

Abstract
Background
In 2013, the Society of Critical Care Medicine published a revised version of the ICU Pain, Agitation, and Delirium (PAD) guidelines. Immobility and sleep were subsequently added in 2018. Despite the well-established advantages of implementing these guidelines, adoption and adherence remain suboptimal. This is especially true in community settings, where PAD assessment is performed less often, and the implementation of PAD guidelines has not yet been studied. The purpose of this prospective interventional study is to evaluate the effect of a multifaceted nurse engagement intervention on PAD assessment in a community intensive care unit (ICU).
Methods
All patients admitted to our community ICU for over 24 hours were included. A 20-week baseline audit was performed, followed by the intervention, and a 20-week postintervention audit. The intervention consisted of a survey, focus groups and education sessions. Primary outcomes included rates of daily PAD assessment using validated tools.
Results
There were improvements in the number of patients with at least one assessment per day of pain (67.5% vs 59.3%, p=0.04), agitation (93.1% vs 78.7%, p<0.001) and delirium (54.2% vs 39.4%, p<0.001), and the number of patients with target Richmond Agitation-Sedation Scale ordered (63.1% vs 46.8%, p=0.002). There was a decrease in the rate of physical restraint use (10.0% vs 30.9%, p<0.001) and no change in self-extubation rate (0.9% vs 2.5%, p=0.2).
Conclusion
The implementation of a multifaceted nurse engagement intervention has the potential to improve rates of PAD assessment in community ICUs. Screening rates in our ICU remain suboptimal despite these improvements. We plan to implement multidisciplinary interventions targeting physicians, nurses and families to close the observed care gap.
Keywords: critical care, healthcare quality improvement, nurses, performance measures, quality improvement
Background
Pain is one of the most stressful events experienced by patients during their intensive care unit (ICU) stay.1 2 Its deleterious physical and psychological effects have been described in depth in the literature.1 3–5 Pain is closely linked to agitation and delirium, and all of these are commonly underdiagnosed in the ICU, leading to a number of adverse outcomes.6–9 Despite the widespread availability of validated tools for pain, agitation and delirium (PAD) screening, these assessments are often not done.
The care gap in the assessment and treatment of PAD in the ICU has been well studied, and protocols have been developed to facilitate the transfer of evidence-based practices to the bedside.1 In 2013, the Society of Critical Care Medicine published a revised version of the ICU Pain, Agitation, and Delirium guidelines. These guidelines packaged together individual elements that have consistently been shown to improve both short-term and long-term ICU outcomes and reduce costs of care.1 10–12 In 2018, immobility and sleep were added to form the newer Pain, Agitation/Sedation, Delirium, Immobility, and Sleep (PADIS) guidelines.13
The advantages of applying the PAD guidelines are well established, yet adoption and adherence remain suboptimal.14–16 This is especially true in community hospitals, where monitoring and use of validated scoring systems are less frequent than in university-affiliated hospitals.17 18 Educational interventions have been shown to address barriers to guideline implementation and are recommended as a strategy to facilitate PAD guideline implementation in the ICU.1 19 Education is also crucial for ensuring sustained improvements within the healthcare environment.20 21
The purpose of this prospective interventional study was to evaluate the impact of a multifaceted nurse engagement intervention on PAD assessment in a community ICU. Nurses are positioned to play a significant role in quality improvement initiatives as they are on the frontlines of assessing and treating PAD.21 22 This nurse-focused intervention consists of both an educational component, based on the 2013 PAD guidelines, and engagement components designed to elicit nurses’ perspectives and increase participation. To the best of our knowledge, this is the first study to evaluate the implementation of PAD guidelines in a community setting.
Methods
This study was reported based on the Revised Standards for QUality Improvement Reporting Excellence guidelines.23
Context
The study was conducted in a level 3 community medical–surgical ICU with 14 beds. It is serviced by 10 intensivists, with 1 intensivist during the day (07:30–17:30) and 1 overnight (17:30–07:30). The nurse-to-patient ratio ranges from 1:1 to 1:2 and there is also a dedicated ICU interprofessional team, including respiratory therapists, physiotherapists, and a pharmacist and dietitian. The team provides care to general medical, cardiology, respiratory, nephrology, oncology, general surgical, orthopaedic and vascular surgical patients. All patients admitted to the ICU for over 24 hours were included in the study. There were no exclusion criteria, as PAD guidelines can be applied universally to all patients in the ICU.
Intervention
The nurse engagement intervention consisted of three components: (1) a nurse survey, (2) nurse focus groups and (3) nurse education sessions. The nurse survey was anonymous and aimed to assess nurses’ perceived comfort, knowledge and satisfaction surrounding PAD management in the ICU. It was administered in three different forms—paper survey, fillable PDF form and online survey—to improve response rate. The information gathered in this survey guided the development of the focus groups.
The goals of the nurse focus groups were to (1) understand the barriers to optimal PAD assessment and treatment in the ICU from the nurses’ perspectives, (2) gather information for the development of subsequent nurse education sessions and (3) engage nurses in the PAD initiative to increase buy-in. Facilitators were provided with a semi-structured interview guide with six open-ended questions (see online supplementary appendix A) to guide the discussion. The guide was developed based on the results of the nurse survey by a committee consisting of an intensivist, an associate professor with expertise in quality improvement and safety culture, a research coordinator and an ICU pharmacist. A total of five 1-hour focus group sessions were conducted over 2 weeks, with participants split into 1–3 smaller groups of 4–7 nurses to encourage individual contribution.
bmjoq-2018-000421supp001.pdf (20.2KB, pdf)
Nurse education sessions were then developed using the information collected from the focus groups and survey. The goal of these sessions was to increase nurses’ knowledge on the (1) screening and treatment of PAD, (2) advantages and disadvantages of certain medications that are commonly used in the ICU, (3) deleterious effects of delirium on patient outcomes and (4) benefit of using non-pharmacological approaches in managing PAD. Topics covered included the 2013 guidelines with a focus on core aspects of practice change; delirium; basic pharmacology of analgesics, sedatives and antipsychotics; and non-pharmacological strategies in PAD management. Videos of ICU survivors giving testimonials on their experience in the ICU from the perspective of PAD were included to increase buy-in. These videos detailed the physically and emotionally scarring experience that one patient had with delirium, and another with oversedation. There was, also, a video that highlighted the significant positive influence that nurses can have and how patients may remember this many years later. A total of five 1.5-hour education sessions were conducted over 4 weeks, with approximately nine nurses per session.
Study of the intervention
A 20-week baseline audit was performed during the second quarter of 2016, followed by implementation of the nurse engagement intervention for 44 weeks, and a 20-week postintervention audit during the third quarter of 2017. Prospective data collection, including demographics, process of care and patient outcomes, was performed for both audits. Findings from the survey and focus groups are described in a separate paper.
Measures
To evaluate changes in daily PAD assessment, the following process measures were examined as the outcomes of this study: rate of pain assessment using the Numeric Pain Rating Scale (NRS), rate of agitation assessment using the Richmond Agitation-Sedation Scale (RASS), rate of delirium assessment using the Confusion Assessment Method for the ICU (CAM-ICU) and rate of target RASS ordered by intensivists. All of these have been widely studied and determined to be among the most valid and reliable screening tools, and are recommended in the 2013 guidelines. Self-extubation and physical restraint use were examined as balancing measures as they are known complications of inappropriate levels of sedation.
Analysis
Weekly rates expressed in patient percentage were presented on run charts (figure 1). A preintervention and postintervention analysis was performed using a two-sample Student’s t-test, with p<0.05 indicating significance.
Figure 1.
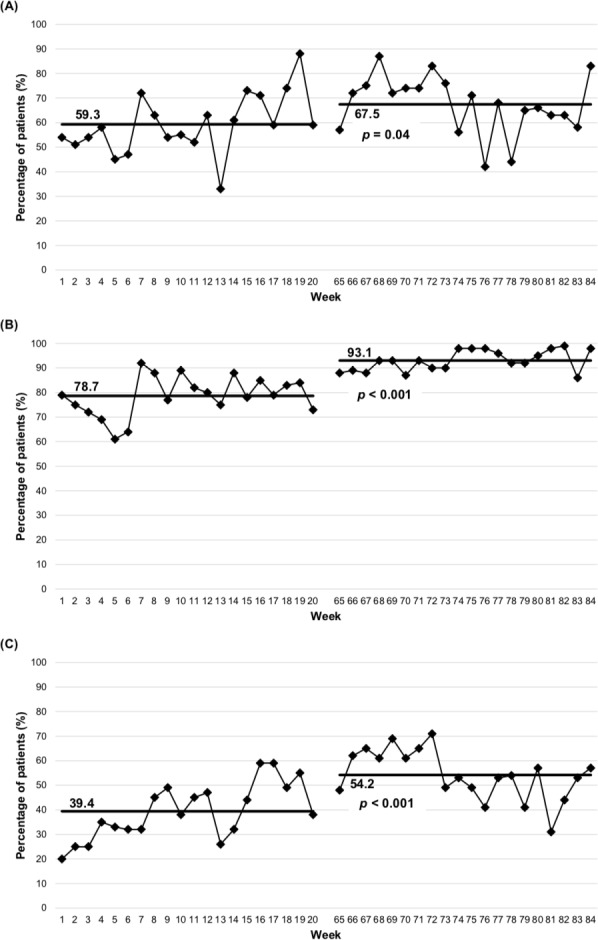
Mean percentage of patients with at least one assessment per day of pain (A), agitation (B) and delirium (C) preintervention and postintervention.
Ethical considerations
The focus groups and education sessions were funded by the Ontario Nurses’ Association so that nurses could be reimbursed for their time.
Results
Nurse engagement intervention improved PAD assessment rate
The nurse survey, focus groups and education sessions together resulted in significant improvements in the number of patients with at least one pain, agitation or delirium assessment per day (figure 2). The rate of pain assessment using NRS was 59.3%±12.2% preintervention and 67.5%±11.9% postintervention (p=0.04). The rate of agitation assessment using RASS was 78.7%±8.2% preintervention and 93.1%±4.3% postintervention (p<0.001). Lastly, the rate of delirium assessment using CAM-ICU was 39.4%±11.6% preintervention and 54.2%±10.2% postintervention (p<0.001). However, the assessment rates were still suboptimal, with large care gaps persisting postintervention.
Figure 2.

Mean percentage of patients with at least one assessment per day of pain, agitation and delirium preintervention and postintervention.
Nurse engagement intervention improved intensivist process metric
As recommended by the 2013 PAD guidelines, intensivists should order target RASS scores to facilitate goal-directed sedation. In this study, we showed that the nurse engagement intervention also influenced intensivists’ behaviour, reflected by an improvement in the rate of target RASS score ordered by intensivists (figure 3). The rate of target RASS scores being ordered by intensivists was 46.8%±15.6% preintervention and 63.1%±15.8% postintervention (p=0.002).
Figure 3.
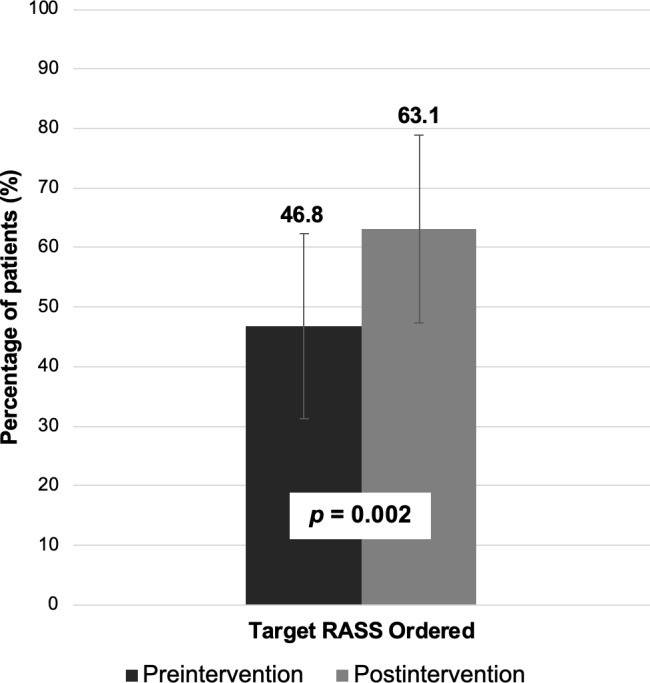
Mean percentage of patients with target RASS ordered preintervention and postintervention. RASS, Richmond Agitation-Sedation Scale.
Nurse engagement intervention did not increase adverse outcomes
It has been shown that by decreasing sedation in the ICU, there is a potential risk of increasing the rate of physical restraint use or inadvertent extubation by patients due to agitation. The nurse engagement intervention was not associated with increased rates of physical restraint use or inadvertent extubation by patients (figure 4). The rate of physical restraint use was 30.9%±15.9% preintervention and 10.0%±7.2% postintervention (p<0.001). The rate of inadvertent extubation by patients was 2.5%±5.2% preintervention and 0.9%±1.9% postintervention (p=0.2).
Figure 4.

Mean percentage of patients on whom physical restraints were used and who self-extubated preintervention and postintervention.
Discussion
Summary and interpretation
The assessment and treatment of PAD in the ICU represents a large care gap that is difficult to close. Protocols have been developed to facilitate the transfer of evidence-based practices to the bedside, and this study was the first to evaluate the implementation of PAD guidelines in a community setting. The nurse survey was a means through which nurses could share their opinions and become involved in the study early on. The subsequent focus groups provided the opportunity to further explore nurses’ perspectives on PAD assessment and treatment and for nurses to contribute to the design of the education sessions. Together, the nurse survey and focus groups facilitated earlier, multilevel and more widespread engagement.
Information gathered from the nurse survey and focus groups suggested that the largest care gap existed in assessing and treating delirium, and that communication about PAD is lacking among members of the healthcare team.24 25 These findings led to the creation of nurse education sessions on PAD assessment, treatment and prevention, with a focus on delirium. The majority of full-time ICU nurses participated in the three parts of this multifaceted nurse engagement intervention, which was associated with significantly improved rates of daily PAD assessment using valid and reliable scoring tools. This is consistent with previous studies those described the importance of educational interventions for nurses in healthcare quality improvement initiatives.21 26
The postintervention improvements in screening rates may have been the result of increased comfort with PAD assessment, which was identified as a care gap in an earlier part of this study.24 Other potential contributors include increased awareness of the importance of evaluating for PAD and clarification of misconceptions surrounding screening tools, both of which have been identified as barriers to optimal PAD assessment.26 The positive changes in screening rates did not appear to be associated with adverse effects on PAD management, as there was no change in the rate of inadvertent extubation by patients, and was actually a significant decrease in the rate of physical restraint use.
There was also a significant improvement in the rate of target RASS being ordered by intensivists. This may have occurred because more nurses started asking for target RASS scores when they were not ordered, either secondary to increased awareness of the importance of PAD assessment or increased comfort discussing PAD assessment. Alternatively, it may have been the result of intensivists being more aware that this project was being conducted during the postintervention phase.
Despite these improvements, daily screening rates in our ICU remain low at 67.5%, 93.1% and 54.2% for pain, agitation and delirium, respectively. This is particularly important for pain, because even with various effective treatments available, the majority of patients recall having moderate-to-severe pain in the ICU.27 Furthermore, pain is one of the most stressful events for patients during their ICU stay and is associated with significant long-term negative physiological and psychological consequences.1 2
In addition to the concern of undertreatment, there is also the concern of low PAD screening rates contributing to overtreatment. Payen et al found that the observed rates of assessment for sedation (43%) and analgesia (42%) in the ICU were significantly lower than the use of sedatives (72%) and opioids (90%).19 The discrepancy is concerning because sedatives and opioids are not benign, and the adverse effects associated with their use have been well described.13 19 Regular, standardised assessments are needed to allow for a better match between analgesic and sedative requirements and administration.2 8
Previous studies have identified significant knowledge gaps when it comes to PAD assessment and treatment.24 26 28 Educational interventions have an important role in closing these gaps and are recommended as a strategy to facilitate PAD guideline implementation in the ICU.1 19 That being said, educational interventions appear to be necessary but not sufficient to advance PAD assessment. This has been proposed by earlier studies and may help to explain the persistently suboptimal screening rates postintervention in our study.27 28
In addition to knowledge deficits, Glynn and Ahern27 found that personal beliefs and the influence of peers are strong determinants of nurses’ pain management behaviour in the ICU. Nurses are strongly committed to pain relief, yet they often fail to accurately document pain and they continue to underestimate and undertreat their patients’ pain. An example of a harmful but commonly held belief is that ‘those who do not evidence overt signs of pain are not experiencing pain that requires treatment’. To the dismay of patients and their families, nurses also tend to believe that patients often overstate their pain.28 The 2018 PADIS guidelines were the first to include patients as collaborators and co-authors.13 Direct involvement of patients and their families may be an important first step to addressing these harmful beliefs that pose a barrier to improving PAD assessment and treatment.
As suggested by Glynn and Ahern, and many others, advancing PAD assessment should be an interdisciplinary endeavour.1 27 Studies have found that senior nurses and other healthcare team members influence the importance that nurses place on pain assessment and treatment as well as the improvements they make in the long-term. With these findings in mind, future quality improvement initiatives should consider focusing on belief-altering interventions and multidisciplinary involvement.
Limitations
Limitations of this study include the fact that rates of PAD assessment completion were recorded without consideration of assessment accuracy. An earlier study by Devlin et al evaluated the impact of an educational intervention on correct use of the Intensive Care Delirium Screening Checklist (ICDSC), another delirium screening tool recommended in the 2013 PAD guidelines.1 26 They found that education increased the number of nurses who correctly used the ICDSC from 8% to 62%. While this suggests that educational interventions are also associated with more accurate delirium screening, future quality improvement initiatives should consider including assessment accuracy as an outcome measure.
Conclusions
The implementation of a multifaceted nurse engagement intervention has the potential to improve rates of PAD assessment in the community ICU setting. Even with the improvements made during this study, PAD assessment frequency in the community ICU remains suboptimal according to the 2013 guidelines. This points towards the importance of multidisciplinary interventions for both nurses and other members of the healthcare team. The next phase of this study will involve additional interventions targeting physicians, nurses and family members. Caring for ICU patients is a team effort, and further quality improvement initiatives are necessary to close the care gap and better patient outcomes in community ICUs.
Footnotes
Presented at: This work was presented at ESICM LIVES 2018.
Contributors: CMT completed the data analysis and wrote this manuscript. MC acquired and analysed the data. FM contributed to the data analysis and implementation of the interventions. KR, GF and ML contributed to the conception and design of this study and implementation of the interventions. RM contributed to the data analysis. PY and CM contributed to the implementation of the interventions. JLYT contributed to the conception and design of this study, implementation of the interventions, and writing and revision of this manuscript.
Funding: This work was supported by the Ontario Nurses’ Association and the McMaster University, Department of Medicine, E.J. Moran Campbell Internal Research Career Award 2015–2018 (JLYT).
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: Local research ethics committee approval was obtained for this study.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Barr J, Fraser GL, Puntillo K, et al. . Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013;41:263–306. 10.1097/CCM.0b013e3182783b72 [DOI] [PubMed] [Google Scholar]
- 2. Chanques G, Pohlman A, Kress JP, et al. . Psychometric comparison of three behavioural scales for the assessment of pain in critically ill patients unable to self-report. Crit Care 2014;18 10.1186/cc14000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Novaes MA, Aronovich A, Ferraz MB, et al. . Stressors in ICU: patients' evaluation. Intensive Care Med 1997;23:1282–5. 10.1007/s001340050500 [DOI] [PubMed] [Google Scholar]
- 4. Puntillo KA, Max A, Timsit J-F, et al. . Determinants of procedural pain intensity in the intensive care unit. The Europain® study. Am J Respir Crit Care Med 2014;189:39–47. 10.1164/rccm.201306-1174OC [DOI] [PubMed] [Google Scholar]
- 5. Rotondi AJ, Chelluri L, Sirio C, et al. . Patients' recollections of stressful experiences while receiving prolonged mechanical ventilation in an intensive care unit. Crit Care Med 2002;30:746–52. 10.1097/00003246-200204000-00004 [DOI] [PubMed] [Google Scholar]
- 6. Chanques G, Jaber S, Barbotte E, et al. . Impact of systematic evaluation of pain and agitation in an intensive care unit. Crit Care Med 2006;34:1691–9. 10.1097/01.CCM.0000218416.62457.56 [DOI] [PubMed] [Google Scholar]
- 7. Dunwoody CJ, Krenzischek DA, Pasero C, et al. . Assessment, physiological monitoring, and consequences of inadequately treated acute pain. J Perianesth Nurs 2008;23(1 Suppl):S15–S27. 10.1016/j.jopan.2007.11.007 [DOI] [PubMed] [Google Scholar]
- 8. Georgiou E, Hadjibalassi M, Lambrinou E, et al. . The impact of pain assessment on critically ill patients' outcomes: a systematic review. Biomed Res Int 2015;2015:1–18. 10.1155/2015/503830 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Vasilevskis EE, Ely EW, Speroff T, et al. . Reducing iatrogenic risks: ICU-acquired delirium and weakness--crossing the quality chasm. Chest 2010;138:1224–33. 10.1378/chest.10-0466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Barnes-Daly MA, Phillips G, Ely EW. Improving Hospital survival and reducing brain dysfunction at seven California community hospitals: implementing pad guidelines via the ABCDEF bundle in 6,064 patients. Crit Care Med 2017;45:171–8. 10.1097/CCM.0000000000002149 [DOI] [PubMed] [Google Scholar]
- 11. Ely EW. The ABCDEF bundle: science and philosophy of how ICU liberation serves patients and families. Crit Care Med 2017;45:321–30. 10.1097/CCM.0000000000002175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kram SL, DiBartolo MC, Hinderer K, et al. . Implementation of the ABCDE bundle to improve patient outcomes in the intensive care unit in a rural community hospital. Dimens Crit Care Nurs 2015;34:250–8. 10.1097/DCC.0000000000000129 [DOI] [PubMed] [Google Scholar]
- 13. Devlin JW, Skrobik Y, Gélinas C, et al. . Clinical practice guidelines for the prevention and management of pain, Agitation/Sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med 2018;46:e825–73. 10.1097/CCM.0000000000003299 [DOI] [PubMed] [Google Scholar]
- 14. Mehta S, McCullagh I, Burry L. Current sedation practices: lessons learned from international surveys. Crit Care Clin 2009;25:471–88. 10.1016/j.ccc.2009.04.001 [DOI] [PubMed] [Google Scholar]
- 15. Tanios MA, de Wit M, Epstein SK, et al. . Perceived barriers to the use of sedation protocols and daily sedation interruption: a multidisciplinary survey. J Crit Care 2009;24:66–73. 10.1016/j.jcrc.2008.03.037 [DOI] [PubMed] [Google Scholar]
- 16. Boehm LM, Dietrich MS, Vasilevskis EE, et al. . Perceptions of workload burden and adherence to ABCDE bundle among intensive care providers. Am J Crit Care 2017;26:e38–47. 10.4037/ajcc2017544 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Luetz A, Balzer F, Radtke FM, et al. . Delirium, sedation and analgesia in the intensive care unit: a multinational, two-part survey among intensivists. PLoS One 2014;9:e110935 10.1371/journal.pone.0110935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Van Eijk MMJ, Kesecioglu J, Slooter AJC. Intensive care delirium monitoring and standardised treatment: a complete survey of Dutch intensive care units. Intensive Crit Care Nurs 2008;24:218–21. 10.1016/j.iccn.2008.04.005 [DOI] [PubMed] [Google Scholar]
- 19. Payen J-F, Chanques G, Mantz J, et al. . Current practices in sedation and analgesia for mechanically ventilated critically ill patients: a prospective multicenter patient-based study. Anesthesiology 2007;106:687–95. 10.1097/01.anes.0000264747.09017.da [DOI] [PubMed] [Google Scholar]
- 20. Balas MC, Burke WJ, Gannon D, et al. . Implementing the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility bundle into everyday care: opportunities, challenges, and lessons learned for implementing the ICU pain, agitation, and delirium guidelines. Crit Care Med 2013;41(9 Suppl 1):S116–27. 10.1097/CCM.0b013e3182a17064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Albanese MP, Evans DA, Schantz CA, et al. . Engaging clinical nurses in quality and performance improvement activities. Nurs Adm Q 2010;34:226–45. 10.1097/NAQ.0b013e3181e702ca [DOI] [PubMed] [Google Scholar]
- 22. Needleman J, Hassmiller S. The role of nurses in improving Hospital quality and efficiency: real-world results. Health Aff 2009;28(Supplement 3):w625–33. 10.1377/hlthaff.28.4.w625 [DOI] [PubMed] [Google Scholar]
- 23. Ogrinc G, Davies L, Goodman D, et al. . Squire 2.0 (standards for quality improvement reporting excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf 2016;25:986–92. 10.1136/bmjqs-2015-004411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Maximous R, Miller F, Tan C, et al. . Pain, agitation and delirium assessment and management in a community medical-surgical ICU: results from a prospective observational study and nurse survey. BMJ Open Qual 2018;7:e000413 10.1136/bmjoq-2018-000413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Tsang JLY, Ross K, Miller F, et al. . Qualitative descriptive study to explore nurses' perceptions and experience on pain, agitation and delirium management in a community intensive care unit. BMJ Open. In Press 2019;9:e024328 10.1136/bmjopen-2018-024328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Devlin JW, Marquis F, Riker RR, et al. . Combined didactic and scenario-based education improves the ability of intensive care unit staff to recognize delirium at the bedside. Crit Care 2008;12 10.1186/cc6793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Glynn G, Ahern M. Determinants of critical care nurses' pain management behaviour. Aust Crit Care 2000;13:144–51. 10.1016/S1036-7314(00)70642-4 [DOI] [PubMed] [Google Scholar]
- 28. Watt-Watson J, Stevens B, Garfinkel P, et al. . Relationship between nurses' pain knowledge and pain management outcomes for their postoperative cardiac patients. J Adv Nurs 2001;36:535–45. 10.1046/j.1365-2648.2001.02006.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjoq-2018-000421supp001.pdf (20.2KB, pdf)