixture) modelling. Longitudinal and Life Course Studies, 2(3), 319–330. [Google Scholar]
- Joint United Nations Programme on HIV/AIDS (2013). Global report: UNAIDS report on the global AIDS epidemic 2013. Geneva: UNAIDS. [Google Scholar]
- Kamudoni, P. , Maleta, K. , Shi, Z. , & Holmboe‐Ottesen, G. (2015). Exclusive breastfeeding duration during the first 6 months of life is positively associated with length‐for‐age among infants 6–12 months old, in Mangochi district, Malawi. European Journal of Clinical Nutrition, 69(1), 96–101. 10.1038/ejcn.2014.148 [DOI] [PubMed] [Google Scholar]
- Kuchenbecker, J. , Jordan, I. , Reinbott, A. , Herrmann, J. , Jeremias, T. , Kennedy, G. , … Krawinkel, M. B. (2015). Exclusive breastfeeding and its effect on growth of Malawian infants: Results from a cross‐sectional study. Paediatrics and International Child Health, 35(1), 14–23. 10.1179/2046905514Y.0000000134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuhn, L. , Kasonde, P. , Sinkala, M. , Kankasa, C. , Semrau, K. , & Scott, N. (2005). Does severity of HIV disease in HIV‐infected mothers affect mortality and morbidity among their uninfected infants? Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 41(11), 1654–1661. 10.1086/498029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landa, R. J. , Gross, A. L. , Stuart, E. A. , & Bauman, M. (2012). Latent class analysis of early developmental trajectory in baby siblings of children with autism. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 53(9), 986–996. 10.1111/j.1469-7610.2012.02558.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lartey, A. , Marquis, G. S. , Mazur, R. , Perez‐Escamilla, R. , Brakohiapa, L. , Ampofo, W. , … Adu‐Afarwuah, S. (2014). Maternal HIV is associated with reduced growth in the first year of life among infants in the Eastern region of Ghana: The research to improve infant nutrition and growth (RIING) project. Maternal & Child Nutrition, 10(4), 604–616. 10.1111/j.1740-8709.2012.00441.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Le Roux, S. , Abrams, E. , Nguen, K. , & Myer, L. (2016). Clinical outcomes of HIV‐exposed, HIV‐uninfected children in sub‐Saharan Africa. Tropical Medicine and International Health, 21(7), 829–845. 10.1111/tmi.12716 [DOI] [PubMed] [Google Scholar]
- Li, C. , Goran, M. I. , Kaur, H. , Nollen, N. , & Ahluwalia, J. S. (2007). Developmental trajectories of overweight during childhood: Role of early life factors. Obesity (Silver Spring, Md.), 15(3), 760–771. 10.1038/oby.2007.585 [DOI] [PubMed] [Google Scholar]
- Makasa, M. , Kasonka, L. , Chisenga, M. , Sinkala, M. , Chintu, C. , Tomkins, A. , & Filteau, S. (2007). Early growth of infants of HIV‐infected and uninfected Zambian women. Tropical Medicine and International Health, 12(5), 594–602. 10.1111/j.1365-3156.2007.01836.x [DOI] [PubMed] [Google Scholar]
- McGarth, C. , Nduati, R. , Richardson, B. , Kristal, A. , Mbori‐Ngacha, D. , & Farquhar, C. (2012). The prevalence of stunting is high in HIV‐1–exposed uninfected infants in Kenya. The Journal of Nutrition, 142(4), 757–763. 10.3945/jn.111.148874 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mebrahtu, T. F. , Feltbower, R. G. , Petherick, E. S. , & Parslow, R. C. (2015). Growth patterns of white British and Pakistani children in the born in Bradford cohort: A latent growth modelling approach. Journal of Epidemiology and Community Health, 69(4), 368–373. 10.1136/jech-2014-204571 [DOI] [PubMed] [Google Scholar]
- National Institute of Statistics , Ministry of Health , & ICF International (2015). Rwanda Demographic and Health Survey. Rwanda. Rockville, Maryland, USA: NISR, MOH, and ICF International; https://doi.org/March, 2016. [Google Scholar]
- Ndirangu, J. , Newell, M.‐L. , Bland, R. M. , & Thorne, C. (2012). Maternal HIV infection associated with small‐for‐gestational age infants but not preterm births: Evidence from rural South Africa. Human Reproduction, 27(6), 1846–1856. 10.1093/humrep/des090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neri, D. , Somarriba, G. A. , Schaefer, N. N. , Chaparro, A. I. , Scott, G. B. , Lopez Mitnik, G. , … Miller, T. L. (2013). Growth and body composition of uninfected children exposed to human immunodeficiency virus: Comparison with a contemporary cohort and United States National Standards. Journal of Pediatrics, 163(1), 249–254.e2. 10.1016/j.jpeds.2012.12.034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nicholson, L. , Chisenga, M. , Siame, J. , Kasonka, L. , & Filteau, S. (2015). Growth and health outcomes at school age in HIV‐exposed, uninfected Zambian children: Follow‐up of two cohorts studied in infancy. BMC Pediatrics, 15(1), 1–10. 10.1186/s12887-015-0386-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Omoni, A. O. , Ntozini, R. , Evans, C. , Prendergast, A. J. , Moulton, L. H. , Christian, P. S. , & Humphrey, J. H. (2017). Child growth according to maternal and child HIV status in Zimbabwe. Pediatric Infectious Disease Journal, 36(9), 869–876. 10.1097/INF.0000000000001574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Onis, M. , & Blossner, M. (2003). The World Health Organization global database on child growth and malnutrition: Methodology and applications. International Journal of Epidemiology, 32, 518–526. 10.1093/ije/dyg099 [DOI] [PubMed] [Google Scholar]
- Pierre, R. , Fulford, T. , Lewis, K. , Palmer, P. , Walters, C. , & Christie, C. D. (2016). Infectious disease morbidity and growth among young HIV‐exposed and uninfected children in Jamaica. Revista Panamericana de Salud Pública, 40(6), 401–409. [PubMed] [Google Scholar]
- Powis, K. , Seaton, L. , Ogqu, A. , Lockman, S. , Dryden‐Peterson, S. , & van Widenfelt, E. (2011). Effects of in utero antiretroviral exposure on longitudinal growth of HIV‐exposed uninfected infants in Botswana. Journal of Acquired Immune Deficiency Syndromes, 56(2), 131–138. 10.1097/QAI.0b013e3181ffa4f5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prost‐Lima, C. , Phillips, V. , Diakite, A. , & Liquet, B. (2017). lcmm: Extended mixed models using latent classes and latent processes.
- R Core Team (2013). R: A language and environment for statistical computing.
- Ribe, I. G. , Svensen, E. , Lyngmo, B. A. , Mduma, E. , & Hinderaker, S. G. (2018). Determinants of early child development in rural Tanzania. Child and Adolescent Psychiatry and Mental Health, 12(1), 1–8. 10.1186/s13034-018-0224-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rzehak, P. , Wijga, A. H. , Keil, T. , Eller, E. , Bindslev‐Jensen, C. , Smit, H. A. , … Heinrich, J. (2013). Body mass index trajectory classes and incident asthma in childhood: Results from 8 European birth cohorts—A Global Allergy and Asthma European Network initiative. Journal of Allergy and Clinical Immunology, 131(6). 10.1016/j.jaci.2013.01.001), 1528–1536.e13. [DOI] [PubMed] [Google Scholar]
- Slogrove, A. L. (2016). Pattern of infectious morbidity in HIV‐exposed uninfected infants and children. Frontiers in Immunology, 7, 164 10.3389/fimmu.2016.00164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sofeu, C. L. , Warszawski, J. , Ndongo, F. A. , Penda, I. C. , Nadiang, S. T. , Guemkam, G. , … Obedat, S. (2014). Low birth weight in perinatally HIV‐exposed uninfected infants: Observations in urban settings in Cameroon. PLoS One, 9(4), e93554 10.1371/journal.pone.0093554 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sugandhi, N. , Rodrigues, J. , Kim, M. , Ahmed, S. , Amzel, A. , & Tolle, M. (2013). HIV‐exposed infants: Rethinking care for a lifelong condition. AIDS, 27, S187–S195. 10.1097/QAD.0000000000000090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taha, T. , Nour, S. , Li, Q. , Kumwenda, N. , Kafulafula, G. , & Nkhoma, C. (2010). The effect of human immunodeficiency virus and breastfeeding on the nutritional status of African children. Pediatric Infectious Disease Journal, 29(6), 514–518. [DOI] [PubMed] [Google Scholar]
- Victora, C. G. , de Onis, M. , Hallal, P. C. , Blossner, M. , & Shrimpton, R. (2010). Worldwide timing of growth faltering: Revisiting implications for interventions. Pediatrics, 125, e473–e480. 10.1542/peds.2009-1519 [DOI] [PubMed] [Google Scholar]
- Webb, A. , Manji, K. , Fawzi, W. , & Villamor, E. (2009). Time‐independent maternal and infant factors and time‐dependent infant morbidities including HIV infection, contribute to infant growth faltering during the first 2 years of life. Journal of Tropical Pediatrics, 55(2), 83–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (2006). The new WHO child growth standards. Geneva, Switzerland: World Health Organization; 10.4067/S0370-41062009000400012 [DOI] [Google Scholar]
- World Health Organization (2011). WHO Anthro: igrowup. Geneva, Switzerland: Department of Nutrition. [Google Scholar]
- World Health Organization (2016). Guideline: Updates on HIV and infant feeding. Geneva: World Health Organization. [PubMed] [Google Scholar]