

Abstract
Aims
The aim of this study was to compare the clinical effectiveness of Kirschner wire (K-wire) fixation with locking-plate fixation for patients with a dorsally displaced fracture of the distal radius in the five years after injury.
Patients and Methods
We report the five-year follow-up of a multicentre, two-arm, parallel-group randomized controlled trial. A total of 461 adults with a dorsally displaced fracture of the distal radius within 3 cm of the radiocarpal joint that required surgical fixation were recruited from 18 trauma centres in the United Kingdom. Patients were excluded if the surface of the wrist joint was so badly displaced it required open reduction. In all, 448 patients were randomized to receive either K-wire fixation or locking-plate fixation. In the K-wire group, there were 179 female and 38 male patients with a mean age of 59.1 years (19 to 89). In the locking-plate group, there were 194 female and 37 male patients with a mean age of 58.3 years (20 to 89). The primary outcome measure was the patient-rated wrist evaluation (PRWE). Secondary outcomes were health-related quality of life using the EuroQol five-dimension three-level (EQ-5D-3L) assessment, and further surgery related to the index fracture.
Results
At 12 months, 402/448 participants (90%) recruited into the main study provided PRWE scores. At year two, 294 participants (66%) provided scores; at year five, 198 participants (44%) provided scores. There was no clinically relevant difference in the PRWE at any point during the five-year follow-up; at five years, the PRWE score was 8.3 (12.5) in the wire group and 11.3 (15.6) in the plate group (95% confidence interval -6.99 to 0.99; p = 0.139). Nor was there a clinically relevant difference in health-related quality of life. Only three participants had further surgery in the five years after their injury (one in the wire group and two in the plate group).
Conclusion
This follow-up study continues to show no evidence of a difference in wrist pain, wrist function, or quality of life for patients treated with wires versus locking plates in the five years following a dorsally displaced fracture of the distal radius.
Cite this article: Bone Joint J 2019;101-B:978–983.
Keywords: Distal radius, Kirschner wire, Locking plate, Long-term, Randomized controlled trial
In 2014, we published the Distal Radius Acute Fracture Fixation Trial (DRAFFT).1 This compared percutaneous Kirschner wire (K-wire) fixation with volar locking-plate fixation for patients with a dorsally displaced fracture of the distal radius (wrist fracture). The trial showed no evidence of a difference in functional outcome or quality of life for patients at any time during the first year after the injury. The associated health economic evaluation demonstrated that that locking-plate fixation is very unlikely to be cost effective.2,3 These findings contradicted much of the existing literature and led to a rapid and substantial change in clinical practice in the United Kingdom.4
However, a major criticism of the original DRAFFT report was that it only included one year of follow-up.5 What if patients developed persistent symptoms that affected their wrist function in the longer-term? What if patients required revision surgery after one year, or required extensive salvage surgery for arthritis?
We therefore present the outcomes at five years of the original DRAFFT trial cohort. The primary objective was to estimate differences in the patient-rated wrist evaluation (PRWE) between those patients treated with K-wire fixation and those treated with locking-plate fixation. Secondary objectives were to estimate differences in health-related quality of life and the need for further surgery related to the fracture.
Patients and Methods
Synopsis of the DRAFFT trial
DRAFFT was a two-arm, parallel-group randomized controlled trial (RCT) that recruited from 18 trauma centres in the United Kingdom. Adults with a dorsally displaced fracture of the distal radius within 3 cm of the radiocarpal joint were eligible for inclusion if their treating surgeon believed that they would benefit from surgical fixation. Patients were excluded if the surgeon thought that the surface of the wrist joint was so badly displaced that it required open reduction. Half of the patients were randomized to receive K-wire fixation and the other half locking-plate fixation. Following the completion of the first 12 months of clinical review, participants were approached to provide consent to be included in the five-year long-term follow-up. Participants were contacted yearly by post, to complete the PRWE (which was the primary outcome measure) and the EuroQol five-dimension three-level (EQ-5D-3L) health-related quality of life assessment, and to report any additional surgery related to the index wrist fracture. The PRWE score6 is a questionnaire designed specifically for assessment of distal radial fractures and wrist injuries that rates wrist function using a range of questions in two (equally weighted) sections concerning the patient’s experience of pain and function. Scoring for all the questions is via an 11-point, ordered, categorical scale ranging from ‘no pain’ or ‘no difficulty’ (0) to ‘worst possible pain’ or ‘unable to do’ (10). The EQ-5D is a validated generalized quality of life questionnaire consisting of five domains of health; patients’ responses can be converted to health state utility values,7 anchored at 1 (perfect health) and 0 (death).8
Statistical analysis
Mixed-effects linear regression analysis was used for longitudinal analysis of PRWE and EQ-5D scores using data from years one to five postoperation, with sex, age group (dichotomized into patients younger and older than 50 years of age), intra-articular extension, and year of follow-up (log-transformed) as explanatory variables. The significance of terms in the fitted models were assessed using likelihood ratio tests (LRT), with significance set at the 5% level. Cross-sectional analysis of scores was also undertaken using Student’s t-tests to assess differences between treatment groups at each assessment occasion. Mixed-effect logistic regression analysis was used to assess patterns of missing PRWE data during follow-up with participant as the random effect, and with sex, age group, and intra-articular extension added as explanatory variables. A complete-case analysis was used for consistency with previous reporting of data from the DRAFFT study. No adjustments were made for multiple testing. All analyses were implemented in R (version 3.3.0; R Foundation for Statistical Computing, Vienna, Austria) using the package lme4.9
Results
Population
For the DRAFFT RCT, 461 patients were recruited and followed to one year. Of these, 230 were allocated to the wire arm and 231 to the plate arm of the study. In the wire arm, 208 participants received the allocated intervention and 18 went on to receive the plate intervention; in the plate group, 213 participants received the allocated intervention and nine received the wire intervention. In all, 13 patients did not receive either of the treatments under investigation; the majority (85%) were treated with a cast. For the purposes of this follow-up study, patients are analyzed according to the treatment they received. Therefore, in total, 217 participants received the wire intervention and 231 participants received the plate intervention.
Table I shows the main characteristics of the population. There was no evidence that the participants differed between intervention arms.
Table I.
Population characteristics at recruitment (baseline)
| Variable | Wire (n = 217) | Plate (n = 231) | p-value |
|---|---|---|---|
| Mean age, (sd); range | 59.1 (16.5); 19 to 89 | 58.3 (14.3); 20 to 89 | 0.599* |
| Sex, female:male (%) | 179:38 (82.4) | 194:37 (84.0) | 0.705† |
| Intra-articular extension, no:yes (%) | 115:102 (53.0) | 121:110 (52.4) | 0.925† |
| Pre-injury baseline scores | |||
| Mean PRWE, (sd); range | 2.3 (7.4); 0 to 53 | 2.9 (9.5); 0 to 76 | 0.460* |
| Mean DASH, (sd); range | 4.9 (11.9); 0 to 80 | 4.9 (11.3); 0 to 66 | 0.999* |
| Mean EQ-5D-3L, (sd); range | 0.93 (0.16); 0.1 to 1.0 | 0.93 (0.17); 0.0 to 1.0 | 0.806* |
Student’s t-test
Fisher’s exact test
PRWE, patient-rated wrist evaluation; DASH, Disabilities of Arm, Shoulder, And Hand; EQ-5D-3L, EuroQol five-dimension three-level health-related quality-of-life assessment
Follow-up patterns
At the 12-month assessment, 402/448 participants (90%) recruited into the main study provided PRWE scores. A total of 301 patients provided consent for the long-term follow-up phase of the trial. At year two, 294 participants (66%) provided scores; by year five, 198 (44%) of the original cohort provided scores (Fig. 1).
Fig. 1.

Overall flow of participants and follow-up for the long-term follow-up (LTFU) study. DRAFFT, Distal Radius Acute Fracture Fixation Trial; RCT, randomized controlled trial.
Response rates declined significantly during the data collection period from year two to year five (Figure 2), and were lower for those participants under 50 years of age than for those over 50 years of age. However, there was no evidence that response rates were different between treatment groups.
Fig. 2.

Percentage of the missing data for long-term follow-up (LTFU) study population by year of follow-up for: a) treatment; b) age; c) sex; and d) intra-articular extension. Population size from years one to five was 415, 300, 241, 213, and 203, respectively.
Outcomes
Figure 3 shows the changes in PRWE and EQ-5D scores during the five-year follow-up study, and Table II shows means, differences, and unadjusted tests of treatment differences calculated on a cross-sectional basis.
Table II.
Treatment differences on a yearly cross-sectional basis for PRWE and EQ-5D scores
| Outcome/year | Wire (n = 217) | Plate (n = 231) | Raw difference (95% CI) | Adjusted difference (95% CI) | p-value* | ||
|---|---|---|---|---|---|---|---|
| n | Mean (sd) | n | Mean (sd) | ||||
| PRWE | |||||||
| 1 | 198 | 15.1 (15.7) | 204 | 14.1 (17.3) | 1.04 (-2.20 to 4.29) | 1.06 (-2.19 to 4.31) | 0.521 |
| 2 | 137 | 11.7 (15.0) | 157 | 13.6 (16.9) | -1.84 (-5.54 to 1.85) | -1.84 (-5.53 to 1.86) | 0.328 |
| 3 | 106 | 9.9 (14.4) | 129 | 11.1 (14.2) | -1.22 (-4.93 to 2.48) | -1.12 (-4.81 to 2.56) | 0.549 |
| 4 | 97 | 8.7 (13.0) | 110 | 11.6 (15.1) | -2.87 (-6.76 to 1.02) | -2.75 (-6.63 to 1.13) | 0.164 |
| 5 | 93 | 8.3 (12.5) | 105 | 11.3 (15.6) | -3.00 (-6.99 to 0.99) | -2.91 (-6.91 to 1.08) | 0.152 |
| EQ-5D | |||||||
| 1 | 191 | 0.84 (0.19) | 195 | 0.84 (0.20) | 0.00 (-0.04 to 0.04) | 0.00 (-0.04 to 0.04) | 0.999 |
| 2 | 135 | 0.88 (0.15) | 155 | 0.86 (0.18) | 0.03 (-0.01 to 0.07) | 0.03 (-0.01 to 0.06) | 0.185 |
| 3 | 105 | 0.87 (0.19) | 129 | 0.88 (0.17) | -0.01 (-0.05 to 0.04) | -0.01 (-0.05 to 0.04) | 0.769 |
| 4 | 96 | 0.88 (0.16) | 110 | 0.86 (0.18) | 0.02 (-0.02 to 0.07) | 0.02 (-0.02 to 0.07) | 0.339 |
| 5 | 93 | 0.89 (0.17) | 105 | 0.84 (0.20) | 0.05 (0.00 to 0.10) | 0.05 (0.00 to 0.10) | 0.055 |
p-value from regression analysis after adjusting for age group and intra-articular extension
PRWE, patient-rated wrist evaluation; EQ-5D, EuroQol EQ-5D; CI, confidence interval
Fig. 3.
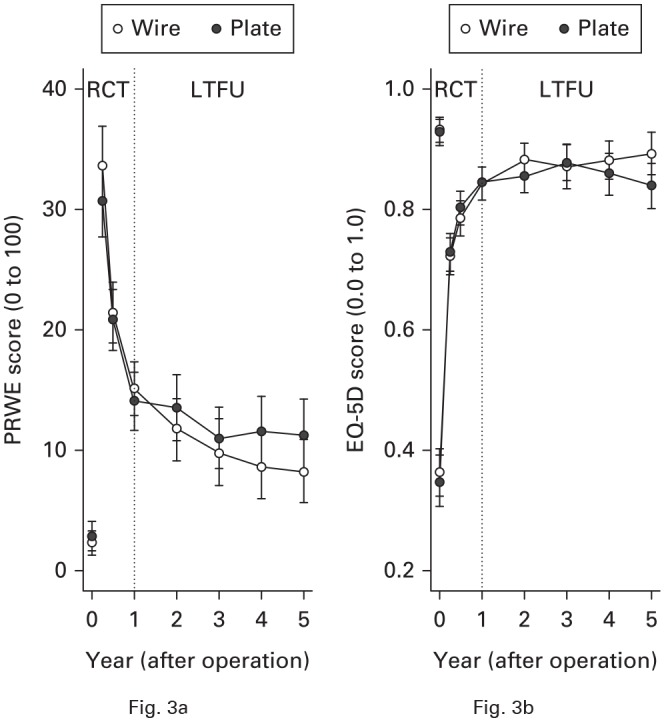
Temporal trends in mean (95% confidence interval (CI)) for a) patient-rated wrist evaluation (PRWE) scores, and b) EuroQol five-dimension three-level (EQ-5D) assessment scores during the randomized controlled trial (RCT) and long-term follow-up (LTFU) study.
There was no evidence to support differences between groups in the primary outcome measure of PRWE. There was no evidence of a difference in health-related quality of life, other than some weak evidence in favour of wire fixation at five years; this difference was of borderline statistical significance (p = 0.055) and the difference was below the level of clinical significance prespecified in the DRAFFT trial.
Longitudinal analysis of the PRWE scores showed that treatment (LRT p = 0.550), age group (LRT p = 0.856), and intra-articular extension (LRT p = 0.449) did not exert a significant effect on outcome. However, year of follow-up (LRT p < 0.001) and sex (LRT p = 0.009) were significant. That is, participant wrist function continued to improve during the follow-up period (PRWE scores became lower) and men had better wrist function than women. Participants with poor function in the first 12 months after their injury tended to improve more during long-term follow-up than those participants with initially better function.
Longitudinal analysis of the EQ-5D scores showed that treatment (LRT p = 0.470), year of follow-up (LRT p = 0.429), sex (LRT p = 0.067), and intra-articular extension (LRT; p = 0.930) were not significant. However, age (LRT p = 0.023) was marginally significant, with health-related quality of life being lower in the over 50-year age group than in the under 50-year age group, although the model estimate of -0.05 (95% confidence interval -0.09 to -0.01) indicated that the difference was unlikely to be clinically important.
In terms of further surgery, only three participants reported having additional surgery in years two to five. In year two, one patient in the wire group reported having an ulna shortening osteotomy for restricted wrist movement. In the plate group, there was one late tendon rupture four years after the index fracture, and one other patient reported having further surgery to remove a retained suture following a previous repair of a tendon rupture that occurred in the first year after the fracture.
Discussion
This five-year follow-up study showed no evidence of a difference in wrist pain or function as indicated by the PRWE between patients randomized to K-wire fixation and those randomized to locking-plate fixation for a dorsally displaced fracture of the distal radius. Secondary analyses showed no evidence of a difference in health-related quality of life in years two, three, and four. There was weak evidence of a difference in quality of life at five years in favour of wire fixation, although the absolute difference was small and less than the prespecified clinically important difference in the DRAFFT trial. In general, patients recover well after this injury, with good wrist function and quality of life even after a wrist fracture that requires surgical fixation.
One of the concerns raised by clinicians when the DRAFFT trial was published was that patients may develop post-traumatic arthritis in the wrist joint, leading to reduced function in the longer term and further surgery, including extensive salvage operations such as wrist fusion. Although there is now strong evidence that radiological parameters do not correlate with functional outcome in the short term,10 the worry was that problems related to arthritis may not manifest until after the 12-month follow-up period of the first trial report. Furthermore, since wire fixation has previously been associated with worse radiological outcomes than locking-plate fixation,11 the rate of wrist arthritis and the need for salvage surgery may be greater in the group treated with wire fixation. This study, however, found that further surgery was very uncommon, with only three operations between years two and five, albeit with lower rates of follow-up as the study progressed.
Other findings of note were that PRWE scores declined during follow-up, meaning that function continued to improve from years one to five, albeit more slowly than in the first year after their injury. This is reassuring information and should be helpful to clinicians when counselling patients with regard to the longer-term outcome of their injury. Despite the continued improvement in wrist function, there was no significant change in health-related quality of life scores during the follow-up period.
The major limitation of this study is the loss to follow-up during the five years after participants agreed to take part in the DRAFFT trial. Other large-scale randomized trials in orthopaedic trauma have reported higher rates of follow-up, albeit in different populations of patients.12,13 The sponsor of the study required that patients reconsent to take part in the longer-term follow-up of the trial. This, along with the fact that many patients had returned to near normal function at the end of the 12-month follow-up period, led to some patients declining to take part in the longer-term follow-up. This was particularly the case for younger patients; response rates were lower for those participants aged under 50 years than for those participants aged over 50 years. However, there was no evidence to support differences in response rates between treatment groups. Therefore, although the loss to follow-up does limit the external validity of the study, we can be reasonably confident when making comparisons between treatment groups.
In conclusion, and contrary to concerns raised after the DRAFFT trial, this study shows no evidence of a difference in wrist function or quality of life at five years for patients randomized to wire fixation versus locking-plate fixation for a dorsally displaced fracture of the distal radius. Patients may be reassured that their wrist function is likely to continue to improve in the five years following their injury.
Take home message
- Patients may be reassured that their wrist function is likely to continue to improve in the five years following their injury.
- Most patients can expect very good function with little pain from their wrist, albeit not quite back to their preinjury level.
- There is no evidence of a difference in outcome for patients treated with wire fixation versus locking plate fixation.
Author contributions
M. L. Costa: Responsible for concept and design, Acquired, analyzed, and interpreted the data, Wrote and revised the manuscript, Obtained funding, Offered administrative, technical, or material support, Had full access to all of the data in the study, Took responsibility for the integrity of the data and the accuracy of the data analysis.
J. Achten: Responsible for concept and design, Acquired, analyzed, or interpreted the data, Wrote and revised the manuscript, Obtained funding, Offered administrative, technical, or material support.
A. Rangan: Concept and design, Acquired, analyzed, or interpreted the data, Revised the manuscript, Obtained funding.
S. E. Lamb: Responsible for concept and design, Acquired, analyzed, or interpreted the data, Revised the manuscript, Obtained funding.
N. R. Parsons: Responsible for concept and design, Acquired, analyzed, and interpreted the data, Wrote and revised the manuscript, Statistical analysis, Had full access to all of the data in the study, Took responsibility for the integrity of the data and the accuracy of the data analysis.
Funding statement
This project was funded by the NIHR HTA Programme (project number 08/116/97 & 15/143/02) and was supported by the NIHR Oxford Biomedical Research Centre and the NIHR Collaboration for Leadership in Applied Health Research and Care Oxford at Oxford Health National Health Service (NHS) Foundation Trust (Dr Lamb).
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The views expressed in this article are those of the authors and not necessarily those of the NHS, the National Institute for Health Research (NIHR), or the United Kingdom Department of Health.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Acknowledgements
We would like to thank all the participants of the Distal Radius Acute Fracture Fixation Trial (DRAFFT) for their continued support throughout the five-year follow-up period. Further thanks go to the administrative DRAFFT team at the University of Warwick who was instrumental in the collection of the data.
Ethical review statement
Ethical approval for this study was given by the Coventry and Warwickshire NHS Research Ethics Committee on the 24 April 2010 under reference number 10/H1210/10.
Open access statement
This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC BY-NC), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
Trial registration number
Current Controlled Trials ISCRTN 31379280. UKCRN 8956.
This article was primary edited by A. D. Liddle.
References
- 1.Costa ML, Achten J, Parsons NR, et al. . Percutaneous fixation with Kirschner wires versus volar locking plate fixation in adults with dorsally displaced fracture of distal radius: randomised controlled trial. BMJ 2014;349:g4807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Costa ML, Achten J, Plant C, et al. . UK DRAFFT: a randomised controlled trial of percutaneous fixation with Kirschner wires versus volar locking-plate fixation in the treatment of adult patients with a dorsally displaced fracture of the distal radius. Health Technol Assess 2015;19:1–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tubeuf S, Yu G, Achten J, et al. . Cost effectiveness of treatment with percutaneous Kirschner wires versus volar locking plate for adult patients with a dorsally displaced fracture of the distal radius: analysis from the DRAFFT trial. Bone Joint J 2015;97-B:1082–1089. [DOI] [PubMed] [Google Scholar]
- 4.Costa ML, Jameson SS, Reed MR. Do large pragmatic randomised trials change clinical practice?: assessing the impact of the distal radius acute fracture fixation trial (DRAFFT). Bone Joint J 2016;98-B:410–413. [DOI] [PubMed] [Google Scholar]
- 5.Fullilove S, Gozzard C. Dorsally displaced fractures of the distal radius: a critical appraisal of the DRAFFT (distal radius acute fracture fixation trial) study. Bone Joint J 2016;98-B:298–300. [DOI] [PubMed] [Google Scholar]
- 6.MacDermid JC, Turgeon T, Richards RS, Beadle M, Roth JH. Patient rating of wrist pain and disability: a reliable and valid measurement tool. J Orthop Trauma 1998;12:577–586. [DOI] [PubMed] [Google Scholar]
- 7.Dolan P. Modeling valuations for EuroQol health states. Med Care 1997;35:1095–1108. [DOI] [PubMed] [Google Scholar]
- 8.Brooks R. EuroQol: the current state of play. Health Policy 1996;37:53–72. [DOI] [PubMed] [Google Scholar]
- 9.Bates D, Maechler M, Bolker B, et al. . Fitting linear mixed-effects models using lme4. J Stat Softw 2015;67:1–48. [Google Scholar]
- 10.Plant CE, Parsons NR, Edwards AT, et al. . A comparison of electronic and manual dynamometry and goniometry in patients with fracture of the distal radius and healthy participants. J Hand Ther 2016;29:73–80. [DOI] [PubMed] [Google Scholar]
- 11.McFadyen I, Field J, McCann P, et al. . Should unstable extra-articular distal radial fractures be treated with fixed-angle volar-locked plates or percutaneous Kirschner wires? A prospective randomised controlled trial. Injury 2011;42:162–166. [DOI] [PubMed] [Google Scholar]
- 12.Handoll HH, Keding A, Corbacho B, et al. . Five-year follow-up results of the PROFHER trial comparing operative and non-operative treatment of adults with a displaced fracture of the proximal humerus. Bone Joint J 2017;99-B:383–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Keene DJ, Lamb SE, Mistry D, et al. . Three-year follow-up of a trial of close contact casting vs surgery for initial treatment of unstable ankle fractures in older adults. JAMA 2018;319:1274–1276. [DOI] [PMC free article] [PubMed] [Google Scholar]