

Abstract
Background:
The use of non-scalp donor hair is considered in situations of a relative or absolute lack of head donor hair supply. Till now, very few published works are present on body hair transplant. None of them have compared scalp and non-scalp hair in terms of survival as well as characteristics.
Objective:
To compare the characteristics such as rate of anagen effluvium and survival rates of scalp, beard, and chest hair in hair restoration procedure of scalp.
Materials and Methods:
Three blocks of 1cm2 were marked on a non-frontal area. Thirty slits with a 0.9mm blade were made in each block. Single follicular unit was taken from scalp, beard, and chest area and was implanted simultaneously in each block, respectively. The areas were evaluated for any graft loss, anagen effluvium, and survival rate.
Results:
During initial period of 2 months, anagen effluvium in scalp (40%) and beard (30%) were significantly less than body (53.3%) hair with excellent survival rate of beard (95%), followed by scalp (89%) and then followed by chest hair (76%) at 1 year.
Conclusion:
Non-scalp hair can become an excellent source of donor area for hair restoration procedure.
Keywords: Anagen effluvium, body hair transplant, hair restoration procedure
Introduction
The goal of every hair transplant surgery should be regrowth of all transplanted hair follicles with natural distribution and without any alteration of scalp surface, leading to patient satisfaction. It is not possible to attain these goals in each and every surgery. There will be candidates who will have scarcity of donor area as compared to requirement in recipient site. Also, there can be need of follicles with different characteristics (finer, shorter hair) to restore different recipient sites. With the advent of follicular unit extraction (FUE), it has become possible to extract follicles effectively not only from scalp but from different body parts too without visible scarring.
The proposed indications for use of non-scalp hair are as follows:
Resource versus recipient mismatch [Figure 1]: This type of mismatch can be because of low-donor reserve (such as low-donor density, narrow-donor fringe, retrograde alopecia, previous surgical or traumatic scarring, miniaturization in superior fringe region, diffuse thinning, and fine and straight hair) or high-recipient requirement (such as big skull size, family history of advanced androgenetic alopecia, young age of onset, rapid progression of baldness, low-residual hairline, and high hair–scalp color contrast), which is very common in Asian patients.[1]
Hairline recreation preferably for the vanguard hair at hairline where only fine one hair follicular unit (FU) is required for adding softer appearance, especially in Asian patients, where there is high contrast between skin and hair color, and putting scalp hair in hairline, which is too dark in Asians can create unnatural look.[2,3,4] Beard hair is never preferred in hairline but other body hair gives excellent aesthetic appearance.
Scar reconstruction such as repair of donor strip scar in case of poor donor reserve.
Facial and body hair restoration such as temple or eyebrow recreation where hair thickness, growth rate, and length desired are optimal for body but not for scalp hair.
Figure 1.

Low-donor reserve (A) versus high-recipient requirement (B)
Most of the surgeons do not prefer non-scalp donor hair because of variable reasons. No ideal method is established to score and extract non-scalp hair. Body hair can spread over 1.5–2mm, requiring the need for larger extraction punches. Transection rates are considered higher in body areas, that is, up to 30% as compared to scalp hair, which is less than 5%.[2,5] The survival rate is unknown as only subjective studies are available, and hence unpredictable.[2,3,4,5] Chest hair grows shorter and beard hair is too curly, leading to difficulty in styling. The extraction process takes longer procedural hours and requires high surgical skill. The use of body hair becomes restricted in non-hairy individuals. It is unclear and yet to be studied on how different characters such as density, thickness, growth rate, anagen/telogen ratio, amount of tethering, and level of arrector pili affect the overall survival of follicles.[6]
Hair transplantation is based on the phenomenon of “donor dominance,” meaning that autografts maintain their integrity and characteristics after transplantation to a new site. However, because of the influence of recipient area’s cutaneous structures, it is now postulated that the survival rate, growth rate, and cycles of the transplanted hairs can be affected known as recipient codominance.[7] The phenomenon of recipient codominance is still unclear, making body hair not a preferred choice in hair restoration procedures (HRPs).
This study was conducted with the aim of comparing the survival rates of scalp, beard, and chest hair in HRP of scalp. Beard and chest have been the most frequent areas to be used as non-scalp donor hair in HRPs in previous studies, and therefore were opted for the study.[2,3,4,5,6]
Materials and Methods
An interventional study was carried out on five patients requiring HRP. Standard pre-op evaluation was carried out. Patients with grade 6–7 (Hamilton–Norwood scale of male pattern baldness) were selected where two sessions were planned to be performed at a gap of 1 year. Three blocks of 1cm2 were marked on a mid-frontal area [Figure 2]. Thirty slits were made with a 0.9-mm blade in each block, that is, 30 slit/cm2 at a depth of approximately 3–4mm depending on the length of the graft in brick/staggered pattern [Figure 3].[8] Only one hair FU was extracted from the scalp, beard, and chest area using sharp punch.[9] Each FU was a medium-sized FU (0.8–1mm). Simultaneous implantation with forceps was carried out using “no touch to root” technique [Figure 4].[10] Patients were instructed to spray normal saline every 2h for initial 7 days. The areas were evaluated at day 2, 7, and 14 for any graft loss; week 8 for anagen effluvium; and month 3, 6, and 12 for survival rate.
Figure 2.

Marked blocks as scalp, beard, and chest (left to right) on mid-frontal area
Figure 3.

Thirty slits in 1cm2 of size 0.9mm in brick pattern
Figure 4.

Grafts after implantation as scalp, beard, and chest (left to right)
Statistical Analysis
Qualitative variables were compared using chi-square test/Fisher’s exact test. A P value of <0.05 was considered statistically significant. The data was analysed using Statistical Package for Social Sciences version (SPSS) 21.0 (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY).
Results
Of the five patients taken up for study, two had grade 6 baldness and three had grade 7 baldness. Thirty hairs of scalp, beard, and chest each, were implanted in a single patient, amounting to 150 hairs of scalp, beard, and chest each, in five patients. No graft loss was seen at the end of day 2, 7, and 14 [Figure 5]. However, beard hair did outgrow as compared to scalp and chest hair. At the end of 2 months, the mean survival rate was 60%, 70%, and 46.7% for scalp, beard, and chest hair, respectively [Figure 6], which means the rate of anagen effluvium at 2 months was 40%, 30%, and 53.7% for scalp, beard, and chest, respectively. Figure 7 shows the survival of different sites of all patients at the end of 2 months. The mean survival rate at 3 and 6 months [Figures 8 and 9] for scalp, beard, and chest was 62%, 73.3%, and 57.3% and 80%, 86.6%, and 67.3%, respectively. Final evaluation was carried out at the end of 1 year. Figure 10 shows the mean and individual patients’ graft survival rate % at the end of one year. The comparison of survival rate of scalp, beard, and chest hair is shown in Table 1.
Figure 5.
No graft loss at 2 weeks, note the beard hair outgrowth (scalp, beard, and chest: left to right)
Figure 6.

Graft survival at 2 months (scalp, beard, and chest: left to right)
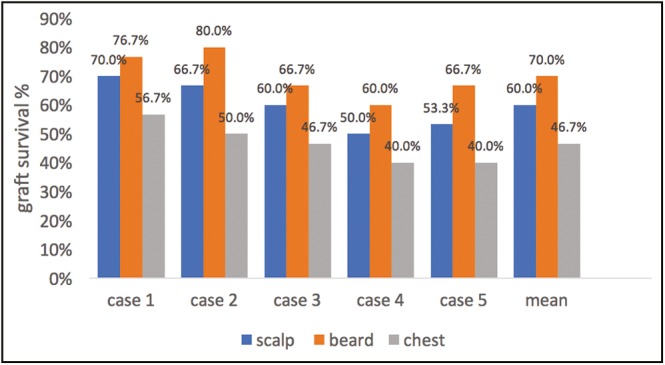
Figure 7.
Graph showing graft survival after 2 months, subject wise
Figure 8.

Immediately after implantation (A), after 2 weeks of transplant (B), after 3 months of transplant (C) (scalp, beard, and chest: left to right)
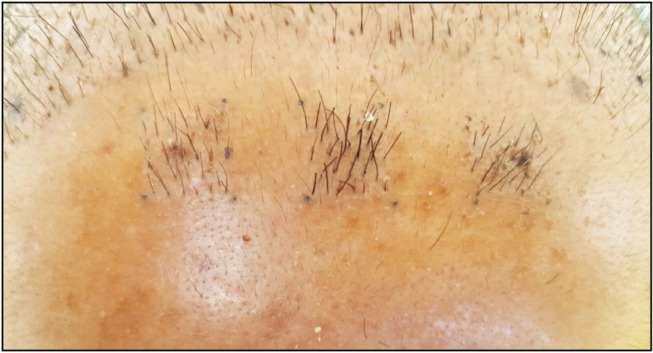
Figure 9.

Immediately after implantation (A), after 3 months of transplant (B), after 6 months of transplant (C) with marker pen to demarcate the areas (scalp, beard, and chest: left to right)
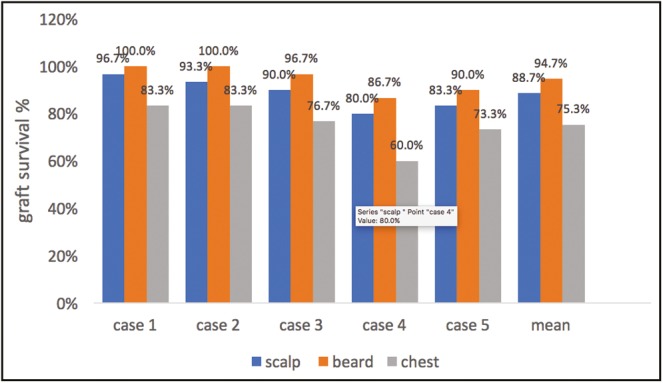
Figure 10.
Graph showing graft survival after 1 year, subject wise
Table 1.
Comparison of mean survival rates, n (%)
| Time period | Scalp | Beard | Chest | P value |
|---|---|---|---|---|
| 2 months | 90 (60.00%) | 105 (70.00%) | 70 (46.70%) | 0.0002* |
| 3 months | 93 (62.00%) | 110 (73.30%) | 86 (57.30%) | 0.012* |
| 6 months | 120 (80.00%) | 130 (86.60%) | 101 (67.30%) | 0.0002* |
| 1 year | 133 (88.70%) | 142 (94.70%) | 113 (75.30%) | <0.0001* |
*P < 0.05: significant difference in the mean survival rates of scalp, beard and chest hair
Four of five patients had hypopigmented spots at the donor area. One of the patients had hyperpigmented spots and folliculitis, which was treated with topical antibiotic in 2 weeks. All complications were mild and were not given any treatment as they were not a major concern to any of the patients.
Discussion
With the advent of FUE, it has become possible to expand the donor area beyond the scalp. It is now possible to give full and better coverage in a bald area with different types and characteristics of hair, which can be chosen according to the need of recipient area. However, one of the major limiting factor for opting body hair as donor area is its inability to predict the survival rate. Very few published data regarding the survival rate of body hair are available.
Single patient case reports with satisfactory coverage with body hair have been reported by many authors. However, none of them have mentioned about the rate of survival.[6,11] A retrospective study conducted by Umar[2] on 122 patients showed that they were generally very satisfied with the results of their procedure, giving mean scores of at least a 7.8 on a Likert-like scale of 0–10 for their healing status, hair growth in recipient areas, and overall satisfaction with their surgeries. Patients who had only body hair and no head or beard hair taken had marginally lower score (6.9), but they were equally satisfied as their other counterparts.[2]
Few studies have objectively measured the survival rate. Umar S[4,12] reported overall graft survival of 95% for scalp and 75–8% for body hair. We almost found the same survival rate of 75% in chest hair and exceptionally higher survival rates in beard hair (94%). A case reported on single patient comparing different areas of body showed mean survival of 53%.[5] The individual survival rates were 60.4%, 39%, 39.2%, 51.6%, and 29% for chest, abdomen, arms, thighs, and back, respectively. We selected chest for body hair as it has got best density, least transection, and highest yield. Our survival rate for chest was better than this case report (76% vs. 60%). However, one of our patients also had the same survival rate (Case 4), showing the need for increasing the sample size to predict the right survival rates. Also, more studies are required to compare different body areas on a bigger sample size as different areas behave differently in terms of survival.
Apart from different types of body hair, many factors, which can affect the final survival of grafts and studies, are still lacking. What is the ideal density (15–60/cm2) for implantation is still unknown. It is also postulated that the dermal papilla is attenuated during telogen and is more prone to damage during individual follicular extraction. Therefore, some prefer to extract only active anagen phase in body hair as a high percentage (40%–70%) of the body hair is in resting telogen phase at any particular time. Therefore, preshaving protocol has been advised by few authors for body hair.[13] However, we did not carry out any anagen selection and we hope for further studies to notify any practical difference between anagen and telogen growth.
It was noted that the rate of effluvium, that is, the amount of graft loss in the initial period of 2 months can predict the rate of survival too. It was noted that effluvium, that is, at 2 months was the lowest for beard, followed by scalp and then by chest follicles, whereas survival rate was the highest for beard, followed by scalp and then by chest follicles. The better growth of beard hair can be explained by the increased thickness of beard hair, faster growth rate of beard hair, and easily extractable characteristics because of shallow depth of scoring (1–2mm) as compared to scalp hair, which has 3–4mm depth of scoring.
An observational study carried out on 35 subjects showed that the body and beard donor hair are not going to change their characteristic curl, color, and caliber after transplant to the scalp and due care is needed to use a mix of the various donor hair in any bald area of the scalp.[14] This study do not corroborate with the theory of recipient codominance. In our study also, it was easy to distinguish between scalp, beard, and chest hair because of different types of curl and thickness. Beard hair still looks curly with robust growth and chest hair was still short and thin. However, no objective scales were used in our study. It is required to have more studies and longer follow-up time to have clarity about recipient codominance.
Most of the patients had hypopigmented spots at the area of extraction but it was too insignificant to be pointed out by patients and required no treatment. No cases of keloid or hypertrophic scars were reported and all patients were satisfied with final healing of donor area.
To the best of our knowledge, this is the only study till date, which has eliminated inter-patient or inter-operator variation by comparing all three types of hair on same subjects. However, sample size is too small, but it is difficult to convince patients to participate and follow up for these many times till 1 year. Most of the studies conducted earlier are either survey based, retrospective, or on single patient only. This is the first prospective study with these many subjects, and this will definitely encourage other hair restoration surgeons to start performing more work with body hair.
Conclusion
Body hair can become an excellent source of donor area for HRP. Body hair transplant requires longer procedural time and needs high surgical skill, which takes years to achieve. The results achieved can be tremendous but may not satisfy every patient because of different characteristics of hair implanted, and therefore, proper counseling is needed.
Financial support and sponsorship
This study was funded by International Society of Hair Restoration Surgery (ISHRS) under research grant 2015.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Konior RJ, Simmons C. Patient selection, candidacy, and treatment planning for hair restoration surgery. Facial Plast Surg Clin North Am. 2013;21:343–50. doi: 10.1016/j.fsc.2013.04.004. [DOI] [PubMed] [Google Scholar]
- 2.Umar S. Body hair transplant by follicular unit extraction: my experience with 122 patients. Aesthet Surg J. 2016;36:1101–10. doi: 10.1093/asj/sjw089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Umar S. Use of body hair and beard hair in hair restoration. Facial Plast Surg Clin North Am. 2013;21:469–77. doi: 10.1016/j.fsc.2013.05.003. [DOI] [PubMed] [Google Scholar]
- 4.Umar S. The transplanted hairline: leg room for improvement. Arch Dermatol. 2012;148:239–42. doi: 10.1001/archdermatol.2011.2196. [DOI] [PubMed] [Google Scholar]
- 5.Mysore V. Body hair transplantation: case report of successful outcome. J Cutan Aesthet Surg. 2013;6:113–6. doi: 10.4103/0974-2077.112676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jones R. Body hair transplant into wide donor scar. Dermatol Surg. 2008;34:857. doi: 10.1111/j.1524-4725.2008.34163.x. [DOI] [PubMed] [Google Scholar]
- 7.Hwang S, Kim JC, Ryu HS, Cha YC, Lee SJ, Na GY, et al. Does the recipient site influence the hair growth characteristics in hair transplantation? Dermatol Surg. 2002;28:795–8. doi: 10.1046/j.1524-4725.2002.02041.x. discussion 798-9. [DOI] [PubMed] [Google Scholar]
- 8.Farjo B, Farjo N. Dense packing: surgical indications and technical considerations. Facial Plast Surg Clin North Am. 2013;21:431–6. doi: 10.1016/j.fsc.2013.06.004. [DOI] [PubMed] [Google Scholar]
- 9.Cole JP. An analysis of follicular punches, mechanics, and dynamics in follicular unit extraction. Facial Plast Surg Clin North Am. 2013;21:437–47. doi: 10.1016/j.fsc.2013.05.009. [DOI] [PubMed] [Google Scholar]
- 10.Sethi P, Bansal A. Direct hair transplantation: a modified follicular unit extraction technique. J Cutan Aesthet Surg. 2013;6:100–5. doi: 10.4103/0974-2077.112672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Poswal A. Body hair transplant: an additional source of donor hair in hair restoration surgery. Ind J Dermatol. 2007;52:104–5. [Google Scholar]
- 12.Umar S. Hair transplantation in patients with inadequate head donor supply using nonhead hair: report of 3 cases. Ann Plast Surg. 2011;67:332–5. doi: 10.1097/SAP.0b013e318209a61a. [DOI] [PubMed] [Google Scholar]
- 13.Poswal A. The preshaving protocol in body hair-to-scalp transplant to identify hair in anagen phase. Indian J Dermatol. 2010;55: 50–2. doi: 10.4103/0019-5154.60353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Poswal A. Use of body and beard donor hair in surgical treatment of androgenic alopecia. Indian J Plast Surg. 2013;46:117–20. doi: 10.4103/0970-0358.113728. [DOI] [PMC free article] [PubMed] [Google Scholar]