

Abstract
Background
Road traffic accidents (RTA) remain a global public health concern in developing countries. The aim of the study was to document the frequency, characteristics and hospital outcomes of road traffic accidents in Guinea from 2015 to 2017.
Methods
We conducted a retrospective cohort study using medical records of RTA victims from 20 hospitals and a cross-sectional study of RTA cases from eight police stations in eight districts in Guinea, West Africa. Data analysis included descriptive statistics, trends of RTA, a sequence of interrupted time-series models and a segmented ordinary least-squares (OLS) regression.
Results
Police stations recorded 3,140 RTA over 3 years with an overall annual increase in RTA rates from 14.0 per 100,000 population in 2015, to 19.2 per 100,000 population in 2016 (37.1% annual increase), to 28.7 per 100,000 population in 2017 (49.5% annual increase).
Overall, the injury rates in 2016 and 2017 were .05 per 100,000 population higher on average per month (95% CI: .03–.07). Deaths from RTA showed no statistical differences over the 3 years and no association of RTA trends with season was found.
Overall, 27,751 RTA victims were admitted to emergency units, representing 22% of all hospitals admissions. Most victims were males (71%) and young (33%). Deaths represented 1.4% of all RTA victims. 90% of deaths occurred before or within 24 h of hospital admission. Factors associated with death were being male (p = .04), being a child under 15 years (p = .045) or an elderly person aged ≥65 years (p < .001), and having head injury or coma (p < .001).
Conclusions
RTA rates in Guinea are increasing. There is a need for implementing multisectoral RTA prevention measures in Guinea.
Keywords: Road traffic accident, Injuries, Death, Guinea, Police station, Hostpital, SORT IT
Background
Road traffic accidents (RTA) represent a huge global public health concern due to their increasing occurrence, related deaths and disabilities, social and financial consequences [1]. In 2018, the World Health Organization (WHO) estimated that 1.35 million people globally die each year from RTA [1, 2], and this is alongside the additional 20–50 million people who are seriously injured or disabled [3]. Low and Middle-Income countries, which house more than half (60%) of the world’s motor vehicles, bear more than 90% of RTA deaths and associated morbidities [1]. This growing public health problem has led to one of the health-related Sustainable Development Goals (SDGs) being focused on RTA with a target to halve the global number of accidents by 2020 [4]. This will be a major challenge because without effective interventions and action on the ground, RTA are estimated to increase by 67%, and become the fifth leading cause of death globally by 2030 [5].
In Sub-Saharan Africa, RTA have increased from 41 to 93 per 100,000 population over a fifteen-year period up to 2015, and currently account for one third of trauma cases admitted to health facilities [6, 7]. RTA case fatality rates for the Africa region in 2013 were estimated at 27 per 100,000 population [8]. Survivors of RTA are additionally burdened with physical disabilities and psychological disorders, especially affecting young adults, and the consequences of RTA also extend beyond the victims to the families and the associated communities. This high burden of RTA and associated deaths is due to a number of factors including inadequate or weakly enforced road safety legislation or ignorance of this legislation by road users, bad road infrastructure, irregular or non-existent vehicle maintenance and poor access to good quality health care [9].
Various studies in Africa have reported on RTA mortality rates ranging from 0.3 to 41% and occurring among car drivers, passengers, pedestrians, cyclists or users of motorcycles, with victims being predominantly males and in the age group of 20 to 44 years [6, 7]. In Nigeria, the most populated country in the continent, the trend in RTA has been reported to be increasing and RTA represent the leading cause of injury related deaths and the most common cause of disability in the country [10]. Recently in Ethiopia, similar findings reported that only one third of RTA victims received urgent/immediate surgical intervention before admission to hospital [11].
In Guinea, West Africa, the number of motor vehicles and motorcycles have increased from approximately 16,000 in 2010 to 37,000 in 2015 [12]. In line with other countries in the region, RTA have also been reported to be increasing in recent years [12], with RTA-related death rates estimated at 10–20 per 100,000 population [13, 14]. In terms of morbidity there has only been one publication from Guinea which focused solely on brain injury [15]. Given the rising importance of this public health problem, it is crucial for Guinea to assess the burden, characteristics and hospital outcomes of RTA, and especially to have baseline data by which to monitor the RTA-related SDG targets.
The study aimed therefore to document the frequency, characteristics and hospital outcomes of RTA in Guinea from 2015 to 2017 by using two data sources (police station and hospital records).
Methods
Study design
This study combined a retrospective cohort study using routinely collected data of RTA victims admitted to 20 hospitals from eight health districts and a cross-sectional study of RTA cases from eight police stations from the same districts.
Setting
General setting
Guinea, located in West Africa, is one of the low-income countries in the world with 55% of its population living below the national poverty line [12]. According to the Health Management and Information System data published in 2016, there were more than 11 million inhabitants with the majority living in rural settings (71%) and over half being illiterate (67%) [12].
The country comprises eight administrative regions including the capital city Conakry and 33 districts. The national public health system is tiered into a primary level (413 rural and urban health centers), a secondary level (7 regional and 26 district hospitals, 8 communal health centers with five in Conakry), and a tertiary level (3 national hospitals) [12]. There are 33 Medical and Surgical clinics and 11 polyclinics in the country. In Guinea, the total length of the road network is about 44,000 km of which only 2,220 is paved with asphalt nationwide [12].
Site specific setting
In the eight urban districts including the capital city (Conakry, Boké, Kindia, Kankan, N’Zérékoré, Mamou, Faranah and Siguiri), there have been reports of a high burden of RTA from 2014 to 2016 [12]. These districts constituted our study sites in which approximately 4.71 million people live (45% of the national population). Only one district (the capital city) out of the eight has a low proportion of its population living beneath the national poverty line (27.4 to 37.3%) [12].
General management of RTA
There are two police stations in Conakry and one in each of the seven urban districts which have a register in which to record details of all RTA. Generally, all RTA should be reported to the nearest police station, following which the police makes a report and enters specific data into the police register on: date of RTA, vehicle types, numbers of persons involved in the RTA, injuries (minor or severe) and death. Persons with no injury are sent home whereas those with injuries and the dead bodies are sent to the nearest hospital emergency unit. Alternatively, some RTA victims make their own way to a hospital without involving the police stations. At hospital, the injured victims are clinically assessed by trauma specialists or general surgeons according to the type of hospital (tertiary or secondary) and a record made in case files and registers of socio-demographic and clinical characteristics, types of injury sustained and death that occurred before or on arrival. Therefore, information collected at police stations fit the pre-crash and crash phase of Haddon Matrix while those of hospitals correspond to the post-crash phase [16].
Furthermore, the injured victims, according to their clinical status and Glasgow Coma Score (GCS) that had been adapted for Guinea [17], can stay in the emergency unit for up to 24 h at which time they are either discharged home or admitted to an appropriate departmental ward (surgical, orthopedic or intensive care unit). The emergency unit case files of those admitted are transferred to the wards, and in these case files and in the ward registers, a record is made of types of intervention, duration of hospital stay and discharge outcome including death. In addition, police stations record all reported RTA cases along with number of victims, with or without injury and death, and hospitals also record details of all admitted RTA victims even those with no injuries.
Emergency units and admission to hospitals departments
In Conakry, the public health hospitals included the three national tertiary hospitals and five communal medical centers, all of which have an emergency unit. The two frequently used private hospitals and one private clinic, which all had an emergency unit, were also included, giving a total of 11 hospitals in Conakry. In each of the seven urban districts, the referral district hospital and two private clinics that had an emergency unit were included, giving a total of 20 hospitals.
Study population
All RTA and all persons involved in RTA registered at the selected police stations and public/private hospitals in eight urban districts of Guinea between January 2015 and December 2017 were included in the study.
Data variables, sources of data and data collection
Police station data variables included: month and year of RTA; type of RTA (motor vehicle, motorcycle, bicycle, motor vehicle + motor vehicle, motor vehicle + motorcycle, motor vehicle + bicycle, motor vehicle + pedestrian, motorcycle + motorcycle, motorcycle + bicycle, motorcycle + pedestrian); persons involved in the RTA along with injury (minor or severe) and death. Data were collected from RTA registers at the eight selected police stations. Data from one police station were not included because these were raw annual aggregated data rather daily or monthly.
Hospital data variables included: age, sex, occupation, type of road user, month and year of admission to the emergency unit, type of hospital (public or private), predominant type and anatomical location of the injury, GCS (Normal = 15; Mild coma = 14–10; Heavy coma = 9–7; Deep coma = 6–3), interventions, hospital departmental wards, hospital discharge outcomes (including death, abscondment or transfer to another facility) and date of discharge. The WHO definition of death due to RTA is “death within 30 days of an RTA” [18], but since this was a retrospective study, we, in this paper defined “hospital deaths” as death that occurred at the hospital emergency unit and after admission to a hospital department. Data were also collected on the total number of all patients admitted to emergency units in the three-year period.
Data sources were the registers of the emergency units and hospital departmental wards (surgery, orthopedic and intensive care units) in 20 hospitals of the selected districts. A standardized Excel spreadsheet (version 2016) was used to collect the information from the different registers at police stations and hospitals. The data were collected by a team of 11 trained health professionals, supervised by the principal investigator, between April and August 2018.
Analysis
Data from the Excel spreadsheet were exported into EpiData (version 2.2.2.182, EpiData Association, Odense, Denmark) for analysis. Results were analyzed using descriptive statistics (proportions, measures of central tendency, and variation). Selected socio-demographic and clinical characteristics were assessed in relation to hospital deaths using the chi square test and results presented as relative risks (RR) along with 95% confidence intervals (CI). The level of significance was set at 5% (P < .05).
The trends of RTA and their impacts were also assessed through compiling the existing data across the eight districts and a sequence of interrupted time-series models was estimated, one each for the number of RTA, injuries and death across the study periods: 2015, 2016 and 2017. Segmented ordinary least-squares (OLS) regression were employed using Newey-West standard errors to accommodate for serial auto-correlation [19, 20], and adjusted for any potential effect of seasonality (e.g., rainy versus dry) on the outcomes. The interrupted time-series regression model followed the format:
where β0 estimates the rate of the indicator of interest per 100,000 population at the beginning of 2015, β1 estimates the average monthly change in the indicator rate during 2015, Tt is the time in months since the start of the study, β2 represents the change in the indicator rate that occurred in 2016 and 2017 (2017 designated by indicator variable Xt), β3 represents the difference between the trend in indicator rate during 2016 and 2017 compared to 2015, βm represents rainy versus dry season, and ϵt the random error term [20]. Autocorrelation of up to three logs was accommodated within our models [21, 22]. Overall trends across the periods defining 2015, 2016 and 2017 were calculated as follows: linear trend during 2015 = β1; and linear trend in 2016 and 2017 = β1 + β3. Differences were considered statistically significant at p < .05.
Results
Police station records
There was a total of 3,140 RTA with annual and monthly trends shown in Fig. 1. There was an overall annual increase in RTA rates from 14.0 per 100 000 population in 2015, to 19.2 per 100 000 population in 2016 (37.1% annual increase), to 28.7 per 100 000 population in 2017 (49.5% annual increase).
Fig. 1.
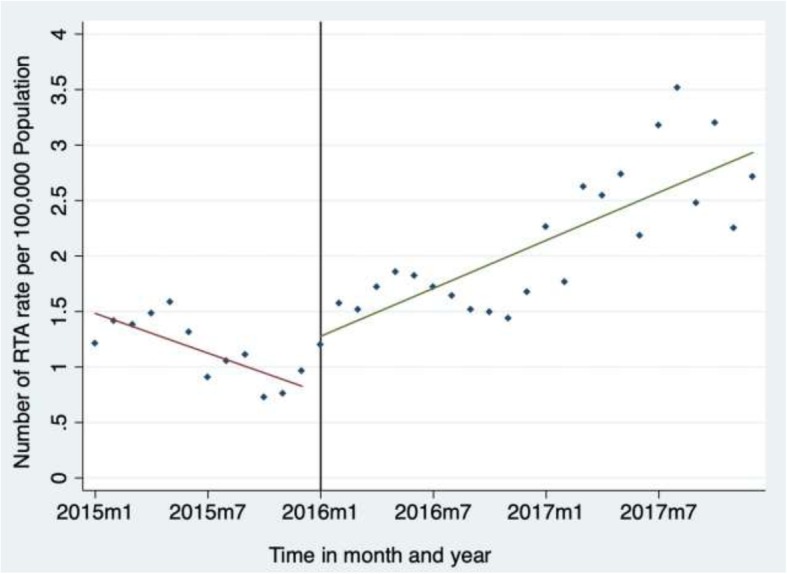
Annual and monthly trends in rates of road traffic accidents (RTA) recorded by police stations in seven districts of Guinea from 2015 to 2017. RTA rates per 100,000 population. Fitted values. Fitted values. m1: first month (January) of each year (2015, 2016 and 2017). m7: seventh month (July) of each year (2015, 2016 and 2017)
The time-series analysis is shown in Table 1. In the first month of 2015, there were 1.39 RTA cases per 100 000 population (95% CI: 1.21–1.57). During 2015, there was a mean decrease in RTA rate of −.06 per 100 000 population (95% CI: − 0.10, − 0.03) per month. Compared to the trend in RTA rates observed during 2015, the trend in RTA rates in 2016 and 2017 were .14 per 100 000 population higher (95% CI: .10–.19). Overall, the rate of RTA during 2016 and 2017 increased by .07 per 100 000 population on average per month. For injuries, there were .77 RTA victims injured per 100 000 population (95% CI: .66–.88) in January 2015. Over the same year (2015), there was a mean decrease in injury rates of − 0.02 per 100 000 population (95% CI: −.03–.00) per month. Compared to the trend in injury rates during 2015, the trend in injury rates in 2016 and 2017 increased by .07 per 100 000 population (95% CI: .04–.09). Globally, the injury rate during 2016 and 2017 was .05 per 100 000 population (95% CI: .03–.07) higher on average per month. Deaths from RTA showed no statistical difference over the 3 years. There were no associations of RTA trends with season.
Table 1.
Parameter estimates for monthly RTA, injuries and deaths from 2015 to 2017 in the selected eight urban districts, Guinea from 2015 to 2017
| RTA | Injuries | Deaths | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | P | β | 95% CI | P | β | 95% CI | P | |
| Rate of outcome in 2015 (β0) | 1.39 | (1.21; 1.57) | <.001 | .77 | (.66; .88) | <.001 | .13 | (.03; .27) | .0460 |
| Average monthly change in rate in 2015 (β1) | −.06 | (−.10; −.03) | <.001 | −.02 | (−.03; −.00) | .0470 | .01 | (−.02; .01) | .3430 |
| Change in rate from 2015 to 2016 and 2017 (β2) | −.56 | (.19;.93) | .0040 | .01 | (−.21; .24) | .9120 | −.00 | (−.07; .02) | .9850 |
| Difference between trend in outcome rate in 2016 and 2017 compared to 2015 (β3) | .14 | (.10; .19) | <.001 | .07 | (.04; .09) | <.001 | .01 | (−.01; .02) | .2800 |
| Overall trends | |||||||||
| Linear Trend in 2015 Period (β1) | −.06 | (−.10; −.03) | <.001 | −.02 | (−.03; −.00) | .0470 | .01 | (−.02; .01) | .3430 |
| Linear Trend in 2016 and 2017 (β1 + β3) | .07 | (.05; .09) | <.001 | .05 | (.03; .07) | <.001 | 0 | (−.00; .00) | .3039 |
For each type of RTA, there was an annual increase from 1 year to the next as shown in Fig. 2. The most common type of RTA involved a combination of two vehicles (motor vehicles and/or motor cycles) representing 76% of all RTA cases. This was followed by collisions of a vehicle with pedestrians (13%) and a motor vehicle or motor cycle alone (9%). Motorcycle accidents increased dramatically in the three-year period from 12.0% (2015) to 30.7% (2017).
Fig. 2.

Annual trends in types of road traffic accident (RTA) recorded by police stations in seven districts of Guinea from 2015 to 2017. (a): vehicle + pedestrian; motorcycle + pedestrian. (b): motorcycle + bicycle; motor vehicle + bicycle; bicycle alone; not recorded. Note: there were 10 RTA with no information recorded
In 925 RTA, there was no record of the number of persons involved. In the remaining 2,215 RTA, there were 4,340 persons involved resulting in 40% being injured and 4% being killed (Fig. 3).
Fig. 3.

Annual trends in injuries and deaths among road traffic accident (RTA) victims recorded by police stations in seven districts of Guinea from 2015 to 2017. Of the 1717 injuries, 870 (51%) were minor and 847 (49%) were severe based on the opinion of the receiving health facility
Hospital records
There was a total of 27,751 RTA victims admitted to hospital emergency units: this comprised 22% of the 125,882 persons admitted with all types of illness during the 3 years. The annual rate of RTA victims decreased from 177.3 per 100 000 population in 2015 to 164.5 per 100 000 population in 2016 and then increased at 210.1 per 100 000 population in 2017 (27.7% annual increase).
Socio-demographic characteristics of RTA victims are shown in Table 2. The commonest age group was 15–24-year old (33%) and more males (71%) were victims than females. There was no clear pattern regarding occupation. In two thirds of cases, there was no information about the type of road user involved in the RTA. In the other one third of victims, passengers, motorcyclists and pedestrians were the most affected group.
Table 2.
Sociodemographic characteristics of road traffic accident victims admitted to hospital emergency units in eight districts of Guinea from 2015 to 2017
| Characteristics | N | (%) |
|---|---|---|
| Age in years | ||
| <15 | 4395 | (15.8) |
| 15–24 | 9132 | (32.9) |
| 25–34 | 6855 | (24.7) |
| 35–44 | 3241 | (11.7) |
| 45–64 | 3052 | (11) |
| ≥65 | 913 | (3.3) |
| Not recorded | 163 | (0.6) |
| Sex | ||
| Male | 19747 | (71.2) |
| Female | 7991 | (28.8) |
| Not recorded | 13 | (0.0) |
| Occupation | ||
| Students | 7151 | (25.8) |
| Work men/women | 7120 | (25.7) |
| Farmer/housewife | 5186 | (18.7) |
| Sellers | 3372 | (12.2) |
| Employees | 2513 | (9.1) |
| Children (< 15 and not a student) | 1723 | (6.2) |
| Not recorded | 686 | (2.5) |
| Type of road user | ||
| Passengers | 4626 | (16.7) |
| Motorcyclists | 3092 | (11.1) |
| Pedestrians | 1129 | (4.1) |
| Drivers | 60 | (0.2) |
| Pedal cyclists | 56 | (0.2) |
| Not recorded | 18788 | (67.7) |
RTA Road traffic accident
Clinical characteristics of RTA victims are shown in Table 3. The large majority of victims presented to hospitals and 86% were managed in the emergency unit without being admitted to hospital wards. The predominant injury involved soft tissue and about 10% of victims sustained a fracture, usually of the lower limbs. The head and lower limbs were the two commonest anatomical sites of injury. Most patients had a normal Glasgow coma score, but 1.9% of all RTA victims had heavy or deep coma.
Table 3.
Clinical characteristics of road traffic accident victims admitted to hospital emergency units in eight districts of Guinea from 2015 to 2017
| Characteristics | N | (%) | |
|---|---|---|---|
| Type of hospital | Public hospitals | 27348 | (98.5) |
| Private hospitals | 403 | (1.5) | |
| Admission to hospital departments | No hospital admission | 23240 | (83.6) |
| Surgery department | 2171 | (7.8) | |
| Orthopedic department | 546 | (2.0) | |
| Intensive care unit | 207 | (0.7) | |
| Neurosurgery department | 17 | (< 0.1) | |
| Not recorded | 824 | (3) | |
| Predominant type of injury | Soft tissue | 21160 | (76.2) |
| Facture | 2682 | (9.7) | |
| Joint | 377 | (1.4) | |
| Dislocation | 295 | (1.1) | |
| Main anatomical site of injury | Head | 10350 | (37.3) |
| Lower limb | 9179 | (33.1) | |
| Upper limb | 5514 | (19.9) | |
| Chest | 604 | (2.2) | |
| Abdominal –Lumbar | 951 | (3.4) | |
| Location of fracture | Lower limb | 1770 | (6.4) |
| Upper limb | 764 | (2.8) | |
| Mandible | 164 | (0.6) | |
| Ribs | 61 | (0.2) | |
| Glasgow Coma Score a | Normal | 25769 | (92.9) |
| Mild coma | 1185 | (4.3) | |
| Heavy coma | 327 | (1.2) | |
| Deep coma | 201 | (0.7) | |
| Not recorded | 269 | (1.0) | |
RTA Road traffic accident, Glasgow coma score- normal = 15; mild coma = 14–10; heavy coma = 9–7; deep coma = 6 = 3
Hospital interventions are shown in Table 4. Skin cleansing and simple bandaging together comprised 69.1% of all interventions, but 13.5% required general surgery (usually minor in nature) and 4% had reductions or fixations of their fractures.
Table 4.
Medical and surgical interventions on road traffic accident victims admitted to hospital emergency units in eight districts of Guinea from 2015 to 2017
| Medical and surgical interventions | N | (%) |
|---|---|---|
| Total number of medical and surgical interventions | 34832 | |
| Skin cleansing | 15393 | (44.2) |
| Simple bandaging | 8672 | (24.9) |
| Fracture reduction or fixation | 1322 | (3.8) |
| Blood transfusion | 28 | (< 0.1) |
| Neurological surgery | 17 | (< 0.1) |
| General Surgery | 4704 | (13.5) |
| Minor | 4416 | (12.7) |
| Complex | 280 | (0.8) |
Of 27,751 RTA victims, there were 0.7% victims who were dead on arrival and 0.6% who died in the emergency department (all the deaths occurred within 24 h with the time of death recorded in 67% of patients). About 14% of victims were admitted to hospital wards, 84% were discharged home. Of those admitted to hospital wards, about 1% of the victims died. About 58% were discharged home with the remainder absconding from hospital or transferring to another hospital. Also, 27% of the patients had no record about their outcomes (Fig. 4). The median duration of hospital stay was 5 days (IQR = 1–20).
Fig. 4.
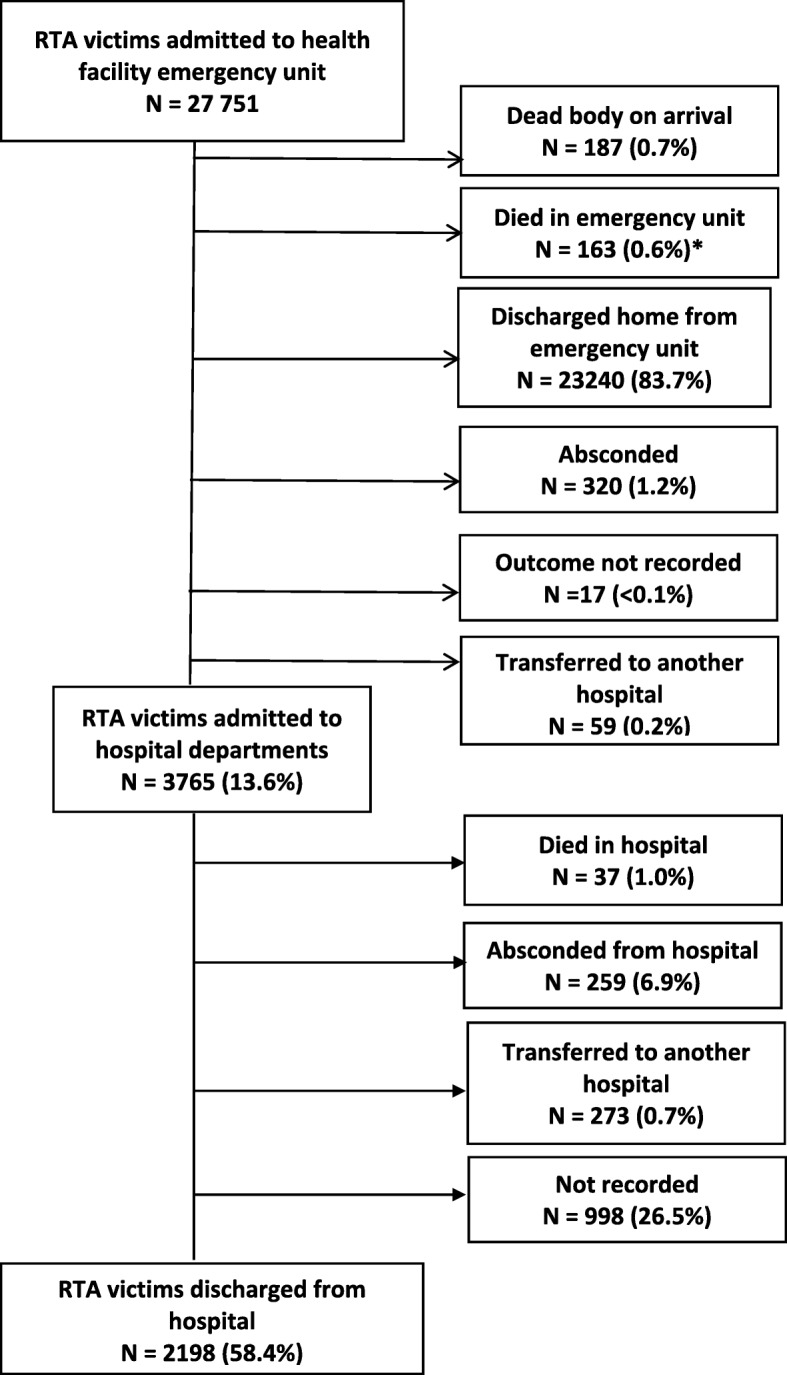
Outcomes of road traffic accident victims presenting to emergency units of health facilities and admitted to hospital in eight districts of Guinea from 2015 to 2017. RTA = road traffic accident. *109 patients died within 24 h and 54 died in the emergency unit but the time was not recorded
Altogether there were 1.4% deaths of all RTA victims admitted to hospitals. The death rate ranged from 2.4 per 100 000 population in 2015 to 3.7 in 2017. Baseline risk factors for death after admission to hospital are shown in Table 5. Factors associated with death were being male (p = .04), being a child under 15 years (p = .045) or an elderly person aged ≥65 years (p < .001), and having head injury or coma (p < .001). The risk of death in relation to lower GCS increased progressively, with 54% of those in heavy or deep coma dying in hospital.
Table 5.
Selected baseline characteristics associated with risk of death in road traffic accident victims admitted to hospital in eight districts of Guinea from 2015 to 2017
| Baseline characteristics | Admitted to hospital | Known death occurring after presentation to a hospitalb | Crude RRc (95% CI) |
P value | ||
|---|---|---|---|---|---|---|
| Na | n | (%) | ||||
| Sex: | ||||||
| Female | 7691 | 45 | (0.59) | Ref | ||
| Male | 18850 | 155 | (0.82) | 1.41 (1.01–1.96) | 0.04 | |
| Not recorded | 8 | 0 | ||||
| Age in years | Children (< 15) | 4238 | 40 | (0.94 | 1.43 (1.01–2.02) | 0.045 |
| Adults (15–64) | 21321 | 141 | (0.60) | Ref | ||
| Elderly (≥65) | 855 | 16 | (1.87) | 2.83 (1.70–4.72) | < 0.001 | |
| Not recorded | 135 | 3 | (2.22) | |||
| Type of hospital | Public | 26159 | 197 | (0.75) | Ref | |
| Private | 390 | 3 | (0.77) | 1.02 (0.33–3.18) | 0.999 | |
| Main anatomical site of injury | ||||||
| Head | No | 16739 | 72 | (0.43) | Ref | |
| Yes | 981 | 128 | (1.31) | 3.01 (2.26–4.01) | < 0.001 | |
| Not recorded | 9 | 0 | ||||
| Chest | ||||||
| No | 25960 | 196 | (0.76) | Ref | ||
| Yes | 585 | 3 | (0.51) | 0.68 (0.22–2.12) | 0.717 | |
| Not recorded | 4 | 1 | ||||
| Abdominal | ||||||
| No | 26158 | 196 | (0.75) | Ref | ||
| Yes | 389 | 4 | (1.30) | 1.37 (0.51–3.67) | 0.674 | |
| Not recorded | 2 | 0 | ||||
| Glasgow Coma Score | ||||||
| Normal | 24945 | 75 | (0.30) | Ref | ||
| Mild coma | 1134 | 21 | (1.85) | 6.16 (3.81–9.96) | < 0.001 | |
| Heavy | 286 | 53 | (18.53) | 8.45 (5.96–11.98) | < 0.001 | |
| Dep coma | 59 | 21 | (35.59) | 178.4 (118.5–178.5) | < 0.001 | |
| Not recorded | 125 | 30 | ||||
a = 187 RTA victims dead on arrival, 998 RTA victims with unrecorded unit of admission and those who absconded were excluded
b = includes death occurring in hospital emergency unit and after admission to a hospital department
RR Relative risk, CI Confidence interval
c = Fisher exact test
Discussion
This is the first study in Guinea to comprehensively examine RTA in eight districts where there have been reports of a high burden of RTA in the past years, using both data from hospitals and police stations. There were three main findings.
First, according to police records, the burden of RTA increased during the three-year study period. Over three quarters of RTA involved two vehicles, which may relate to the growing number of motor vehicles on the road. The rise in the rate of RTA cases was accompanied by a similar rise in the rate of RTA victims. These findings are in line with previous studies from other African countries [6, 7, 10].
Even though we did not assess why the burden of RTA has increased, there might be several possible reasons. First, improvements in socio-economic standards and the production of more affordable second-hand vehicles imported from European countries and motorcycles imported from India and China have led to a growing number of vehicles on the roads. Road safety legislation, road infrastructure and affordable ways to maintain vehicles have not kept pace with the surge in vehicle numbers. Studies in Gambia, Burkina Faso and Tanzania have shown that many injuries occur at hot spots such as road intersections with or without traffic lights, during rush hours and at night [23–25], and these factors may play a part in Guinea. Human behavior also plays an important role with speeding, careless driving and driving under the influence of alcohol being important factors contributing to RTA in many countries, and probably also in Guinea [26, 27].
Second, according to police records, 40% of RTA victims were injured and were referred to hospital. These numbers were much lower than the numbers admitted to emergency units according to hospital records. Reasons for the observed discrepancies are speculative but include lack of information about injuries in police records and self-reporting of RTA victims to hospital without involving the police. From hospital records, over 27,000 RTA victims were admitted to emergency units during the study period. This resulted in an increased workload for hospitals requiring more staff and resources. The fact that most RTA victims presenting to hospital emergency units were discharged home and did not require admission to a hospital ward contrast with some studies reporting higher RTA-related morbidity and mortality [27, 28]. This discrepancy may be explained by the fact that those RTA victims who were discharged home had minor injuries such as scratches or slight confusion. However, our findings are similar to those conducted in Ethiopia and Gambia which found low rates of hospital admission and deaths [11, 23].
Males and young adults were predominant among the RTA victims which concurs with studies from everywhere including industrialised countries [23, 25, 29–31]. The reasons that male and young adults are predominant are several. It relates to their inexperience [32] and the fact that they are a very active group on the roads, i.e. they drive more than other groups. Furthermore, higher exposure (mileage) together with psychological factors (sensation seeking, peer influence, driving under the influence of alcohol) make them a risky group [33, 34]. Injuries to the head and limbs and soft tissue trauma were the predominant types of injury, confirming findings from a study in Gambia [23].
Third, serious injury resulted in death but altogether just over 1% of all RTA victims died. This mortality may be underestimated as a quarter or more of patients admitted to hospital had no record of their outcome. In addition, we could not document the outcomes in those transferred to hospitals other than those included in the study. The case-fatality rate observed in our study was therefore lower than what has been reported in other studies [7, 28, 35, 36]. However, it was similar to the general low morbidity and mortality rates reported in Ethiopia and Gambia [11, 23]. According to the police records, the numbers of fatal RTA at the scene of the accident remained the same over the 3 years. These findings, therefore, call for urgent attention to address this growing health threat by putting in place a solid surveillance system through enforcement of the police stations’ capacity to control road traffic, improve the design of roads and keep in place periodic education of people to prevent RTA fatality and guarantee the safety of road users.
In hospital records, nearly half of the deaths occurred at the site of the RTA with the remainder occurring within 24 h. Risk factors for death in those admitted to hospital included being male, a child or an elderly person, having an injury involving the head and being in coma with progressively lower GCS predicting higher probabilities of death. These findings are similar to previous reports on the subject [37].
This study had several strengths. First, the selection of eight urban districts as study sites meant that we covered 45% of the national population, and our findings are probably representative of what is happening in Guinea. Second, we collected data from police stations and hospitals, and while these could not be linked, they nevertheless provide a more holistic picture of RTA in Guinea. Such an approach of using different data sources has been recently recommended as a way of improving data collection and completeness of information about road traffic injury [37]. Third, hospital data were individual-based and thus provided information on RTA victims from admission to emergency units to their outcomes. Finally, the study was conducted and reported in line with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [38].
However, there were some limitations. Some information in the police station records were missing, such as numbers of injured persons and in hospital records, such as details about road users. Valuable information in police records was also not regularly captured such as whether 4-wheel vehicles involved in RTA were cars, taxis, buses or trucks, the potential cause of the accident such as speeding and/or drunk-driving and whether safety belts or crash helmets were worn by drivers and passengers.
There are a number of implications and recommendations from this study. First, there needs to be a serious attempt to improve the recording practices in both police and hospital records, especially about potential causes of RTA, the number of people involved, the type of motor vehicle and the time taken to get victims to hospital. There also needs to be better oversight so that unrecorded outcomes are minimized. In parts of the country where the burden of RTA is high, consideration should be given to using and linking electronic records in both police station and hospital sites. This would facilitate better tracking of RTA and victims from the site of the accident to hospital and to an eventual outcome.
Second, with the increasing numbers of RTA and their victims, the country is not on track to halve RTA by 2020 as pledged in the SDGs [4]. What can be done quickly to reduce the numbers of RTA? Geographic information systems have been set up in Tanzania to identify hot spots of RTA [25], and Guinea should consider setting up similar systems. The country also needs to enforce road safety legislation about drink-driving and speeding, improve infrastructure through more paved and better designed roads, roadway lighting and roundabouts and tighten up measures around vehicle safety [26]. Moreover, police stations and hospitals should consider using a checklist when recording RTA information to capture data about availability of first-aid, easy access to hospital and causes of RTA such as human attitudes [16]. Community-based awareness campaigns might also help [39].
Finally, attention needs to be given to reducing the risk of serious injury and death. The most successful interventions to prevent RTA death are speed and drink-driving enforcement [26]. However, RTA deaths can also be reduced by the availability of fast and reliable emergency services in rural areas, the use of telemetric systems including automated accident notification systems connected to emergency services and post traumatic rehabilitation services to prevent complications [40, 41]. These interventions should be prioritized at all levels along with bicycle and motorcycle helmet use and seat-belt use for front and rear passengers.
Conclusions
Between 2015 and 2017, there was an increase in RTA and numbers of RTA victims in Guinea. The burden on hospitals was high with over 20% of emergency unit admissions being due to RTA. The majority of victims admitted to emergency units were discharged home, but nearly 15% required hospital ward admission. Altogether, there was a low proportion of deaths but about half of the deaths occurred before hospital admission and most of the remainder occurred in the emergency unit and within 24 h. Risk factors for death in those admitted to hospital included being male, a child or elderly person and having head injury and coma. More needs to be done in Guinea to reduce RTA and prevent serious injury and death.
Acknowledgements
This research was conducted through the Structured Operational Research and Training Initiative (SORT IT), a global partnership led by the Special Programme for Research and Training in Tropical Diseases at the World Health Organization (WHO/TDR). The training model is based on a course developed jointly by the International Union Against Tuberculosis and Lung Disease (The Union) and Medécins sans Frontières (MSF). The specific SORT IT program which resulted in this publication was implemented by: Medécins Sans Frontières, Brussels Operational Centre, Luxembourg and the Centre for Operational Research, The Union, Paris, France. Mentorship and the coordination/facilitation of these SORT IT workshops were provided through the Centre for Operational Research, The Union, Paris, France; the Operational Research Unit (LuxOR); AMPATH, Eldoret, Kenya; The Institute of Tropical Medicine, Antwerp, Belgium; The Centre for International Health, University of Bergen, Norway; University of Washington, USA; The Luxembourg Institute of Health, Luxembourg; The Institute of Medicine, University of Chester, UK; The National Institute for Medical Research, Muhimbili Medical Research Centre, Dar es Salaam, Tanzania. We also thank Dr. Alison M. El Ayadi for her help with the time-series analysis of RTA trend (University of California, San Francisco).
Abbreviations
- CI
Confidence Intervals
- GCS
Glasgow Coma Score
- IQR
Inter Quartile Range
- OLS
Ordinary Least-Squares
- RR
Relative Risk
- RTA
Road traffic accidents
- SDG
Sustainable Development Goals
- STROBE
Strengthening the Reporting of Observational Studies in Epidemiology
- WHO
The World Health Organization
Authors’ contributions
KK, SA and ADH designed the study, performed the statistical analyses, the interpretation, and wrote the draft manuscript. PO and MM contributed to the analysis. DK, BSC, LL, SS, AHB and AD contributed to the design, analysis and critically revised successive version of the article. All authors read and approved the final manuscript before submission.
Funding
The programme was funded by: The United Kingdom’s Department for International Development (DFID); La Fondation Veuve Emile Metz-Tesch supported open access publications costs. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
All data generated or analyzed during this study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Ethics approval was obtained from the Guinean Ethics Review Board (Number – 055/CNERS/18) and the Union Ethics Advisory Group (EAG) (International Union against Tuberculosis and Lung Disease, Paris, France – EAG number 04/18). No names were used for data collection and because this was already collected secondary data, patient consent was not required.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Karifa Kourouma, Phone: (+224) 628-765-320, Email: KKourouma@maferinyah.org.
Alexandre Delamou, Email: adelamou@gmail.com.
Léopold Lamah, Email: leolamah@yahoo.fr.
Bienvenu Salim Camara, Email: bienvenusalimcamara@gmail.com.
Delphin Kolie, Email: dkolie@maferinyah.org.
Sidikiba Sidibé, Email: layesidikiba@gmail.com.
Abdoul Habib Béavogui, Email: beavoguia_h@yahoo.com.
Philip Owiti, Email: philip.owiti@gmail.com.
Marcel Manzi, Email: marcel.manzi@luxembourg.msf.org.
Serge Ade, Email: adeserg@yahoo.fr.
Anthony D. Harries, Email: adharries@theunion.org
References
- 1.WHO | World Health Organization. Global Status Report on Road Safety Summary 2018. [cited 2019 Apr 23]. Available from: https://www.who.int/violence_injury_prevention/road_safety_status/2018/English-Summary-GSRRS2018.pdf.
- 2.GBD 2016 Causes of Death Collaborators Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151–1210. doi: 10.1016/S0140-6736(17)32152-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Bank. The high toll of traffic injuries: unacceptable and preventable. 2017. Available from: https://openknowledge.worldbank.org/handle/10986/29129. [cited 2019 May 27]
- 4.United Nations . Transforming our world: the 2030 Agenda for sustainable development. 2015. [Google Scholar]
- 5.WHO World Health Organization. Global status report on road safety 2013: Supporting a decade of action. World Heal Organ. 2013;1:318. [Google Scholar]
- 6.Adeloye D, Thompson JY, Akanbi MA, Azuh D, Samuel V, Omoregbe N, et al. The burden of road traffic crashes, injuries and deaths in Africa: a systematic review and meta-analysis. Bull World Health Organ. 2016;94(7):510–521A. doi: 10.2471/BLT.15.163121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vissoci JRN. Road traffic injury in sub-Saharan African countries: a systematic review and summary of observational studies. Traffic Inj Prev. 2017;18(7):767–773. doi: 10.1080/15389588.2017.1314470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.WHO | World Health Organization, editor. Global status on road safety. 2015. [Google Scholar]
- 9.Juillard C, Labinjo M, Kobusingye O, Hyder AA. Socioeconomic impact of road traffic injuries in West Africa: exploratory data from Nigeria. Inj Prev. 2010;16(6):389–392. doi: 10.1136/ip.2009.025825. [DOI] [PubMed] [Google Scholar]
- 10.Onyemaechi NOC, Ofoma UR. The public health threat of road traffic accidents in Nigeria: a call to action. Ann Med Health Sci Res. 2016;6(5):199–204. doi: 10.4103/amhsr.amhsr_452_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Getachew S, Ali E, Tayler-Smith K, Hedt-Gauthier B, Silkondez W, Abebe D, et al. The burden of road traffic injuries in an emergency department in Addis Ababa, Ethiopia. Public Heal Action. 2016;6(2):66–71. doi: 10.5588/pha.15.0082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Institut National de la Statistique INS; Ministère du Plan et de la Coopération Internationale. Annuaire Statistique 2016. Conakry, Guinée; 2017. [cited 2019 May 28]. Available from: http://www.stat-guinee.org/images/Publications/INS/annuelles/INS_annuaire_2016.pdf
- 13.Mamady Keita, Zou Bin, Mafoule Sylla, Qin Jiabi, Hawa Keita, Lamine Keita Fodé, Hu Guoqing. Fatality from Road Traffic Accident in Guinea: A Retrospective Descriptive Analysis. Open Journal of Preventive Medicine. 2014;04(11):809–821. doi: 10.4236/ojpm.2014.411091. [DOI] [Google Scholar]
- 14.WHO | World Health Organization, editor. Road Safety: Estimated road traffic death rate (per 100 000 population) 2016. [Google Scholar]
- 15.Béavogui K, Koïvogui A, Loua TO, Baldé R, Diallo B, Diallo AR, et al. Traumatic brain injury related to motor vehicle accidents in Guinea: impact of treatment delay, access to healthcare, and Patient’s financial capacity on length of hospital stay and in-hospital mortality. J Vasc Interv Neurol. 2015;8(4):30–38. [PMC free article] [PubMed] [Google Scholar]
- 16.Haddon W., Jr Options for the prevention of motor vehicle crash injury. Keynote address. Isr J Med Sci. 1980;16(1):45–65. [PubMed] [Google Scholar]
- 17.Reith FCM, Van den Brande R, Synnot A, Gruen R, Maas AIR. The reliability of the Glasgow coma scale: a systematic review. Intensive Care Med. 2016;42(1):3–15. doi: 10.1007/s00134-015-4124-3. [DOI] [PubMed] [Google Scholar]
- 18.Peden M, Scurfield R, Sleet D, Mohan D, Hyder AA, Jarawan E, Mathers C. World report on road traffic injury prevention. 2004. [Google Scholar]
- 19.Newey WK, West KD. A simple, positive semi-definite, Heteroskedasticity and autocorrelation consistent covariance matrix. Econometrica. 1987;55(3):703. doi: 10.2307/1913610. [DOI] [Google Scholar]
- 20.Linden A. ITSA: Stata module to perform interrupted time series analysis for single and multiple groups. Stat Softw Components. 2017; Available from: https://ideas.repec.org/c/boc/bocode/s457793.html. [cited 2019 May 28].
- 21.Cumby Robert E., Huizinga John. Testing the Autocorrelation Structure of Disturbances in Ordinary Least Squares and Instrumental Variables Regressions. Econometrica. 1992;60(1):185. doi: 10.2307/2951684. [DOI] [Google Scholar]
- 22.Baum CF, Schaffer ME, Baum C, Schaffer M. ACTEST: Stata module to perform Cumby-Huizinga general test for autocorrelation in time series. 2015. [Google Scholar]
- 23.Sanyang Edrisa, Peek-Asa Corinne, Bass Paul, Young Tracy L., Daffeh Babanding, Fuortes Laurence J. Risk Factors for Road Traffic Injuries among Different Road Users in the Gambia. Journal of Environmental and Public Health. 2017;2017:1–9. doi: 10.1155/2017/8612953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bonnet E, Nikiéma A, Traoré Z, Sidbega S, Ridde V. Technological solutions for an effective health surveillance system for road traffic crashes in Burkina Faso. Glob Health Action. 2017;10(1):1295698. doi: 10.1080/16549716.2017.1295698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Reardon JM, Andrade L, Hertz J, Kiwango G, Teu A, Pesambili M, et al. The epidemiology and hotspots of road traffic injuries in Moshi, Tanzania: an observational study. Injury. 2017;48(7):1363–1370. doi: 10.1016/j.injury.2017.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vecino-Ortiz AI, Jafri A, Hyder AA. Effective interventions for unintentional injuries: a systematic review and mortality impact assessment among the poorest billion. Lancet Glob Heal. 2018;6(5):e523–e534. doi: 10.1016/S2214-109X(18)30107-4. [DOI] [PubMed] [Google Scholar]
- 27.Wangdi C, Gurung MS, Duba T, Wilkinson E, Tun ZM, Tripathy JP. Burden, pattern and causes of road traffic accidents in Bhutan, 2013–2014: a police record review. Int J Inj Control Saf Promot. 2018;25(1):65–69. doi: 10.1080/17457300.2017.1341930. [DOI] [PubMed] [Google Scholar]
- 28.Tékpa BJD, Diemer HC, Mapouka PAI, Ngatchokpo VN, Gassima B, Nali MN. La mortalité au cours des accidents de la circulation routière à Bangui, République centrafricaine. Med Sante Trop. 2017;27(4):426–430. doi: 10.1684/mst.2017.0745. [DOI] [PubMed] [Google Scholar]
- 29.Birua GS, Munda V, Murmu N. Epidemiology of spinal injury in north East India: a retrospective study. Asian J Neurosurg. 2018;13(4):1084. doi: 10.4103/ajns.AJNS_196_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Barrimah I, Midhet F, Sharaf F. Epidemiology of road traffic injuries in Qassim Region, Saudi Arabia: consistency of Police and health data. Int J Health Sci (qassim) 2014;6(1):31–42. doi: 10.12816/0005971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Moreira MR, Ribeiro JM, Motta CT, Motta JIJ. Mortalidade por acidentes de transporte de trânsito em adolescentes e jovens, Brasil, 1996-2015: cumpriremos o ODS 3.6? Cien Saude Colet. 2018;23(9):2785–2796. doi: 10.1590/1413-81232018239.17082018. [DOI] [PubMed] [Google Scholar]
- 32.Box E, Wengraf I. Young driver safety: solutions to an age-old problem. 2013. [Google Scholar]
- 33.Bachoo S, Bhagwanjee A, Govender K. The influence of anger, impulsivity, sensation seeking and driver attitudes on risky driving behaviour among post-graduate university students in Durban, South Africa. Accid Anal Prev. 2013;55:67–76. doi: 10.1016/j.aap.2013.02.021. [DOI] [PubMed] [Google Scholar]
- 34.Constantinou E, Panayiotou G, Konstantinou N, Loutsiou-Ladd A, Kapardis A. Risky and aggressive driving in young adults: personality matters. Accid Anal Prev. 2011;43(4):1323–1331. doi: 10.1016/j.aap.2011.02.002. [DOI] [PubMed] [Google Scholar]
- 35.Schlottmann F, Tyson AF, Cairns BA, Varela C, Charles AG. Road traffic collisions in Malawi: trends and patterns of mortality on scene. Malawi Med J. 2017;29(4):301–305. doi: 10.4314/mmj.v29i4.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Botchey Isaac M., Hung Yuen Wai, Bachani Abdulgafoor M., Saidi Hassan, Paruk Fatima, Hyder Adnan A. Understanding patterns of injury in Kenya: Analysis of a trauma registry data from a National Referral Hospital. Surgery. 2017;162(6):S54–S62. doi: 10.1016/j.surg.2017.02.016. [DOI] [PubMed] [Google Scholar]
- 37.Juillard C, Kouo Ngamby M, Ekeke Monono M, Etoundi Mballa GA, Dicker RA, Stevens KA, et al. Exploring data sources for road traffic injury in Cameroon: collection and completeness of police records, newspaper reports, and a hospital trauma registry. Surgery. 2017;162(6S):S24–S31. doi: 10.1016/j.surg.2017.01.025. [DOI] [PubMed] [Google Scholar]
- 38.von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495–1499. doi: 10.1016/j.ijsu.2014.07.013. [DOI] [PubMed] [Google Scholar]
- 39.Phillips RO, Ulleberg P, Vaa T. Meta-analysis of the effect of road safety campaigns on accidents. Accid Anal Prev. 2011;43(3):1204–1218. doi: 10.1016/j.aap.2011.01.002. [DOI] [PubMed] [Google Scholar]
- 40.Sihvola N, Luoma J, Schirokoff A, Salo J, Karkola K. In-depth evaluation of the effects of an automatic emergency call system on road fatalities. Eur Transp Res Rev. 2009;1(3):99–105. doi: 10.1007/s12544-009-0016-3. [DOI] [Google Scholar]
- 41.Üzümcüoǧlu Y, Özkan T, Lajunen T, Morandi A, Orsi C, Papadakaki M, et al. Life quality and rehabilitation after a road traffic crash: a literature review. Transp Res Part F Traffic Psychol Behav. 2016;40:1–13. doi: 10.1016/j.trf.2016.02.002. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are available from the corresponding author on reasonable request.