

Abstract
Cytochrome P450 2D6 (CYP2D6) is an important drug-metabolizing enzyme involved in the pharmacokinetic metabolism of drugs. CYP2D6 gene is highly polymorphic, and the combination of its different alleles yields different phenotypes including extensive metabolizer (EM), intermediate metabolizer (IM), poor metabolizer (PM), and ultrarapid metabolizer (UM). Genotyping of the important alleles for this gene in different ethnicities is of particular importance for assessing the efficacy of various drugs. In this study, we reviewed the CYP2D6 allele and phenotype frequencies predicted from the genotypes of CYP2D6 in the Middle East area. Regardless of different ethnicities, the CYP2D6*41 allele frequency was shown to be higher than that of other reduced functional alleles. In addition, CYP2D6*4 was the most frequent nonfunctional allele in all studied populations in the Middle East. Taken together, our findings illustrated that the frequencies of PM or IM alleles and different genotypes harboring these alleles are relatively high in the Middle Eastern countries. Therefore, the study of CYP2D6 alleles for each patient to detect those that are at risk is of great importance to prevent adverse drug reactions through individualization therapy.
Keywords: Allele frequency, cytochrome P450 2D6, Middle East
INTRODUCTION
Understanding the genetic pathways involved in pharmacokinetics and pharmacodynamics of the drugs can have a substantial effect on the personalized treatment of the patients.[1] Differences in patients’ response to drug treatment are partly due to individual differences in genetic constitution such as genes encoding drug-metabolizing enzymes.[2,3] Cytochrome P450 2D6 (CYP2D6) is one of the most important drug-metabolizing enzymes implicated in the metabolism of many clinical drugs such as antipsychotic drugs, antiarrhythmic agents, tricyclic antidepressants, β-blockers opioids, and anticancer drugs.[4,5] The CYP2D6 is a highly polymorphic gene, with more than 100 allelic variants being currently reported for.[6] The combination of different alleles yields different phenotypes such as extensive metabolizer (EM), intermediate metabolizer (IM), and poor metabolizer (PM) which have normal, reduced, and no activity of the enzyme, respectively.[7,8] The doubling of the gene that produces an enzyme with increased activity is also called the ultrarapid metabolizer (UM).[9,10] Interindividual differences in the kinetic characteristics of the drugs are partly attributed to the presence of alleles with altered activity.[11] Human variability in the kinetics of CYP2D6 substrates has been shown for different compounds metabolized extensively (>60%) by this polymorphic enzyme.[12]
Due to the effect of the CYP2D6 enzyme activity on drug metabolism, genetic studies of the gene in different populations are needed to determine the frequency of alleles in each ethnic group. This will help choose the effective treatment for the patients based on the genotype. The current study reviews the allele and genotype frequencies of CYP2D6 in the Middle East region. We searched in PubMed and Google Scholar from 1996 to 2017 using the combination of keywords such as CYP2D6, allele, and frequency plus the name of each country in the Middle East region. All studies reported CYP2D6 allele and genotype frequencies in different Middle Eastern countries including Saudi Arabia,[13,14] Egypt,[15,16,17,18,19,20,21] United Arab Emirates (UAE),[22,23] Iran,[24,25,26,27] Jordan,[28] Syria,[29] and Turkey[30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45] performed on healthy unrelated controls or patient samples were reviewed in this article. Overview of the studies evaluated in this review is listed in Table 1, showing the number of studies in each geographic region, number and type of samples (healthy or patients), list of alleles considered, and their frequency in each study.
Table 1.
Overview of the studies evaluated in this review
| Country (reference) | Number of individuals (n) | Subject type | Functional alleles | Reduced functional alleles | Nonfunctional alleles | Duplications | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1* | 2* | 10* | 17* | 41* | 3* | 4* | 5* | 6* | 2×× | |||
| Saudi Arabia[14] | 101 | Healthy | 79.1 | N/A | 3 | 3 | N/A | N/A | 3.5 | 1 | N/A | 10.4 |
| Saudi Arabia[13] | 192 | Healthy | 78.4 | N/A | N/A | N/A | 18.4 | 0 | N/A | N/A | 0 | N/A |
| Egypt[15] | 21+22 | Healthy + bladder cancer | 47.7 | N/A | N/A | N/A | N/A | 52.3* | N/A | N/A | ||
| Egypt[16] | 27+37 | Healthy + bladder cancer | 54.7 | N/A | N/A | N/A | N/A | 45.3* | N/A | N/A | ||
| Egypt[17] | 429+123 | Healthy + hypertensive cases | 85.1 | N/A | N/A | N/A | N/A | 14.9* | N/A | N/A | ||
| Egypt[18] | 11+32 | Healthy + acute leukemia | 53.5 | N/A | N/A | N/A | N/A | N/A | 46.5 | N/A | N/A | N/A |
| Egypt[20] | 308 | Healthy fertile and infertile | 74.4 | N/A | N/A | N/A | N/A | N/A | 25.6 | N/A | N/A | N/A |
| Egypt[21] | 29+30 | Healthy + chronic organophosphate exposed patients | 78 | N/A | N/A | N/A | N/A | N/A | 22 | N/A | N/A | N/A |
| Egypt[19] | 29+40 | Healthy + acute organophosphate exposed patients | 81.9 | N/A | N/A | N/A | N/A | N/A | 18.1 | N/A | N/A | N/A |
| Iran[25] | 100 | Healthy | 43.5 | 32 | 9 | 0 | N/A | N/A | 12.5 | 3 | N/A | N/A |
| Iran[26] | 100 | Healthy | 90 | N/A | N/A | N/A | N/A | 0.5 | 9 | N/A | 0.5 | N/A |
| Iran[27] | 101 | Breast cancer | 63.4 | N/A | N/A | N/A | N/A | N/A | 36.6 | N/A | N/A | N/A |
| Iran[24] | 300 | Healthy | 68.2 | N/A | 31.8 | N/A | N/A | N/A | 0 | N/A | N/A | N/A |
| Turkey[34] | 80+32 | Healthy + SLE patients | 85.3 | N/A | N/A | N/A | N/A | 0.4 | 14.3 | N/A | N/A | N/A |
| Turkey[41] | 53 | Ankylosing spondylitis patients | 84 | N/A | N/A | N/A | N/A | N/A | 16 | N/A | N/A | N/A |
| Turkey[45] | 100 | Healthy | 69 | N/A | 14.5 | N/A | N/A | 1 | 10 | 3 | 2.5 | N/A |
| Turkey[44] | 55+132 | Healthy + epileptic children patients | 81.8 | N/A | N/A | N/A | N/A | 0.8 | 17.4 | N/A | N/A | N/A |
| Turkey[43] | 30+60 | Responsive and nonresponsive FMF patients | 55 | N/A | N/A | N/A | N/A | 4.2 | 15.8 | 2.5 | 22.5 | N/A |
| Turkey[42] | 140+155+94 | Healthy + ALL + AML | 82.8 | N/A | N/A | N/A | N/A | 1.3 | 15.9 | N/A | N/A | N/A |
| Turkey[35] | 249 | Turkey with symptoms of arthritis, sacroiliac, joint and back pain | 87.8 | N/A | N/A | N/A | N/A | N/A | 12.2 | N/A | N/A | N/A |
| Turkey[32] | 160 | Healthy | 81 | N/A | N/A | N/A | 15 | N/A | N/A | N/A | N/A | N/A |
| Turkey[31] | 128+135 | Healthy + breast cancer patients | 66.3 | N/A | N/A | N/A | N/A | N/A | 33.7 | N/A | N/A | N/A |
| Turkey[38] | 52+100 | Healthy + ankylosing spondylitis patients | 83.9 | N/A | N/A | N/A | N/A | N/A | 16.1 | N/A | N/A | N/A |
| Turkey[33] | 140 | Healthy | 83.6 | N/A | N/A | N/A | N/A | 2.5 | 13.9 | N/A | N/A | N/A |
| Turkey[40] | 404 | Healthy | 37.06 | 35.3 | 6.06 | 1.11 | N/A | 0 | 11.3 | 1.49 | 0.74 | 1.98 |
| Turkey[37] | 100 | Healthy | 79 | N/A | N/A | N/A | N/A | N/A | 21 | N/A | N/A | N/A |
| Turkey[36] | 92 | Breast cancer patients | 42.4 | 19.6 | 6 | 0.6 | 15.2 | 1.6 | 10.3 | 1.1 | 1.6 | N/A |
| Turkey[39] | 200 | Healthy | 32 | 35 | 26 | N/A | N/A | 6 | 1 | N/A | N/A | N/A |
| Turkey[30] | 251 | Migraine patients | 81.9 | N/A | N/A | N/A | N/A | 0.4 | 17.7 | N/A | 0 | N/A |
| Emirates[23] | 50+101 | Healthy + antidepressants | 39.1 | 12.2 | 3.3 | 2.5 | 15.2 | N/A | 9 | N/A | N/A | 4.3 |
| Syria[29] | 51 | Healthy | 47.07 | 30.39 | 2.94 | 0 | N/A | 0 | 9.8 | 0.98 | 0.98 | 3.92 |
| Jordan[28] | 192 | Healthy | 50.6 | N/A | 14.8 | 8.3 | N/A | N/A | 12.8 | N/A | N/A | 13.5 |
*Related to the *3, *4, and *5 together. ALL=Acute lymphoid leukemia; AML=Acute myeloid leukemia; FMF=Familial Mediterranean fever; SLE=Systemic lupus erythematous; N/A=Not applicable
DISTRIBUTION OF THE CYTOCHROME P450 2D6 ALLELIC FREQUENCIES IN THE MIDDLE EAST
In the present study, alleles were assigned according to the nomenclature for human CYP2D6 alleles.[46] The examined alleles were classified according to their function labeled with functional, reduced, nonfunctional, and duplications. The average frequency of the CYP2D6 alleles in each country is shown in Figure 1.
Figure 1.

The allelic frequency of different cytochrome P450 2D6 alleles in the Middle Eastern countries. The frequency of the alleles with <3% accumulated in the other part of each chart. For each allele in each country, the results of studies that examined the relevant allele have been reported in the mean
The two functional frequent alleles, 2D6*1 or *2, were considered in some previous studies if no variants were found.[47] However, now, the *1 and *2 alleles can be distinguished from one another through the examination of the missense mutation of rs1135840 (4180G>C) for *2 assignment, and 2D6*1 could be assigned if no variants encountered. In the Middle Eastern population studied here, the frequency of CYP2D6*2 was evaluated in different studies in Iran, UAE,[23] and Syria[29] with the frequency of 32%, 12.2%, and 30.39%, respectively, and average frequency of 29.7% in three studies in Turkey.[36,39,40] In these studies, apart from the CYP2D6*1 allele, the CYP2D6*2 was the most abundant allele in the population, except for the UAE,[23] in which the frequency of CYP2D6*41 was reported to be more than CYP2D6*2. Furthermore, in the UAE,[23] other normal alleles such as CYP2D6*27, *34, *35, *39, *43, and *46 were also examined with the frequency of 0.7%, 1%, 2%, 4%, 0.3%, and 0.3%, respectively. For all of the populations reviewed here, CYP2D6*1 allele frequency was calculated accordingly as shown in Table 1.
Of the reduced functional alleles, the CYP2D6*41 was presented in Saudi Arabia,[13] UAE,[23] and Turkey[32,36] with the frequency of 18.4%, 15.2%, and 15.1%, respectively. In these populations, the CYP2D6*41 had the highest frequency between the reduced functional alleles. In terms of CYP2D6*10 allele frequency, Iran[24,25] had the highest rate (20.4%), followed by Jordan[28] and Turkey[36,39,40,45] with 14.8% and 13.14% frequency, respectively. Finally, UAE,[23] Saudi Arabia,[14] and Syria[29] with the frequency of 3.3%, 3%, and 2.94%, respectively, ranked the last. The CYP2D6*29 allelic frequency had only been reported in the populations of Saudi Arabia[13] and the UEA,[23] with a frequency of 2.9% and 1.6%, respectively. The CYP2D6*17 allele was absent in the population of Iran[25] and Syria,[29] but this allele was reported with a frequency of 3%, 2.5%, and 0.85% in Saudi Arabia,[14] UAE,[23] and Turkey,[36,40] with the highest frequency being in the Jordan[28] population (8.3%). In addition, the presence of the CYP2D6*9 was reported only in the two Turkish populations[32,40] at a frequency of 2.31%.
Of nonfunctional alleles, a low frequency of CYP2D6*7 was only observed in Turkey,[36,40] CYP2D6*14 in Saudi Arabia,[13] and CYP2D6*3 in Iran[26] and Turkey.[33,34,42,43,44,45] Furthermore, CYP2D6*5 and CYP2D6*6 showed the highest frequency in the Iranian[25] and Turkish[30,36,40,43,45] populations, respectively. The CYP2D6*4 allele had the highest frequency of 28.05% in Egypt[18,19,20,21] and the lowest frequency of 3.5% in Saudi Arabia[14] (3.5%). Between these two intervals, Turkey, Iran, Jordan, Syria, and UAE had the CYP2D6*4 abundance of 15.1%, 14.5%, 12.8%, 9.8%, and 9%, respectively. In Egypt, although some studies[18,19,20,21] showed only the frequency of *4 among nonfunctional alleles, three studies[15,16,17] reported the frequency of *3, *4, and *5 together. We averaged all of them for reporting nonfunctional alleles in the Egyptian population [Figure 1].
Among the countries that gene duplication had been studied, Turkey[40] showed the least frequent and Saudi Arabia[14] indicated the highest.
VARIABILITY OF THE CYTOCHROME P450 2D6 PHENOTYPE FREQUENCIES PREDICTED FROM GENOTYPES IN THE MIDDLE EAST
EM (individuals with at least one functional allele), IM (individuals with a combination of two decreased function variants or a combination of one nonfunctional allele with a functional or reduced function variants), PM (individuals with two nonfunctional variants), and UM (individuals with more than two functional alleles) phenotype frequencies were evaluated in a study by Ingelman-Sundberg et al.[48] Summary of the CYP2D6 phenotype frequencies in each country is shown in Figure 2.
Figure 2.
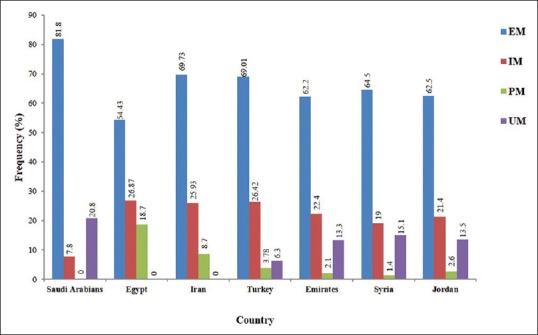
The genotype frequency of cytochrome P450 2D6 in different Middle Eastern countries. EM; IM; PM; and UM; frequencies was presented in the chart for each country, separately. EM = Extensive metabolizer; IM = Intermediate metabolizer; PM = Poor metabolizer; and UM = Ultrarapid metabolizer
Differentiating by ethnic groups, the EM frequency is found to be higher in Saudi Arabia than other countries. It is of note that Egyptian showed the highest PM and IM frequency among Middle East populations. Furthermore, UM frequency varies widely among different populations of the Middle East, with the highest frequency in Saudi Arabians.
DISCUSSION
In a previously reviewed study[49] of the CYP2D6 allele frequencies worldwide, the Middle East was mentioned as a single area, but different countries in the Middle East were not evaluated separately. Interestingly, the result of our study in the Middle East as a whole was different from the previous one in some of CYP2D6 allele frequencies. Two of the most frequent alleles in the present study, CYP2D6*4 and *10, had been reported with less frequency in the previous study. These differences may be because limited parts of the Middle East were evaluated in the previous study, not including all the countries. Other allele frequencies were approximately the same in the two studies.
Frequency of CYP2D6 alleles in various regions of the Middle East is different. These different results are due to the different ethnic groups and different methods used. Of note, most of the articles studied here used polymerase chain reaction (PCR) restriction fragment length polymorphism (PCR-RFLP) method for determining the CYP2D6 alleles, and other methods such as real-time PCR, allele-specific PCR, and sequencing were used less. Hence, ethnic differences seem to be more important in presenting different allelic frequencies than the discrepancy of the methods used.
Here, the comparison of the frequency of different CYP2D6 alleles in the Middle East with Asia, Africa, America, and Europe had been discussed. The incidence of CYP2D6*2 allele in the Middle East appeared to be as frequent as that in Americans (23.48%), Europeans (26.91%), and South/Central Asians (31.90%),[10] whereas lower frequencies of this allele were reported among Africans (17.13%) and Asians (12.82%).[9]
The allelic frequency of CYP2D6*10 in the Middle East was higher than Africans (5.47%), Americans (3.37%), and Europeans (3.16%), but much lower than those reported for Asians (42.31%). Unlike Asia, the prevalence of IM alleles mostly contributed to CYP2D6*41 (15.95%). There were no published studies on the prevalence of this allele in the Iranian ethnic populations. The CYP2D6*41 allele frequency in the Middle East was higher than that found in the Africans (10.18%), Europeans (8.56%), South/Central Asians (10.5%), Americans (5.93%), and Asians (1.97%). In addition, the CYP2D6*17 allele frequency was higher than that reported in the Europeans (0.32%) and South/Central Asians (0.38%), but much lower than Africans (19.1%). Furthermore, the allelic frequency of CYP2D6*9 in our study was comparable with Americans (1.32%) and South/Central Asians (1.4%), but lower than Europeans (2.4%) and higher than Africans (0.3%) and Asians (0.07%).[9]
The allelic frequency of CYP2D6*3 in the Middle East was higher than that reported for Africans (0.17%) and Americans (0.73%), but was comparable with that found in the Europeans (1.2%). The allelic frequency of CYP2D6*4 in our samples was higher than that reported for Africans (4.8%), Asians (0.4%), Americans (11.3%), and South/Central Asians (6.6%), but was lower than those reported for Europeans (18.5%). Few studies had been conducted on the frequency of the CYP2D6*6 allele; nonetheless, the frequencies of this allele in Africans, Americans, Asians, and Europeans were reported to be 0.24%, 0.43%, 0.02% and 0.95%, respectively. The allelic frequency of CYP2D6*5 was comparable to Americans (1.9%), but lower than Africans (6.11%), Asians (5.61%), Europeans (2.69%), and South/Central Asians (2.54%). Our allelic frequency of CYP2D6*5 was higher than that reported in Europeans (0.11%). The *14 allelic frequency in our study was lower than Africans (0.26%), Americans (0.33%), Asians (5.61%), Europeans (2.69%), and South/Central Asians (2.54%).[9]
CONCLUSION
Taken together, our study on the allelic frequency of CYP2D6 in the Middle East demonstrated that allele *4 is the most frequent PM allele in this region as well as other parts of the world. In case of IM alleles, the allele *41 is the most common allele in the populations, of which the *41 allele frequency was evaluated. However, in other populations, like the rest of the world, the most abundant allele is *10. Observing the different allelic frequencies of CYP2D6 gene in this region, these results should be considered in the application of the treatment protocol.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study was financially supported by the Isfahan University of Medical Sciences, Isfahan, Iran (project number: 394446), and also by the Cellular, Molecular and Genetics Research Center, Isfahan University of Medical Sciences, Isfahan, Iran. The results described in this paper were part of the PhD thesis of Z. Kh.
REFERENCES
- 1.Shokri F, Ghaedi H, Ghafouri Fard S, Movafagh A, Abediankenari S, Mahrooz A, et al. Impact of ATM and SLC22A1 polymorphisms on therapeutic response to metformin in Iranian diabetic patients. Int J Mol Cell Med. 2016;5:1–7. [PMC free article] [PubMed] [Google Scholar]
- 2.Meisel C, Roots I, Cascorbi I, Brinkmann U, Brockmöller J. How to manage individualized drug therapy: Application of pharmacogenetic knowledge of drug metabolism and transport. Clin Chem Lab Med. 2000;38:869–76. doi: 10.1515/CCLM.2000.126. [DOI] [PubMed] [Google Scholar]
- 3.Meyer UA. Pharmacogenetics and adverse drug reactions. Lancet. 2000;356:1667–71. doi: 10.1016/S0140-6736(00)03167-6. [DOI] [PubMed] [Google Scholar]
- 4.Ingelman-Sundberg M. Genetic polymorphisms of cytochrome P450 2D6 (CYP2D6): Clinical consequences, evolutionary aspects and functional diversity. Pharmacogenomics J. 2005;5:6–13. doi: 10.1038/sj.tpj.6500285. [DOI] [PubMed] [Google Scholar]
- 5.Zanger UM, Raimundo S, Eichelbaum M. Cytochrome P450 2D6: Overview and update on pharmacology, genetics, biochemistry. Naunyn Schmiedebergs Arch Pharmacol. 2004;369:23–37. doi: 10.1007/s00210-003-0832-2. [DOI] [PubMed] [Google Scholar]
- 6.Gough AC, Smith CA, Howell SM, Wolf CR, Bryant SP, Spurr NK. Localization of the CYP2D gene locus to human chromosome 22q13.1 by polymerase chain reaction, in situ hybridization, and linkage analysis. Genomics. 1993;15:430–2. doi: 10.1006/geno.1993.1082. [DOI] [PubMed] [Google Scholar]
- 7.Eichelbaum M, Ingelman-Sundberg M, Evans WE. Pharmacogenomics and individualized drug therapy. Annu Rev Med. 2006;57:119–37. doi: 10.1146/annurev.med.56.082103.104724. [DOI] [PubMed] [Google Scholar]
- 8.Gardiner SJ, Begg EJ. Pharmacogenetics, drug-metabolizing enzymes, and clinical practice. Pharmacol Rev. 2006;58:521–90. doi: 10.1124/pr.58.3.6. [DOI] [PubMed] [Google Scholar]
- 9.Bradford LD. CYP2D6 allele frequency in European caucasians, Asians, Africans and their descendants. Pharmacogenomics. 2002;3:229–43. doi: 10.1517/14622416.3.2.229. [DOI] [PubMed] [Google Scholar]
- 10.van Schaik RH. Cancer treatment and pharmacogenetics of cytochrome P450 enzymes. Invest New Drugs. 2005;23:513–22. doi: 10.1007/s10637-005-4019-1. [DOI] [PubMed] [Google Scholar]
- 11.Marcucci KA, Pearce RE, Crespi C, Steimel DT, Leeder JS, Gaedigk A. Characterization of cytochrome P450 2D6.1 (CYP2D6.1), CYP2D6.2, and CYP2D6.17 activities toward model CYP2D6 substrates dextromethorphan, bufuralol, and debrisoquine. Drug Metab Dispos. 2002;30:595–601. doi: 10.1124/dmd.30.5.595. [DOI] [PubMed] [Google Scholar]
- 12.Dorne JL, Walton K, Slob W, Renwick AG. Human variability in polymorphic CYP2D6 metabolism: Is the kinetic default uncertainty factor adequate? Food Chem Toxicol. 2002;40:1633–56. doi: 10.1016/s0278-6915(02)00117-5. [DOI] [PubMed] [Google Scholar]
- 13.Al-Dosari MS, Al-Jenoobi FI, Alkharfy KM, Alghamdi AM, Bagulb KM, Parvez MK, et al. High prevalence of CYP2D6 * 41 (G2988A) allele in Saudi Arabians. Environ Toxicol Pharmacol. 2013;36:1063–7. doi: 10.1016/j.etap.2013.09.008. [DOI] [PubMed] [Google Scholar]
- 14.McLellan RA, Oscarson M, Seidegård J, Evans DA, Ingelman-Sundberg M. Frequent occurrence of CYP2D6 gene duplication in Saudi Arabians. Pharmacogenetics. 1997;7:187–91. doi: 10.1097/00008571-199706000-00003. [DOI] [PubMed] [Google Scholar]
- 15.Anwar WA, Abdel-Rahman SZ, El-Zein RA, Mostafa HM, Au WW. Genetic polymorphism of GSTM1, CYP2E1 and CYP2D6 in Egyptian bladder cancer patients. Carcinogenesis. 1996;17:1923–9. doi: 10.1093/carcin/17.9.1923. [DOI] [PubMed] [Google Scholar]
- 16.Abdel-Rahman SZ, Anwar WA, Abdel-Aal WE, Ghoneim MA, Au WW. The CYP2D6 extensive metabolizer genotype is associated with increased risk for bladder cancer. Cancer Lett. 1997;119:115–22. doi: 10.1016/s0304-3835(97)00265-6. [DOI] [PubMed] [Google Scholar]
- 17.Ali AA, Wassim NM, Dowaidar MM, Yaseen AE. Genetic polymorphism of CYP2D6 gene among Egyptian hypertensive cases. J Basic Appl Zool. 2013;66:228–33. [Google Scholar]
- 18.Eyada TK, El Ghonemy EG, El Ghoroury EA, El Bassyouni SO, El Masry MK. Study of genetic polymorphism of xenobiotic enzymes in acute leukemia. Blood Coagul Fibrinolysis. 2007;18:489–95. doi: 10.1097/MBC.0b013e3281eec930. [DOI] [PubMed] [Google Scholar]
- 19.Zayed AA, Ahmed AI, Khattab AM, Mekdad AA, AbdelAal AG. Paraoxonase 1 and cytochrome P450 polymorphisms in susceptibility to acute organophosphorus poisoning in Egyptians. Neurotoxicology. 2015;51:20–6. doi: 10.1016/j.neuro.2015.08.011. [DOI] [PubMed] [Google Scholar]
- 20.Zalata A, El-Samanoudy AZ, Osman G, Elhanbly S, Nada HA, Mostafa T. Cytochrome P450-2D6 * 4 polymorphism seminal relationship in infertile men. Andrologia. 2015;47:525–30. doi: 10.1111/and.12298. [DOI] [PubMed] [Google Scholar]
- 21.Tawfik Khattab AM, Zayed AA, Ahmed AI, AbdelAal AG, Mekdad AA. The role of PON1 and CYP2D6 genes in susceptibility to organophosphorus chronic intoxication in Egyptian patients. Neurotoxicology. 2016;53:102–7. doi: 10.1016/j.neuro.2015.12.015. [DOI] [PubMed] [Google Scholar]
- 22.Scantamburlo G, Tziolia K, Zopf M, Bernardinelli E, Soyal SM, Civello DA, et al. Allele drop out conferred by a frequent CYP2D6 genetic variation for commonly used CYP2D6 * 3 genotyping assays. Cell Physiol Biochem. 2017;43:2297–309. doi: 10.1159/000484380. [DOI] [PubMed] [Google Scholar]
- 23.Qumsieh RY, Ali BR, Abdulrazzaq YM, Osman O, Akawi NA, Bastaki SM. Identification of new alleles and the determination of alleles and genotypes frequencies at the CYP2D6 gene in Emiratis. PLoS One. 2011;6:e28943. doi: 10.1371/journal.pone.0028943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bagheri A, Kamalidehghan B, Haghshenas M, Azadfar P, Akbari L, Sangtarash MH, et al. Prevalence of the CYP2D6*10 (C100T), *4 (G1846A), and *14 (G1758A) alleles among Iranians of different ethnicities. Drug Des Devel Ther. 2015;9:2627–34. doi: 10.2147/DDDT.S79709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kouhi H, Hamzeiy H, Barar J, Asadi M, Omidi Y. Frequency of five important CYP2D6 alleles within an Iranian population (Eastern Azerbaijan) Genet Test Mol Biomarkers. 2009;13:665–70. doi: 10.1089/gtmb.2009.0009. [DOI] [PubMed] [Google Scholar]
- 26.Hashemi-Soteh SM, Sarzare F, Merat F, Salehifar E, Shiran MR. Frequencies of three CYP2D6 nonfunctional alleles (CYP2D6 * 3, *4, and *6) within an Iranian population (Mazandaran) Genet Test Mol Biomarkers. 2011;15:821–5. doi: 10.1089/gtmb.2011.0033. [DOI] [PubMed] [Google Scholar]
- 27.Yazdi MF, Rafieian S, Gholi-Nataj M, Sheikhha MH, Nazari T, Neamatzadeh H. CYP2D6 genotype and risk of recurrence in tamoxifen treated breast cancer patients. Asian Pac J Cancer Prev. 2015;16:6783–7. doi: 10.7314/apjcp.2015.16.15.6783. [DOI] [PubMed] [Google Scholar]
- 28.Zihlif M, Imraish A, Irshaid YM. Frequency of certain single-nucleotide polymorphisms and duplication of CYP2D6 in the Jordanian population. Genet Test Mol Biomarkers. 2012;16:1201–5. doi: 10.1089/gtmb.2012.0122. [DOI] [PubMed] [Google Scholar]
- 29.Fuselli S, Dupanloup I, Frigato E, Cruciani F, Scozzari R, Moral P, et al. Molecular diversity at the CYP2D6 locus in the Mediterranean region. Eur J Hum Genet. 2004;12:916–24. doi: 10.1038/sj.ejhg.5201243. [DOI] [PubMed] [Google Scholar]
- 30.Atasayar G, Eryilmaz IE, Karli N, Egeli U, Zarifoglu M, Cecener G, et al. Association of MDR1, CYP2D6, and CYP2C19 gene polymorphisms with prophylactic migraine treatment response. J Neurol Sci. 2016;366:149–54. doi: 10.1016/j.jns.2016.05.019. [DOI] [PubMed] [Google Scholar]
- 31.Altayli E, Gunes S, Yilmaz AF, Goktas S, Bek Y. CYP1A2, CYP2D6, GSTM1, GSTP1, and GSTT1 gene polymorphisms in patients with bladder cancer in a Turkish population. Int Urol Nephrol. 2009;41:259–66. doi: 10.1007/s11255-008-9444-6. [DOI] [PubMed] [Google Scholar]
- 32.Arici M, Özhan G. CYP2C9, CYPC19 and CYP2D6 gene profiles and gene susceptibility to drug response and toxicity in Turkish population. Saudi Pharm J. 2017;25:376–80. doi: 10.1016/j.jsps.2016.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Aydin M, Hatirnaz O, Erensoy N, Ozbek U. CYP2D6 and CYP1A1 mutations in the Turkish population. Cell Biochem Funct. 2005;23:133–5. doi: 10.1002/cbf.1222. [DOI] [PubMed] [Google Scholar]
- 34.Kortunay S, Bozkurt A, Bathum L, Basci NE, Calgüneri M, Brøsen K, et al. CYP2D6 polymorphism in systemic lupus erythematosus patients. Eur J Clin Pharmacol. 1999;55:21–5. doi: 10.1007/s002280050587. [DOI] [PubMed] [Google Scholar]
- 35.Sahin S, Aydogan L, Benli I, Ozyurt H. Distribution of HLA-B27 and CYP2D6*4 mutations in the middle black sea area (Tokat) of Turkey. Genet Mol Res. 2011;10:3987–91. doi: 10.4238/2011.December.2.3. [DOI] [PubMed] [Google Scholar]
- 36.Günaldı M, Erkisi M, Afşar CU, Erçolak V, Paydas S, Kara IO, et al. Evaluation of endometrial thickness and bone mineral density based on CYP2D6 polymorphisms in Turkish breast cancer patients receiving tamoxifen treatment. Pharmacology. 2014;94:183–9. doi: 10.1159/000363304. [DOI] [PubMed] [Google Scholar]
- 37.Koseler A, Ilcol YO, Ulus IH. Frequency of mutated allele CYP2D6 * 4 in the Turkish population. Pharmacology. 2007;79:203–6. doi: 10.1159/000100959. [DOI] [PubMed] [Google Scholar]
- 38.Erden G, Acar FS, Inal EE, Soydas AO, Ozoran K, Bodur H, et al. Frequency of mutated allele CYP2D6*4 in the Turkish ankylosing spondylitis patients and healthy controls. Rheumatol Int. 2009;29:1431–4. doi: 10.1007/s00296-009-0874-y. [DOI] [PubMed] [Google Scholar]
- 39.Taskin B, Percin FE, Ergun MA. Investigation of CYP2D6 gene polymorphisms in Turkish population. Psychopharmacol Bull. 2016;46:67–72. doi: 10.64719/pb.4343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Aynacioglu AS, Sachse C, Bozkurt A, Kortunay S, Nacak M, Schröder T, et al. Low frequency of defective alleles of cytochrome P450 enzymes 2C19 and 2D6 in the Turkish population. Clin Pharmacol Ther. 1999;66:185–92. doi: 10.1053/cp.1999.v66.100072001. [DOI] [PubMed] [Google Scholar]
- 41.Inanır A, Yigit S, Sarıyıldız MA, Sogut E. Outcomes of Turkish ankylosing spondylitis patients. Eur J Gen Med. 2013;10:145–9. [Google Scholar]
- 42.Aydin-Sayitoglu M, Hatirnaz O, Erensoy N, Ozbek U. Role of CYP2D6, CYP1A1, CYP2E1, GSTT1, and GSTM1 genes in the susceptibility to acute leukemias. Am J Hematol. 2006;81:162–70. doi: 10.1002/ajh.20434. [DOI] [PubMed] [Google Scholar]
- 43.Yalcıntepe S, Ozdemır O, Sılan C, Ozen F, Uludag A, Candan F, et al. The CYP4502D6*4 and *6 alleles are the molecular genetic markers for drug response: Implications in colchicine non-responder FMF patients. Eur J Drug Metab Pharmacokinet. 2016;41:281–6. doi: 10.1007/s13318-015-0255-8. [DOI] [PubMed] [Google Scholar]
- 44.Seven M, Batar B, Unal S, Yesil G, Yuksel A, Guven M. The effect of genetic polymorphisms of cytochrome P450 CYP2C9, CYP2C19, and CYP2D6 on drug-resistant epilepsy in Turkish children. Mol Diagn Ther. 2014;18:229–36. doi: 10.1007/s40291-013-0078-8. [DOI] [PubMed] [Google Scholar]
- 45.Serin A, Canan H, Alper B, Gulmen M. The frequencies of mutated alleles of CYP2D6 gene in a Turkish population. Forensic Sci Int. 2012;222:332–4. doi: 10.1016/j.forsciint.2012.07.012. [DOI] [PubMed] [Google Scholar]
- 46.Gjerde J, Hauglid M, Breilid H, Lundgren S, Varhaug JE, Kisanga ER, et al. Effects of CYP2D6 and SULT1A1 genotypes including SULT1A1 gene copy number on tamoxifen metabolism. Ann Oncol. 2008;19:56–61. doi: 10.1093/annonc/mdm434. [DOI] [PubMed] [Google Scholar]
- 47.Gaedigk A, Gotschall RR, Forbes NS, Simon SD, Kearns GL, Leeder JS. Optimization of cytochrome P4502D6 (CYP2D6) phenotype assignment using a genotyping algorithm based on allele frequency data. Pharmacogenetics. 1999;9:669–82. doi: 10.1097/01213011-199912000-00002. [DOI] [PubMed] [Google Scholar]
- 48.Ingelman-Sundberg M, Oscarson M, McLellan RA. Polymorphic human cytochrome P450 enzymes: An opportunity for individualized drug treatment. Trends Pharmacol Sci. 1999;20:342–9. doi: 10.1016/s0165-6147(99)01363-2. [DOI] [PubMed] [Google Scholar]
- 49.Sistonen J, Fuselli S, Palo JU, Chauhan N, Padh H, Sajantila A. Pharmacogenetic variation at CYP2C9, CYP2C19, and CYP2D6 at global and microgeographic scales. Pharmacogenet Genomics. 2009;19:170–9. doi: 10.1097/FPC.0b013e32831ebb30. [DOI] [PubMed] [Google Scholar]