

Abstract
Aims
To compare the efficacy and safety of an intensification strategy of early triple combination therapy with dapagliflozin (DAPA) plus saxagliptin (SAXA) to a dual therapy strategy with sitagliptin (SITA) in patients with type 2 diabetes who are inadequately controlled with metformin (MET) monotherapy.
Materials and methods
This multinational, active‐controlled, parallel‐group phase 3b trial randomized 461 patients, at least 18 years of age, with glycated haemoglobin (HbA1c) of 8%–10.5% (64–91 mmol/mol), to either DAPA plus SAXA or SITA, added to MET, for a 26‐week double‐blind treatment period and an extension of a 26‐week blinded treatment period.
Results
Mean (± SD) baseline HbA1c was 8.8% ± 0.9% (73.0 ± 9.3 mmol/mol). DAPA plus SAXA (n = 232) provided a greater reduction from baseline in HbA1c at Weeks 26 and 52 compared with SITA (n = 229) (adjusted mean ± SE change, Week 26: −1.41 ± 0.07% vs −1.07 ± 0.07% [−15.4 ± 0.8 mmol/mol vs 11.7 ± 0.8 mmol/mol]; P = 0.0008; Week 52: −1.29 ± 0.08% vs −0.81 ± 0.09% [14.1 ± 0.9 mmol/mol vs 8.9 ± 1.0 mmol/mol]). The between‐group difference in adjusted mean (95% CI) change from baseline in HbA1c increased from −0.34 (−0.54, −0.14) at Week 26 to −0.48 (−0.71, −0.25) at Week 52. DAPA plus SAXA was generally well tolerated and the incidence of adverse events was similar in both treatment arms.
Conclusions
Early intensification to triple therapy with DAPA plus SAXA results in better, more durable glycaemic control than addition of SITA only (dual therapy) in patients with high HbA1c levels who are uncontrolled with MET monotherapy.
Keywords: dapagliflozin, DPP‐IV inhibitor, GLP‐1, saxagliptin, SGLT2 inhibitor, type 2 diabetes
1. INTRODUCTION
Clinical guidelines recommend the use of metformin (MET) monotherapy as first‐line anti‐hyperglycaemic therapy for the majority of patients with type 2 diabetes, but treatment intensification will probably be required to maintain glycaemic control as the disease progresses.1, 2 However, the addition of individual oral therapies to MET may be inadequate to reach glycaemic targets in patients with very high levels of glycated haemoglobin (HbA1c) because of the complex multi‐system pathophysiology of type 2 diabetes, which requires a multi‐faceted treatment approach.3, 4 Simultaneous intensification with two therapies that have different mechanisms of action has the potential to provide more rapid, greater and sustained reductions in HbA1c; however, it is not known whether this form of therapy increases the risk of adverse events. Simultaneous intensification with two therapies may have benefits, such as improved adherence, reduced clinical inertia and increased durability, but the safety of such an approach is yet to be established.
In the present study, we report results from a randomized, double‐blind, active‐controlled trial evaluating the efficacy and safety of triple therapy, with the addition of the sodium‐glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin (DAPA) plus the dipeptidyl peptidase‐4 (DPP‐4) inhibitor saxagliptin (SAXA), vs dual therapy, with the addition of the DPP‐4 inhibitor sitagliptin (SITA) alone, in patients with type 2 diabetes who are inadequately controlled with MET monotherapy. The objective of this study, which included a short‐term 26‐week treatment period and a further 26‐week extension treatment period, was to assess the efficacy, safety and long‐term sustained control of a strategy of adding an early combination of two drugs to MET (triple therapy), compared with the commonly used strategy of adding only one drug (dual therapy).
2. MATERIALS AND METHODS
2.1. Study design
This multinational, randomized, double‐blind, active‐controlled, double‐dummy parallel‐group phase 3b trial (ClinicalTrials.gov Identifier: NCT02284893) was conducted in Hungary, Mexico, Poland, Romania, South Africa and the USA, in accordance with the principles of the Declaration of Helsinki. The protocol and its amendments were reviewed and approved by an Independent Ethics Committee or Institutional Review Board at each study site, and all patients provided written informed consent.
The study comprised a 2‐week screening period, a 2‐week lead‐in period, an initial 26‐week randomized, double‐blind treatment period, and an extension 26‐week site‐blind and patient‐blind treatment period (Figure S1). During the lead‐in period, patients continued to receive background MET medication (≥1500 mg/d). After completing the lead‐in period, eligible patients were randomized (1:1) using an interactive voice‐response system to receive a combination of DAPA (10 mg/d) and SAXA (5 mg/d) or SITA (100 mg/d), in addition to their regular MET dose for 26 weeks. After completing the 26‐week double‐blind treatment period, patients entered the extension 26‐week site‐ and patient‐blind treatment period, during which they received the same blinded study treatment as during the initial 26‐week period in addition to their regular MET dose. Study sites and patients were blinded to the treatment during the extension period, but the study sponsor's delegate, Bristol‐Myers Squibb, was unblinded.
2.2. Patients
Men and women at least 18 years of age, with inadequately controlled type 2 diabetes, defined as HbA1c of 8%‐10.5% (64‐91 mmol/mol) at screening were eligible for inclusion in the study if they had undergone stable MET therapy for at least 8 weeks prior to enrolment (≥1500 mg/d) and had received no other anti‐diabetes agent for more than 14 days during the 12 weeks prior to screening. Other inclusion criteria included having a body mass index (BMI) greater than 20 kg/m2 at the enrolment visit and a fasting plasma glucose (FPG) level of at least 270 mg/dL (≤ 15 mmol/L) at randomization. Exclusion criteria included diagnosis of type 1 diabetes, history of cardiovascular disease within 3 months of screening, hepatic insufficiency, medical history of diabetic ketoacidosis, renal impairment (defined as creatinine clearance <60 mL/min or serum creatinine ≥1.5 mg/dL in men or ≥ 1.4 mg/dL in women), history of acute pancreatitis and haemoglobinopathy.
Treatment compliance was assessed through patient interview and by counting returned tablets. Patients were strongly advised to adhere to both a diet and exercise programme and to the schedule of study assessments and procedures. Any concomitant use of a new prescription or over‐the‐counter or herbal/nutritional therapies was discussed with the investigator to avoid any alterations to glycaemic control; medications that were not included in the prohibited medications list were authorized at the discretion of the investigator. Patients meeting the criterion for rescue medication at any time (FPG > 270 mg/dL [> 15.0 mmol/L] before Week 6; FPG > 240 mg/dL [> 13.3 mmol/L] during Weeks 7‐11; FPG > 200 mg/dL [>11.1 mmol/L] during Weeks 12‐26; and HbA1c > 8% [≥64 mmol/mol] during Weeks 27‐51) received basal insulin or other anti‐diabetes agents, with the exception of glucagon‐like peptide‐1 receptor agonists, other DPP‐4 or SGLT2 inhibitors and MET, at the investigator's discretion.
2.3. Study assessments
The primary efficacy end point was mean change in HbA1c from baseline to Week 26. Secondary efficacy measures were the proportion of patients with HbA1c less than 7% (< 53 mmol/mol) at Week 26 and mean changes in FPG and body weight from baseline to Week 26.
Efficacy end points assessed at 52 weeks were all considered exploratory and included mean change in HbA1c from baseline, proportion of patients achieving glycaemic control (HbA1c < 7% [<53 mmol/mol]), mean change from baseline in total body weight and FPG level, proportion of patients requiring treatment intensification and time to intensification, mean change from baseline in seated systolic blood pressure, change from baseline in biomarkers, including high‐sensitivity C‐reactive protein (hsCRP) and B‐type natriuretic protein (BNP), and mean change from baseline in urinary glucose: creatinine ratio at each time point.
Safety assessments at 52 weeks included proportion of patients experiencing adverse events (AEs) or serious AEs (SAEs), changes in selected safety clinical laboratory measures and confirmed hypoglycaemia, defined as plasma blood glucose of at least 70 mg/dL (≤3.9 mmol/L) or signs/symptoms of hypoglycaemia with self‐monitored blood glucose of at least 70 mg/dL (≤3.9 mmol/L), and percentage change from baseline in fasting serum lipids (total cholesterol, low‐density lipoprotein [LDL] cholesterol, high‐density lipoprotein [HDL] cholesterol and triglycerides).
AEs of special interest included genital infections and urinary tract infections (UTIs), pancreatitis and pancreatic cancer, worsening renal function, decreased thrombocyte and lymphocyte counts, hypersensitivity reactions, severe cutaneous adverse reactions, bladder and breast neoplasms, and volume depletion.
2.4. Statistical analysis
A sample size of 210 patients per group was determined a priori to yield approximately 89% power to detect a difference in mean HbA1c of 0.35% (3.8 mmol/mol) between the two groups at a two‐sided significance level of 0.05 and assuming a standard deviation (SD) of 1.1% and a 5% dropout rate. Efficacy analyses included all randomized patients who received at least one dose of study medication during the full double‐blind treatment period (intention‐to‐treat population). The DAPA plus SAXA plus MET group was tested against the SITA plus MET group for the primary efficacy end point at a two‐sided 5% α level. Analysis of the primary efficacy end point was performed using a longitudinal repeated‐measures analysis with the factors of baseline value, treatment group, time, interaction between treatment group and time, and interaction between baseline value and time, including observations made prior to rescue medication until treatment discontinuation. Point estimates and 95% CIs were calculated for adjusted mean changes within each treatment group, as well as for differences in adjusted mean (± standard error [SE]) changes between treatment groups. Secondary efficacy end points were tested sequentially at a two‐sided 5% α level. To limit the overall type I error rate, interpretation of the statistical significance of treatment comparisons for each secondary efficacy end point was tested using a stepwise procedure. For the long‐term 52‐week extension period, no statistical hypothesis tests were performed and no P values were calculated because all efficacy end points for this period were considered exploratory. Mean changes in HbA1c from baseline until Week 52 were compared between treatment groups using the same longitudinal repeated‐measures analysis as described above. The proportion of patients achieving HbA1c less than 7% (<53 mmol/mol) at Weeks 26 and 52 were compared between treatment groups using previously published methods.5, 6 Mean changes from baseline to Weeks 26 and 52 in FPG and total body weight, and urinary glucose: creatinine ratio mean changes from baseline to Week 52 were compared using the same longitudinal repeated‐measures model as used for the HbA1c efficacy end point. Exploratory biomarker measurements of hsCRP and BNP were summarized with descriptive statistics.
Safety analyses included all randomized patients who received at least one dose of study medication (intention‐to‐treat population). The percentage change in lipids from baseline at Week 52 was compared between treatment groups using a longitudinal repeated measures analysis of the logarithms of the post‐ to pre‐treatment ratios, including treatment group, time, interaction of treatment and time, the natural logarithm of the baseline measurement (ln [baseline]), and the interaction of ln (baseline) and time.
3. RESULTS
3.1. Patient disposition and baseline characteristics
The first patient visit for this study took place 22 December 2014 and the last patient visit took place 26 October 2016. The number of patients enrolled was 861; of these, 487 entered the lead‐in period and 461 were randomized to receive at least one dose of medication during the double‐blind treatment period (DAPA plus SAXA, n = 232; SITA, n = 229) (Figure S2). Of the 461 patients randomized, 411 (89.2%) completed the short‐term 26‐week treatment period, 402 (87.2%) entered the long‐term 26‐week extension period and 378 (82.0%) (DAPA plus SAXA, n = 198; SITA, n = 180) completed the study. Patient demographics and characteristics at baseline were similar across treatment groups (Table 1). Mean (±SD) baseline HbA1c was 8.8 ± 0.9% (73.0 ± 9.3 mmol/mol). More than 99% of patients in both treatment groups were compliant with the study medication (patients received ≥80% and ≤120% of planned drug doses).
Table 1.
Baseline patient demographics and characteristics (intention‐to‐treat population)
| DAPA plus SAXA plus MET | SITA plus MET | Total | |
|---|---|---|---|
| N = 232 | N = 229 | N = 461 | |
| Age, y | |||
| Mean ± SD | 55.9 ± 8.9 | 55.8 ± 9.6 | 55.9 ± 9.2 |
| Age categories, n (%) | |||
| <65 y | 197 (84.9) | 184 (80.3) | 381 (82.6) |
| ≥65 y | 35 (15.1) | 45 (19.7) | 80 (17.4) |
| ≥75 y | 3 (1.3) | 6 (2.6) | 9 (2.0) |
| Sex, n (%) | |||
| Male | 100 (43.1) | 110 (48.0) | 210 (45.6) |
| Female | 132 (56.9) | 119 (52.0) | 251 (54.4) |
| Race, n (%) | |||
| White | 153 (65.9) | 149 (65.1) | 302 (65.5) |
| Black or African‐American | 34 (14.7) | 32 (14.0) | 66 (14.3) |
| Asian | 8 (3.4) | 12 (5.2) | 20 (4.3) |
| Other | 37 (15.9) | 36 (15.7) | 73 (15.8) |
| Geographic region, n (%) | |||
| North America | 114 (49.1) | 113 (49.3) | 227 (49.2) |
| Latin America | 46 (19.8) | 42 (18.3) | 88 (19.1) |
| Europe | 72 (31.0) | 74 (32.3) | 146 (31.7) |
| BMI, kg/m2 | |||
| Mean ± SD | 33.3 ± 6.1 | 32.8 ± 6.3 | 33.1 ± 6.2 |
| BMI categories, n (%) | |||
| <25 kg/m2 | 14 (6.0) | 20 (8.7) | 34 (7.4) |
| ≥25 kg/m2 | 218 (94.0) | 209 (91.3) | 427 (92.6) |
| ≥27 kg/m2 | 202 (87.1) | 191 (83.4) | 393 (85.2) |
| ≥30 kg/m2 | 151 (65.1) | 147 (64.2) | 298 (64.6) |
| Duration of type 2 diabetes, years | |||
| Mean ± SD | 7.9 ± 5.7 | 8.2 ± 5.2 | 8.0 ± 5.4 |
| Duration of type 2 diabetes categories, n (%) | |||
| <3 years | 51 (22.0) | 35 (15.3) | 86 (18.7) |
| 3‐10 years | 115 (49.6) | 119 (52.0) | 234 (50.8) |
| >10 years | 66 (28.4) | 75 (32.8) | 141 (30.6) |
| Recent history of congestive cardiac failure, n (%) | 2 (0.9) | 3 (1.3) | 5 (1.1) |
| HbA1c | |||
| Mean ± SD, % | 8.8 ± 0.8 | 8.9 ± 0.9 | 8.8 ± 0.9 |
| Mean ± SD, mmol/mol | 73.0 ± 9.2 | 74.0 ± 9.4 | 73.0 ± 9.3 |
| HbA1c categories, n (%) | |||
| <8% [<64 mmol/mol] | 33 (14.2) | 27 (11.8) | 60 (13.0) |
| 8%‐9% [64‐74 mmol/mol] | 108 (46.6) | 96 (41.9) | 204 (44.3) |
| ≥9% [≥75 mmol/mol] | 91 (39.2) | 106 (46.3) | 197 (42.7) |
| Fasting plasma glucose | |||
| Mean ± SD, mg/dL | 171.8 ± 42.3 | 175.0 ± 43.4 | 173.4 ± 42.9 |
| Mean ± SD, mmol/L | 9.5 ± 2.4 | 9.7 ± 2.4 | 9.6 ± 2.4 |
| eGFR, mL/min/1.73 m2 | |||
| Mean ± SD | 92.2 ± 20.2 | 92.9 ± 22.5 | 92.5 ± 21.3 |
| eGFR categories, n (%) | |||
| <30 mL/min/1.73 m2 | 0 | 0 | 0 |
| 30‐59 mL/min/1.73 m2 | 9 (3.9) | 13 (5.7) | 22 (4.8) |
| 60‐89 mL/min/1.73 m2 | 96 (41.4) | 96 (41.9) | 192 (41.6) |
| ≥90 mL/min/1.73 m2 | 127 (54.7) | 120 (52.4) | 247 (53.6) |
| MET dose category, n (%) | |||
| <1500 mg/d | 1 (0.4) | 1 (0.4) | 2 (0.4) |
| 1500‐1700 mg/d | 66 (28.4) | 73 (31.9) | 139 (30.2) |
| 1701‐2499 mg/d | 112 (48.3) | 108 (47.2) | 220 (47.7) |
| ≥2500 mg/d | 53 (22.8) | 47 (20.5) | 100 (21.7) |
| Seated SBP, mm Hg | |||
| Mean ± SD | 130.0 (14.0) | 128.7 (13.3) | ‐ |
| Biomarker, SI units (mean ± SD) | |||
| hsCRP | 4.8 (5.3) | 5.0 (9.3) | ‐ |
| BNP | 9.4 (32.7) | 9.0 (16.2) | ‐ |
| Urine glucose: Creatinine ratio | |||
| Mean ± SD | 4.6 (13.7) | 6.0 (23.4) | ‐ |
| Fasting serum lipids, mg/dL (mean ± SD) | |||
| Total cholesterol | 183.5 (37.4) | 181.3 (38.8) | ‐ |
| LDL cholesterol | 101.5 (31.6) | 101.9 (32.7) | ‐ |
| HDL cholesterol | 45.7 (12.2) | 43.8 (10.7) | ‐ |
| Triglycerides | 190.4 (110.9) | 183.4 (102.1) | ‐ |
Abbreviations: BMI, body mass index; BNP, B‐type natriuretic protein; DAPA, dapagliflozin; eGFR, estimated glomerular filtration rate; HbA1c, glycated haemoglobin; hsCRP, HDL, high density lipoprotein; high‐sensitivity C‐reactive protein; LDL, low density lipoprotein; MET, metformin; SAXA, saxagliptin; SBP, systolic blood pressure; SD, standard deviation; SI units, international system of units; SITA, sitagliptin.
3.2. Efficacy
Patients receiving DAPA plus SAXA add‐on therapy showed a greater reduction from baseline in HbA1c at both Week 26 and Week 52 compared with those receiving SITA add‐on therapy (adjusted mean ± SE change, Week 26: −1.41 ± 0.07% vs −1.07 ± 0.07% [15.4 ± 0.8 mmol/mol vs 11.7 ± 0.8 mmol/mol]; P = 0.0008; Week 52: −1.29 ± 0.08% vs −0.81 ± 0.09% [14.1 ± 0.9 mmol/mol vs 8.9 ± 1.0 mmol/mol]) (Figure 1A). The between‐group difference in adjusted mean (95% CI) change in HbA1c from baseline increased from −0.34 (−0.54, −0.14) at Week 26 to −0.48 (−0.71, −0.25) at Week 52. More patients achieved HbA1c less than 7% with DAPA plus SAXA add‐on therapy than did patients who received SITA add‐on therapy at Weeks 26 and 52 (adjusted mean percentage ± SE, Week 26: 37.3 ± 3.2% vs 25.1 ± 2.9%; P = 0.0034; week 52: 33.0 ± 3.1% vs 19.5 ± 2.6%). At Week 52, the adjusted difference (95% CI) between treatment groups was 13.5% (5.6, 21.4) (Figure 1B).
Figure 1.
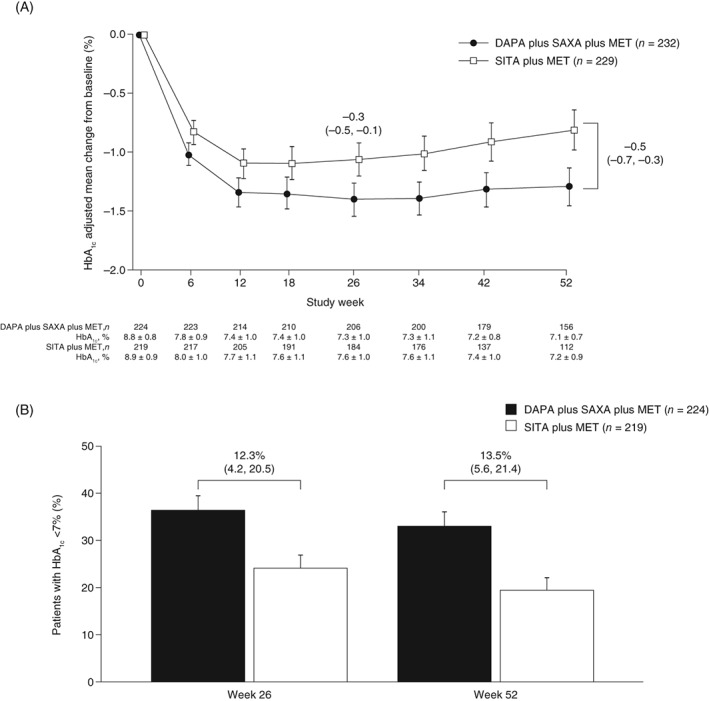
A) Baseline‐adjusted mean change in HbA1c from baseline to week 52. B) Proportion of patients achieving HbA1c < 7% at weeks 26 and 52 in the DAPA plus SAXA vs SITA add‐on therapy groups (excluding data after rescue medication). Data are presented as A) baseline adjusted mean (95% CI) change in HbA1c from baseline in randomized patients; B) baseline (last observation carried forward) adjusted mean (+ SE) proportion of randomized patients. Differences between groups (95% CI) at Weeks 26 and 52 are indicated. n is the number of randomized patients with non‐missing baseline values and at least one post‐baseline value. Values presented are from the combined 26‐week and 52‐week treatment periods. Abbreviations: DAPA, dapagliflozin; HbA1c, glycated haemoglobin; MET, metformin; SAXA, saxagliptin; SE, standard error; SITA, sitagliptin
At Weeks 26 and 52, patients in the DAPA plus SAXA group showed a greater reduction in FPG (adjusted mean ± SE change, week 26: −32 ± 3 vs −11 ± 3 mg/dL [−1.8 ± 0.1 vs −0.6 ± 0.1 mmol/L]; P < 0.0001; Week 52: −26 ± 3 vs −4 ± 4 mg/dL [−1.4 ± 0.2 mmol/L vs −0.2 ± 0.2 mmol/L]) (Figure S3A) and greater weight loss (adjusted mean ± SE change, Week 26: −1.9 ± 0.2 vs −0.5 ± 0.2 kg; P < 0.0001; Week 52: −2.3 ± 0.3 vs −0.8 ± 0.3 kg) (Figure S3B) than did those in the SITA group. The adjusted differences (95% CI) between treatment groups in FPG and weight loss were −22 mg/dL (−32, −12) and −1.6 kg (−2.4, −0.8), respectively, at Week 52.
The proportion of patients who discontinued the study because of a lack of glycaemic control or who were rescued because of failure to achieve pre‐specified glycaemic targets are included in Table 2. By Week 52, 18.1% of patients in the DAPA plus SAXA group and 32.8% of patients in the SITA group had received rescue medication. The most commonly used rescue medication over the 52‐week study period was glimepiride (used by 23 patients in the DAPA plus SAXA group and by 39 patients in the SITA group). Five patients in the DAPA plus SAXA group and nine patients in the SITA group used basal insulin. No patient discontinued the study because of a lack of glycaemic control.
Table 2.
Additional exploratory end points at week 52
| Study end point | DAPA plus SAXA plus METN = 232 | SITA plus METN = 229 | Difference (95% CI) |
|---|---|---|---|
| Proportion of patients discontinued because of a lack of glycaemic control or rescued for not achieving pre‐specified glycaemic targets, %a |
n = 42b
18.6 ± 2.5 |
n = 75b
32.3 ± 3.1 |
−13.8 (−21.4, −6.1) |
| Seated SBP, mm Hga |
n = 157 −2.6 ± 0.9 |
n = 112 2.5 ± 1.0 |
−5.1 (−7.7, −2.5) |
| Change in biomarkers from baseline, SI unitsc | |||
| hsCRP, mg/L |
n = 195 0.43 ± 0.54 |
n = 176 − 0.09 ± 0.75 |
‐ |
| BNP, ng/L |
n = 183 −1.39 ± 0.84 |
n = 168 4.10 ± 3.61 |
‐ |
| Change in urine glucose: Creatinine ratio from baselinec |
n = 186 40.1 ± 2.3 |
n = 171 −1.1 ± 2.4 |
41.2 (34.7, 47.7) |
| Percentage change in fasting serum lipids from baseline, mg/dL (95% CI) | |||
| Total cholesterol |
n = 196 2.1 (−0.4, 4.7) |
n = 177 3.0 (0.3, 5.8) |
−0.9 (−4.4, 2.8) |
| LDL cholesterol |
n = 196 2.2 (−2.0, 6.6) |
n = 177 5.6 (1.0, 10.4) |
−3.2 (−8.9, 2.9) |
| HDL cholesterol |
n = 196 3.9 (1.8, 6.1) |
n = 177 1.8 (−0.3, 4.0) |
2.0 (−0.9, 5.1) |
| Triglycerides |
n = 196 −2.4 (−7.5, 3.0) |
n = 177 −1.7 (−7.1, 3.9) |
−0.7 (−8.1, 7.4) |
Values are adjusted mean ± SE unless otherwise specified.
Abbreviations: BNP, B‐type natriuretic protein; DAPA, dapagliflozin; hsCRP, HDL, high density lipoprotein; high‐sensitivity C‐reactive protein; LDL, low density lipoprotein; MET, metformin; SAXA, saxagliptin; SBP, systolic blood pressure; SE, standard error; SI units, international system of units; SITA, sitagliptin.
Excluding data after rescue medication.
Number of patients discontinued owing to lack of glycaemic control or rescued for not achieving pre‐specified glycaemic targets.
Including data after rescue medication.
From baseline levels, systolic blood pressure decreased in the DAPA plus SAXA group and increased in the SITA group at Week 52 (adjusted mean ± SE change, −2.6 ± 0.9 vs +2.5 ± 1.0 mm Hg, respectively) (Table 2). The adjusted difference (95% CI) between treatment groups was −5.1 mm Hg (−7.7, −2.5).
The changes from baseline in hsCRP, BNP and urinary glucose: creatinine ratio are included in Table 2. Patients in the DAPA plus SAXA group showed a greater change from baseline in urinary glucose: creatinine ratio than did those in the SITA group (adjusted mean ± SE change, 40.1 ± 2.3 vs −1.1 ± 2.4).
Adjusted mean changes from baseline in fasting serum lipids (total cholesterol, LDL‐cholesterol, HDL‐cholesterol, and triglycerides) were small and no clinically meaningful differences between treatment groups were observed, with all lipid values remaining in the normal to borderline ranges up to Week 52 (Table 2).
3.3. Safety
Triple therapy with DAPA plus SAXA add‐on to MET was generally well tolerated after 52 weeks of treatment; the incidence of AEs in patients receiving triple therapy was similar to that in patients receiving dual therapy with SITA add‐on (Table 3). AEs that were determined by the investigator to be related to the study drug were reported by 22 (9.5%) patients in the DAPA plus SAXA group and by 17 (7.4%) patients in the SITA group. Few patients discontinued the study because of AEs (DAPA plus SAXA, 1.7%; SITA, 4.4%) and none of these discontinuations was because of hypoglycaemia. The proportion of patients who experienced SAEs was low in both treatment groups (DAPA plus SAXA, 3.9%; SITA, 5.7%). Of the SAEs reported, none was considered by the investigator to be related to DAPA plus SAXA treatment, and only one SAE, drug hypersensitivity, was reported to be related to SITA treatment. The most common SAEs were pneumonia, endometriosis and osteoarthritis, which were reported for two patients each in the SITA group; no other SAEs were reported more than once in either treatment group.
Table 3.
Summary of adverse events over 52 weeks of treatment (safety set)
| Adverse events, n (%) | DAPA plus SAXA plus MET N = 232 | SITA plus MET N = 229 |
|---|---|---|
| Overall summary | ||
| At least one AE | 133 (57.3) | 132 (57.6) |
| At least one treatment‐related AE | 22 (9.5) | 17 (7.4) |
| At least one SAE | 9 (3.9) | 13 (5.7) |
| At least one treatment‐related SAEa | 0 (0.0) | 1 (0.4) |
| AE leading to discontinuation of study drug | 4 (1.7) | 10 (4.4) |
| SAE leading to discontinuation of study drug | 0 (0.0) | 4 (1.7) |
| Hypoglycaemiab | 29 (12.5) | 27 (11.8) |
| Confirmed hypoglycaemiab | 12 (5.2) | 9 (3.9) |
| Hypoglycaemia leading to discontinuation of study drug | 0 (0.0) | 0 (0.0) |
| Genital infections | 8 (3.4) | 5 (2.2) |
| Urinary tract infections | 15 (6.5) | 8 (3.5) |
| Deaths | 0 (0.0) | 0 (0.0) |
| AEs occurring in ≥2% of treated patients in either treatment group | ||
| Nasopharyngitis | 18 (7.8) | 12 (5.2) |
| Headache | 13 (5.6) | 10 (4.4) |
| Urinary tract infection (unclassified) | 10 (4.3) | 7 (3.1) |
| Influenza | 8 (3.4) | 11 (4.8) |
| Bronchitis | 8 (3.4) | 2 (0.9) |
| Upper respiratory tract infection | 7 (3.0) | 8 (3.5) |
| Back pain | 5 (2.2) | 9 (3.9) |
| Dyslipidaemia | 5 (2.2) | 3 (1.3) |
| Arthralgia | 5 (2.2) | 2 (0.9) |
| Sinusitis | 5 (2.2) | 2 (0.9) |
| Vulvovaginal mycotic infection | 5 (2.2) | 2 (0.9) |
| Gastroesophageal reflux disease | 5 (2.2) | 1 (0.4) |
| Gastroenteritis | 4 (1.7) | 5 (2.2) |
| Hypertension | 3 (1.3) | 8 (3.5) |
| Cough | 3 (1.3) | 7 (3.1) |
| Pain in extremity | 3 (1.3) | 6 (2.6) |
| Diarrhoea | 2 (0.9) | 6 (2.6) |
| Anaemia | 1 (0.4) | 7 (3.1) |
| Atrial fibrillation | 1 (0.4) | 5 (2.2) |
| Gastritis | 1 (0.4) | 5 (2.2) |
| Hyperglycaemia | 0 (0.0) | 5 (2.2) |
Abbreviations: AE, adverse event; DAPA, dapagliflozin; MET, metformin; SAE, serious adverse event; SAXA, saxagliptin; SITA, sitagliptin.
Drug hypersensitivity.
Excluding data after rescue medication.
Confirmed hypoglycaemia was reported in similar numbers of patients in each treatment group after 26 weeks and after 52 weeks of treatment (26 weeks: DAPA plus SAXA, 9 [3.9%]; SITA, 6 [2.6%]); 52 weeks: DAPA plus SAXA, 12 [5.2%]; SITA, 9 [3.9%]); no major episodes were reported.
The proportion of patients experiencing genital infections was similar in the DAPA plus SAXA group and the SITA group (3.4% vs 2.2%, respectively). Vulvovaginal mycotic infection was the most common genital infection (DAPA plus SAXA, n = 5 women; SITA, n = 2 women). In the DAPA plus SAXA group, two women experienced vaginal infection; one experienced vulvovaginitis and one experienced vulvovaginal candidiasis. In the SITA group, one woman experienced vulvitis and two men experienced balanoposthitis.
UTIs occurred in 6.5% of patients in the DAPA plus SAXA group and in 3.5% of patients in the SITA group (men, 4.0% vs 1.8%; women, 8.3% vs 5.0%, respectively). Unclassified UTIs were more common in women than in men (DAPA plus SAXA, n = 9 women, n = 1 man; SITA, n = 6 women, n = 1 man). In the DAPA plus SAXA group, one man experienced a fungal UTI, one man experienced prostatitis, one man experienced urethritis and two women experienced cystitis. In the SITA group, one man experienced cystitis.
The following conditions were reported as other AEs of special interest; definitions are based on preferred terms in the Standardised Medical Dictionary for Regulatory Activities Queries of cardiac failure. In the DAPA plus SAXA group, one patient reported an AE of syncope, one patient experienced adenocarcinoma of the colon, two patients reported an AE of peripheral oedema and three patients reported an AE of renal impairment/failure (n = 1, acute kidney injury; n = 1, decreased glomerular filtration rate; n = 1, increased blood creatinine); none of these AEs was deemed by the investigator to be related to the study drug. In the SITA group, seven patients experienced at least one cardiac event (n = 4, peripheral swelling; n = 2, peripheral oedema; n = 1, congestive cardiac failure; n = 1, chronic cardiac failure; n = 1, BNP increased); of these events, only one incidence of peripheral swelling was considered by the investigator to be related to the study drug. In addition, five patients in the SITA group reported AEs potentially related to hypotension, hypovolaemia or dehydration, and one patient experienced a decreased glomerular filtration rate. Hypersensitivity AEs were reported in six patients (2.6%) in the DAPA plus SAXA group and in seven patients (3.1%) in the SITA group; the most common hypersensitivity AE was rash (DAPA plus SAXA, n = 2 [0.9%]; SITA, n = 4 [1.7%]). No other AEs of special interest were reported (ie, pancreatitis, pancreatic cancer, breast/bladder neoplasms, severe cutaneous adverse reactions, decreased thrombocyte or lymphocyte counts).
One patient in the SITA group requested to discontinue the study because of suspected diabetic ketoacidosis. No deaths were reported for patients who received treatment during the study.
After 52 weeks, no clinically meaningful differences were observed in adjusted mean percentage change from baseline in fasting serum lipids between treatment groups (Table 2).
4. DISCUSSION
In this double‐blind, double‐dummy 52‐week trial, we report that an intensification strategy of early triple combination therapy with the addition of DAPA plus SAXA provides significantly greater improvements in glycaemic control than a dual therapy strategy with the addition of SITA alone in patients with inadequately controlled MET‐treated type 2 diabetes. These improvements were sustained after 52 weeks and were not associated with an increased risk of hypoglycaemia or other diabetes‐specific events, and the overall incidence of AEs was low. Furthermore, the improvement in glycaemic control with DAPA plus SAXA treatment was accompanied by a greater reduction in body weight and systolic blood pressure compared with treatment with SITA.
Therapeutic guidelines recommend treatment intensification through addition of anti‐diabetes agents for patients with inadequate glycaemic control with MET.7 However, dual add‐on therapy is rarely used, despite the knowledge that glycaemic control is seldom achieved with single‐agent add‐ons. The use of single‐agent add‐ons often leads to long periods of hyperglycaemia,8 which are associated with increased morbidity.9 The objective of this study was to evaluate the strategy of adding two anti‐hyperglycaemic agents (DAPA plus SAXA) simultaneously compared with the more common approach of adding one agent at a time (SITA) in patients with type 2 diabetes that is uncontrolled by MET. Adding two therapies simultaneously led to more rapid glucose control, which was sustained over 52 weeks, suggesting that there may be underlying improvements in insulin sensitivity and β‐cell function.10, 11, 12, 13, 14, 15 Treatment with DAPA plus SAXA add‐on to MET provided greater reductions in HbA1c and FPG than treatment with SITA add‐on, although, even with triple therapy, mean final HbA1c values were greater than 7% (53 mmol/mol), probably the result of the patients' high baseline HbA1c levels. However, a significantly greater proportion of patients achieved HbA1c less than 7% (<53 mmol/mol) with DAPA plus SAXA add‐on therapy than with SITA add‐on after 26 and 52 weeks, despite high baseline HbA1c levels. Differences in adjusted mean change from baseline in both HbA1c and FPG between the two treatment groups increased from Week 26 to Week 52, and a lower proportion of patients in the DAPA plus SAXA group required rescue therapy, indicating that SITA add‐on therapy is associated with more rapid increases in HbA1c and FPG over time, and that the efficacy of early triple therapy with DAPA plus SAXA add‐on to MET is durable. These improvements in glycaemic control are consistent with those reported in a previous clinical study that investigated the efficacy and safety of DAPA plus SAXA add‐on to MET compared with the addition to MET of each agent alone.16 In separate 52‐week studies in patients with inadequately controlled type 2 diabetes, triple therapy with the SGLT2 inhibitor ertugliflozin plus SITA add‐on to MET resulted in greater improvements in glycaemic control compared with SITA add‐on,17 and triple therapy with the SGLT2 inhibitor empagliflozin plus the DPP‐4 inhibitor linagliptin added to MET significantly reduced HbA1c levels compared with the individual drugs added to MET.18 Together, these studies indicate that a treatment strategy with early combination therapy may result in more rapid and more durable glycaemic control, with no increase in AEs, than single‐agent sequential add‐on therapy in patients with type 2 diabetes that is inadequately controlled with MET. The proportion of patients experiencing AEs and hypoglycaemia was similar for treatment with DAPA plus SAXA add‐on and for treatment with SITA add‐on therapies. The incidence of genital infections was low and similar between treatment groups; the incidence of UTIs was slightly higher in both men and women with triple therapy than with dual therapy (men, 4.0% vs 1.8%; women, 8.3% vs 5.0%, respectively). The overall incidence of both genital infections and UTIs after 52 weeks was only slightly higher than that observed at 26 weeks, were only mild or moderate in severity, and were similar to those previously reported for DAPA.19, 20 Triple therapy with DAPA plus SAXA add‐on to MET was associated with cumulative weight loss from 26 to 52 weeks, which was greater than that with dual therapy with SITA add‐on.
A limitation of the present study is that the effect of dual add‐on therapy with DAPA plus SAXA was compared with that of single add‐on of a different DPP‐4 inhibitor, SITA, and that there were no comparisons with single add‐on therapy with DAPA. However, this approach was used to indicate the effects of early combination therapy, rather than sequential add‐on therapy, on glycaemic control in patients with high baseline HbA1c levels. Studies have shown that SAXA and SITA have comparable efficacy when added to MET as monotherapy,21 which suggests that their respective use in the triple and dual therapy arms is unlikely to have had a large effect on the overall change in HbA1c. Furthermore, a comparison of initial add‐on therapy with DAPA plus SAXA with commonly used add‐on therapy is useful for informing future treatment guidelines. However, beyond the scope of this manuscript, further analyses should be undertaken to establish whether there is an interaction between diabetes duration and treatment efficacy and durability.
In conclusion, the treatment strategy of triple therapy with the early combination of DAPA plus SAXA add‐on to MET was well tolerated and resulted in significantly improved and long‐term sustained glycaemic control and weight loss, without increasing the risk of hypoglycaemia, compared with the usual approach of adding only SITA to MET therapy in patients with inadequately controlled type 2 diabetes. These results suggest that, when MET alone becomes inadequate to control HbA1c, a strategy of early intensification with triple therapy using a combination of DAPA plus SAXA may result in better, more durable and well‐tolerated glycaemic control than adding only a single drug (SITA) as a dual combination therapy in patients with high HbA1c levels.
CONFLICTS OF INTEREST
Y. H. has received honoraria for consultancy from Amarin Pharmaceuticals, Amgen, AstraZeneca, Boehringer Ingelheim, Eisai, Intarcia Therapeutics, Eli Lilly & Company, Janssen Pharmaceuticals, Merck KGaA, Pfizer, Novo Nordisk, Regeneron Pharmaceuticals and Sanofi; has received research support from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Lexicon Pharmaceuticals, Merck KGaA, Novo Nordisk and Sanofi; and serves or has served on speakers bureaus for Amarin Pharmaceuticals, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly & Company, Janssen Pharmaceuticals, Merck KGaA, Novo Nordisk, Regeneron Pharmaceuticals and Sanofi.
C. M. serves or has served on advisory panels for AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Eli Lilly & Company, Hanmi Pharmaceuticals, Intrexon, Janssen Pharmaceuticals, Mannkind, Medtronic, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, Roche Diagnostics, Sanofi and UCB; has received research support from Abbott, Eli Lilly & Company, Intrexon, Merck Sharp & Dohme, Novartis, Novo Nordisk, Roche Diagnostics and Sanofi; and serves or has served on speakers bureaus for AstraZeneca, Boehringer Ingelheim, Eli Lilly & Company, Merck Sharp & Dohme, Novartis, Novo Nordisk and Sanofi.
S. D. P. has received research support from AstraZeneca, Boehringer Ingelheim, Merck Sharp & Dohme, Novartis Pharmaceuticals; and has received honoraria for consultancy from AstraZeneca, Boehringer Ingelheim, Eli Lilly & Company, GlaxoSmithKline, Hanmi Pharmaceuticals, Janssen Pharmaceuticals, Merck Sharp & Dohme, Novartis Pharmaceuticals, Novo Nordisk, Sanofi, Servier and Takeda Pharmaceuticals.
E. J., R. K., N. I. and R. G‐S. are employees of AstraZeneca.
J. R. serves or has served on advisory panels for, and has received honoraria from, AstraZeneca, Boehringer Ingelheim, Eli Lilly & Company, Intarcia Therapeutics, Janssen Pharmaceuticals, Novo Nordisk and Sanofi; and has received research support from AstraZeneca, Asahi Kasei Corporation, Boehringer Ingelheim, Bristol‐Myers Squibb, Eli Lilly & Company, GlaxoSmithKline, Hanmi Pharmaceuticals, Intarcia Therapeutics, Janssen Pharmaceuticals, Lexicon Pharmaceuticals, Merck, Novartis, Novo Nordisk and Pfizer.
Author contributions
E. J., R. K., N. I. and R. G‐S. were involved in study design and conduct. All authors (Y. H., C. M., S. D. P., E. J., R. K., N. I., R. G‐S. and J. R.) had full access to study data and were involved in data interpretation and drafting and critically reviewing the manuscript. All authors approved the final version of the manuscript for submission.
Supporting information
Figure S1 Study design. DAPA, dapagliflozin; HbA1c, glycated haemoglobin; IR, immediate release; MET, metformin; SAXA, saxagliptin; SITA, sitagliptin; XR, extended release.
Figure S2 Patient disposition. DAPA, dapagliflozin; MET, metformin; SAXA, saxagliptin; SITA, sitagliptin.
Figure S3 Baseline‐adjusted mean changes in A, FPG and B, body weight from baseline to week 52 in the DAPA plus SAXA versus SITA add‐on therapy groups (excluding data after rescue medication).
ACKNOWLEDGMENTS
Medical writing support was provided by Tim Ellison, PhD, of PharmaGenesis London, UK, with funding from AstraZeneca. Statistical analyses of the data were performed by John Monyak, with funding from AstraZeneca. The results of this study were presented as an oral presentation at the 77th Scientific Sessions of the American Diabetes Association, San Diego, California, USA, 9‐13 June 2017 and as a poster at the 53rd Annual Meeting of the European Association for the Study of Diabetes, Lisbon, Portugal, 11‐15 September 2017.
Handelsman Y, Mathieu C, Del Prato S, et al. Sustained 52‐week efficacy and safety of triple therapy with dapagliflozin plus saxagliptin versus dual therapy with sitagliptin added to metformin in patients with uncontrolled type 2 diabetes. Diabetes Obes Metab. 2019;21:883–892. 10.1111/dom.13594
Funding information This study was funded by Bristol‐Myers Squibb and AstraZeneca. None of the authors received any financial or monetary transfer of value for their participation in the writing of the manuscript.
REFERENCES
- 1. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes, 2015: a patient‐centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of diabetes. Diabetologia. 2015;58:429‐442. [DOI] [PubMed] [Google Scholar]
- 2. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient‐centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of diabetes (EASD). Diabetes Care. 2012;35:1364‐1379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Mearns ES, Sobieraj DM, White CM, et al. Comparative efficacy and safety of antidiabetic drug regimens added to metformin monotherapy in patients with type 2 diabetes: a network meta‐analysis. PLoS One. 2015;10:e0125879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Raz I. Guideline approach to therapy in patients with newly diagnosed type 2 diabetes. Diabetes Care. 2013;36(suppl 2):S139‐S144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tsiatis AA, Davidian M, Zhang M, Lu X. Covariate adjustment for two‐sample treatment comparisons in randomized clinical trials: a principled yet flexible approach. Stat Med. 2008;27:4658‐4677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zhang M, Tsiatis AA, Davidian M. Improving efficiency of inferences in randomized clinical trials using auxiliary covariates. Biometrics. 2008;64:707‐715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Garber AJ, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of endocrinology on the comprehensive type 2 diabetes management algorithm—2017 executive summary. Endocr Pract. 2017;23:207‐238. [DOI] [PubMed] [Google Scholar]
- 8. Khunti K, Wolden ML, Thorsted BL, Andersen M, Davies MJ. Clinical inertia in people with type 2 diabetes: a retrospective cohort study of more than 80,000 people. Diabetes Care. 2013;36:3411‐3417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Stettler C, Allemann S, Juni P, et al. Glycemic control and macrovascular disease in types 1 and 2 diabetes mellitus: meta‐analysis of randomized trials. Am Heart J. 2006;152:27‐38. [DOI] [PubMed] [Google Scholar]
- 10. Ekholm E, Hansen L, Johnsson E, et al. Combined treatment with saxagliptin plus dapagliflozin reduces insulin levels by increased insulin clearance and improves beta‐cell function. Endocr Pract. 2017;23:258‐265. [DOI] [PubMed] [Google Scholar]
- 11. Forst T, Alghdban MK, Fischer A, et al. Sequential treatment escalation with dapagliflozin and saxagliptin improves beta cell function in type 2 diabetic patients on previous metformin treatment: an exploratory mechanistic study. Horm Metab Res. 2018;50:403‐407. [DOI] [PubMed] [Google Scholar]
- 12. Leibowitz G, Cahn A, Bhatt DL, et al. Impact of treatment with saxagliptin on glycaemic stability and beta‐cell function in the SAVOR‐TIMI 53 study. Diabetes Obes Metab. 2015;17:487‐494. [DOI] [PubMed] [Google Scholar]
- 13. Merovci A, Mari A, Solis‐Herrera C, et al. Dapagliflozin lowers plasma glucose concentration and improves beta‐cell function. J Clin Endocrinol Metab. 2015;100:1927‐1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Merovci A, Solis‐Herrera C, Daniele G, et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J Clin Invest. 2014;124:509‐514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ramirez‐Rodriguez AM, González‐Ortiz M, Martinez‐Abundis E. Effect of dapagliflozin on insulin secretion and insulin sensitivity in patients with prediabetes. Exp Clin Endocrinol Diabetes. 2018. 10.1055/a-0664-7583. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 16. Rosenstock J, Hansen L, Zee P, et al. Dual add‐on therapy in type 2 diabetes poorly controlled with metformin monotherapy: a randomized double‐blind trial of saxagliptin plus dapagliflozin addition versus single addition of saxagliptin or dapagliflozin to metformin. Diabetes Care. 2015;38:376‐383. [DOI] [PubMed] [Google Scholar]
- 17. Pratley RE, Eldor R, Raji A, et al. Ertugliflozin plus sitagliptin versus either individual agent over 52 weeks in patients with type 2 diabetes mellitus inadequately controlled with metformin: the VERTIS FACTORIAL randomized trial. Diabetes Obes Metab. 2018;20:1111‐1120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Defronzo RA, Lewin A, Patel S, et al. Combination of empagliflozin and linagliptin as second‐line therapy in subjects with type 2 diabetes inadequately controlled on metformin. Diabetes Care. 2015;38:384‐393. [DOI] [PubMed] [Google Scholar]
- 19. Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List JF. Urinary tract infections in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27:473‐478. [DOI] [PubMed] [Google Scholar]
- 20. Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List JF. Vulvovaginitis and balanitis in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27:479‐484. [DOI] [PubMed] [Google Scholar]
- 21. Scheen AJ, Charpentier G, Ostgren CJ. Efficacy and safety of saxagliptin in combination with metformin compared with sitagliptin in combination with metformin in adult patients with type 2 diabetes mellitus. Diabetes Metab Res Rev. 2010;26:540‐549. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Study design. DAPA, dapagliflozin; HbA1c, glycated haemoglobin; IR, immediate release; MET, metformin; SAXA, saxagliptin; SITA, sitagliptin; XR, extended release.
Figure S2 Patient disposition. DAPA, dapagliflozin; MET, metformin; SAXA, saxagliptin; SITA, sitagliptin.
Figure S3 Baseline‐adjusted mean changes in A, FPG and B, body weight from baseline to week 52 in the DAPA plus SAXA versus SITA add‐on therapy groups (excluding data after rescue medication).