

In this correspondence, we briefly explain how details on cardio-ankle vascular index (CAVI; [1]) as recently released by Fukuda Denshi [2] can be used to convert CAVI into CAVI0[3]. We provide an easy-to-use PDF calculator as well as a Microsoft Excel workbook to facilitate this process (Supplemental digital content 1 and 2).
We have recently investigated the theoretical blood pressure dependence of cardio-ankle vascular index as measured using the VaSera device (Fukuda Denshi Co., Ltd., Tokyo, Japan) and proposed a novel, corrected index: CAVI0[3]. Direct conversion between CAVI and CAVI0 proved difficult, as the CAVI equation contains two proprietary scale coefficients a and b[1]:
 |
with PWV the pulse wave velocity from the heart to the left or right ankle (resulting in L-CAVI or R-CAVI, respectively), Ps and Pd the SBP and DBP as measured by the VaSera device at the right upper arm (regardless of computing L-CAVI or R-CAVI [2,4]), and  the blood mass density [2].
the blood mass density [2].
We previously set out to estimate scale coefficients a and b from measurement data [4]. Such method, however, necessarily has the limitation that a and b can only be obtained approximately and not exactly. Recently, Fukuda Denshi fully disclosed the values of a and b, as well as other details on the calculation of CAVI [2] – a step that should be applauded. This disclosure allows for a direct, exact conversion of CAVI into CAVI0:
 |
with Pref = 100 mmHg a reference pressure [3]. The values of a and b in the CAVI equation are different for different ranges of CAVI [2]. Two cut-off points are implemented, resulting in three sets of values for the coefficients a and b. Figure 1 visualizes these variable scaling coefficients, as well as the cut-off points in CAVI and unscaled CAVI. This also implies that, when converting CAVI to CAVI0 (Eq. 2), the values for a and b should be matched to the measured value of CAVI.
FIGURE 1.

Influence of the use of three sets of scale coefficients a and b[2] on the relationship (y = ax + b) between cardio-ankle vascular index (CAVI, y) and unscaled CAVI (x).
To simplify the CAVI-to-CAVI0 conversion process, we created an easily fillable Adobe PDF form for conversion of single CAVI measurements (Fig. 2, Supplemental digital content 1) as well as a Microsoft Excel workbook for conversion of larger data sets (Supplemental digital content 2). Note that the PDF form was designed to be opened using Adobe Reader (http://www.adobe.com/go/getreader); other PDF readers may not support in-PDF calculations.
FIGURE 2.
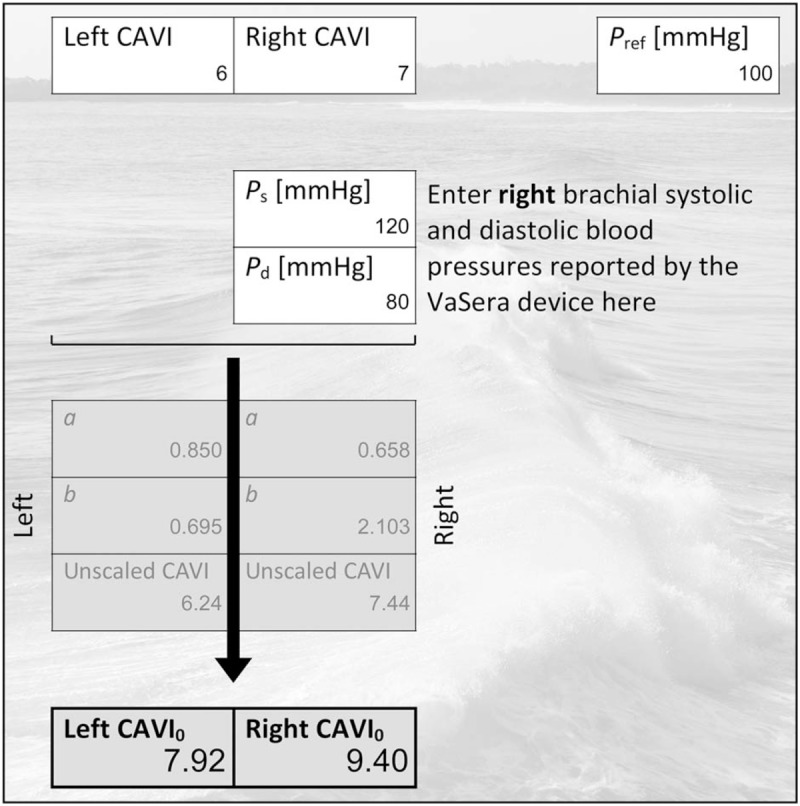
Screenshot of Adobe PDF CAVI-to-CAVI0 conversion tool with a completed CAVI-to-CAVI0 conversion (Supplemental digital content 1). The user enters CAVI and SBP and DBP values (Ps and Pd) in the light boxes, after which the form automatically determines the appropriate scale coefficients (a and b), determines unscaled CAVIs, and converts those to CAVI0s. CAVI, cardio-ankle vascular index; CAVI0, cardio-ankle vascular index zero [3]; Pref, reference pressure [3].
The critical reader is pointed to some nomenclature variations: in this correspondence, CAVI as provided by the VaSera device is simply termed CAVI; our previous studies referred to it as CAVIVS[3,4]. Unscaled CAVI (this correspondence) is called haβ by Takahashi et al.[2] and was referred to simply as CAVI in our previous studies [3,4]. Finally, we would like to point out that a researcher with full access to the CAVI (VaSera) source data can also compute CAVI0 (Eqs. 9 and 10 in [4]) without CAVI as an intermediate step.
In conclusion, we hope that this correspondence and the tools provided will help every user interested in using CAVI0 – whether clinician, researcher, or engineer – to easily convert CAVI into CAVI0 values.
ACKNOWLEDGEMENTS
This work was supported by grants from the Netherlands Organisation for Scientific Research (Rubicon 452172006) and the European Union's Horizon 2020 research and innovation programme (grant agreement 793805). Suggestions by Dr Elien B. Engels are gratefully acknowledged.
Conflicts of interest
There are no conflicts of interest.
Supplementary Material
Supplementary Material
REFERENCES
- 1.Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb 2006; 13:101–107. [DOI] [PubMed] [Google Scholar]
- 2.Takahashi K, Yamamoto T, Tsuda S, Okabe F, Shimose T, Tsuji Y, et al. Coefficients in the CAVI equation and the comparison between CAVI with and without the coefficients using clinical data. J Atheroscler Thromb 2019; 26:465–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Spronck B, Avolio AP, Tan I, Butlin M, Reesink KD, Delhaas T. Arterial stiffness index beta and cardio-ankle vascular index inherently depend on blood pressure but can be readily corrected. J Hypertens 2017; 35:98–104. [DOI] [PubMed] [Google Scholar]
- 4.Spronck B, Mestanik M, Tonhajzerova I, Jurko A, Jurko T, Avolio AP, Butlin M. Direct means of obtaining CAVI0-a corrected cardio-ankle vascular stiffness index (CAVI)-from conventional CAVI measurements or their underlying variables. Physiol Meas 2017; 38:N128–N137. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.