

Abstract
Sudden illness while driving has been identified as a major cause of vehicle collisions, particularly among taxi drivers. However, no previous studies have examined the factors contributing to the occurrence of health-related vehicle collisions. The current study aimed to identify the risk factors causing health-related vehicle collisions among taxi drivers, and to inform preventative interventions. A cross-sectional survey involving a written anonymous questionnaire was conducted for company-employed taxi drivers in Chiba Prefecture, Japan. A total of 1,739 drivers returned questionnaires. Drivers were classified into those who had experienced collisions or near-miss incidents caused by health problems (Event group), and those who had not (Non-event group). According to a multivariable logistic regression analysis, being unable to take vacation time (odds ratio [OR] 4.59, 95% confidence interval [CI] 2.2–9.58), having chronic diseases (OR 1.52, 95% CI 1.02–2.27), taking insufficient vacation time (OR 1.81, 95% CI 1.19–2.79), and difficulty reporting poor health conditions (OR 2.29, 95% CI 1.36–3.87) were significant factors for the likelihood of an event. Support for drivers to maintain well-balanced control of illnesses and improvement of working environments could prevent health-related events while driving.
Keywords: Health-related vehicle collisions, Risk factors, Taxi drivers, Prevention, Health management
Introduction
The number of traffic fatalities in Japan has decreased in recent years, reaching 3,694 in 20171), which is only 22.0% of the peak number of 16,765 fatalities in 1970. Moreover, the total number of casualties decreased from 1,183,616 in the peak year of 2004 to 580,847 in 20171). Many factors have contributed to these trends, including the development of safety vehicles and equipment, improvements in pre-hospital management, increasing public criticism in relation to collisions attributable to drunk driving and other avoidable causes, and judicial policy to impose more severe punishments related to vehicle collisions. However, because the number of fatalities has not substantially decreased in the last several years, the Japanese government has failed to achieve the objectives stated in the 9th Fundamental Traffic Safety Program, which had a target of less than 3,000 fatalities in 2015. Therefore, the development of effective preventive measures requires new perspectives.
Aging is a significant problem in developed countries, particularly for transportation-related workers. The average age of commercial drivers is 58.7 yr for taxi drivers, 49.9 yr for bus drivers and 47.5 yr for truck drivers, which is substantially older than the average age of all workers (42.2 yr) in Japan2). Older people are typically more likely to suffer from disease than younger people. Because of aging and work-related physical and mental loading, commercial drivers are considered to be at higher risk of lifestyle-related diseases, heart disease and cerebrovascular disease3). Especially for taxi drivers, progress of the coronary arteriosclerosis was more extensive than in the non-taxi drivers and had higher prevalence of diabetes mellitus and obesity4). In recent years, sudden illness while driving a vehicle has been identified as a major cause of vehicle collision, accounting for approximately one in 10 collisions5). Hitosugi et al. analyzed acute health changes while driving and subsequent collisions among commercial drivers6). The results indicated that taxi drivers had a relatively high number of collisions, and poor survival rates.
Therefore, the development of interventions for preventing vehicle collisions related to taxi drivers’ health problems is particularly important. Despite the need for improving understanding of taxi drivers’ health problems under current circumstances and developing countermeasures, no previous studies have examined the factors contributing to the occurrence of health-related vehicle collisions.
To identify the risk factors causing health-related vehicle collisions and to inform the development of preventative interventions, we conducted a cross-sectional survey in one urban district of Japan.
Subjects and Methods
We performed a cross-sectional survey in Chiba Prefecture. Chiba Prefecture has a population of approximately 6,260,000 people, and is located next to metropolitan Tokyo, in Japan7). Because Narita International Airport is located in Chiba Prefecture, a relatively large number of taxi drivers work there.
Subjects
The current study targeted company-employed taxi drivers belonging to the Chiba Association of TAXI. Among the approximately 9,000 drivers, the association randomly selected 4,581 drivers for the study, approximately half the total number of drivers.
Methods
The survey was conducted from September to November 2014. To protect the privacy of respondents and to obtain reliable answers to the questionnaire, we used an anonymous written questionnaire. The Association distributed the questionnaires to a half of drivers in each company and the participants were asked to return their completed questionnaires in a sealed envelope to one of the authors (MH) directly. The protocol of this study was approved by the ethics committee of Shiga University of Medical Science.
Questionnaire survey items
The questionnaire included questions on the following topics:
-
1
General characteristics of the driver: age, sex, height, weight
-
2
Years of work experience
-
3
Employment type: part-time/full-time
-
4
Work shift: day shift/alternate day shift
-
5
Company size: having 50 vehicles or more/10–49 vehicles/less than 10 vehicles
-
6
Living arrangement: living with family/living alone
-
7
Having a diagnosed disease: yes/no. If yes, diagnosed disease (multiple answers)
-
8
If yes in the previous question, the regularity of visiting a physician: regular/irregular
-
9
Annual medical checkup enforced by law: received/not received
-
10
Taking breaks during work: regular (a driver has a definite work schedule to take periodic breaks)/irregular (a driver get a break when he would like to do, such as eating or going to the bathroom); if regular, how many hours working without a break
-
11
Taking vacation time (paid-leave): sufficient/not sufficient/hardly
-
12
Experiences of health-related vehicle collisions or near-miss incidents: yes/no
-
13
If no in the previous question, understanding that acute health problems can cause collisions: yes/no
-
14
Reporting of poor health at any time: easy/difficult
Analysis methods
Drivers who had experienced collisions or near-miss incidents due to health problems were classified as the “Event group” and those without collisions or near-miss incidents were classified as the “Non-event group”. Moreover, quantitative data were classified as categorical data: age was classified as non-elderly persons and elderly persons (less than 65 yr of age/65 yr of age or older). Body mass index (BMI) was classified as low (less than 18.5), normal (18.5 or more and less than 25.0), high (25.0 or more). Work experience was classified as less than the median length in years (12.0 yr) and median length or more.
To explore the relationship between collisions and near-miss incidents with influential risk factors, we performed a logistic regression analysis. Risk factors with p-values <0.10 in univariable analysis were included in the multivariable model. The analyses were performed with SPSS Ver. 23 and p-values <0.05 were considered significant.
Results
Basic information about subjects
A total of 1,739 questionnaires (38.0% of the targeted subjects) were returned (Fig. 1). Most of the respondents (1,658 of 1,739) were male. The mean age was 60.6 ± 9.1 yr (ranging from 24 to 80 yr) and more than half of the drivers were in their sixties (Fig. 2). Elderly persons (65 yr or older) accounted for 39.6% of respondents. The average BMI score was 24.1, with a low range (less than 18.5) of 3.3%, a normal range (not less than 18.5 but less than 25.0) of 60.3% and a high range (25.0 or more) of 36.4%.
Fig. 1.
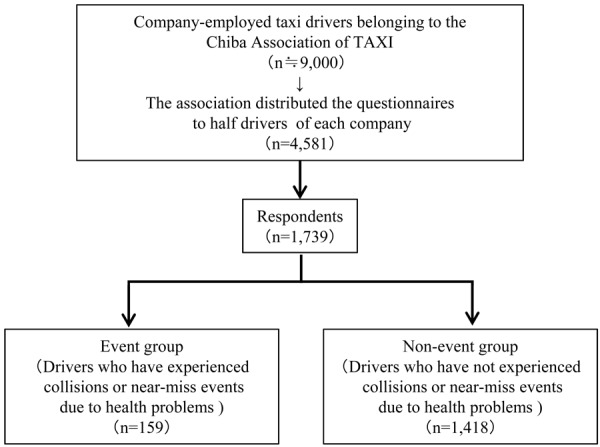
Participants flow.
Fig. 2.
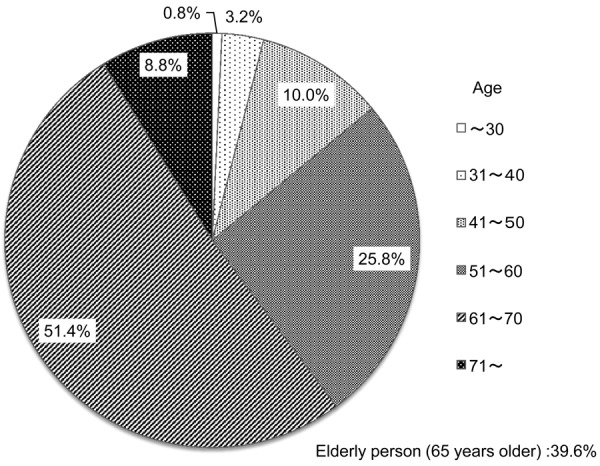
Age profile of drivers.
The results revealed that 79.5% of drivers lived with their family. The average duration of work experience was 14.7 ± 11.7 yr.
Regarding the size of the companies employing the drivers, 2.0% of respondents worked in small companies with less than 10 vehicles, 56.2% worked in medium scale companies with 10 to 49 vehicles and 41.9% worked in large companies with 50 or more vehicles.
Work shift of taxi drivers is roughly categorized into two types based on prescribed working hours. It is provided in the refinement criterion regulated by Ministry of Health, Labour and Welfare. Prescribed working hours of day shift are within 13 h, and that of alternate-day shift are within 21 h. Alternate-day shift drivers work from 11 to 13 times a month. In this study, 66.5% of drivers worked as alternate-day shift.
Lifestyle and driving habits
While working, nearly half of respondents (49.1%) took breaks at regular intervals, 3.3 ± 2.4 h on average, and others (50.9%) took breaks when they wished to do so, or ate a meal, or went to the bathroom.
Of the respondents, 1,243 (75.0%) reported that they were able to take enough vacation time, 367 (22.2%) reported that they could not take enough vacation time, and 47 persons (2.8%) reported that they could hardly take any vacation time. Regarding health complaints of the drivers, 1,535 respondents (92.8%) felt they could easily report their health difficulties to the company. However, the remaining 119 drivers (7.2%) expressed difficulty reporting illness to their employer.
Healthcare
Most respondents (96.2%) received an annual medical checkup enforced by law. We found that 1,021 (60.0%) drivers were diagnosed with chronic diseases, including hypertension (32.0%), hyperlipidemia (15.6%), diabetes (15.0%), lower back pain (14.2%), gout (4.3%), cardiovascular disease (3.9%), gastroduodenal ulcer (2.5%), headache (1.6%), brain disease (0.8%), and other diseases (6.1%). Of the diagnosed drivers, 79.0% regularly referred to a physician.
Events due to health problems
Of the respondents, 465 (26.7%) reported their experiences of acute health change.
Eleven respondents (0.7%) reported having collided with a motor vehicle due to acute health problems, and 148 drivers (9.4%) reported experiencing health-related near-miss incidents. Thus, 10.1% of respondents were included in the Event group. The survey revealed that 1,140 drivers (72.3%) understood that acute health problems can cause collisions, but had not experienced either health-related collisions or near-miss incidents. The remaining 278 drivers (17.6%) did not understand that acute health problems can cause collisions, and had not experienced either health-related collisions or near-miss incidents.
Risk factors
The results of the univariable logistic regression analyses of the relationship between collisions or near-miss incidents and associated risk factors are shown in Table 1. The results revealed that age (elderly or not), having chronic diseases, habits regarding taking breaks while driving, vacation time, and the reporting of poor health had statistically significant effects. To clarify the risk factors of health-related events, we performed a multivariable logistic regression analysis, using event as a dependent variable and elderly status, disease, breaks, vacation time, and the reporting of poor health as independent variables. The results revealed that having a chronic disease (odds ratio [OR] 1.52, confidence interval [95% CI] 1.02–2.27), not taking enough vacation time (OR 1.81, 95% CI 1.19–2.79), and difficulty reporting poor health (OR 2.29, 95% CI 1.36–3.87) were significant risks for event (Table 2). The most influential risk factor was being unable to take vacation time (OR 4.59, 95% CI 2.20–9.58).
Table 1. Results of univariable logistic regression analysis of the relationship between collisions or near-miss incidents and risk factors.
| Event Groupa | Non-event Groupb | Odds ratio | 95%CI | p-value | ||
|---|---|---|---|---|---|---|
| (N=159) | (N=1,418) | |||||
| Gender | ||||||
| Male | 153 | 1,352 | Reference | 0.56–9.69 | 0.25 | |
| Female | 2 | 41 | 0.43 | |||
| Age (elderly person) | ||||||
| Less than 65 yr | 109 | 854 | Reference | 1.01–2.16 | 0.02 | |
| 65 yr or older | 47 | 556 | 0.66 | |||
| Living arrangement | ||||||
| Living with family | 123 | 1135 | Reference | 0.75–1.73 | 0.54 | |
| Living alone | 31 | 251 | 1.14 | |||
| BMI | ||||||
| Normal | 90 | 791 | Reference | - | - | |
| Low | 3 | 48 | 0.55 | 0.67–1.35 | 0.78 | |
| High | 57 | 476 | 1.05 | 0.16–1.73 | 0.52 | |
| Work experiencec | ||||||
| 12 yr or more | 81 | 668 | Reference | 0.58–1.15 | 0.24 | |
| Less than 12 yr | 66 | 667 | 1.23 | |||
| Employment type | ||||||
| Part-time | 36 | 392 | Reference | 0.87–1.91 | 0.21 | |
| Full-time | 111 | 940 | 1.29 | |||
| Work shift | ||||||
| Day Shift | 7 | 74 | Reference | 0.36–1.85 | 0.66 | |
| Alternate-day shift | 111 | 978 | 0.83 | |||
| Company size (Number of vehicles held) | ||||||
| 50 vehicles or more | 55 | 539 | Reference | - | - | |
| 10–49 vehicles | 76 | 721 | 1.17 | 0.34–4.02 | 0.80 | |
| Less than 10 vehicles | 3 | 25 | 1.03 | 0.72–1.45 | 0.86 | |
| Disease | ||||||
| No disease | 50 | 581 | Reference | 1.01–2.13 | 0.02 | |
| Disease | 107 | 830 | 1.50 | |||
| Medical facility visit | ||||||
| Regular | 85 | 727 | Reference | 0.46–1.11 | 0.13 | |
| Irregular | 31 | 189 | 1.40 | |||
| Medical checkup | ||||||
| Every year | 143 | 1,265 | Reference | 0.37–1.88 | 0.67 | |
| Not every year | 7 | 52 | 1.19 | |||
| Breaks | ||||||
| Regular | 51 | 618 | Reference | 0.42–0.86 | 0.01 | |
| Irregular | 84 | 610 | 1.67 | |||
| Vacation time | ||||||
| Sufficient | 88 | 1,076 | Reference | - | - | |
| Not sufficient | 55 | 304 | 2.21 | 0.08–0.31 | <0.01 | |
| Hardly take vacation time | 15 | 29 | 6.32 | 0.18–0.70 | <0.01 | |
| Reporting of poor health | ||||||
| Easy | 127 | 1,275 | Reference | 0.19–0.49 | <0.01 | |
| Difficult | 27 | 83 | 3.27 | |||
aDrivers who have experienced collisions or near-miss events due to health problems. bDrivers who have not experienced collisions or near-miss events due to health problems. c: 12 yr. CI: Confidence Interval; BMI: body mass index.
Table 2. Results of multivariable logistic regression analysis odds ratio.
| Odds ratio | 95%CI | p-value | ||
|---|---|---|---|---|
| Disease | ||||
| No disease | Reference | - | - | |
| Disease | 1.52 | 1.02–2.27 | 0.04 | |
| Vacation time | ||||
| Sufficient | Reference | - | - | |
| Not sufficient | 1.81 | 1.19–2.79 | 0.01 | |
| Hardly take vacation time | 4.59 | 2.20–9.58 | p<0.01 | |
| Reporting of poor health | ||||
| Easy | Reference | - | - | |
| Difficult | 2.29 | 1.36–3.87 | p<0.01 | |
| Elderly person | ||||
| Non-elderly persona | Reference | - | - | |
| Elderly personb | 0.79 | 0.52–1.20 | 0.27 | |
| Breaks | ||||
| Take breaks regularly | Reference | - | - | |
| Do not take breaks regularly | 1.33 | 0.90–1.97 | 0.15 | |
a: Less than 65 yr, b: 65 yr or older. p-value is significant (<0.05). CI: Confidence Interval.
Discussion
To prevent health-related vehicle collisions, The Ministry of Land, Infrastructure, Transport and Tourism developed a Healthcare Manual for Drivers of Commercial Vehicles to manage the health conditions of commercial drivers in 2010, which was revised in 2014 to further improve management in Japan8). Furthermore, in 2016, the revised Road Transportation Act and the Trucking Business Act mandated managers of companies to comprehensively implement healthcare for drivers based on the results of annual medical checkups. In Japan, workers have to receive annual medical checkups in accordance with the Industrial Safety and Health Act. The examination consists of blood pressure, chest X-ray, electrocardiogram, clinical biochemistry, hematology, and urinalysis parameters, and so on. Therefore, detailed measures concerning drivers’ healthcare should be promoted within each company. However, most healthcare providers do not understand which measures are most useful for commercial drivers, owing to a lack of evidence. To our knowledge, there have been no reports analyzing the risk factors of health-related vehicle collisions based on large numbers of taxi drivers.
The current results suggest that having chronic diseases, taking insufficient vacation time, and difficulty reporting poor health conditions were significant risks for collision or near-miss events (Table 2). Among various chronic diseases, hypertension, hyperlipidemia and diabetes, so-called lifestyle diseases, were the three most common in the present survey. Generally, older people are more likely to suffer from disease than younger people6). This trend was also observed by our logistic regression analysis. Because the subjects of our analyses were relatively elder, more than half were sixty yr or more, we obtained high of these diseases. According to reports of health-related vehicle collisions of commercial drivers, heart disease and cerebrovascular disease accounted for approximately half of all collisions6). Lifestyle diseases also are known risk factors for cardiovascular and cerebrovascular diseases. Thus, maintaining a well-balanced control of lifestyle diseases is an important issue. One previous report suggested that blood pressure, cholesterol, triglycerides and blood glucose of drivers who caused health-related collisions were higher than the overall national average in Japan9). Therefore, keeping clinical examination results within a normal range is important for preventing health-related events.
We found that most respondents (96.2%) received law-enforced annual health checkups, and 60.0% of drivers were diagnosed with a chronic disease. However, not all diagnosed drivers had referred to a physician or received medical care. The results revealed that 79.0% of drivers regularly refer to a physician. Therefore, not only drivers themselves, but also the operations managers of the companies should check whether drivers have referred to a physician regularly and received medical care or not.
The current results indicate that insufficient vacation time was the most influential risk factor for collision-related events. A lack of sufficient vacation time is generally associated with a person experiencing accumulated fatigue and a lack of sufficient ability to care for their own health10). Ishimaru et al. suggested that taxi drivers’ cardiovascular disease risk might be increased by their unhealthy work style11). Thus, taking sufficient vacation time is likely to strongly influence the mental and physical health of drivers. In recent years, the taxi industry has faced increasingly difficult circumstances due to a reduction in the number of passengers and the impact of deregulation. The annual number of hours worked by taxi drivers is 192 h longer than the average for all workers2). The annual income (for males) is approximately 2,170,000 yen (19,200 dollars) lower than the average of all workers12). The taxi industry is a typical labor-intensive industry, and to improve labor productivity, there is no alternative but to depend on drivers working longer hours at lower wages. To improve this situation, official support for taxi drivers by government is required.
The current results revealed that difficulty reporting poor health conditions was associated with the occurrence of health-related events while driving. According to one report analyzing health changes of commercial drivers while driving, the survival rate of drivers after disease onset was significantly higher in bus drivers (93.2%) than taxi drivers (48.6%)6). Furthermore, sudden-illness related collision avoidance rates among drivers of moving vehicles were significantly higher among bus drivers (56.8%) than taxi drivers (17.8%)6). Also, the duration between starting work and the event was significantly shorter in bus drivers than in taxi drivers. Noticing an acute health changes in trivial state of taxi drivers is required for preventing health-related vehicle collisions. If a driver is aware of health difficulties while driving, they should voluntarily report their health problems to the company immediately, and avoid driving. Accordingly, operations managers should encourage drivers to voluntarily report their poor health and provide opportunities to cease driving easily.
The current study involved several limitations that should be considered. First, because information about medical histories and adherence of referral to the physician were obtained via self-assessment, the information may have differed from medical records. Thus, more reliable data (i.e., medical records or the results of annual health checkups) should be used for further analyses in future studies. Second, the amount of vacation time is subjectively decided. Because we sought to understand whether drivers were satisfied with their current situation concerning vacation time, we analyzed subjective responses about vacation time. However, to objectively examine the vacation time of each driver, the number of holidays within several months should be examined in further analyses. Third, this survey did not include questions about the adverse effects of medicines. Some medicines may influence drivers’ cognitive function or driving ability. In future, both positive and negative effects of medicine should be examined among drivers who use medicines daily. Fourth, because enough data set about the work environment or personal impressions of workplace were insufficient, we could not determine the impact of the working atmosphere on reporting health problems. Thus, more detailed data about the workplaces environment in each company would be accumulated for future analyses.
The results of the present study suggest that supporting drivers to maintain well-balanced control of their health, establishment of a working environment in which drivers can take sufficient vacation time and immediately stop driving when they feel the onset of poor physical health could lead to the prevention of health-related events. The interventions may also valuable for safety promotion, which leads to the prevention of health-related vehicle collisions of taxi drivers.
Conflict of Interest
The authors report no conflicts of interest.
Acknowledgments
We would like to acknowledge and express our gratitude to all respondents from the Chiba Association of TAXI who took part in this questionnaire survey.
References
- 1.National Police Agency. State of occurrence of traffic accidents in 2017. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&lid=000001202708. Accessed May 1, 2018.
- 2.Japan Ministry of Health, Labour and Welfare. Basic survey on working conditions in 2017. https://www.e-stat.go.jp/stat-search/files?page=1&layout=datalist&toukei=00450091&tstat=000001011429&cycle=0&tclass1=000001098975&tclass2=000001098977&tclass3=000001098985&second2=1. Accessed May 1, 2018.
- 3.Fujino Y, Tsukahara T, Mizogami T, Yoshimura T. (2002) Field survey of health management work by operations manager. Occup Health J 25, 45–9. [Google Scholar]
- 4.Kurosaka K, Daida H, Muto T, Watanabe Y, Kawai S, Yamaguchi H. (2000) Characteristics of coronary heart disease in Japanese taxi drivers as determined by coronary angiographic analyses. Ind Health 38, 15–23. [DOI] [PubMed] [Google Scholar]
- 5.Tervo TMT, Neira W, Kivioja A, Sulander P, Parkkari K, Holopainen JM. (2008) Observational failures/distraction and disease attack/incapacity as cause(s) of fatal road crashes in Finland. Traffic Inj Prev 9, 211–6. [DOI] [PubMed] [Google Scholar]
- 6.Hitosugi M, Gomei S, Okubo T, Tokudome S. (2012) Sudden illness while driving a vehicle—a retrospective analysis of commercial drivers in Japan. Scand J Work Environ Health 38, 84–7. [DOI] [PubMed] [Google Scholar]
- 7.Chiba Prefectural Government. Introduction of Chiba. https://www.pref.chiba.lg.jp/toukei/toukeidata/joujuu/geppou/2018/201804.html. Accessed May 1, 2018.
- 8.Japan Ministry of Land, Infrastructure, Transport and Tourism. Healthcare manual for drivers of fleet vehicles (revised edition, 2016). http://www.mlit.go.jp/jidosha/anzen/03analysis/resourse/data/h26_2.pdf. Accessed May 1, 2018.
- 9.Japan Ministry of Land, Infrastructure, Transport and Tourism. Traffic accident factor analysis report for fleet vehicles. 2014. http://www.mlit.go.jp/jidosha/anzen/03analysis/resourse/data/h25_2.pdf. Accessed Aug. 28, 2018.
- 10.Koyama H, Suzuki K, Sakai K. (2011) Working conditions, fatigue, and sleep of truck drivers (2nd report): an analysis of cases of fatigue and related factors in long-haul truck drivers. Rodo Kagaku 87, 121–35. [Google Scholar]
- 11.Ishimaru T, Arphorn S, Jirapongsuwan A. (2016) Hematocrit levels as cardiovascular risk among taxi drivers in Bangkok, Thailand. Ind Health 54, 433–8. 10.2486/indhealth.38.15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Japan Federation of Hire-Taxi Associations. Current state of wages and working hours of taxi drivers for 2016. http://www.taxi-japan.or.jp/pdf/toukei_chousa/tingin28.pdf. Accessed May 1, 2018.