

Abstract
Purpose
To systematically review, summarise and evaluate the evidence on the effectiveness of automation systems in the outpatient and community settings.
Methods
A literature search was performed using PubMed, Embase, Cochrane Library and CINAHL databases. A pre-defined search strategy focusing on the context of implementation, function and automation was used to identify articles published over the past decade. Two researchers independently screened the search results sequentially by title, abstract and full text using pre-defined inclusion/exclusion criteria. A third researcher was consulted to resolve disagreements. Data extraction and quality assessment were performed using a standardised form.
Results
Thirteen references were selected for data extraction, of which most were conducted in Europe and North America. Improvement in medication safety was most commonly reported, with findings of up to 37% reduction in medication-related reportable occurrences. Manpower requirements were found to decrease by 0.3–1.4 full-time equivalents and productivity increased by ~4 items per person/hour. Patient waiting time and prescription filling time also decreased by 17–20 s (from an average of 19–49 s), but no reductions in workload or time savings were felt by staff. While the perception of work stress decreased, job satisfaction remained unchanged. Significant cost savings and an increase in over-the-counter sales were also noted post-automation.
Conclusion
Implementing pharmacy automation technologies in an outpatient or community pharmacy setting may reduce medication errors, increase productivity and save costs but does not affect staff satisfaction. However, the available literature remains patchy and more research in this area is needed.
Keywords: hospital pharmacy automation, robots, dispensing robots, compounding robots, uni dose system
Background
Countries globally have been struggling to keep up with increasing healthcare needs due to ageing populations and the shrinking dependency ratio.1–5 Along with the rising prevalence of chronic diseases and increasing complexity of pharmaceutical care, there is a shift in the role of pharmacists towards knowledge-based optimisation and management of pharmaceutical therapies, while delegating traditional dispensing and supply functions to robotics and automation.6 7 Besides tangible manpower savings, studies have also demonstrated intangible benefits in pharmacists’ job satisfaction when they spend more time performing value-added patient care activities such as therapeutic drug monitoring and clinical consultations.8 9
Aimed at improving operational efficiency, pharmacy automation technology originated decades ago with relatively simple functions like tablet counting, barcode reading and labelling.10 Today, there is a plethora of automated solutions available in the market with a wide spectrum of functions that reduce prescription filling time and also improve medication safety.11
As automation technology matured, more pharmacies worldwide began implementing automation in their medication supply and distribution processes.12–15 In Singapore, pharmacy automation was deployed at a tertiary academic hospital in 2013, a RFID-assisted manual drug-picking system with enhanced safety and manpower reduction.16 17 This was quickly followed by similar implementations in three other public hospitals and a chain of polyclinics. Further expansions to other public institutions island-wide are currently being planned.16
With the increasingly widespread use of automation, it is important for us to evaluate if these systems are truly able to deliver their marketed claims such as improving productivity and reducing medication errors, given our complex healthcare needs and high degree of prescription customisation. While inpatient pharmacy automation solutions—especially unit dose packaging and automated dispensing cabinets—have been relatively well studied,13–15 18–20 outpatient solutions have not received similar research attention. A systematic review21 conducted in 2013 on an Automated Dose Dispensing Service for primary healthcare patients demonstrated improved accuracy of medication administration and appropriateness of medication use. It provided some secondary evidence that robotics may be used to provide unit dose packaging for medications dispensed in primary care. However, none of the included studies evaluated the impact of automation on pharmacy processes and workflows. Thus, it is still unclear how significant are the potential benefits in medication safety and productivity that automation may bring to pharmacies’ operations.
The aim of this study is to systematically review and summarise the different types of outpatient pharmacy automation systems and to evaluate the evidence of the effectiveness of these systems on improving medication safety, workflow productivity, healthcare professionals' perceptions and patient satisfaction. Through this we hope to help inform future decision-making on automating outpatient pharmacy processes in healthcare institutions worldwide.
Methods
Literature search and screening processes
A literature search was performed in August 2016 using PubMed, Embase, Cochrane Library and CINAHL databases. The search strategy was limited to articles published over the past 10 years, focusing on keywords related to the setting of implementation, functions and automation (see online supplementary appendix A). Key search terms included: medication, medicament, dose, dosage, drug, pharmacy, pharmacist, pharmaceutical, prescription, inventory, stock, pick, pack, label, dispense, distribute, electronic, robotic, automate. Together with the free-text searches, relevant medical subject headings in the thesauruses of the respective databases were also used (see online supplementary appendix A).
ejhpharm-2017-001424supp001.pdf (173.3KB, pdf)
Search hits were imported into a Citation Manager (Endnote X7; Thomson Reuters, New York, USA) and sequentially screened, first by title, then by abstract and finally full text. Articles were screened by two independent reviewers and a consensus was sought for any discrepancy through discussions at the end of each screening. A third reviewer was consulted when there were unresolved contradicting opinions between the initial reviewers. Candidate articles were accepted based on the following criteria: (1) studies reporting any impact or outcome related to the implementation of an automated dispensing machine (ADM); (2) studies conducted in a hospital pharmacy, community pharmacy or ambulatory care setting; (3) studies of experimental, observational and qualitative designs; (4) studies published between 2006 and 2016. Articles were excluded if they were: (1) solutions based in inpatient wards, clinics or nursing homes; (2) commentaries, newsletters, guidelines and methodological papers; or (3) not reported in the English language. Finally, studies done in an outpatient pharmacy, community pharmacy or ambulatory care setting were selected for data extraction.
Data extraction and quality assessment
Reported information on study characteristics (country, design, site), study aim, target population, intervention, comparator, outcome, conclusion and recommendations were extracted to a table using a data extraction form. We analysed each study intervention and extracted the brand and model of the automation system as well as the stage(s) of dispensing process automated, if reported. A three-stage categorisation of the processes in a pharmacy dispensing workflow, from receiving a prescription and checking the script to patient contact, was devised to facilitate analysis of the interventions:
Transcribing: entering the prescription into the system
Prescription filling: picking, packing and labelling of medications
Dispensing/patient counselling: final patient contact
All of the articles were then evaluated for their methodological quality using the Newcastle–Ottawa Rating Scale (NOS).22
All data extraction and quality assessment were conducted independently by two reviewers and consensus was reached by discussion to prevent bias and inconsistency. Final decisions were made by consultation with the senior author for any unresolved discrepancies.
Data synthesis and analysis
Articles were grouped according to their study types and summarised in a table (see online supplementary appendix B). For each article the study objectives, context of implementation, study intervention and outcome measures were extracted and presented. The outcome measures were categorised into: (1) medication errors; (2) manpower/workload; (3) time savings; (4) cost savings; and (5) job satisfaction/staff perceptions, and the results under each category were subsequently quoted and presented in a narrative form.
Update search
An update search was performed in late March 2017 using the same search strategy on the four databases, limited to articles published between August 2016 and March 2017. Search hits were imported into a separate Endnote library and duplicates were removed by software. Additionally, the update search hits were compared with those from the original search and duplicates were excluded.
Unique references from the updated search were then screened (by title, abstract, then full-text) by a single author using the same methodology and inclusion/exclusion criteria as that of the original search.
Results
Included studies and study quality
A total of 16 505 relevant references were found, with 13 434 references remaining after software removal of duplicates. Of these, 369 references were included in the abstract screening phase and 69 were chosen for full-text article review. Thirteen articles were finally shortlisted for data extraction and quality assessment (figure 1), 11 of which were published papers and two were published conference abstracts. No additional articles were shortlisted in the update search.
Figure 1.
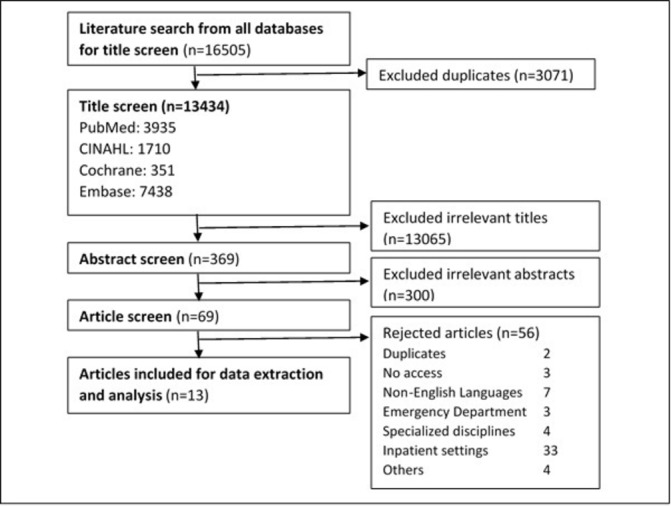
Process of article screening and number of shortlisted articles at each stage. No additional articles were shortlisted from the update search.
Seven of the 13 articles were case studies (including both conference papers), five were cross-sectional studies and one was an interventional study. There was originally a third conference abstract, the full article of which was obtained via correspondence with the lead author. It was then classified as a case study as part of the 11 journal articles. The studies were rated using NOS which showed that two studies were ‘Fair’, eight were ‘Good’ and three were of ‘Excellent’ quality (see online supplementary appendix B).
Twelve studies compared post-automation outcomes against manual dispensing (either pre-automation or against another pharmacy without automation). Of these, one study additionally compared the implementation of another ADM (Swisslog vs ROWA). The last study did not have any comparator or control.
Study demographics
Eight studies were conducted in Europe (five in the UK, two in Netherlands and one in Germany). Three other studies were carried out in North America (two in the USA and one in Canada), one study in Australia and one in Asia (Singapore). All articles were published between 2006 and 2014.
Four studies were conducted solely in community pharmacies, eight in a hospital and one in both community and hospital settings. Of the eight studies performed in a hospital setting, one focused specifically on an outpatient dispensary, five included analysis of both inpatient and outpatient dispensaries while the remaining two did not specify the pharmacy setting in which they were conducted.
Type of pharmacy automation and stages automated
Of the 13 studies, seven did not report the brand or model of the automation system implemented. The most reported ADM studied was the ROWA Speedcase (four studies), followed by ScriptPro Sp-200 (two studies) and Swisslog (one study), with one study comparing two systems. Of the remaining studies, two focused on unit dose dispensing while two provided no description on which the ADM was studied. Eight articles provided brief descriptions of the various automation functions.
Two studies involved the programmed automated transcription of physicians’ orders into the systems through an e-prescription system/electronic order scanning system (ie, transcribing process). Some of the automation reported also included additional functions such as medication distribution via a conveyor belt system or medication storage using a drug dispensing cabinet.
All the automation systems employed involved some degree of automation of the prescription filling process, while no studies included automating the patient dispensing/counselling process.
Outcome measures
Two articles reported qualitative measures of satisfaction level and perceptions among pharmacy staff. The remaining 11 articles reported quantitative outcome measures such as medication error rate, workload of staff/manpower, cost savings and time savings. The most common outcome measure reported was that of medication errors (primary outcome in five articles and secondary outcome in three articles), followed by workload/manpower savings, time savings and lastly cost savings. Two articles did not have any secondary outcomes while three articles included more than one secondary outcome, most commonly in the form of a qualitative measure of staff satisfaction or perceptions (tables 1 and 2).
Table 1.
Primary outcome measures reported
| Primary outcome measurements | No of studies | Details |
| Qualitative: satisfaction/perception | 2 | Staff experience of occupational stressors Staff perceptions of ADM |
| Quantitative: medication errors | 5 | Number and types of dispensing errors reported Stage at which the errors happened Number of errors prevented |
| Quantitative: workload/manpower | 3 | Items or prescriptions/person/ hour Full-time equivalents |
| Quantitative: time saving | 2 | Time spent on different part of the pharmacy workflow such as prescription filling/counselling/etc |
| Quantitative: cost saving | 1 | Savings in departmental and personnel costs Over-the-counter sales volume |
| Total | 13 |
Table 2.
Secondary outcome measures reported
| Secondary outcome measurements | No of studies | Details |
| Qualitative: satisfaction/perception | 1 | Staff perceptions of the impact of AMD on their life/work |
| Quantitative: medication errors | 3 | Immediate cause of medication error Number of dispensing incidents prevented |
| Quantitative: workload/manpower | 2 | Full-time equivalent needed before and after installation of ADM |
| Quantitative: time saving | 3 | Time spent on different parts of the pharmacy workflow Patient waiting time Time needed for stock taking/annual inventory |
| Quantitative: cost savings | 2 | Medication departmental cost savings Stock saving efficiency |
| Not specified | 2 | |
| Total | 13 |
Job satisfaction/perception
Pharmacy automation was generally concluded to reduce work stress and workload. The percentage of respondents who reported stress at work decreased by 21.8% post-automation (from 34.3% to 12.5%).23 24 It was also observed that ADM was able to provide a better work/life balance for staff as the percentage of respondents indicating that their work had adversely affected their private life decreased from 14% to 0% post-automation.23
However, two studies showed that automation did not have any impact on staff satisfaction with their job,23 25 while only one study found that pharmacy staff were more satisfied with their work after the implementation of Swisslog Pack Picker in their hospital.26 Generally, dispensary staff with experience in using the ADM had a more positive impression of automation systems.27
Medication errors
Medication errors were generally measured in terms of reduction in the rate of dispensing incidents prevented (ie, percentage of near misses or medication interventions made before the error reached the patient) or reduction of reportable medication-related occurrences (ie, number of medication errors that reached the patient). The number of medication errors made or prevented was used to indirectly measure the improvement in medication safety, as it is difficult to measure the number of correct medications dispensed to the patient given the large workload and general low rate of medication errors.
Our analysis showed that all studies reporting on medication errors observed an improvement in medication safety post-automation, with the rate of prevented dispensing incidents compared with manual dispensing24 25 28–30 reducing from 0.6–2.7% to 0–1.0% following ADM implementation and medication-related reportable occurrences decreasing by up to 37%.31
One study29 further categorised the various medication errors reported into labelling errors, drug errors, issue errors or a combination of these three errors, and noted no significant difference in the categories of error types reported pre- and post-automation. A separate study32 reported that most medication errors occur during the transcription process where prescriptions are entered into the system manually, while the most frequent immediate causes of medication errors were a change in the medication regimen, admission of patients to hospital, transfer of patients between wards or discharge.
Manpower/workload
Productivity changes were measured either in terms of the number of full-time equivalents (FTE), the change in workload or change in number of items processed per person per unit time.
Most studies showed an increase in productivity post-automation,30 with 0.3–1.4 less FTE compared with pre-automation28 33 (average of 6.5 FTE was required pre-automation in both studies) and mean workload increasing by approximately four items/person/ hour from 7.5 to 9.20 items/person/ hour to 11.7–13.17 items/person/hour.24 29 However, one study26 concluded that the modest increase in mean productivity (1.8 prescriptions per FTE) was not statistically significant and the pharmacists surveyed felt no difference in their workload or general responsibilities/duties between pre- and post-ADM implementation.
Time saving
Time saving was documented in terms of the time spent filling or packing the prescription, the total patient waiting time from prescription processing to receiving their medications, and the administrative time spent on stock taking or inventory counting.
Studies measuring time saved with ADM yielded varying results. Following the automation of the prescription filling process, studies25 34 have quantitatively suggested a reduction in time spent on filling of 17–20 s compared with manual dispensing (from an average of 19–49 s). However, the time saving was not found to be statistically significant in one study34 after accounting for non-productive time, while another study26 reported that the time saved on prescription filling was not felt by the pharmacy staff as they did not report spending less time filling medication orders.
In addition, although one study33 found that the total patient waiting time decreased post-ADM implementation, a separate study26 reported that the patient counselling time pre- and post-automation was similar. However, time spent on inventory stock taking was found to be reduced significantly by 64% post-automation.31
Cost savings
The implementation of the robotic dispensing machine was reported to significantly decrease the cost of hospital/pharmacy expenditure in terms of stock values, inventory space and sales volume by 24–50% and personnel/labour costs by 4.6–25%, while increasing the over-the-counter (OTC) sales by 6.8%.28 31 35
Discussion
Adequacy and applicability of evidence base
As observed from our results, there is a paucity of literature documenting the possible benefits or drawbacks of pharmacy automation technologies. Given that pharmacy automations do not have or share a unified or widely recognised terminology, a large number of less specific search terms were used in order to minimise any arbitrary or incidental exclusion of papers. This resulted in 16 505 hits, of which less than 0.1% (13 of 16 505) formed the available data that could be used to evaluate the effectiveness of automation in an outpatient or community pharmacy, and many are cross-sectional or case studies which are considered low-strength evidence compared with the one interventional study.
Although many of these studies compared indicators pre- and post-automation, only one attempted to make a comparison of two automation solutions25 and another did not provide a comparator.32 This makes it difficult to determine if any particular solution or brand is better than another, so hospitals and pharmacies may find it difficult to assemble a credible evidence-backed proposal to justify the implementation of automation.
It does not help that, geographically, a great majority of evidence is based on study sites in the Western world (North America and Europe), while only one study was based in Asia (Singapore). This mounts an even greater challenge and roadblock for hospitals and pharmacies outside the Western bloc in gathering, evaluating and applying evidence regarding the impact that automation may bring, given the diverse differences in the structure of healthcare systems and mechanism of financing between different countries. Therefore, any benefits and impact that is applicable to the Western context may not be directly applicable to our local context, especially if taking into consideration the differences in pharmacy size, scale, volume and regulations.
Impact of pharmacy automation technologies
Despite the scarce evidence base, our results suggest that pharmacy automation does bring some benefits in various indicators.
Most studies24 25 28–30 concurred that pharmacy automation has indeed brought about a reduction in medication errors. This finding corroborated with other studies conducted in other settings, such as the ICU where medication preparation errors were reduced post-automation19 and also in an inpatient setting which showed that automation (specifically the unit dose dispensing system) prevented administration errors when used with appropriate surveillance.36
The additional finding that medication errors most commonly occurred during transcription32 suggests that we can consider focusing on automating the transcribing process and make use of technology to bring about an improvement in medication safety.
In addition, although automating the prescription filling process was found to lead to an increase in productivity and reduction in manpower required for the same job,24 28–30 33 pharmacy staff did not report any reduction in their workload post-automation.26 This could be attributed to a redeployment of manpower to automation-related job functions previously not required. Despite this, staff claimed in other studies that their stress level had reduced post-automation and their work/life balance had improved.23 24 Hence, although workload did not decrease, this apparent contradiction could suggest that there are intangible or indirect benefits for staff resulting from implementation of automation.
The cost savings reported by the studies could possibly be passed on to patients, but as neither return of investment measures nor capital costs or operating costs of the automation systems were commonly reported, there are insufficient data to determine if the marginal benefits reported outweigh the invisible costs of implementation and maintenance of these systems. More studies will thus need to be conducted to find out the actual overall cost of the implementation of these pharmacy automation systems and, by including estimated cost avoidance analyses from errors averted, to give a better picture of the financial viability of such implementations.
In addition, our findings revealed time savings post-automation in terms of patient waiting time, time spent on preparation of medications as well as on stock-taking.25 33–35 However, pharmacy staff noted no reduction in time spent on prescription filling even after automation was implemented.26 It is doubtful if such a small magnitude of time savings could bring about any perceivable benefits such as improving patient satisfaction or staff having more free time for other activities. This is in line with the ambiguity on the impact of automation on productivity and workload, as mentioned above, and it is thus difficult to justify time savings as a deciding factor in whether to implement automation systems in pharmacies.
Lastly, job satisfaction of pharmacy staff was generally not affected by implementing automation,23 25 although one study did observe an increase in satisfaction level post-automation.26 These results suggest that, even though manual prescription filling is associated with overwork and stress, staff satisfaction level is not much affected by it and automation solutions may not be the key to improving employee satisfaction. In fact, the job satisfaction level may not be an effective indicator to evaluate the merits of automation, given that it can be easily influenced by factors such as working environment, remuneration and corporate policies.
A survey previously performed in Singapore37 found that, from the patient’s point of view, the top three most important pharmacy services are: (1) prescription waiting time of less than 30 min; (2) accurate dispensing of medications; and (3) reasonable pricing. Our findings show that, although the effects of automation on work productivity and on time savings are uncertain, automation has indeed brought about reductions in medication errors.
With this limited knowledge, we can only propose that ADM implementation may be more beneficial in public hospitals or large community pharmacy chains that aim to provide affordable healthcare to patients which could be achieved through cost savings and economies of scale.
Our search strategy attempted to include automation in multiple aspects of outpatient pharmacy operations as a whole. However, the majority of identified studies focused solely on automating the prescription filling process. Further studies on new avenues to implement automation in this setting are needed to allow for comparison between the various robotic systems and selection of the best suited system needed, especially so with more new up-and-coming innovations such as the ‘drug vending machine’.
Examining later publications showed attempts to push boundaries on this front. One study each in 201131 and 201328 included ADM coupled with additional functions such as the automated transcription of medication orders through e-prescribing system. This is in line with the increasing adoption and integration of different electronic prescription systems worldwide, suggesting that, in the future, more segments of the pharmacy process may be automated with the use of other technological systems coupled with ADM to bring about greater efficacy and productivity in the workflow. For instance, a study has shown that ADM and bar coding systems have synergistic effects that further reduce medication errors.38
Conclusion
In this systematic review of pharmacy automation in the outpatient and community pharmacy setting, the results from the reviewed articles support the notion that pharmacy automation reduces medication error and brings about manpower savings and also possible cost savings. However, as to whether these positive impacts translate into perceivable benefits for staff and patients, the result is inconclusive as evidence was scarce and conclusions were sometimes contradictory between different studies. With the scarcity of studies conducted in this field and the over-representation of studies in the European/American setting, the generalisability of our conclusions to a local setting may be limited.
Footnotes
Contributors: YS and OCK implemented the study, monitored data collection for the whole project, cleaned and analysed the data, and drafted the paper. YS revised the final paper. YFL served as scientific advisor and oversaw the entire study. All authors approved the final script to be published.
Funding: The authors have not received a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Roser M. Life expectancy. 2016. https://ourworldindata.org/life-expectancy/
- 2. Department of Statistics, Singapore. Statistics Singapore - Life Expectancy at Birth. Singapore: Department of Statistics, 2016. http://www.singstat.gov.sg/statistics/visualising-data/charts/life-expectancy-at-birth [Google Scholar]
- 3. The World Bank Group. Population, total. 2016. http://data.worldbank.org/indicator/SP.POP.TOTL?locations=1W
- 4. Roser M, Ortiz-Ospina E. World population growth. 2017. https://ourworldindata.org/world-population-growth/
- 5. Ministry of Health, Singapore. Speech by Mr Gan Kim Yong, Minister for Health at The Groundbreaking Of The Lee Kong Chian School Of Medicine’s Novena Campus. 2012. https://www.moh.gov.sg/content/moh_web/home/pressRoom/speeches_d/2012/speech_by_Mr_Gan_Kim_Yong_Minister_for_Health_Groundbreaking_Lee_Kong_Chian_School_Of_Medicine_Novena_Campus.html
- 6. American College of Clinical Pharmacy. A vision of pharmacy’s future roles, responsibilities, and manpower needs in the United States. Pharmacotherapy 2000;20:991–1047. [DOI] [PubMed] [Google Scholar]
- 7. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm 1990;47:533–43. [PubMed] [Google Scholar]
- 8. Olson DS, Lawson KA. Relationship between hospital pharmacists' job satisfaction and involvement in clinical activities. Am J Health Syst Pharm 1996;53:281–4. [DOI] [PubMed] [Google Scholar]
- 9. Schommer JC, Pedersen CA, Gaither CA, et al. . Pharmacists' desired and actual times in work activities: evidence of gaps from the 2004 National Pharmacist Workforce Study. J Am Pharm Assoc 2006;46:340–7. 10.1331/154434506777069606 [DOI] [PubMed] [Google Scholar]
- 10. Goundrey-Smith S, Automation P. Pharmacy automation. Information technology in pharmacy: an integrated approach. London: Springer, 2013:95–119. [Google Scholar]
- 11. Koutnik-Fotopoulos E. Automation benefits pharmacies large and small Pharmacy Times . 2008. http://www.pharmacytimes.com/publications/issue/2008/2008-12/2008-12-5030
- 12. Fox BI, Pedersen CA, Gumpper KF. ASHP national survey on informatics: assessment of the adoption and use of pharmacy informatics in U.S. hospitals-2013. Am J Health Syst Pharm 2015;72:636–55. 10.2146/ajhp140274 [DOI] [PubMed] [Google Scholar]
- 13. Alonso AH, González CGR, Sáez MS. Information technology and automation in hospitals: strategies and experience in a tertiary hospital in Spain. EJHP Pract 2011;17:26–31. [Google Scholar]
- 14. Al Muallem Y, Al Dogether M, Al Assaf R, et al. . The implementation experiences of a pharmacy automation drug dispensing system in Saudi Arabia. Stud Health Technol Inform 2015;208:22–6. [PubMed] [Google Scholar]
- 15. Al Adham M, Abu Hamad B. Drug dispensing systems in Gaza hospitals: a comparative study. East Mediterr Health J 2011;17:722–9. 10.26719/2011.17.10.722 [DOI] [PubMed] [Google Scholar]
- 16. Singapore IHIS. Outpatient pharmacy automation system. 2017. https://www.ihis.com.sg/Project_Showcase/Healthcare_Systems/Pages/OPAS.aspx
- 17. Ng D. Automation hastens pharmacy dispensing Singapore Health . 2013. https://www.sgh.com.sg/about-us/newsroom/News-Articles-Reports/Documents/Singapore%20Health/SH25%20Nov-Dec%202013/08%20NEWS-Pharmacy%20using%20RFID%20V3%20AB.pdf
- 18. James KL. Assessing the impact of automated dispensing. 2013. http://www.hospitalpharmacyeurope.com/featured-articles/assessing-impact-automated-dispensing
- 19. Chapuis C, Roustit M, Bal G, et al. . Automated drug dispensing system reduces medication errors in an intensive care setting. Crit Care Med 2010;38:2275–81. 10.1097/CCM.0b013e3181f8569b [DOI] [PubMed] [Google Scholar]
- 20. Fayard C, Schweitzer M, Recoules C, et al. . Management of automated dispensing systems in oncology and haematology units. Int J Clin Pharm 2012;34:226. [Google Scholar]
- 21. Sinnemäki J, Sihvo S, Isojärvi J, et al. . Automated dose dispensing service for primary healthcare patients: a systematic review. Syst Rev 2013;2:1 10.1186/2046-4053-2-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wells GA, Shea B, O’Connell D, et al. . The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses, 2014. [Google Scholar]
- 23. James KL, Barlow D, Bithell A, et al. . The impact of automation on pharmacy staff experience of workplace stressors. Int J Pharm Pract 2013;21:105–16. 10.1111/j.2042-7174.2012.00231.x [DOI] [PubMed] [Google Scholar]
- 24. James L, Barlow D, Bithell A, et al. . Role conflict: occupational stressors versus patient safety. The effect of workload and pharmacy staff stressors on prevented dispensing incidents in hospitals with manual and automated dispensing systems. Int J Clin Pharm 2009;17(S2):B2–B3. [Google Scholar]
- 25. Franklin BD, O’Grady K, Voncina L, et al. . An evaluation of two automated dispensing machines in UK hospital pharmacy. Int J Pharm Pract 2008;16:47–53. 10.1211/ijpp.16.1.0009 [DOI] [Google Scholar]
- 26. Humphries TL, Delate T, Helling DK, et al. . Impact of an automated dispensing system in outpatient pharmacies. J Am Pharm Assoc 2008;48:774–9. 10.1331/JAPhA.2008.07114 [DOI] [PubMed] [Google Scholar]
- 27. Blaker K, White L, Poyser W. Dispensary assistants' attitudes and perceptions regarding automated dispensing machines in community pharmacies. Int J Healthc Technol Manage 2013;14:90–109. 10.1504/IJHTM.2013.055088 [DOI] [Google Scholar]
- 28. Beard RJ, Smith P. Integrated electronic prescribing and robotic dispensing: a case study. Springerplus 2013;2:295 10.1186/2193-1801-2-295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. James KL, Barlow D, Bithell A, et al. . The impact of automation on workload and dispensing errors in a hospital pharmacy. Int J Pharm Pract 2013;21:92–104. 10.1111/j.2042-7174.2012.00238.x [DOI] [PubMed] [Google Scholar]
- 30. Ysp O, Chen LL, Wong JA, et al. . Evaluating the impact of drug dispensing systems on the safety and efficacy in a Singapore outpatient pharmacy. Value Health 2014;17:A791–2. [DOI] [PubMed] [Google Scholar]
- 31. Walser L, Skinner J, Chisholm A. Early impact of a decentralized automated dispensing system in a small regional hospital. Can J Hosp Pharm 2011;64:81. [Google Scholar]
- 32. Cheung KC, van den Bemt PM, Bouvy ML, et al. . Medication incidents related to automated dose dispensing in community pharmacies and hospitals--a reporting system study. PLoS One 2014;9:e101686 10.1371/journal.pone.0101686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Mobach MP. The merits of a robot: a Dutch experience. J Pharm Pharm Sci 2006;9:376–87. [PubMed] [Google Scholar]
- 34. Lin AC, Huang YC, Punches G, et al. . Effect of a robotic prescription-filling system on pharmacy staff activities and prescription-filling time. Am J Health Syst Pharm 2007;64:1832–9. 10.2146/ajhp060561 [DOI] [PubMed] [Google Scholar]
- 35. Ruhle F, Braun R, Ostermann H. Impact of robotic dispensing machines in German pharmacies on business performance indicators. Libyan J Med 2009;4:146–51. 10.3402/ljm.v4i4.4840 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Pelayo S, Hassler S, Bernonville S, et al. . Safety-oriented usability test of a semi-automated unit dose system: role of task allocation between human and machine. Stud Health Technol Inform 2013;194:103–9. [PubMed] [Google Scholar]
- 37. Vhy T, Lim MM. Patients' perceptions and expectations of outpatient pharmacy services in a teaching hospital. Int J Pharm Pract 1997;5:128–32. 10.1111/j.2042-7174.1997.tb00897.x [DOI] [Google Scholar]
- 38. Oldland AR, Golightly LK, May SK, et al. . Electronic inventory systems and barcode technology: impact on pharmacy technical accuracy and error liability. Hosp Pharm 2015;50:34–41. 10.1310/hpj5001-034 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
ejhpharm-2017-001424supp001.pdf (173.3KB, pdf)