

Abstract
Background and study aim Malignant bowel obstruction can cause significantly distressing symptoms in patients with end stage cancers, often requiring invasive surgical intervention. With such procedures, risks often outweigh the benefit. We report a novel application of the AXIOS stent and electrocautery-enhanced delivery system to create an enterocolostomy to bypass a small bowel obstruction in the setting of recurrent malignant bowel obstruction. A 72-year-old patient presented with recurrent malignant bowel obstruction and was deemed unfit for surgery. Endoscopic ultrasound was used to deploy an AXIOS stent, creating an enterocolostomy resolving the obstruction.
Introduction
Malignant intestinal obstruction often results in distressing symptoms and may complicate end-of-life decision-making. Surgery is invasive and the clinical setting is typically complex, introducing additional adverse events (AEs). Recovery from surgery may be prolonged, especially in patients with advanced cancers, complicated medical issues, and diminished life expectancy. With terminal cancers, the expected survival is limited and going through invasive surgical procedures increases morbidity, involving up to two-thirds of the patient’s remaining life 1 . Mortality can be as high as 32 % and the chances for serious AE are significant (up to 44 %) 1 .
We report a novel application of the AXIOS stent and electrocautery-enhanced delivery system (Boston Scientific, Marlborough, Massachusetts, United States) to create an enterocolostomy to bypass a small bowel obstruction in the setting of recurrent malignant bowel obstruction in a patient with terminal cancer.
Case report
A 72-year-old female with past medical history of non-Hodgkin lymphoma, breast cancer, advanced metastatic pancreatic adenocarcinoma on chemotherapy, and recent history of large bowel obstruction status post-placement of a transverse colonic stent, presented with chief complaints of abdominal pain, nausea and vomiting. Computerized tomography (CT) of the abdomen demonstrated small bowel obstruction ( Fig. 1 )
Fig. 1.

Dilated loops of small bowel (left) and previously placed transverse colonic stent (right).
Conservative management with bowel rest, nasogastric suction, and intravenous fluids failed to resolve symptoms. Small bowel obstruction was presumed due to tumor burden. After detailed interdisciplinary discussions with the patient, it was decided to pursue endoscopic guided decompression.
The patient was placed supine on a fluoroscopy table and sigmoidoscopy performed to remove stool and introduce water to promote acoustic coupling. A GF-UCT180 curved linear array echoendoscope (Olympus, Tokyo, Japan) was advanced into the sigmoid colon identifying multiple dilated bowel loops. The bowel was punctured with a 19-gauge EZ Shot 3 needle (Olympus, Tokyo Japan) and contrast was injected delineating the local small bowel anatomy ( Fig. 2a ). A 0.025” VisiGlide guidewire (Olympus, Tokyo, Japan) was advanced into the small bowel and the needle exchanged for a 15 mm × 10 mm AXIOS stent and electrocautery-enhanced delivery system (Boston Scientific, Marlborough, Massachusetts, United States) which was deployed using endoscopic ultrasound (EUS) and fluoroscopic guidance ( Fig. 2b ).
Fig. 2 a.
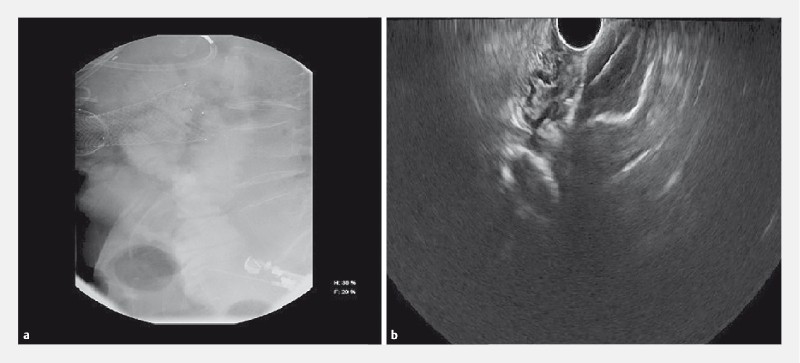
Fluoroscopic image depicting small bowel puncture using the Olympus needle. b Endoscopic ultrasound image demonstrating the AXIOS stent.
The linear echoendoscope was withdrawn, and a sigmoidoscope was used to inspect the stent and visualize the small bowel mucosa through the stent ( Fig. 3 ).
Fig. 3.
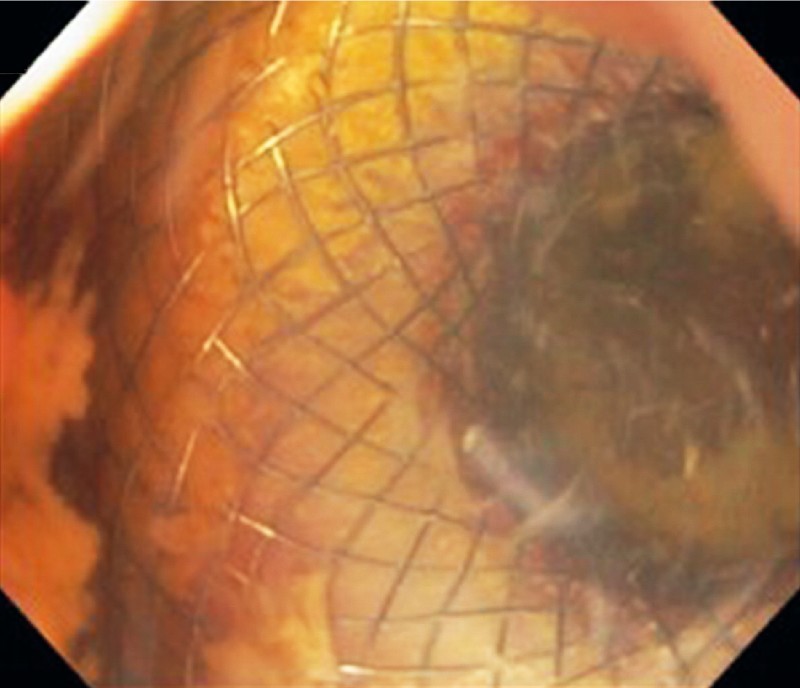
Endoscopic image showing the small bowel mucosa through the AXIOS stent.
Repeat CT scan with oral contrast demonstrated decompression of the small bowel and patency of the enterocolostomy stent ( Fig. 4 ).
Fig. 4.
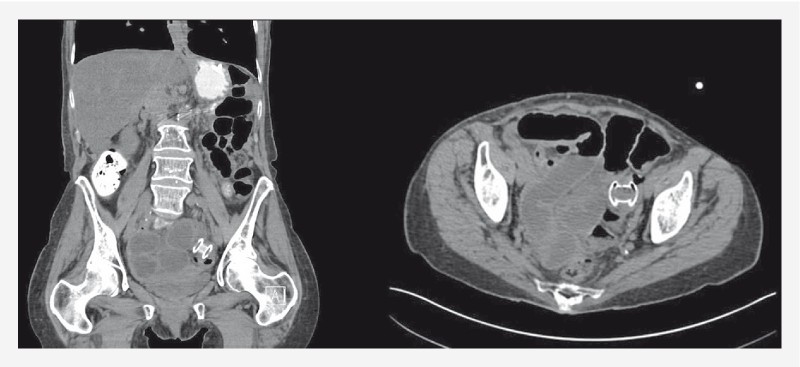
Successful placement of the AXIOS stent, coronal section (left) and transverse section (right).
The patient improved symptomatically after the procedure and tube feeding was resumed within 24 hours of the procedure. Antibiotics were continued for 5 days post-procedure. No immediate postoperative AEs were noted with our patient. The patient was subsequently discharged and followed up as an outpatient. After months of progressively worsening metastatic cancer and decline in functional status, the patient opted for palliative care. At this point discussions are underway regarding hospice care.
Discussion
Three percent to 15 % of cancer patients with intraabdominal tumors have malignant bowel obstruction 2 . It may be acute or chronic; partial or complete. Typically acute and complete obstructions present with severe symptoms compared to partial and slowly developing ones. Also, bowel obstruction can have varying predominance of symptoms depending on the site of obstruction. Typically, proximal obstruction presents with nausea/vomiting as the predominant complaint 3 . It may lead to dehydration, significant electrolyte imbalance, toxemia (related to decomposition of intestinal contents and bacterial overgrowth), bowel infarction and/or perforation 4 . The initial approach includes bowel rest, intravenous fluids, nasogastric decompression and avoidance of medications that impede bowel motility. If conservative measures fail, surgical intervention is often required. However, surgery is a source of significant morbidity in patients with end-stage diseases/malignancies who already have a low life expectancy.
Our case depicts a novel technique to bypass the mechanically obstructed zone as a palliative approach to malignant bowel obstructions. This approach, as described above, not only minimizes perioperative morbidity, but also allows for early functional return, which is essential for patients with already decreased life expectancy. A major challenge to this procedure is the technical ability to choose the most distal loop of bowel among the multiple dilated loops available, which may be complicated by anatomical restraints, and the ability to successfully deploy the stent. Such cases can be technically challenging and the failure to successfully complete the procedure may lead to an iatrogenic perforation requiring emergent surgical intervention and laparotomy.
Conclusion
EUS use to deploy an AXIOS stent, creating an enterocolostomy resolving malignant bowel obstruction, was successful in the case presented here. Further prospective studies of this procedure will help to better understand the long-term and short-term effects on morbidity and mortality.
Footnotes
Competing interests None
References
- 1.Paul Olson T J, Pinkerton C, Brasel K J et al. Palliative surgery for malignant bowel obstruction from carcinomatosis: a systematic review. JAMA Surgery. 2014;149:383–392. doi: 10.1001/jamasurg.2013.4059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tuca A, Guell E, Martinez-Losada E et al. Malignant bowel obstruction in advanced cancer patients: epidemiology, management, and factors influencing spontaneous resolution. Cancer Man Res. 2012;4:159–169. doi: 10.2147/CMAR.S29297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cheadle W G, Garr E E, Richardson J D. The importance of early diagnosis of small bowel obstruction. Am Surg. 1988;54:565–569. [PubMed] [Google Scholar]
- 4.Wright H K, OʼBrien J J, Tilson M D. Water absorption in experimental closed segment obstruction of the ileum in man. Am J Surg. 1971;121:96–99. doi: 10.1016/0002-9610(71)90083-3. [DOI] [PubMed] [Google Scholar]