

Abstract
Objective: This study is the first in a series of four empirical investigations to develop International Classification of Functioning, Disability and Health (ICF) Core Sets for Autism Spectrum Disorder (ASD). The objective was to use a systematic review approach to identify, number, and link functional ability and disability concepts used in the scientific ASD literature to the nomenclature of the ICF‐CY (Children and Youth version of the ICF, covering the life span). Methods: Systematic searches on outcome studies of ASD were carried out in Medline/PubMed, PsycINFO, ERIC and Cinahl, and relevant functional ability and disability concepts extracted from the included studies. These concepts were then linked to the ICF‐CY by two independent researchers using a standardized linking procedure. New concepts were extracted from the studies until saturation of identified ICF‐CY categories was reached. Results: Seventy‐one studies were included in the final analysis and 2475 meaningful concepts contained in these studies were linked to 146 ICF‐CY categories. Of these, 99 categories were considered most relevant to ASD (i.e., identified in at least 5% of the studies), of which 63 were related to Activities and Participation, 28 were related to Body functions, and 8 were related to Environmental factors. The five most frequently identified categories were basic interpersonal interactions (51%), emotional functions (49%), complex interpersonal interactions (48%), attention functions (44%), and mental functions of language (44%). Conclusion: The broad variety of ICF‐CY categories identified in this study reflects the heterogeneity of functional differences found in ASD—both with respect to disability and exceptionality—and underlines the potential value of the ICF‐CY as a framework to capture an individual's functioning in all dimensions of life. The current results in combination with three additional preparatory studies (expert survey, focus groups, and clinical study) will provide the scientific basis for defining the ICF Core Sets for ASD for multipurpose use in basic and applied research and every day clinical practice of ASD. Autism Res 2015, 8: 782–794. © 2015 The Authors Autism Research published by Wiley Periodicals, Inc. on behalf of International Society for Autism Research
Keywords: neurodevelopmental disorder, assessment, child psychiatry, diagnostics, International Classification of Diseases, Diagnostic and Statistical Manual of Mental Disorders, autism
Background
The Diagnostic and Statistical Manual of Mental Disorders [5th ed.; American Psychiatric Association, 2013] stresses the importance of functional disabilities to the understanding and definition of mental disorders in general (p. 20), as well as specifically for certain diagnoses (e.g., neurodevelopmental disorders, pp. 31–86). For a diagnosis of Autism Spectrum Disorder (ASD), apart from qualitative alterations in social communication and interaction (criterion A) in addition to stereotyped, repetitive, restricted behavior patterns (criterion B), that present in the early developmental period (criterion C), it is also required that these “symptoms cause clinically significant impairment in social, occupational and other important areas of current functioning” (p. 50, criterion D), and that they are not better explained otherwise (criterion E). Indeed, ASD research has shown that, irrespective of cognitive level, outcome is often poor in terms of employment, establishment and maintenance of social relationships, physical and mental health, and quality of life [Howlin & Moss, 2012]. However, there is also evidence that ASD is not exclusively characterized by deficits but also certain strengths [Happé & Frith, 2009; Mottron, Dawson, & Soulières, 2009] which may have a positive impact on an individual's overall functioning and satisfaction with life. To date, there is no comprehensive tailored system to classify disability and ability in mental health or in ASD. However, the International Classification of Functioning, Disability and Health (ICF) provides a feasible framework for this purpose.
The ICF, which was developed by the World Health Organization [WHO, 2001] is rooted in the interactive biopsychosocial model of functioning, and provides detailed classifications of ability and disability in the areas of Body functions (i.e., physiological functions of body systems), Body structures (i.e., anatomical parts of the body), Activities (i.e., execution of tasks), Participation (i.e., involvement in life situations), and Environmental factors (i.e., physical, social, and attitudinal environment). Personal factors are also included in the biopsychosocial model but are not yet classified in the ICF given the large social and cultural variance associated with them [WHO, 2001]. There is ongoing debate about the definition of Personal factors and which factors should be included in such a category [Müller and Geyh, 2015; Simeonsson et al., 2014]. Commonly addressed Personal factors are sociodemography, lifestyle, and coping strategies. ICF's descriptions of functional categories allow for a common language which can be applied by professionals from various disciplines, researchers, clinicians, teachers, and health care authorities, to facilitate effective communication in the context of assessment, treatment and health policy issues.
Derived from the ICF (for adults) in 2007, the ICF Children and Youth version (ICF‐CY) was designed to capture functional abilities and disabilities in developing individuals, by adding and expanding on the descriptions of existing ICF categories [WHO, 2007]. Field trials have demonstrated the utility of the ICF‐CY for tailored intervention planning in children with several specific developmental disabilities (i.e., cerebral palsy, autism, language and speech disorders), as well as its acceptability among health care professionals [Ibragimova, Granlund, & Björck‐Åkesson, 2009]. Studies using the ICF‐CY in ASD have demonstrated that ASD experts consider ICF‐CY categories from all areas of the biopsychosocial model as relevant in the assessment‐intervention process with young children with ASD [Castro & Pinto, 2013], and that there are strong associations between ICF‐CY findings, and data from diagnostic instruments for ASD (i.e., Autism Diagnostic Observation Scale [ADOS], Autism Diagnostic Interview –Revised [ADI‐R], Childhood Autism Rating Scale [CARS]) [Castro, Ferreira, Dababnah, & Pinto, 2013]. In addition, an ICF‐CY derived parent‐report questionnaire for the assessment of the functional profile of preschool children with ASD has been developed and validated [Gan, Tung, Yeh, & Wang, 2013].
The ICF and ICF‐CY provide methods for classifying functioning within four key components of the biopsychosocial model, that is, Body functions, Body structures, Activities and Participation, and Environmental factors. For each of these components, aspects of functioning are described in hierarchically structured categories with up to four levels of increasing detail. At the first level are chapters, which provide a general overview of the areas of functioning that are covered by the ICF and ICF‐CY. The chapters consist of second, third, and fourth level categories, as can be seen in the following example of an ASD‐relevant classification from the Activities and Participation component:
Level 1 chapter: d7 Interpersonal interactions and relationships
Level 2 category: d710 Basic interpersonal interactions
Level 3 category: d7104 Social cues in relationships
Level 4 category: d71040 Initiating social interactions
Both the ICF and the ICF‐CY (referred to as “ICF(‐CY)” from now on) contain over 1400 categories that together provide an exhaustive classification of an individual's functioning. Nevertheless, given its comprehensiveness, the ICF(‐CY) in its current complete form is rather impractical for daily clinical use or research purposes. For instance, many categories are irrelevant if applied to any particular health condition. To address this issue, the development of ICF Core Sets was initiated; that is, the selection of ICF(‐CY) categories that are considered most relevant to individuals with a particular health condition [Selb et al., 2015; Stucki & Grimby, 2004; Üstün, Chatterji, & Kostanjsek, 2004]. The development of Core Sets uses a rigorous and systematic scientific approach that comprises a systematic literature review (current study; research perspective), an expert survey (expert perspective), focus groups (clients and social environment perspective), and clinical investigation (clinical perspective). These include a wide range of professions and other stakeholders across all of the WHO regions. The present study is therefore part of a larger project, aiming to develop standardized ICF Core Sets for ASD. To develop a tool that covers functional abilities and disabilities over the whole life span of ASD, ICF Core Sets are designed to be equally applicable to children, adolescents, and adults. The development is based on the ICF‐CY, which includes all “adult” ICF categories as well as extended categories to capture functioning across childhood and youth. A complete description of the overall ASD ICF Core Set development process has been published in a previous issue of this journal [Bölte et al., 2013].
This systematic review is the first empirical work of four comprehensive preparatory studies which will form the scientific basis of the ICF Core Sets development project. Its objective was to identify ICF‐CY categories particularly relevant for ASD using the data from the published scientific literature. The study followed a methodology that has been successfully developed and implemented for other health conditions (e.g., spinal cord injury [Kirchberger et al., 2010; Cieza et al., 2010]; depression [Cieza et al., 2004]; diabetes mellitus [Ruof et al., 2004]; hearing loss [Danermark, Granberg, Kramer, Selb, & Möller, 2013]) by the ICF Research Branch in cooperation with the WHO Collaborating Centre for the Family of International Classifications in Germany (at DIMDI – German Institute of Medical Documentation and Information), in collaboration with the WHO [Selb et al., 2015].Together with the other three preparatory studies, this review will provide content for an international ICF Core Sets Consensus Conference, during which a group of experts from all WHO regions will follow a formal decision‐making process to arrive at a consensus on the ICF‐CY categories to be included in the ICF Core Sets for ASD.
Methods
Design
A systematic literature review was conducted following the principles outlined by the WHO and ICF Research Branch [Selb et al., 2015]. These principles have previously been applied in the development of ICF Core Sets for several neurological and psychiatric disorders, such as cerebral palsy [Schiariti et al., 2014], spinal cord injury [Post, Kirchberger, Scheuringer, Wollaars, & Geyh, 2010], bipolar disorder [Ávila, Cabello, Cieza, Vieta, & Ayuso‐Mateos, 2010], and depressive disorder [Brockow et al., 2004]. They are configurative in nature, that is, aiming to generate theory concerning functioning in ASD [Gough, Thomas, & Oliver, 2012], and can be summarized in the following review question: What aspects of ability and disability are considered most relevant to individuals with ASD from a research perspective? This review question can be further specified into a series of four review aims: (1) identify studies that focus on ability and disability in ASD, (2) identify outcome measures used in these studies to define and measure ability and disability in ASD, (3) identify meaningful concepts representing aspects of ability and disability contained in these measures, and (4) link the meaningful concepts to corresponding ICF‐CY categories.
The project is being conducted under the guidance of an international Steering Committee (SC), representing ASD opinion leaders from all six WHO regions. Among the SC duties are to provide input on the search strategy and eligibility criteria for included studies. In addition, SC members were requested to provide information on studies they considered to be landmark research in the functioning of individuals with ASD (e.g., intervention, quality of life, observation studies) that should be included in the study to comprehensively represent the research perspective. These 26 selected studies (“positive list” – see Supporting Information Appendix 1) were used for two purposes: first, to determine the relevant publication timeframe for the literature search (i.e., the range was set to include the oldest study in the selection), and second, to determine validity of the search itself (i.e., the search should include all studies of the positive list). Finally, when the literature search yielded a large number of studies, different options for narrowing down the number of articles to be analyzed were discussed with the SC, that is, restricting the publication years or the designs included in the search, drawing a random sample from the total results, or analyzing until saturation. Based on the discussion with the SC the decision was made to analyze until saturation. A detailed description of this method can be found below.
Eligibility Criteria
Types of publication
Original journal articles, published in English in 1992 or later.
Types of design
Studies of any design that present original data (including case studies, but not theoretical papers).
Types of population
Participants of any age with any ASD diagnosis (ASD, pervasive developmental disorder [PDD], autism, Asperger disorder, PDD not otherwise specified) as the primary diagnosis.
Types of outcome
Any self‐report, proxy (e.g., parent‐) report or observational/performance data that was measured as a potential outcome of ASD.
Information Sources
A systematic literature search was applied to the electronic databases Medline/PubMed, PsycINFO, ERIC and Cinahl. The search was performed in two steps: First, we selected free text terms for ASD and related functional outcomes. Terms were selected based on suggestions from the SC, previous ICF research, and systematic reviews of functioning in ASD. Second, we identified controlled vocabulary (e.g., MeSH terms, Index terms) to cover the free text terms that were selected in step one. An optimization of the search strategy was conducted by a librarian at the Karolinska Institutet University Library. Each of the four databases was examined first with the controlled vocabulary to identify relevant studies from the indexed articles, and thereafter PubMed was searched with the free text terms to identify the most recent relevant articles that had not yet been indexed (previous year only). All searches were automatically limited to journal articles that included abstracts, were in English, and involved human study populations. To create a broad selection of studies, no further restrictions were employed. The search was run on September 3, 2013. The full search strategy can be found in Supporting Information Appendix 2.
Study Selection, Data Extraction and Linking
All identified studies were collected in EndNote (Version X6, ©2012 Thomson Reuters) and duplicates were removed. The search resulted in a large number of retrieved articles (N = 17,909). We, therefore, followed the guidelines for ICF Core Sets development recommendation to analyze of a random sample of articles when the initial search yields a large number [Selb et al., 2015]. To ensure that the random selection of articles would capture the research perspective comprehensively, it was decided that the data from the articles would be analyzed until saturation of identified ICF‐CY (Children and Youth version) categories. Saturation of data refers to the point at which exhaustion is sufficiently approximated. Following procedures used in previous ICF Core Sets studies [e.g., Ávila, Alarcos, Anaya, & Ayuso‐Mateos, 2012; Glässel et al., 2011], saturation of data was defined as the point during data analysis at which the linking of concepts of two consecutive samples each revealed no more than 5% new ICF‐CY categories in relation to the number of categories already identified in this study. As a consequence of this method, the total number of studies to be analyzed was determined by the point at which saturation was reached, as this marked the end of data analysis. The size for the random samples was set at 100, because this number of studies was manageable and could provide enough information to be meaningful in the analysis.
The saturation method was applied as follows: First, full text articles for the 26 studies from the positive list were retrieved and screened for inclusion. Information was extracted from each included study on (1) characteristics of study participants (including age, diagnosis, WHO region where they were recruited); (2) type of study (observational, intervention, control group); and (3) outcome measures related to ASD (standardized and nonstandardized measures of functioning, disability and quality of life). Meaningful concepts, that is, concise descriptions of specific behaviors, skills, or other aspects of functioning to be linked to ICF‐CY categories, were extracted from the measures identified in the studies. Whenever possible concepts were extracted on the item level, but if items did not clearly represent by themselves a concept of function (e.g., items/tasks in IQ tests), concepts were extracted on subscale or full‐scale level. Screening and data extraction were conducted independently by two researchers (EdS, AL), and consensus was reached after discussion between them. The meaningful concepts identified during consensus were then linked to ICF‐CY categories, independently by the two researchers. The linked results were then compared and consensus discussions were used to determine the most relevant ICF‐CY category each of the concepts should be linked to. This resulted in a list of ICF‐CY categories that served as the baseline from which the point of data saturation was determined. Next, a random sample of 100 studies was drawn from the search results (excluding the studies from the positive list) with the help of a random integer set generator (www.random.org). Abstracts were screened for inclusion according to the eligibility criteria, independently by the two researchers. After comparing the screening results and discussing disagreements, the two researchers came to a consensus about which full text articles to include. The full text articles were then retrieved and screened for inclusion separately by the two researchers again, and data were extracted from the studies. Thereafter, the two researchers compared their screening and data extraction results, discussed disagreements and came to a consensus about meaningful concepts to be included in the linking process. Independent linking by the two researchers followed, after which linking results were compared and consensus was reached on which ICF‐CY categories concepts should be linked to after discussion of disagreements. The linking results from this sample were then compared to those from the first sample to see if more than 5% new ICF‐CY categories had been identified. This procedure was repeated by the two researchers (EdS, AL) for each following sample, until two consecutive samples revealed no more than 5% new ICF‐CY categories and saturation of data was reached (see Fig. 1). The linking was carried out according to the formalized linking rules and procedures determined by the WHO ICF research branch [Cieza et al., 2002, 2005]. Different meaningful concepts can be linked to the same ICF(‐CY) category, for example “having temper tantrums” and “feeling sad” can both be linked to the ICF(‐CY) category b152 emotional functions. The linking rules provide guidance not only on how to link concepts to ICF(‐CY) categories, but also on cases in which it is not possible to link concepts. Specific codes assigned to these concepts are (i) Personal factor, if the concept is not contained in the ICF(‐CY), but is clearly a Personal factor as defined in the ICF(‐CY); (ii) not covered, if the concept is not contained in the ICF(‐CY) and also is not a Personal factor; (iii) not definable, when the information provided in the concept is not sufficient for assigning it to a specific ICF(‐CY) category; and (iv) health condition, if the concept refers to a diagnosis or health condition.
Figure 1.
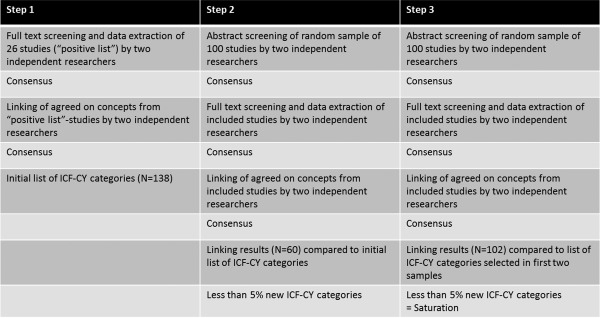
Schematic presentation of saturation method.
To evaluate initial agreement (prior to consensus in case of disagreement) between the two researchers for the linking process, the overall percentage of agreement was calculated and found to be 56% for second‐level ICF‐CY categories and 61% at the level of ICF‐CY chapters. Kappa coefficients and confidence intervals were calculated to examine the extent to which the agreements exceed chance. The Kappa value was 0.53 (SE = 0.012), with a confidence interval of 0.51‐0.55, for second‐level ICF‐CY categories, and at the level of ICF‐CY chapters the Kappa value was 0.55 (SE = 0.013), with a confidence interval of 0.53—0.58. Both Kappa values indicate a moderate agreement.
Data Analysis
Frequency analysis was used to examine the absolute number of studies in which each of the ICF‐CY categories were identified, along with the corresponding percentages relative to the total number of studies. ICF‐CY categories are presented at the second‐level. If a concept is linked to a third‐ or fourth‐level ICF‐CY category, the corresponding second‐level category is reported. Because the ICF‐CY is organized hierarchically, aspects of the more specific third‐ and fourth‐level categories are included in the less specific second‐level categories. Following the ICF Core Sets development guidelines [Selb et al., 2015], a second‐level ICF‐CY category that was identified repeatedly in one and the same study was counted only once, and only ICF‐CY categories that were identified in at least 5% of the studies were included in the list of candidate categories. The latter was done to ensure that only those categories that are most relevant to ASD were included. Additional frequency analysis was used to explore the possible relation between developmental stage of the participants and ICF‐CY categories identified in the study.
Results
Study Selection
The systematic literature search yielded a total of 17,909 citations (see Fig. 2). Out of these, a first sample of 26 citations was selected based on the positive list provided by the SC. Thereafter, two computer‐generated random samples of 100 citations were included in the analysis consecutively. As a result, a total of 226 citations were included for initial screening. Based on screening of abstracts and full text articles following eligibility criteria as described in the Methods‐section, 155 citations were excluded, leaving a total of 71 studies to be included in the data extraction and linking procedures (n = 22 for the first sample; n = 19 for the second sample; and n = 30 for the third sample). Reasons for exclusion were that the citations constituted an excluded publication (e.g., books, dissertation abstracts, published in a language other than English – 14%), the main outcome of the studies was not ability or disability in ASD (e.g., epidemiological studies – 54%), they had applied an excluded design (i.e., review study or meta‐analysis – 13%), or an excluded population (i.e., participants not having a primary diagnosis of ASD – 19%). After data extraction and linking for the 71 studies data saturation, as described above, was reached (see Supporting Information Appendix 3 for a full list).
Figure 2.
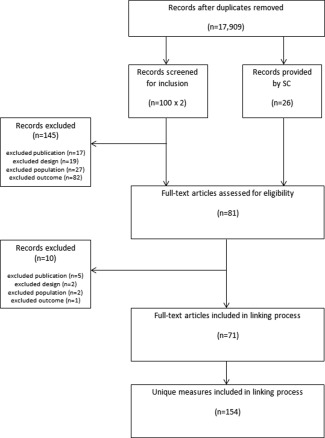
Flow diagram of study selection.
Study Characteristics
Most of the studies included in the data extraction procedure were conducted in the WHO region of the Americas (n = 38), followed by the European region (n = 22), and the Western Pacific Region (n = 10), which among others includes Australia, Japan, and China. One study was conducted in both the region of the Americas and the European region. None of the included studies were conducted in the African, Eastern Mediterranean, or South East Asian Regions. About half of the studies focused exclusively on children (n = 37), the remainder was divided among those which focused exclusively on adults (n = 14), on both children and adolescents (n = 14), on both adolescents and adults (n = 3), or on adolescents only (n = 2). One study included participants from all three different age groups [range: 9–26 yrs; Brown & Prelock, 1995].
A total of n = 101,812 individuals participated in the 71 eligible studies, with the number of participants per study ranging from n = 1 to 93,181 (Md = 44). Mean age per study ranged from 1 year 9 months to 44 year 2 months, while the chronological age range was between 1 and 80 years. Sex distribution was well balanced (47% females). However, 58 studies included more males than females, with a ratio of >3:1. This approximates the ratio commonly reported for ASD [Baird et al., 2006; Fombonne, 2009]. Three studies did not provide information with regard to the gender of participants. Twenty‐six studies included participants with either a broader diagnosis of ASD or PDD, 28 included individuals with classical autism, four included participants with Asperger disorder or high‐functioning autism, and 13 included individuals with mixed ASD diagnoses. Forty‐eight studies were observational in nature, including longitudinal and cross‐sectional studies; descriptive and case‐control studies (ASD vs. typical development or other mental health conditions). Twenty‐one studies involved intervention research, describing interventions targeting among others language abilities (e.g., Picture Exchange Communication System), social‐interaction skills (e.g., Stop‐Observe‐Deliberate‐Act training), and functioning in the workplace. To a lesser extent interventions included medication trials (i.e., naltrexone, methylphenidate, secretin, and donepezil) or alternative forms of intervention (e.g., hyperbaric oxygen therapy). One study described a Delphi exercise among ASD experts aiming to identify core functioning features in ASD [Castro & Pinto, 2013], and one was a psychometric study of an ICF‐CY‐based assessment tool for children with ASD [Gan et al., 2013]. In 17 of the studies information about the functioning of the participants was obtained from a proxy (e.g., parents, peers), whereas in 14 of the studies information was obtained from professionals working with the participants (e.g., teachers, health professionals). Five studies used information obtained from the participants themselves, while 16 studies used information from cognitive skills tests, such as the Wechsler Intelligence Scales for Children and the Theory of Mind Test. Finally, 19 studies used information from a combination of sources.
Few differences were found between characteristics of studies from the positive list and the full sample of studies, except that the positive list contained a larger proportion of observational studies (86% vs. 67%) and a smaller proportion intervention studies (5% vs. 30%); a larger proportion of studies focusing on adults (41% vs. 14%), a smaller proportion of studies focusing on children (27% vs. 52%); a larger proportion of studies using information from combination of sources (41% vs. 27%), and a smaller proportion of studies using information from cognitive and skills tests (5% vs. 23%).
Linking Results
From the 71 studies 154 unique functional outcome measures were extracted. These included 63 standardized psychometric measures, that is, questionnaires, rating scales, observation schedules, structured and semi‐structured interviews and cognitive tests, such as the Child Autism Rating Scale, Child Behavior Checklist, Vineland Adaptive Behavior Scales, Wechsler Intelligence Scales for Children, Pediatric Quality of Life Inventory, Children's Sleep Habits Questionnaire, and the Beck Depression Inventory (see Supporting Information Appendix 4 for a complete list). The remaining 91 measures were nonstandardized, for example, single questions to parents or health professionals, measures designed specifically for a study, information obtained from medical records, and clinical assessments.
From these standardized and nonstandardized outcome measures included in the linking process, 2475 meaningful concepts were extracted. Following the formalized linking rules [Cieza et al., 2002, 2005], 1920 of the meaningful concepts could be linked to ICF‐CY categories. Of the 555 concepts that could not be linked, 218 were coded as Personal factors, including general characteristics such as income or living situation; personality characteristics such as being stubborn or willing to accept help; and characteristics related to lifestyle, such as hobbies or alcohol and drug use. An additional 214 concepts were considered not to be covered by the ICF‐CY, such as self‐injurious and destructive behaviors, preference for objects or animals, and resistance to change. A total of 121 concepts provided insufficient information to be linked and were coded not definable, including concepts that were formulated in such general terms that they could not be linked to one specific category, such as “mental health,” “eye contact,” and “language.” Finally, two concepts reflected diagnoses or health conditions, such as depression, and were assigned the code health condition.
The 1920 meaningful concepts were linked to 146 different second level ICF‐CY categories. Of these, 99 were found in at least 5% of the studies (range: 6%–51%) representing those most relevant to ASD, including 63 from the Activities and Participation component, 28 from the ICF‐CY Body functions component, and 8 from the Environmental factors component.
None of the concepts was linked to categories from the Body structures component. Table 1 presents the second level categories that were identified in the Body functions component, along with the number and percentage of studies in which they were identified. As can be seen here, most of the categories identified in the Body functions component were from chapter b1 mental functions, covering the functions of the brain. The category most frequently identified here was b152 emotional functions, representing the ability to experience emotions that are consistent with a situation, and the regulation and expression of emotions. The categories b140 attention functions and b167 mental functions of language were also frequently identified. Attention functions include concepts such as sustaining attention for a required period of time, shifting attention, and sharing attention. Mental functions of language include the reception and expression of spoken, written, and other forms of language. The other chapters from which categories were identified are chapter b2 sensory functions and pain (e.g., seeing, hearing, experience of pain); chapter b3 voice and speech functions (e.g., articulation, fluency and melody of speech); chapter b4 functions of the cardiovascular, haematological, immunological and respiratory systems (e.g., hyperventilation); chapter b5 functions of the digestive, metabolic and endocrine systems (e.g., vomiting, sucking); and chapter b7 neuromusculoskeletal and movement‐related functions (e.g., coordination, motor perseveration, gait pattern).
Table 1.
Absolute and Relative Frequencies of ICF‐CY Categories From the Body Functions Component
| Second level category | N (%) |
| b152 emotional functions | 35 (49%) |
| b140 attention functions | 31 (44%) |
| b167 mental functions of language | 31 (44%) |
| b147 psychomotor functions | 30 (42%) |
| b130 energy and drive functions | 29 (41%) |
| b765 involuntary movement functions | 28 (39%) |
| b122 global psychosocial functions | 27 (38%) |
| b134 sleep functions | 26 (37%) |
| b125 dispositions and intra‐personal functions | 25 (35%) |
| b144 memory functions | 24 (34%) |
| b126 temperament and personality functions | 23 (32%) |
| b164 higher‐level cognitive functions | 21 (30%) |
| b156 perceptual functions | 20 (28%) |
| b160 thought functions | 20 (28%) |
| b330 fluency and rhythm of speech functions | 20 (28%) |
| b114 orientation functions | 19 (27%) |
| b280 sensation of pain | 19 (27%) |
| b180 experience of self and time functions | 17 (24%) |
| b110 consciousness functions | 15 (21%) |
| b320 articulation functions | 15 (21%) |
| b117 intellectual functions | 14 (20%) |
| b760 control of voluntary movement functions | 14 (20%) |
| b163 basic cognitive functions | 13 (18%) |
| b440 respiration functions | 9 (13%) |
| b770 gait pattern functions | 9 (13%) |
| b230 hearing functions | 7 (10%) |
| b172 calculation functions | 6 (8%) |
| b510 ingestion functions | 4 (6%) |
Table 2 shows the absolute and relative frequencies of the second level categories that were identified in the Activities and Participation component. Categories were identified in each of the nine chapters included in this component. The two most identified categories are from chapter d7 interpersonal interactions and relationships, and they reflect both basic and complex interaction skills, such as giving and responding appropriately to social cues in interactions, making and responding to physical contact appropriately, forming relationships, and regulating behaviors within interactions. The categories that were second most frequently identified belong to chapter d3 communication and represent the production and comprehension of verbal and nonverbal communication. Other categories from the same chapter, describing further forms of communication were also included in the selection in Table 2. The remaining chapters included in the Activities and Participation component were chapter d1 learning and applying knowledge (e.g., different ways of learning, reading, writing, thinking, directing attention); chapter d2 general tasks and demands (e.g., undertaking and completing tasks, managing daily routine, handling responsibilities, managing behavior); chapter d4 mobility (e.g., moving around, fine hand use, driving); chapter d5 self‐care (e.g., washing oneself, toileting, looking after one's health); chapter d6 domestic life (e.g., preparing meals, doing housework); chapter d8 major life areas (e.g., education, employment, economic life); and chapter d9 community, social and civic life (e.g., sports, hobbies, socializing).
Table 2.
Absolute and Relative Frequencies of ICF‐CY Categories From the Activities and Participation Component
| Second level category | N (%) |
| d710 basic interpersonal interactions | 36 (51%) |
| d720 complex interpersonal interactions | 34 (48%) |
| d335 producing nonverbal messages | 29 (41%) |
| d310 communicating with – receiving – spoken messages | 28 (39%) |
| d130 copying | 27 (38%) |
| d250 managing one's own behavior | 26 (37%) |
| d330 speaking | 25 (35%) |
| d880 engagement in play | 25 (35%) |
| d315 communicating with – receiving – nonverbal messages | 24 (34%) |
| d750 informal social relationships | 24 (34%) |
| d920 recreation and leisure | 24 (34%) |
| d163 thinking | 23 (32%) |
| d350 conversation | 23 (32%) |
| d161 directing attention | 22 (31%) |
| d210 undertaking a single task | 22 (31%) |
| d530 toileting | 22 (31%) |
| d160 focusing attention | 21 (30%) |
| d331 pre‐talking | 21 (30%) |
| d132 acquiring information | 20 (28%) |
| d230 carrying out daily routine | 20 (28%) |
| d540 dressing | 20 (28%) |
| d550 eating | 20 (28%) |
| d220 undertaking multiple tasks | 19 (27%) |
| d440 fine hand use | 19 (27%) |
| d445 hand and arm use | 19 (27%) |
| d455 moving around | 19 (27%) |
| d137 acquiring concepts | 18 (25%) |
| d177 making decisions | 18 (25%) |
| d240 handling stress and other psychological demands | 18 (25%) |
| d475 driving | 18 (25%) |
| d630 preparing meals | 18 (25%) |
| d850 remunerative employment | 18 (25%) |
| d170 writing | 17 (24%) |
| d470 using transportation | 17 (24%) |
| d510 washing oneself | 17 (24%) |
| d560 drinking | 17 (24%) |
| d640 doing housework | 17 (24%) |
| d110 watching | 16 (23%) |
| d155 acquiring skills | 16 (23%) |
| d166 reading | 16 (23%) |
| d172 calculating | 16 (23%) |
| d435 moving objects with lower extremities | 16 (23%) |
| d571 looking after one's safety | 16 (23%) |
| d845 acquiring, keeping and terminating a job | 16 (23%) |
| d134 acquiring additional language | 15 (21%) |
| d140 learning to read | 15 (21%) |
| d145 learning to write | 15 (21%) |
| d360 using communication devices and techniques | 15 (21%) |
| d450 walking | 15 (21%) |
| d520 caring for body parts | 15 (21%) |
| d570 looking after one's health | 15 (21%) |
| d660 assisting others | 15 (21%) |
| d910 community life | 15 (21%) |
| d410 changing basic body position | 14 (20%) |
| d415 maintaining a body position | 14 (20%) |
| d430 lifting and carrying objects | 14 (20%) |
| d650 caring for household objects | 14 (20%) |
| d865 complex economic transactions | 14 (20%) |
| d120 other purposeful sensing | 6 (8%) |
| d760 family relationships | 6 (8%) |
| d855 nonremunerative employment | 6 (8%) |
| d131 learning through actions with objects | 5 (7%) |
| d770 intimate relationships | 4 (6%) |
Absolute and relative frequencies of the categories identified in the Environmental factors component are summarized in Table 3. Categories from three different chapters were identified, the two most identified coming from chapter e5 services, systems and policies. The first category, e585 education and training services, systems and policies, include schools and special education services. The second, e580 health services, systems and policies, represents health services aimed at treating and preventing health problems and promoting a healthy lifestyle. Five of the categories come from chapter e3 support and relationships, which includes different (groups of) persons that can provide physical or emotional support, such as friends and family. Finally, one category was identified from chapter e4 attitudes, which describes how attitudes of different (groups of) people can influence their behavior toward the individual with a health condition.
Table 3.
Absolute and Relative Frequencies of ICF‐CY Categories From the Environmental Factors Component
| Second level category | N (%) |
| e585 education and training services, systems and policies | 11 (15%) |
| e580 health services, systems and policies | 6 (8%) |
| e310 immediate family | 4 (6%) |
| e315 extended family | 4 (6%) |
| e320 friends | 4 (6%) |
| e325 acquaintances, peers, colleagues, neighbours and community members | 4 (6%) |
| e355 health professionals | 4 (6%) |
| e425 individual attitudes of acquaintances, peers, colleagues, neighbours and community members | 4 (6%) |
Additional frequency analysis exploring the possible relationships between the developmental stage of the participants and the concepts measured in the study revealed no specific relations. Due to the limited number of studies in the different age groups, it was not possible to draw any meaningful conclusions. However, apart from certain typically age related categories, such as d475 driving and d770 intimate relationships, there was no obvious tendency for categories being measured specific to age group.
Discussion
The purpose of this study was to capture from prior research perspectives on what constitute the relevant aspects of ability and disability in individuals with ASD of all ages. Applying a formalized procedure developed by the WHO and the ICF Research Branch in a systematic review of the literature on functioning in ASD we extracted meaningful ability and disability concepts from standardized and nonstandardized measures used in the included studies and translated them into ICF‐CY categories. This way of analyzing the literature is currently unique to the ICF Core Sets development process and was performed for the first time in ASD. Together with the results from three additional ongoing preparatory studies, this review will provide the scientific basis for the definition of ICF Core Sets for ASD.
The relatively large number of ICF‐CY categories most relevant to ASD (i.e., found in at least 5% of the studies) reflects the heterogeneity of functional affects typically associated with ASD, with difficulties in numerous areas of everyday life, thereby emphasizing the potential importance of the ICF‐CY as a structured means of describing functioning in ASD. In line with the current study, a recent review of the literature on outcomes in adolescents and adults with ASD [Levy & Perry, 2011] identified aspects of functioning comparable to the ones found here as the basis for linking to the ICF‐CY, for instance cognitive and language skills, adaptive behavior, education, occupation, living situation, and social integration.
Our study found that with regards to the core defining features of ASD, social‐communication characteristics were captured by ICF‐CY categories from the interpersonal interaction and communication chapters, while some of the repetitive and stereotyped behaviors were found in the categories reflecting psychomotor functions and various movement functions. Some of these behaviors were also found to be not covered by the ICF‐CY. This seems contradictory, but can be understood by taking a closer look at the concepts involved. Concepts such as “rocking body back and forth repeatedly” and “meaningless, recurring body movements” clearly fall within the ICF‐CY category of stereotypies and motor perseveration. However, concepts like “rituals” and “limited behaviors and interests” may also be considered part of the ASD defining characteristic of restricted and repetitive behaviors, but do not in themselves represent deficits in functioning and are therefore considered not to be covered by the ICF‐CY. In this regard, it is important to keep in mind that ICF‐CY aims to assess the impact of a health condition or the individual ability and disability associated with it, rather than to record the diagnostic criteria of a particular disorder in another form. Thus, a wide range of other ICF‐CY categories were identified as particularly relevant for individuals with ASD. These included many cognitive and language outcomes which are described within the mental functions of language and the basic and higher‐level cognitive functions chapter of the ICF‐CY. Adaptive behaviors in ASD (i.e., an individual's ability to complete everyday skills) were represented by categories from the entire Activities and Participation component, and concrete social outcomes by the interpersonal interaction and communication chapters of the same component. Social integration outcomes were identified in the interpersonal interactions chapter, and even in the categories describing community, social and civic life. Education and occupation can be found in the categories of the major life areas chapter. The living situation of an individual, however, would be considered a Personal factor and as these are not coded in ICF‐CY could, therefore, not be classified directly.
In their review, Levy and Perry [2011] concluded that hitherto most ASD outcome studies focused merely on one aspect of functioning, and that more comprehensive outcome research in ASD is imperative. Moreover, the fact that the most frequently identified categories in the current study most frequently represent diagnostic symptoms of ASD (i.e., interpersonal interactions, social communication, language) suggests a bias in the research toward studying these core features rather than broader impacts. The much wider range of functional aspects found to be related to ASD in this review encourages future research with a broad focus on ability and disability in all areas of life. By providing scientifically derived clear guidelines about “what to measure” if trying to gain a comprehensive assessment of functioning in individuals with ASD, the ICF Core Sets for ASD will be valuable tools in filling that gap. The selection of ICF‐CY categories resulting from this study, which represents the research and researchers' perspectives, is simply the first step toward the development of a comprehensive but usable toolkit. It will be complemented by information from a diverse and international range of clinical experts, individuals with ASD and other stakeholders across WHO regions, and by clinical studies in different countries.
Twenty‐two percent of the concepts identified could not be linked to ICF‐CY categories. Nearly half of these were found to be Personal Factors, that is, features that are intrinsic to the individual and are not part of a health condition. Although Personal factors are considered essential for fully describing functional outcome by the ICF(‐CY), their large diversity and variety of significance among cultures has resulted in them not being systematized within the manuals to date. Instead, it is recommended that ICF(‐CY) users assess and describe them in another manner that is suitable for their practical use. It is important to include Personal factors in the description of an individual's functioning, because they may influence ability and disability. For example, in ASD gender differences have been found, with females showing higher degrees of social, attention and thought problems [Holtmann, Bölte, & Poustka, 2007]. Gender differences have also been found in executive functioning in ASD, where females showed higher performance on tests of cognitive flexibility but lower performance on attention to detail, as compared to males [Bölte, Duketis, Poustka, & Holtmann, 2011]. Despite their relevance as contributing factors to ability and disability, the use of Personal factors needs to be approached with caution, precisely because they are not yet systematized. In a critical examination of the construct of Personal factors in the ICF(‐CY), Simeonsson et al. point out that there are considerable risks in applying Personal factors in the absence of formal codes [2014]. The lack of a clear definition with inclusion and exclusion criteria, the absence of a clearly stated purpose for their inclusion in the classification, and the need for guidelines about their documentation, combined with the absence of formal codes may have unknown and unwanted consequences when Personal factors are implemented. These could include idiosyncratic use (i.e., each user creates his/her own definition with inclusion and exclusion criteria), establishment of the component of Personal factors based on exemplars provided by users, and the risk of “blaming the victim” where Personal factors are seen as causal or contributing to an individual's health condition or disability. These issues are also discussed by Müller and Geyh [2015] in a recent review of the efforts that have been made to provide categorization of Personal factors. They argue that, despite the potential risks of uncontrolled classification, disregarding Personal factors may likely mean disregarding opportunities to provide individually targeted interventions and support. They conclude that the eight suggestions for categorization of Personal factors presented in their paper provide a valuable basis for the further development of a standardized classification, provided the development follows sophisticated classification methodologies. Given this debate on the value of classifying Personal factors on the one hand, and the problems and risks involved in doing so based on their lacking conceptualization and systemization on the other, the ongoing development of the ICF Core Sets for ASD will include a discussion by the SC and Consensus Conference experts, whether such a more systematic approach to Personal factors would be feasible.
Another 9% of identified concepts were deemed not to be covered by the ICF(‐CY). These included many key diagnostic features of ASD, such as restricted and repetitive behaviors, self‐injurious behaviors, and behaviors that reflect poor adjustment. The fact that these specific ASD behaviors fall outside the scope of the ICF‐CY raises questions about the usefulness of this system in the assessment and classification of functioning in individuals with ASD. However, as mentioned earlier, the ICF‐CY is intended to complement rather than duplicate the International Classification of Diseases (ICD)‐10 classification, which provides diagnosis of a certain health condition and describes its specific symptoms. We would argue that the ASD specific behaviors coded as “not covered” in this study fall more within the scope of a diagnostic classification system such as the ICD‐10, while impairments in the individual's everyday living resulting from these behaviors are within the remit of a functional classification system such as the ICF‐CY. For example, the preference for objects over humans could be considered the expression of an ASD symptom and covered by the ICD‐10 while difficulties forming relationships with peers are an impairment resulting from this symptom and are covered by the ICF‐CY. The finding thus stresses the need to use the ICF‐CY as a complement to the ICD‐10, as is intended.
Limitations
Certain limitations of the study may have led to an underrepresentation of ICF‐CY categories that are relevant to the assessment and classification of functioning in individuals with ASD. First, there was a restriction of the search results to studies published in English. Indeed the majority of the studies included in the review were conducted in the United States, Canada, and European countries. If there are any ICF‐CY categories that are specifically relevant in low‐ and middle income countries they may have been overlooked. In addition, most of the studies focused on children. Even though this represents a general tendency in research on ASD [Howlin & Moss, 2012], it may have resulted in an underrepresentation of ICF‐CY categories that are specifically relevant for adults with ASD. In addition, there is an emerging recognition that ASD differences produce traits of exceptionality in some people, but the current ASD literature is focused almost exclusively on disability effect. Consequently, those traits may be underrepresented here to the extent that they are different from the recognized traits associated with disability in ASD. Finally, based on the large number of studies identified in the literature search it was decided to analyze a smaller sample of studies. Even though measures have been taken to ensure that the researchers' perspective was captured comprehensively, including the analysis of the studies provided by the SC and analysis of additional random samples of studies until saturation was reached, it is still possible that additional ICF‐CY categories would have been identified if a larger selection of studies had been included. However, we believe that these shortcomings will be adequately compensated for by the three additional preparatory studies to be conducted in the development process. These were designed specifically to ensure that a global perspective on functioning in a certain health condition is captured and to enable appropriate implementation of ICF Core Sets. In the expert survey, for example, opinion leaders from all six WHO‐regions will be included, so that aspects of functioning that are relevant in low‐ and middle‐income countries across high and low resource environments and cultures will be captured. Furthermore, the focus group study will include children, adolescents and adults, as well as parents, teachers and other people living or working closely with individuals with ASD in nonclinical settings, so that each of their perspectives and the ICF‐CY categories that may be relevant for their specific situations will be included in the selection. In addition, the focus groups will be held in various parts of the world so that a global perspective on functioning in ASD from the client's point of view is captured. Finally, a group of experts from various backgrounds, disciplines, low‐, middle‐, and high‐income countries and cultures across all WHO regions will decide which ICF‐CY categories are to be included in the ICF Core Sets for ASD, ensuring that they will be universally applicable across the life span.
Acknowledgments
The development of the ICF Core Sets for ASD is a cooperative effort of the WHO, the ICF Research Branch, a partner of the WHO Collaborating Centre for the Family of International Classifications in Germany (at DIMDI), the International Society for Autism Research (INSAR), and the Center of Neurodevelopmental Disorders at the Karolinska Institutet (KIND) in Sweden. Guidance on this project is provided by a Steering Committee comprised of key opinion leaders in the field of ASD from all six WHO regions. This Steering Committee consists of the coauthors of this paper and Judith Hollenweger, Omar Al‐Modayfer, Melissa Selb, Susan Swedo, Bedirhan Üstün. The development of ICF Core Sets for ASD is supported by the Swedish Research Council (grant nr. 523‐2009‐7054), and the Swedish Research Council in partnership with FAS (now renamed FORTE), FORMAS and VINNOVA (cross‐disciplinary research program concerning children's and youth's mental health, grant nr. 259‐2012‐24).
Conflict of interest
The authors declare that they have no conflict of interest related to this work.
Supporting information
Additional Supporting Information may be found in the online version of this article at the publisher's web‐site:
Appendix 1—List of Essential Studies Provided by the Steering Committee
Appendix 2—Search Strategies
Appendix 3—Studies Included in the Data Extraction and Linking Procedure
Appendix 4—Standardized Measures Identified in the Studies
References
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Ávila, C.C. , Alarcos, C. , Anaya, C. , & Ayuso‐Mateos, J.L. (2012). The patients' perspective on relevant areas and problems in the bipolar spectrum disorder: Individual interviews using the International Classification of Functioning, Disability and Health as a reference tool. American Journal of Physical Medicine and Rehabilitation, 91 (Suppl.), s181–s188. [DOI] [PubMed] [Google Scholar]
- Ávila, C.C. , Cabello, M. , Cieza, A. , Vieta, E. , & Ayuso‐Mateos, J.L. (2010). Functioning and disability in bipolar disorders: A systematic review of literature using the ICF as a reference. Bipolar Disorders, 12, 473–482. [DOI] [PubMed] [Google Scholar]
- Baird, G. , Simonoff, E. , Pickles, A. , Chandler, S. , Loucas, T. , Meldrum, D. , et al. (2006). Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). Lancet, 368, 210–215. [DOI] [PubMed] [Google Scholar]
- Brockow, T.T. , Wohlfahrt, K. , Hillert, A. , Geyh, S. , Weigl, M. , Franke, T. , et al. (2004). Identifying the concepts contained in outcome measures of clinical trials on depressive disorders using the International Classification of Functioning, Disability and Health as a reference. Journal of Rehabilitation Medicine, Suppl. 44, 49–55. [DOI] [PubMed] [Google Scholar]
- Brown, J. , & Prelock, P.A. (1995). Brief report: The impact of regression on language development in autism. Journal of Autism and Developmental Disorders, 25, 305–309. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , Duketis, E. , Poustka, F. , & Holtmann, M. (2011). Sex differences in cognitive domains and their clinical correlates in higher‐functioning autism spectrum disorders. Autism, 15, 497–511. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , de Schipper, E. , Robison, J.E. , Wong, V.C.N. , Selb, M. , Singhal, N. , et al. (2013). Classification of functioning and impairment: The development of ICF Core Sets for Autism Spectrum Disorder. Autism Research, 7(1), 167–172. [DOI] [PubMed] [Google Scholar]
- Castro, S. , Ferreira, T. , Dababnah, S. , & Pinto, A.I. (2013). Linking autism measures with the ICF‐CY: Functionality beyond the borders of diagnosis and interrater agreement issues. Developmental Neurorehabilitation, 16, 321–331. [DOI] [PubMed] [Google Scholar]
- Castro, S. & Pinto, A.I. (2013). Identification of core functioning features for assessment and intervention in autism spectrum disorders. Disability & Rehabilitation, 35, 125–133. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Brockow, T. , Ewert, T. , Amman, E. , Kollerits, B. , Chatterji, S. , et al. (2002). Linking health‐status measurements to the International Classification of Functioning, Disability and Health. Journal of Rehabilitation Medicine, 34, 205–210. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Chatterji, S. , Andersen, C. , Cantista, P. , Herceg, M. , Melvin, J. , et al. (2004). ICF Core Sets for depression. Journal of Rehabilitation Medicine, Suppl. 44, 128–134. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Geyh, S. , Chatterji, S. , Kostanjsek, N. , Üstün, B. , & Stucki, G. (2005). ICF linking rules: An update based on lessons learned. Journal of Rehabilitation Medicine, 37, 212–218. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Kirchberger, I. , Biering‐Sørensen, F. , Baumberger, M. , Charlifue, S. , Post, M.W. , et al. (2010). ICF Core Sets for individuals with spinal cord injury in the long‐term context. Spinal Cord, 48, 305–312. [DOI] [PubMed] [Google Scholar]
- Danermark, B. , Granberg, S. , Kramer, S.E. , Selb, M. , & Möller, C. (2013) The creation of a comprehensive and a brief core set for hearing loss using the International Classification of Functioning, Disability and Health. American Journal of Audiology, 22, 323–328. [DOI] [PubMed] [Google Scholar]
- Fombonne, E. (2009). Epidemiology of pervasive developmental disorders. Pediatric Research, 65, 591–598. [DOI] [PubMed] [Google Scholar]
- Gan, S.M. , Tung, L.C. , Yeh, C.Y. , & Wang, C.H. (2013). ICF‐CY based assessment tool for children with autism. Disability & Rehabilitation, 35, 678–685. [DOI] [PubMed] [Google Scholar]
- Glässel, A. , Finger, M.E. , Cieza, A. , Treitler, C. , Coenen, M. , & Escorpizo, R. (2011). Vocational rehabilitation from the client's perspective using the International Classification of Functioning, Disability and Health (ICF) as a reference. Journal of Occupational Rehabilitation, 21, 167–178. [DOI] [PubMed] [Google Scholar]
- Gough, D. , Thomas, J. , & Oliver, S. (2012). Clarifying differences between review designs and methods. Systematic Reviews, 1, 28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Happé, F. , & Frith, U. (2009). The beautiful otherness of the autistic mind. Philosophical Transactions of the Royal Society B, 364, 1345–1350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holtmann, M. , Bölte, S. , & Poustka, F. (2007). Autism spectrum disorders: Sex differences in autistic behavior domains and coexisting psychopathology. Developmental Medicine & Child Neurology, 49, 361–366. [DOI] [PubMed] [Google Scholar]
- Howlin, P. , & Moss, P. (2012). Adults with autism spectrum disorders. Canadian Journal of Psychiatry, 57(5), 275–283. [DOI] [PubMed] [Google Scholar]
- Ibragimova, N. , Granlund, M. , & Björck‐Åkesson, E. (2009). Field trial of ICF version for children and youth (ICF‐CY) in Sweden: Logical coherence, developmental issues and clinical use. Developmental Neurorehabilitation, 12, 3–11. [DOI] [PubMed] [Google Scholar]
- Kirchberger, I. , Cieza, A. , Biering‐Sørensen, F. , Baumberger, M. , Charlifue, S. , Post, M.W. , et al. (2010). ICF Core Sets for individuals with spinal cord injury in the early post‐acute context. Spinal Cord, 48, 297–304. [DOI] [PubMed] [Google Scholar]
- Levy, A. , & Perry, A. (2011). Outcomes in adolescents and adults with autism: A review of the literature. Research in Autism Spectrum Disorders, 5, 1271–1282. [Google Scholar]
- Mottron, L. , Dawson, M. , & Soulières, I. (2009). Enhanced perception in savant syndrome: Patterns, structure and creativity. Philosophical Transactions of the Royal Society B, 364, 1385–1391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Müller, R. , & Geyh, S. (2015). Lessons learned from different approaches towards classifying personal factors. Disability and Rehabilitation, 37, 430–438. [DOI] [PubMed] [Google Scholar]
- Post, M.W.M. , Kirchberger, I. , Scheuringer, M. , Wollaars, M.M. , & Geyh, S. (2010). Outcome parameters in spinal cord injury research: A systematic review using the International Classification of Functioning, Disability and Health (ICF) as a reference. Spinal Cord, 48, 522–528. [DOI] [PubMed] [Google Scholar]
- Ruof, J. , Cieza, A. , Wolff, B. , Angst, F. , Ergeletzis, D. , Omar, Z. , et al. (2004). ICF core sets for Diabetes Mellitus. Journal of Rehabilitation Medicine, Suppl. 44, 100–106. [DOI] [PubMed] [Google Scholar]
- Schiariti, V. , Klassen, A.F. , Cieza, A. , Sauve, K. , O'Donnell, M. , Armstrong, R. , et al. (2014). Comparing contents of outcome measures in cerebral palsy using the international classification of functioning (ICF‐CY): A systematic review. European Journal of Paediatric Neurology, 18, 1–12. [DOI] [PubMed] [Google Scholar]
- Selb, M. , Escorpizo, R. , Kostanjsek, N. , Stucki, G. , Üstün, B. , & Cieza, A. (2015). A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. European Journal of Physical and Rehabilitation Medicine, 51, 105–117. [PubMed] [Google Scholar]
- Simeonsson, R.J. , Lollar, D. , Björck‐Åkesson, E. , Granlund, M. , Brown, S.C. , Zhuoying, Q. , et al. (2014). ICF and ICF‐CY lessons learned: Pandora's box of personal factors. Disability and Rehabilitation, 36, 2187–2194. [DOI] [PubMed] [Google Scholar]
- Stucki, G. , & Grimby, G. (2004). Applying the ICF in medicine. Journal of Rehabilitation Medicine, 36 (Suppl. 44), 5–6. [DOI] [PubMed] [Google Scholar]
- Üstün, B. , Chatterji, S. , & Kostanjsek, N. (2004). Comments from WHO for the Journal of Rehabilitation Medicine special supplement on ICF Core Sets. Journal of Rehabilitation Medicine, 36 (Suppl. 44), 7–8. [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2001). International classification of functioning, disability and health: ICF. Geneva: World Health Organization. [Google Scholar]
- World Health Organization . (2007). International classification of functioning, disability and health: Children and youth version: ICF‐CY. Geneva: World Health Organization. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional Supporting Information may be found in the online version of this article at the publisher's web‐site:
Appendix 1—List of Essential Studies Provided by the Steering Committee
Appendix 2—Search Strategies
Appendix 3—Studies Included in the Data Extraction and Linking Procedure
Appendix 4—Standardized Measures Identified in the Studies